
Abstract
Background and aims
Comparing safety and technical success of balloon-expandable stents and self-expanding stents for intracranial angioplasty and stenting in medically refractory intracranial atherosclerotic disease in a single center series.
Methods
Fifty-four self-expanding stents and 46 balloon-expandable stents were implanted in 100 consecutive patients (mean age 64 years, 74% male) from April 2000 to September 2009. All patients had symptomatic intracranial stenosis (anterior circulation, n = 40; posterior circulation, n = 60), presenting with recurrent transient ischemic attack or stroke under antithrombotic treatment. Mean degree of stenosis before treatment was 83 ± 13%.
We assessed safety, defined as any stroke or death during the procedure and at 30 days follow-up, and technical success, defined as accurate delivery of the stent at the site of the target lesion.
Results Safety
– periprocedural stroke or hemorrhage occurred in 11 patients treated with balloon-expandable stent, and in 14 of the patients treated with a self-expanding stent. One patient with a balloon-expandable stent died because of acute vessel rupture during treatment. One balloon-expandable stent and one self-expanding stent patient developed a severe reperfusion hemorrhage that resulted in death. Overall, the combined stroke and death rate at 30-day follow-up was 250% (23·9% for balloon-expandable stent group and 25·9% for the self-expanding stent group, P = 0·84). Technical success – intracranial angioplasty and stenting was technically successful in 96·3% of the self-expanding stent and 89·1% of the balloon-expandable stent patients (P = 0·31). Vascular complications were significantly less frequent in patients treated with a self-expanding stent (11·1%) than with a balloon-expandable stent (36·9%, P = 0002).
Conclusion
Despite a high technical success, the rate of clinical adverse events at 30 days after intracranial angioplasty and stenting is high independently of the stent design. Thus, further development of intracranial stent systems and careful patient selection are mandatory.
Keywords
Introduction
Intracranial atherosclerotic disease (ICAD) accounts for 10 to 29% of ischemic events (1,2). Patients with these lesions are at high risk for stroke even under best medical treatment (3). With the improvement of endovascular procedures and the development of new stent devices, intracranial angioplasty and stenting (ICAS) has increasingly become an alternative treatment option in patients with symptomatic ICAD. The first stents used for IACS were balloon expandable stents (BES), primarily designed for coronary interventions (4–6). A major concern of these relatively stiff devices has been accessibility and safety in the tortuous intracranial vasculature. Subsequently, new concepts for stent-assisted procedures in the intracranial vasculature with more flexible BES or self-expanding stents (SES) particularly designed for intracranial lesions have been introduced (7–11). Yet, results from single center series, trials, and registries show a wide range of periprocedural complications with stroke and death rates at 30 days after IACS in up to 36% (12).
Here, we compared safety and technical success of BES with SES in 100 consecutive patients undergoing ICAS for symptomatic stenosis of the intracranial circulation at our institution.
Patients and methods
Study design
We analyzed our prospective database of clinical and angiographic records of 100 consecutive patients undergoing ICAS for the treatment of symptomatic intracranial stenosis. The study was approved by the local ethics committee.
BES systems
Conventional, balloon-mounted ‘coronary’ stents (AVE, Medtronic, Minneapolis, MN) were used in 35 patients prior to approval of dedicated stents for the intracranial vessels. Subsequently, the Neurolink stent (Guidant, Menlo Park, CA), a balloon-mounted stent specifically designed for the treatment of intracranial arteriosclerotic stenosis, was available and implanted in 11 patients.
SES systems
The Neuroform stent system (Boston Scientific, Fremont, CA), primarily developed for the stent-assisted endovascular treatment of wide-necked aneurysms, was used in five patients, and after approval, the Wingspan Stent System (Boston Scientific), a self-expanding nitinol stent for the treatment of intracranial stenoses, was applied in 49 individuals.
Indication for ICAS were arteriosclerotic stenosis >50% of an intradural vessel as shown on digital subtraction angiography and failure of antithrombotic therapy, defined as the occurrence of one or more transient ischemic attacks (TIAs) and/or stroke in the territory of the narrowed artery while taking therapeutic doses of dual antiplatelet therapy or oral anticoagulation. Patients with acute vessel occlusions were excluded from this analysis. In all cases, an interdisciplinary conference of interventional neuroradiologists and neurologists met the indication for ICAS on consensus.
