
Abstract
Patients after stroke who are nonambulatory require resources, and independent walking becomes a major determinant of the ability to participate in activities of daily living. Our objective was to determine the probability of walking for patients who are nonambulatory in the first month after stroke. We performed a systematic review and meta-analysis of consecutive, prospective studies of nonambulatory patients within the first month after stroke in rehabilitation and acute units. The outcomes were the probability of achieving independent walking at three-, six- and 12 months after stroke. Twenty-six studies were included in the review. Seventeen studies comprising 2856 participants were entered into meta-analyses. For initially nonambulatory stroke patients managed in a rehabilitation unit, the probability of independent walking was 0·60 (95% CI 0·47–0·74, 1373 participants) at three-months, 0·65 (95% CI 0·53–0·77, 444 participants) at six-months and 0·91 (95% CI 0·81–1·00, 24 participants) at 12 months. For patients managed in an acute unit, the probability of independent walking was 0·39 (95% CI 0·27–0·52, 634 participants) at three-months, 0·69 (95% CI 0·46–0·92, 405 participants) at six-months and 0·74 (95% CI 0·59–0·88, 34 participants) at 12 months. 60% of patients managed in a rehabilitation unit who are nonambulatory in the first month after stroke will regain independent walking compared with 39% of those managed in an acute unit. This information can be used clinically to make decisions about allocation of rehabilitation resources, education of patients and carers, and for discharge planning.
Introduction
The ability to regain independent walking after stroke is of great importance to patients and health care providers alike. People fear losing independence more than anything else and the ability to walk promotes independence (1). Often after stroke, the probability of walking again is the first question that patients ask of health care providers. Regaining the ability to walk is a major determinant of a person's ability to participate in activities of daily living and therefore of discharge destination (2, 3).
There are two systematic reviews evaluating prognostic factors relating to walking after stroke (4, 5). Kwakkel and colleagues' review suggested that the predictors for outcome of walking after stroke were age; previous stroke; urinary continence; consciousness at onset; disorientation in time and place; severity of paralysis; sitting balance; admission ADL score and level of social support and metabolic rate of glucose outside the infarct area in hypertensive patients (4). More recently, Meijer and colleagues' review suggested that there was insufficient quality of data to provide predictions, although there was some evidence that low initial ADL functioning, high age, cognitive disturbance, paresis of the limbs, reduced initial level of consciousness, previous hemiplegia, homonymous hemianopia, visual extinction, constructional apraxia, no admission to a stroke unit, nonlacunar stroke, visuospatial construction problems, urinary incontinence and female gender were related to poorer outcome after stroke (5). Both these reviews included patients who were initially ambulatory and nonambulatory. What is still not clear is the probability of independent walking for people who are nonambulatory initially after stroke. Patients who are nonambulatory have generally had a devastating stroke, and patients with severe strokes require substantial physical and economic resources for rehabilitation or future care (6, 7). Thus, the objective of this systematic review was to determine the probability of walking for patients who are nonambulatory in the first month after stroke.
This systematic review examined patients managed in rehabilitation and acute units separately, because it is possible that there will be different outcomes in terms of walking between these settings. For example, acute units provide care for a full range of patients after stroke, with varying degrees of disability, including patients who are likely to walk quickly and go directly home without requiring inpatient rehabilitation. Therapeutic input may be more extensive in some rehabilitation units, thus also contributing to a different walking outcome. We were interested in examining the probability of regaining independent walking because it is important in enabling patients to participate in the community (8). Given that the majority of functional recovery after stroke occurs within the first 12 months (9) we examined the recovery of walking across this time frame, which encompasses inpatient rehabilitation (average discharge about three-months) and outpatient rehabilitation (average discharge about six-months).
The specific research questions for this study were:
In patients, who are managed in a rehabilitation unit and are nonambulatory within one-month of stroke, what is the probability of regaining independent walking within 12 months?
Is the probability any different for patients who are managed in an acute unit?
Knowing the probability of regaining walking of patients who are initially nonambulatory will provide a benchmark for walking outcomes. This information may also contribute to the process of triaging patients in acute units to home, rehabilitation or a care facility and would also allow education of family and carers regarding general expectations of walking outcome in patients who are nonambulatory in the first month after stroke.
Method
Identification and selection of studies
Searches were conducted of the following databases: MEDLINE (1966 to September 2010), CINAHL (1982 to September 2010), EMBASE (1980 to September 2010), Web of Science (1982 to September 2010) and Scopus (1960 to September 2010), without language restrictions, for relevant articles. Search terms included words relating to stroke (e.g. cerebrovascular disorder, CVA, infarct, bleed, brain, hemiplegia, etc.), prognosis (e.g. risk, outcome assessment, predict, follow-up, etc.), and locomotion (e.g. walking, gait, ambulation, mobility, etc.). Title and abstracts were displayed and screened by one reviewer to identify relevant studies. Full paper copies of relevant studies were retrieved and their reference lists were screened. The methods of retrieved papers were examined against predetermined inclusion criteria (Fig. 1) by two independent reviewers. Conflict of opinion was resolved by consensus after discussion with a third reviewer.
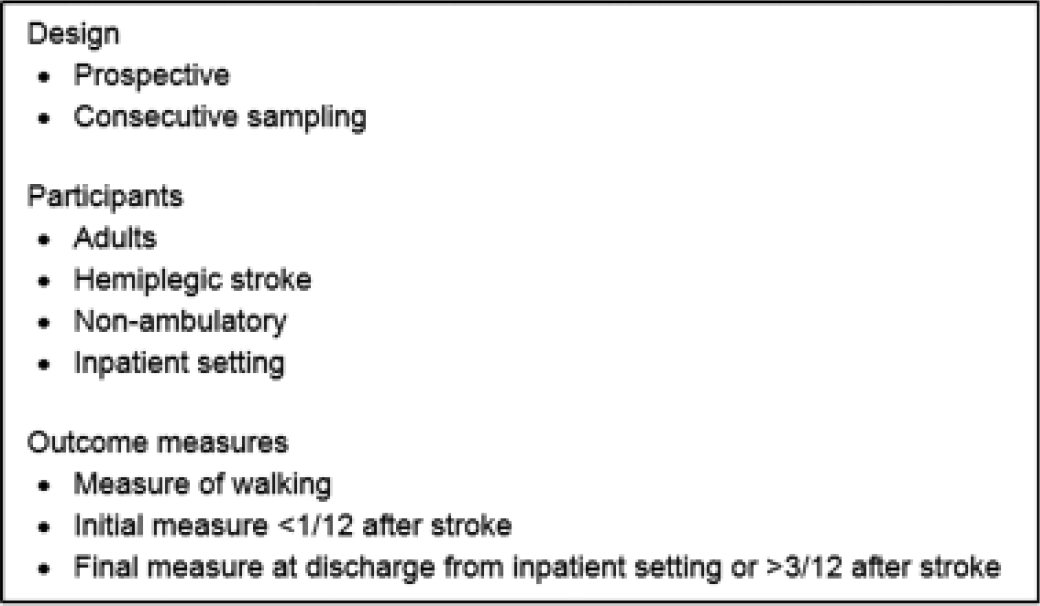
Inclusion criteria.
Assessment of characteristics of studies
Quality
The quality of included studies was determined using the screening tool of prognostic studies developed by Hayden et al. (10). Studies were evaluated using the four categories relevant to this systematic review: study participation (criteria included that the sample represented the population of interest in key characteristics), study attrition (criteria included that the loss to follow-up was not associated with key characteristics), measurement of outcomes (criteria included that the measurement was clearly defined as well as valid and reliable) and measurement of confounders (criteria included that the important potential confounders were appropriately accounted for by valid and reliable measurement). Studies were rated as either meeting the criteria, partly meeting the criteria or not meeting the criteria for each of these categories. A study was defined as good quality if it either
met the criteria for three categories or met the criteria for two categories and partly met the criteria for the other two categories.
Studies were evaluated by two reviewers independently with disagreements resolved by a third reviewer.
Participants
Participants had to be patients within one-month after a stroke, who were nonambulatory. Age, gender, the number of participants in the sample, inclusion criteria into the study and the time between stroke onset and initial walking measure were recorded and compared to examine similarity between the studies.
Settings
Studies where participants were admitted to hospital were included. The setting where the initial measurement of walking ability was completed was recorded and compared to examine similarity between the studies. Acute units included acute stroke units or general medical units, thereby comprising a nonselected population of patients after stroke. Rehabilitation units included any inpatient rehabilitation unit, where patients were selected and transferred after an acute episode of care.
Outcome measures
Measures of walking, time of measurement since stroke and definition of nonambulatory, as well as definition of ambulatory, were recorded and compared to examine similarity between the studies. Where multiple measures of walking were presented, independent walking was defined as being able to walk with/without aids, but without human assistance.
Data analysis
Data were extracted from the included studies by one reviewer and cross-checked by a second reviewer. Information about the method (i.e. design, participants, measures) and outcome data (i.e. number of participants that could walk independently) was extracted. Authors were contacted where there was difficulty extracting the data.
Walking outcome was examined over a 12-month time frame, three categories were then developed: three-, six- and 12-months after stroke. Meta-analyses were performed to calculate the pooled estimate of the proportion of patients that could walk independently and reported with 95% CI. A fixed effects model was used. In the case of significant statistical heterogeneity, I2>50% (11), a random effects model was applied to check the robustness of the results. The meta-analyses were performed using The MIX–Meta-Analysis Made Easy program version 1.7 (12, 13).