Clinical and procedural data were analyzed with regard to the following criteria:
safety = any stroke or death during/after the procedure and at 30-day follow-up
technical success = accurate delivery and deployment of the stent (in all intended stenting procedures), covering the target lesion completely and resulting in a residual stenosis of less than 50%.
Angiographic series and records as well as postinterventional computed tomography (CT) and magnetic resonance imaging (MRI) were evaluated by two experienced interventional neuroradiologists (S. R.; M. H.) with regard to the degree of stenosis, the localization of the lesion, its morphology according to Mori (13), and procedure-related vascular complications, for example, major dissection, symptomatic vasospasm, thrombosis of the treated segment (requiring further treatment), and vessel perforation/rupture. Mori's classification of intracranial arteriosclerotic lesions includes morphological information (e.g. length/degree of stenosis, contour, angulations, calcifications, age) as well as information about the tortuosity of the proximal segment and the accessibility of the lesion (13):
type A lesions are defined as short (<5 mm), nonangulated, and smooth lesions with a 70–90% stenosis, readily accessible
type B lesions are defined as a five-millimeters to 10 mm long, irregular, ≥90% stenosis with calcification, moderate angulation, and tortuosity of the proximal segment
type C lesions are long-segment, high-grade lesions (greater than one-centimeter) with extreme angulations and excessive tortuosity of the proximal segment.
The neurological status was documented by a stroke neurologist according to the National Institute of Health Stroke Scale (NIHSS) score before ICAS and on days one and 30 after the intervention. A TIA was defined as neurological worsening with complete recovery within 24 h after the intervention. Minor and major stroke was defined as persistent worsening of the NIHSS score of <4 or ≥4 points, respectively.
Patients
From April 2000 to September 2009, a total of 100 patients with symptomatic atherosclerotic intracranial stenosis were treated with ICAS. Mean age of the patients was 63 ± 9 years (range, 41–80 years): 74 patients were male. All individuals were selected for ICAS because of recurrent TIA (n = 34) or stroke (n = 66) under combined antithrombotic treatment (n = 99) or oral anticoagulation (international normalized ratio 2·0–3·0, n = 1). A detailed overview about baseline characteristics is given in Table 1.
Gender, characteristics of the target lesion and clinical data of 100 patients who underwent ICAS for symptomatic intracranial stenosis
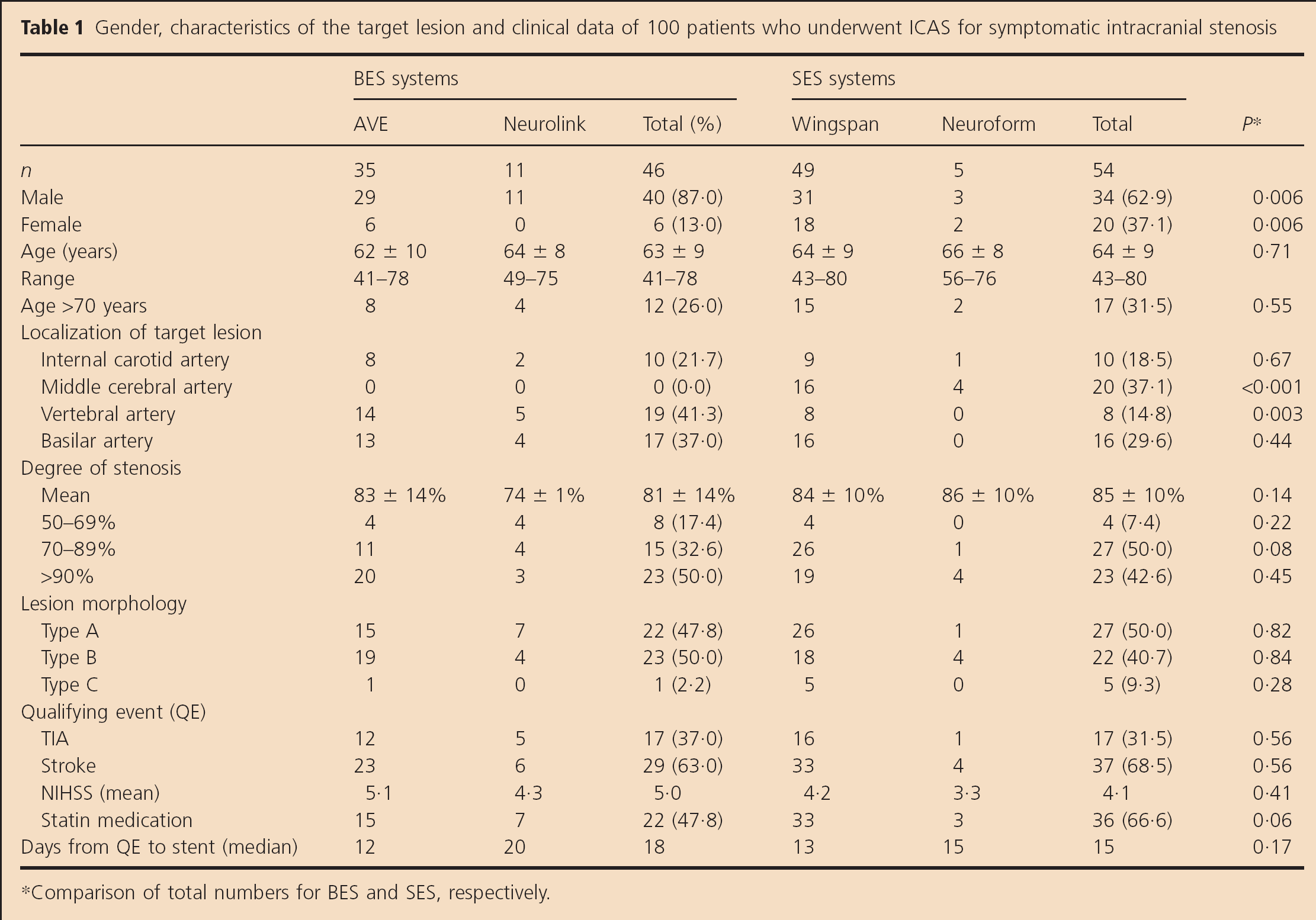
Comparison of total numbers for BES and SES, respectively.