Results
Flow of studies through the review
The search returned 1010 studies. After screening the titles and abstracts, 66 papers were retrieved for evaluation of full text. Forty studies failed to meet the inclusion criteria and therefore 26 papers were included in the review. Of these 26 papers, after contacting authors, 17 had data available to be entered into meta-analyses (Fig. 2).
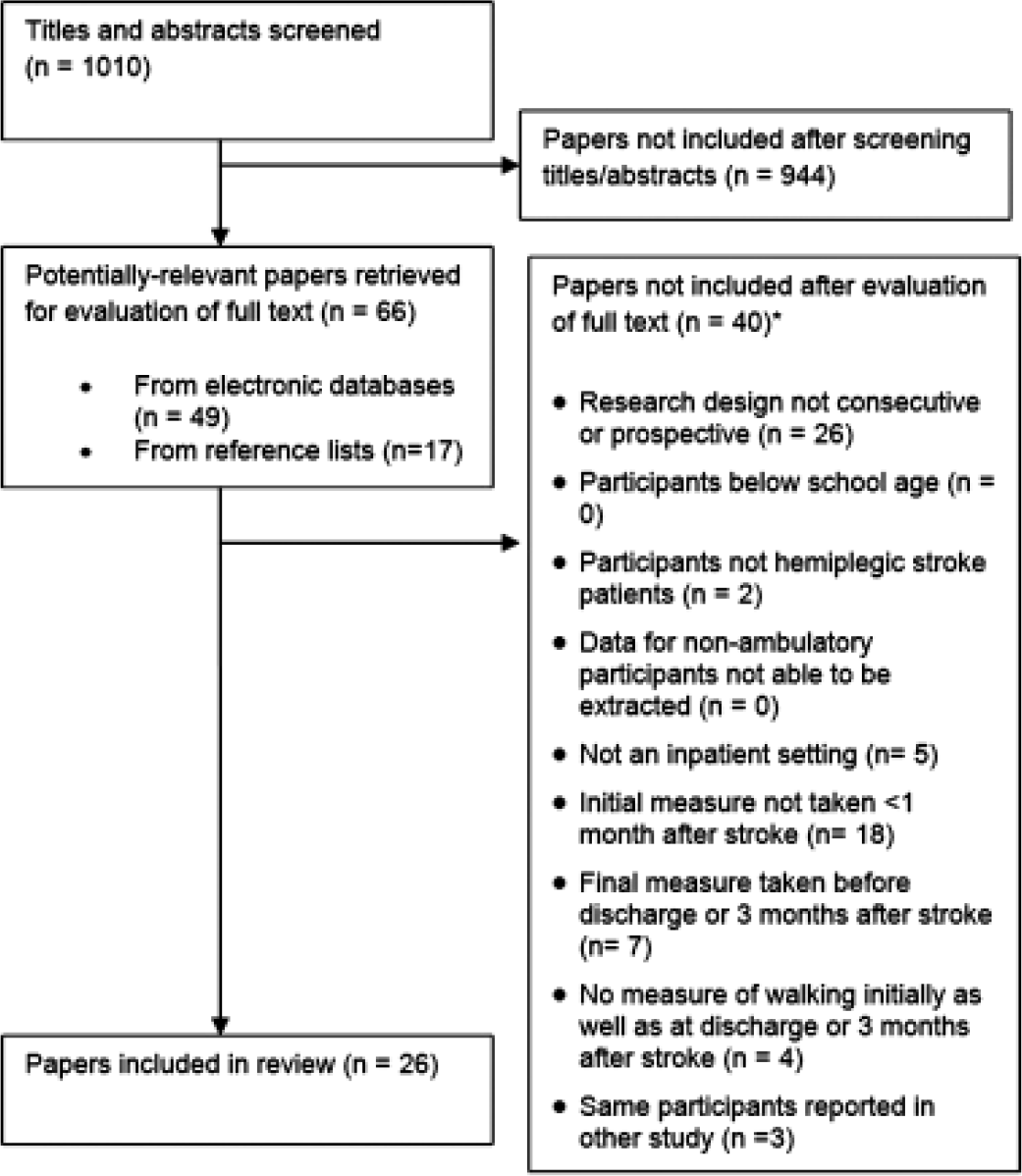
Flow of studies through the review. *Papers may not have been included for failing to meet more than one inclusion criteria.
Description of studies
The quality of the included studies is outlined in Table 1 and a summary of the studies is presented in Table 2.
Quality of included studies (n=26)
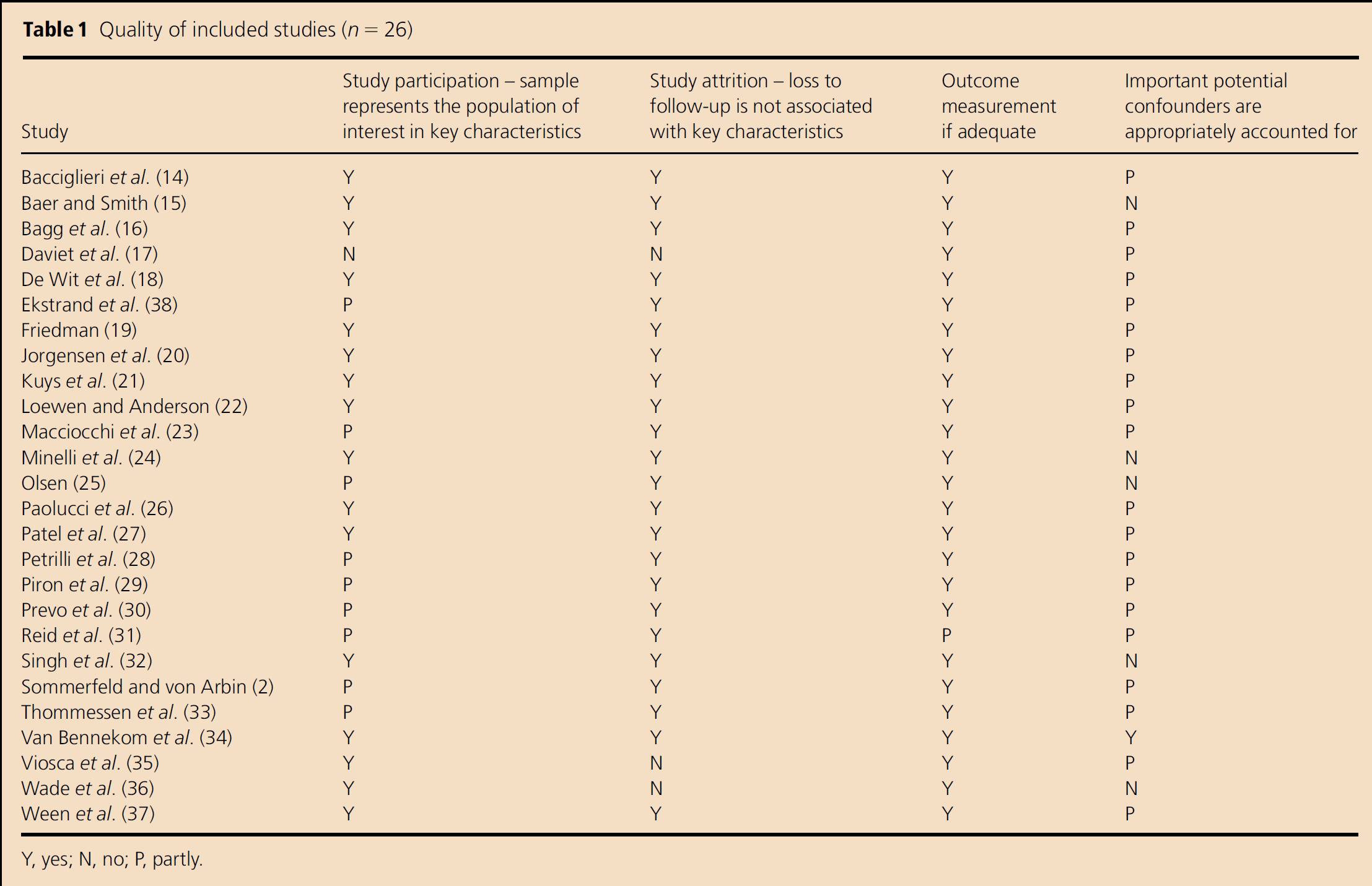
Y, yes; N, no; P, partly.
Summary of included studies (n=26)

Data recorded in the table, including number of nonambulatory participants, the outcome measure (in the case of multiple measures), and the time of follow-up measures were used for the meta-analyses. n, number of nonambulatory participants/number of participants in the sample; Acute, acute unit; rehab, rehabilitation unit; FIM, functional independence measure; MAS, Motor Assessment Scale for Stroke; BI, Barthel Index.
Quality
Of the 26 studies included in this review, 21 were of good methodological quality, and of the 17 entered into the meta-analyses, 13 were of good methodological quality. The sample was representative of the population in 62% of studies and partly representative in 35%, loss to follow-up was not associated with key characteristics in 88% of studies, outcome measurement was adequate in 96% of studies and important potential confounders were at least partly accounted for in 80% of studies.
Participants
The mean ages of participants across the studies ranged from 58 to 80 years old and the mean time of initial measures of walking ranged from two- to 31 days. Patients were managed either in a rehabilitation unit (n=15) or an acute unit (n=11).