Target vessel lesions were located in the anterior circulation in 40 patients and in the posterior circulation in 60 individuals. Mean stenosis before treatment as determined according to the Warfarin-Aspirin Symptomatic Intracranial Disease criteria (14) was 83 ± 13% (range, 50–99%). Each patient received clopidogrel [75 mg per os (PO) for three-days before the procedure or 300 mg PO on the day before treatment] and aspirin (100–300 mg PO); double antiplatelet therapy was continued at least for six-months until control angiogram or MRI was performed to exclude restenosis.
Stenting procedure description
All procedures were performed by experienced interventional neuroradiologists (M. H., S. H.) in a biplane neurovascular angiosuite (Integris, Philips Medical Systems, Eindhoven, the Netherlands) under general anesthesia. All patients gave written informed consent.
A unilateral femoral approach was used after intraarterial standard puncture and a 6-F guiding catheter was placed in the high cervical portion of the artery to be treated. During the intervention, anticoagulation was achieved by intravenous bolus injection of 4000–10 000 IU unfractionated heparin at the beginning of the intervention and repeated boosters of 1000–2000 IU heparin hourly during the procedure according to ACT results.
BES procedure
In case of a tight stenosis, predilatation was performed with a 2·0 to 2·5-mm balloon catheter (Hayhate, Terumo, Tokyo, Japan) with a pressure of six-atmospheres. The balloon-expandable AVE stent and the Neurolink stent were deployed and expanded by slowly inflating the balloon of the delivery system to the nominal parent vessel diameter.
SES procedure
Prior to stent placement, balloon angioplasty was performed in all patients. A microcatheter was used to cross the lesion over a microguide wire (0·014′) and placed distal to the lesion. Subsequently, an exchange-length floppy tip microwire (0·014′) was placed across the lesion, and the microcatheter was removed. Over the exchange microwire, the balloon was introduced and centered across the lesion. In case of the Neuroform stent system, the stenotic lesion was predilated with a Hayate pro-balloon dilation catheter (Terumo; n = 1) or the Maverick balloon dilation catheter (Boston scientific, Maple Grove, MN; n = 4). When using the Wingspan Stent System (Boston Scientific Corp.), predilation was performed with the Gateway balloon catheter. Balloons were slightly undersized and slowly inflated over 60 to 120 s at six-atmosphere pressure. After removal of the balloon, the SES system was introduced and centered across the lesion. Stent size selection was based on the original diameter of the target vessel and length of the stenotic lesion.