Outcome measures
Although many different measurement tools were used to report walking, independent walking was reported in 96% of studies as the ability to walk alone or with an aid, but without human assistance. Nonambulatory was defined as FIM mobility and locomotion subscale score <6 (n=5), Barthel index mobility subscale score of 0, 5 or 10 (n=6), Barthel index mobility subscale score of 0–2 (n=3), MAS item 5 score 0–2 (n=2), COVs mobility scale item 5 score 0–4 (n=1), modified Rankin scale >3 (n=1), Hemiplegic Stroke Severity Scale >3 (n=1) and walking speed <0·15 m/s (n=1). The remaining studies (n=6) used scales developed by the authors to define nonambulatory. Independent walking data were available to be used in a meta-analysis from patients managed in a rehabilitation unit at three-months (n=9) and at six-months (n=3) and from those managed in an acute unit at three-months (n=6) and at six-months (n=3).
Probability of regaining independent walking
Rehabilitation unit
At three-months, the probability of initially nonambulatory stroke survivors regaining independent walking was examined by pooling data from nine studies (14, 18, 21, 25, 26, 28, 29, 32, 35) comprising 1373 participants (Fig. 3). The probability of independent walking in initially nonambulatory stroke patients was 0·60 (95% CI 0·47–0·72). Data were unavailable from three studies.
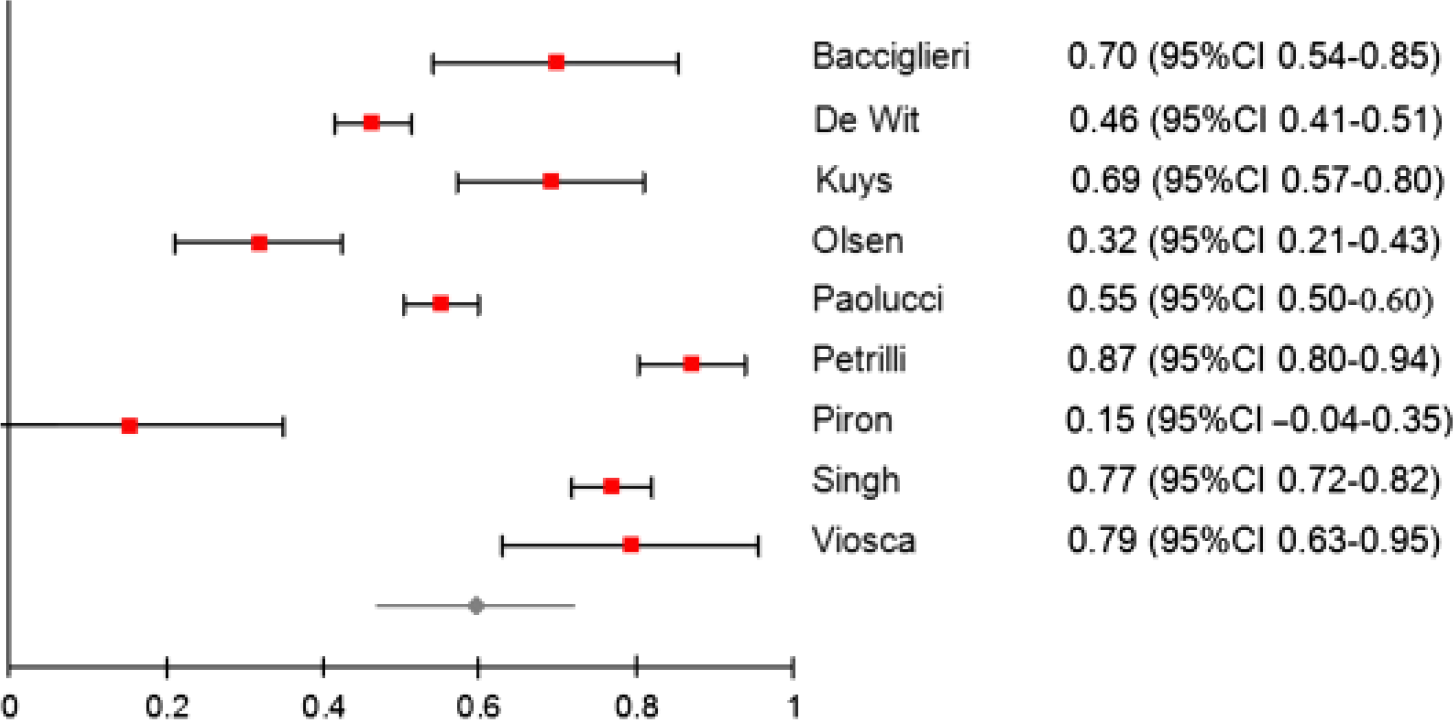
Probability (95% CI) of patients after stroke who are initially nonambulatory regaining independent walking at three-months when managed in a rehabilitation unit by pooling data from nine studies (n=1373).
At six-months, the probability of initially nonambulatory stroke survivors regaining independent walking was examined by pooling data from three studies (18, 29, 30) comprising 444 participants (Fig. 4). The probability of independent walking had increased to 0·65 (95% CI 0·53–0·77).