Additional balloon angioplasty after stent placement was performed in two patients only (Neuroform, n = 1; Wingspan n = 1), in whom angiographic control showed residual stenosis of more than 50%.
Statistical analysis
Mean values, median, and standard deviation were used for descriptive statistics; statistical analysis was performed with Microsoft Excel (Professional Edition 2003, Microsoft Corporation, Redmond, WA, USA). The t-test was applied to determine significant levels between parametric data before and after treatment. The chi-square test was used to evaluate non-parametric data. The relative risk (RR) was calculated to describe the impact of clinical and vascular risk factors on the probability to encounter a clinical adverse event. A probability of >95% was considered significant (P < 0·05).
Results
Safety
Overall, the combined stroke and death rate at 30-day-follow-up after ICAS was 25% without difference in patients treated with a BES (23·9%) or with a SES (25·9%, P = 0·84). Detailed information about the distribution of clinical adverse events is given in Table 2. Periprocedural stroke or hemorrhage occurred in 11 patients treated with BES, and in 14 of the patients treated with a SES. Fourteen patients suffered a major ischemic stroke in the treated territory [BA, n = 8, vertebral artery (VA), n = 1; ICA/MCA, n = 5] and six patients developed intracranial hemorrhage [BA/VA, n = 2; internal carotid artery (ICA)/middle cerebral artery (MCA), n = 4]; five patients had a minor stroke (BA, n = 3; VA, n = 2). Six additional patients had transitory ischemic attacks after the intervention (BA/VA, n = 3; ICA/MCA, n = 3). There were three procedure-related deaths (BES; n = 2; SES, n = 1): one patient died after rupture of the basilar artery during stent placement with a BES, and two patients died due to severe reperfusion hemorrhage.
Safety data: clinical events and 30-day stroke and death rate after ICAS in 100 patients
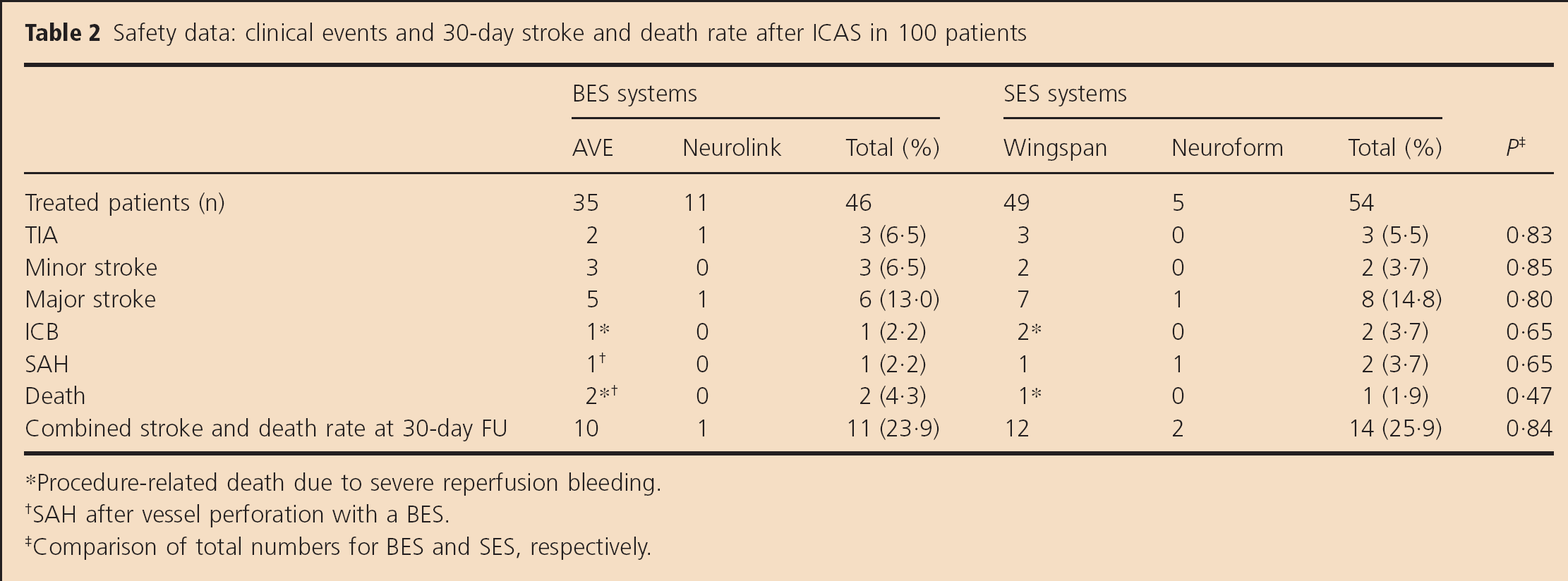
Procedure-related death due to severe reperfusion bleeding.