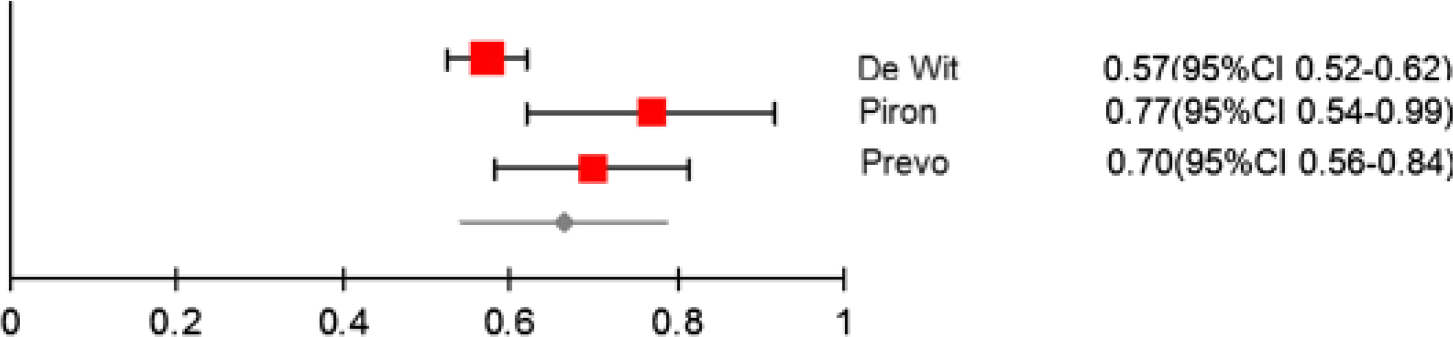
Probability (95% CI) of patients after stroke who are initially nonambulatory regaining independent walking at six-months when managed in a rehabilitation unit by pooling data from three studies (n=444).
At 12 months, the probability of initially nonambulatory stroke survivors regaining independent walking was examined by using data from one study (35) comprising 24 participants. The probability of independent walking had increased to 0·91 (95% CI 0·81–1·00). Data were unavailable from one study.
Acute unit
At three-months, the probability of initially nonambulatory stroke survivors regaining independent walking was examined by pooling data from five studies (2, 19, 20, 36, 38) comprising 634 participants (Fig. 5). The probability of independent walking in initially nonambulatory stroke patients was 0·39 (95% CI 0·27–0·52). Data were unavailable from four studies.
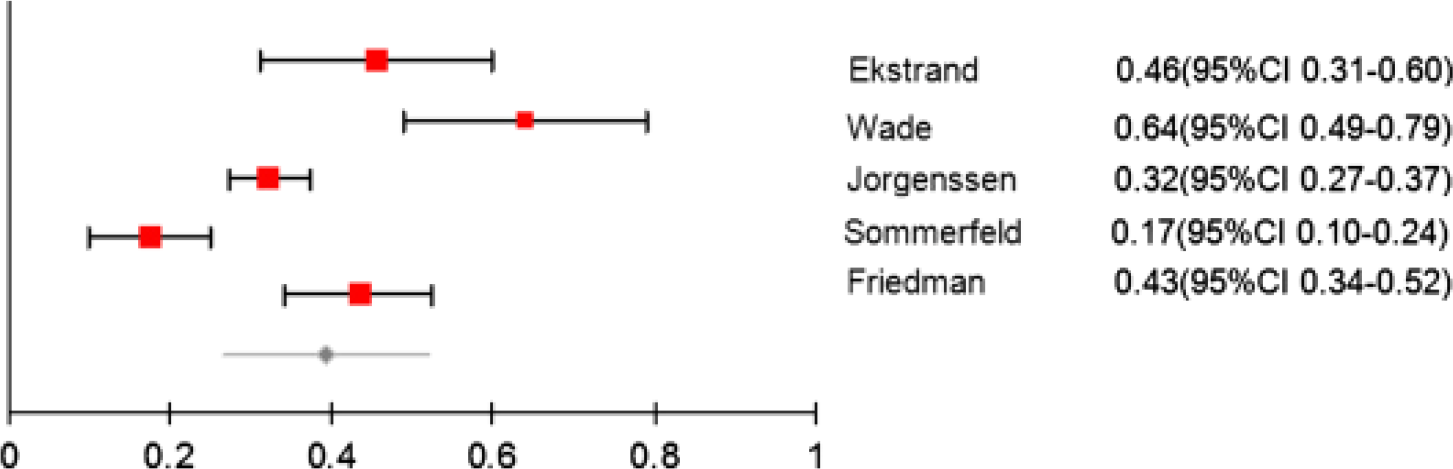
Probability (95% CI) of patients after stroke who are initially nonambulatory regaining independent walking at three-months when managed in an acute unit by pooling data from five studies (n=634).