SAH after vessel perforation with a BES.
Comparison of total numbers for BES and SES, respectively.
Analysis of risk factors
Although not statistically significant, the RR to encounter a clinical adverse event during or after ICAS showed a strong trend for patients with complex lesions type C (compared with lesions type A or B; RR 2·9 (95% confidence interval 1·5–5·6); P = 0·06) and high-grade stenoses ≥70% (compared with patients with lesions <70%; RR 2·8 (0·4–18·5); P = 0·40), for patients who had a stroke as qualifying event (QE; compared with TIA, RR 1·6 (0·7–3·7); P = 0·22), and for patients who underwent ICAS early (≤ 10 days) after the QE (compared with a time interval >10 days; RR 1·4 (0·7–2·8); P = 0·36). Gender, age, lesion site, and number of vascular risk factors had no relevant impact on the frequency of clinical events (Table 3).
Analysis of risk factors: baseline characteristics vs. frequency of clinical events
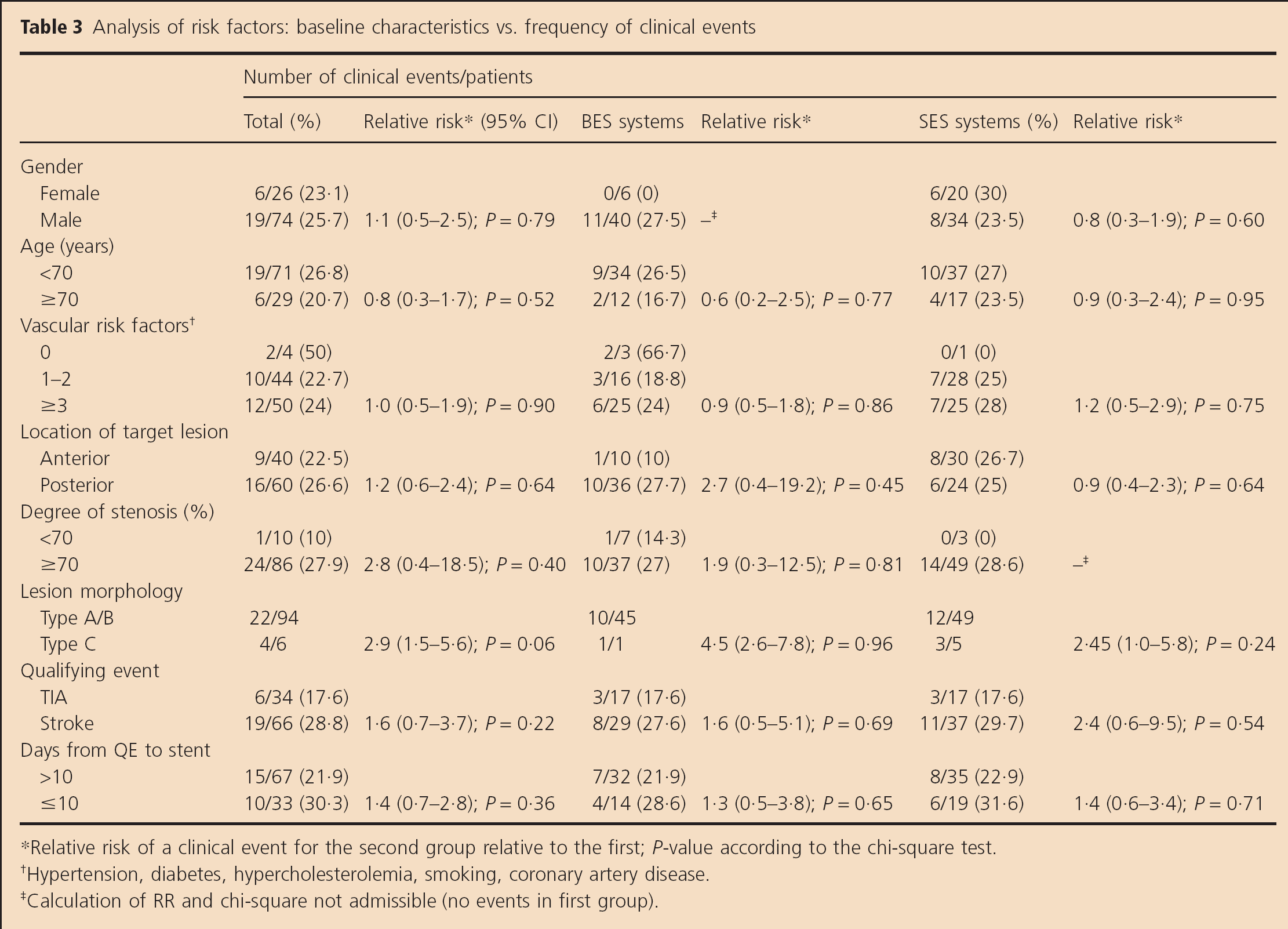
Relative risk of a clinical event for the second group relative to the first; P-value according to the chi-square test.
Hypertension, diabetes, hypercholesterolemia, smoking, coronary artery disease.
Calculation of RR and chi-square not admissible (no events in first group).
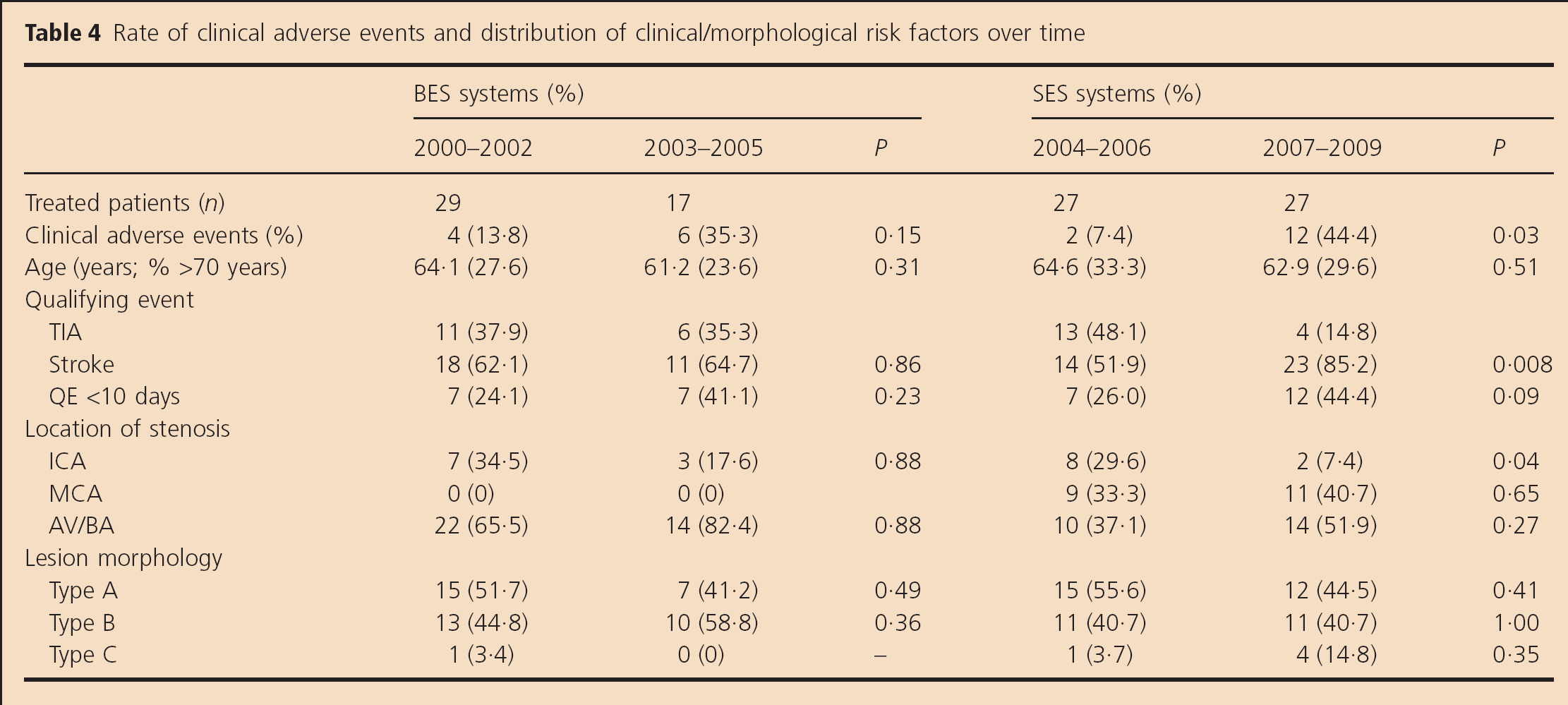
Interestingly, there was an increase of clinical events over time for both groups. While the stroke and death rate was comparably low within the first three-years of each group, it increased within the second half of the time period (BES: 13·8% to 37·5%, P = 0·153; and SES: 11% to 45·2%, P = 0·033). Dynamic analysis of clinical and morphological risk factors over the time revealed an increase of patients with recent stroke as QE, of patients with complex and high-grade type C lesions, and of lesions in the middle cerebral artery for the SES group (Table 4).