At six-months, the probability of initially nonambulatory stroke survivors regaining independent walking was examined by pooling data from two studies (19, 31) comprising 405 participants (Fig. 6). The probability of independent walking had increased to 0·69 (95% CI 0·46–0·92). Data were unavailable from two studies.

Probability (95% CI) of patients after stroke who are initially nonambulatory regaining independent walking at six-months when managed in an acute unit by pooling data from two studies (n=405).
At 12 months, the probability of initially nonambulatory stroke survivors regaining independent walking was examined by using data from one study (24), comprising 34 participants. The probability of independent walking had increased to 0·74 (95% CI 0·59–0·88).
Discussion
This is the first systematic review to pool data from prospective, consecutive studies of patients who are nonambulatory in the first month after stroke to determine the probability of regaining independent walking. A meta-analysis of available data found that 60% of initially nonambulatory stroke patients managed in a rehabilitation unit regained independent walking at three-months and this increased to 65% by six-months after stroke. This differed from the findings for patients managed in an acute unit – at three-months only 39% of initially nonambulatory stroke patients in an acute unit regain independent walking. However, at six-months after stroke, a similar proportion of patients managed in an acute unit (69%) regained independent walking to those managed in a rehabilitation unit (Fig. 7).
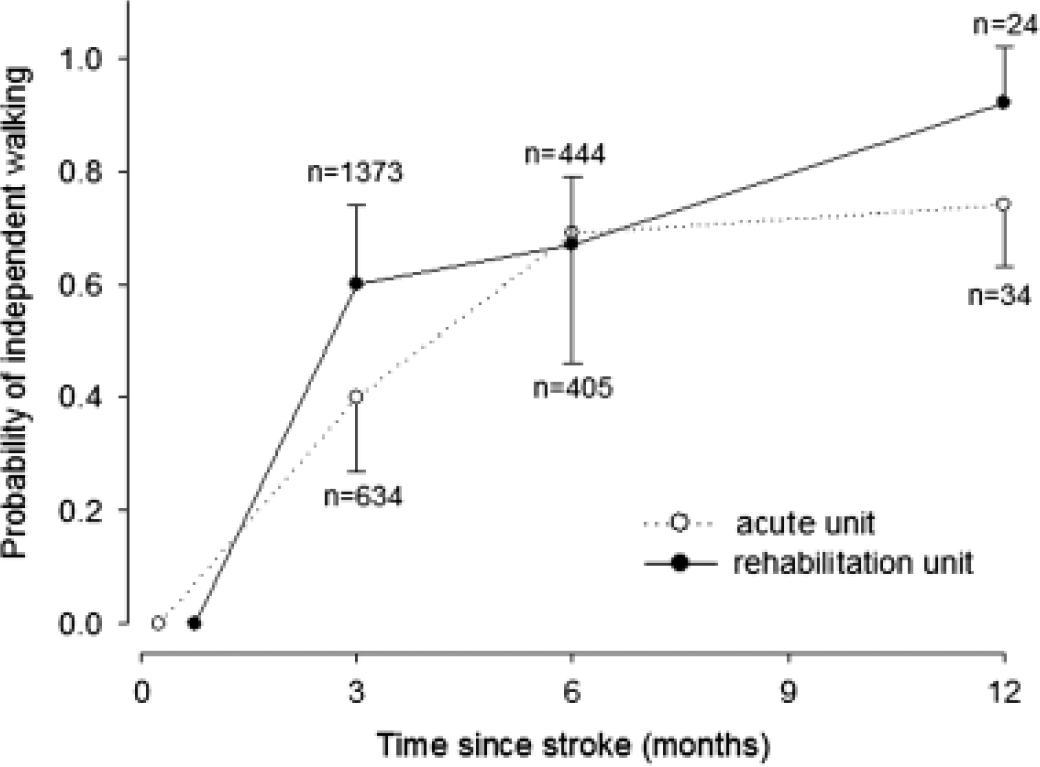
The probability of patients after stroke who are initially nonambulatory regaining independent walking when managed in a rehabilitation unit (closed circles) and an acute unit (open circles).
The overall quality of the included studies was good. The age and gender of participants was similar across the studies, as were the inclusion criteria to enter the studies. There were 15 studies that included participants managed in a rehabilitation setting, and 11 that included participants managed in an acute setting, which included both general acute units and designated stroke units. Initial measures of walking occurred earlier on average in acute units (six-days) than in rehabilitation units (19 days). A variety of measures of walking were used across the included studies, and not all studies defined independent walking. However, of the studies that did, all but one study defined independent walking as the ability to walk without human assistance. There were sufficient data for a meta-analysis to be included at three- and six-months for rehabilitation units and acute units. The number of participants included was 1373 in the rehabilitation unit meta-analysis and 634 in the acute unit meta-analysis at three-months. The good quality and similarity of the studies, as well as the number of participants available for the three-month meta-analyses, suggests that the results for the probability of regaining independent walking at three-months after stroke in patients who are initially nonambulatory are credible. Although there were data available for analysis at six- and 12 months in both settings, the number of participants is too small to draw valid conclusions.