Rate of clinical adverse events and distribution of clinical/morphological risk factors over time
Technical success
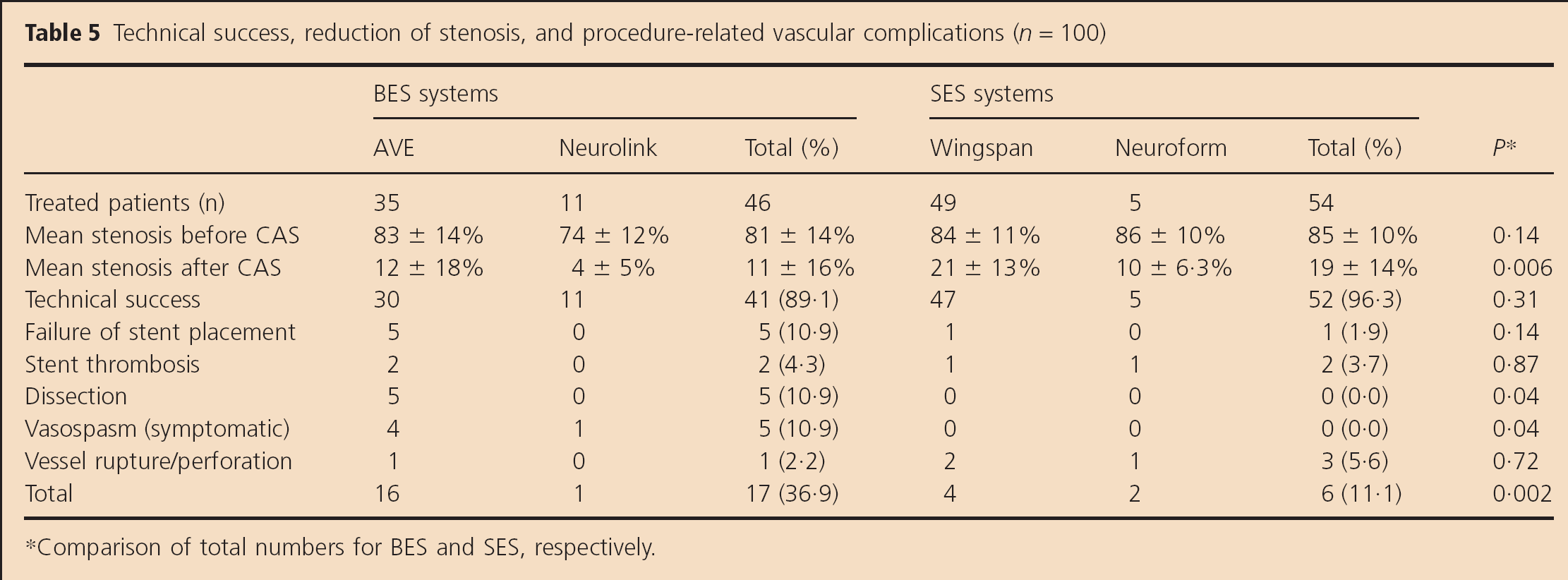
Accurate delivery and deployment of the stent and successful reduction of the degree of stenosis (<50%) was achieved in 94%. Success rates were not higher in patients treated with an SES system than for those treated with a BES (96·3% vs. 89·1%; P = 0·31). Mean residual stenosis of the target lesion after was 14·4 ± 13·9% (range, 0–48%) after successful stent placement. Mean residual stenosis after ICAS was less severe in the BES group (8·5 ± 10·1% (0·40%)) than in the SES group (19·3 ± 14·3% (0–48%); P = 0·006). Table 5 gives detailed information about device related technical success data and procedure related complications.