A substantially greater proportion of patients managed in a rehabilitation unit regained independent walking at three-months compared with those managed in an acute unit. There are several possible explanations for this outcome. Patients admitted to a rehabilitation unit have generally been selected as being likely to benefit from a prolonged period of rehabilitation, thus increasing the probability of this population regaining independent walking, compared with an unselected population of patients managed in an acute unit after stroke. Patients admitted to an acute unit after stroke can include those with severe stroke, including those with significant physical and cognitive impairment. The severity of impairments in these patients would also contribute to a reduced probability of regaining independent walking for patients managed in an acute unit. Moreover, the outcome of stroke is associated with intensity of therapy (39) and rehabilitation units are designed and resourced to provide a greater intensity of therapy than acute units, thus increasing the probability of improved walking outcomes in these patients.
There was variability in the number of days after stroke that the initial measure of walking was completed across studies. The correlation between the average day the participants were measured as nonambulatory and the probability of walking independently at three-months was high in both a rehabilitation unit (r=0·88; P=0·002) and an acute unit (r=0·70; P=0·19). This is not surprising given there is the potential for substantial recovery in walking ability in the first month after stroke (40), and a patient who is still nonambulatory 30 days after stroke is likely to have had a devastating stroke, which is not necessarily the case in patients who are nonambulatory at only three-days after stroke. Therefore, we carried out a post hoc regression analysis taking into account the number of days after stroke that measurement of nonambulatory status occurred. The prediction equation for determining the probability of independent walking at three-months in patients who are nonambulatory in the first month after stroke in a rehabilitation unit is:
probability of walking=1·24–(0·034 × day after stroke measured as nonambulatory)
For an acute unit the prediction equation is:
probability of walking=0·66–(0·04 × day after stroke measured as nonambulatory)
For example, in a rehabilitation unit a patient who is measured as nonambulatory 14 days after stroke has a 76% chance of walking independently at three-months [0·76=1·24–(0·034 × 14)], compared with a patient in an acute unit who is measured as nonambulatory 14 days after stroke who has a 10% chance of walking independently at three-months [0·1=0·66–(0·04 × 14)]. These equations can be used to refine the prediction of probability of individual patients regaining independent walking at three-months after stroke. This more accurate information could be utilized to allocate resources amongst individual patients, as well as to facilitate decisions about discharge destination. It also provides clinical services with a benchmark for evaluating the effectiveness of service provision for patients who are initially nonambulatory after stroke and can also be used as a guide to educate patients and carers of the probability of regaining independent walking. Moreover, these equations can be utilized in clinical research as a benchmark for the performance of control groups in trials examining walking outcome after stroke. For instance in two recent randomized trials examining the effectiveness of treadmill training in nonambulatory participants (41, 42), the outcome of the control group in both studies was consistent with the proportion of independent walkers predicted by the equation, suggesting that the control groups in both studies achieved a reasonable outcome in terms of walking independence.
There are several limitations of this review. Firstly, data were unable to be extracted from nine studies, thus reducing the power of the results. There were substantially more data available for the meta-analyses of walking outcome at three-months than at any other time point, and only two studies had data available for analysis at 12 months after stroke, suggesting that the findings at six- and 12 months in both settings are less robust than the findings at three-months after stroke. Secondly, in line with best practice (43), inclusion in this systematic review required studies to be consecutive with inception cohorts, consequently randomized trials were not screened. However, it has been suggested that the control groups in randomized trials may provide ‘hidden’ information about probability of outcomes (43). As a result, some potentially relevant data may have been excluded from the analysis.
In conclusion, this systematic review found that in a rehabilitation unit, the probability of regaining independent walking for patients who are nonambulatory in the first month after stroke is 60% at three-months. The probability of regaining walking is lower for patients managed in an acute unit at only 39% by three-months. The prediction may be refined by using the time in the first month after stroke that the patient remains nonambulatory, to predict walking outcome at three-months for individual patients in both rehabilitation and acute settings. This information may be used clinically to make decisions about allocation of rehabilitation resources, education of patients and carers, and for discharge planning.
Footnotes
Acknowledgements
We would like to thank Dr Liesbet De Wit, Ms Elisabeth Ekstrand, Dr Cesar Minelli, Dr John Reid, Dr Disa Sommerfeld and Dr Jon Ween for providing additional information for the meta-analyses. We would also like to thank Ms Irmina Nahon, Mrs Helen Preston and Mr Nicholas Stanton for their time and skill in translating papers into English.