Technical success, reduction of stenosis, and procedure-related vascular complications (n = 100)
Comparison of total numbers for BES and SES, respectively.
Vascular complications were significantly more frequent in patients who were treated with a BES than in those treated with an SES (36·9% vs. 11·1%; P = 0·002). In the BES group, five patients developed symptomatic vasospasm (BA, n = 2; VA, n = 3) and five patients had a dissection (BA, n = 1, VA, n = 3, ICA, n = 1). There were no events of vasospasm, and only one minor dissection after predilation in the SES group that could be flattened after stent placement. However, there were two cases of (delayed) in-stent thrombosis (both MCA) and three cases of wire perforation after IACS with a SES (MCA, n = 2; VA, n = 1). A detailed overview about device-related safety data with regard to the different stent systems is given in Table 2.
In four patients in whom placement of a BES was intended, the lesion could not be reached with the device due to a tortuous vessel anatomy (ICA, n = 1; BA, n = 3). In one of these patients with a supraophthalmic ICA stenosis and a tight siphon, the stent slipped off from the balloon. It was possible to retrieve the nondeployed stent with a retriever device and to perform balloon angioplasty afterwards. In the remaining three patients, neither stent placement nor balloon angioplasty of the target lesion was technically possible. In another BES patient, a major dissection of the basilar artery occurred immediately after deployment of the stent, leading to severe subarachnoid hemorrhage and acute thrombosis of the stented segment. Several attempts to recanalize the occluded vessel failed, and the patient died within 24 h after the procedure.
In the SES group, stent placement failed in one patient with a tortuous access and a complex stenosis of the supraohthalmic right ICA due to dislodgement of the stent after deployment, resulting in a 50% residual stenosis without dissection. Angiographic controls showed improved blood flow in the affected hemisphere so PTA was not repeated. However, this patient developed a major embolic stroke two-days after the procedure.
Discussion
In this study, we assessed safety and technical success of ICAS for symptomatic intracranial stenosis with BES and SES in a single-center consecutive patient series. The procedure was technically feasible in a high proportion of patients, leading to a significant reduction of the stenosed vessel. Angiographic complications were lower with more flexible SES adapted to the requirements of the cerebral vasculature. However, despite the relatively high success rate, the procedure had a substantial risk for procedure-related stroke and death at 30 days independent of the stent design.
While in the early 1990s, first publications on intracranial angioplasty reported complication rates up to 40% (4–6,15), the reported 30-day stroke and-death rates for patients undergoing ICAS nowadays range between 0% and 28% with a mean risk of perioperative stroke or death of 9·5% according to a systemic review of 79 studies (7–10,16–18).
Kurre et al. reported the acute results of a large multicenter registry with 372 patients who underwent elective intracranial stenting (19): the rate of disabling strokes and deaths was 4·8% and 2·2%, respectively. Additional transient or minor events were detected in 5·4% of the cases. Likewise, Suh et al. reported a 99% success rate and overall 10% adverse event rate in a series of 100 consecutive patients with severe symptomatic intracranial stenosis that were treated with BES. At six-month follow-up, they documented three major strokes, three minor strokes, and three deaths (16).
In comparison, the overall 30-day stroke and death rate of 25% in our own study is notably high, putting the risk-benefit ratio for IACS into a more unfavorable light. Interestingly, the rate of clinical events after IACS did not differ significantly between stent systems, although procedural angiographic complications were significantly more frequent in the BES group. While the high complication rate of the more rigid balloon-mounted stents is obviously related to the higher rate of technical problems encountered with these devices, the rate of procedure-related complications with SES, especially with the Wingspan Stent System might be explained by a combination of several technical and morphological vascular factors. Moreover, the high rate of strokes in the SES group might be the result of a change toward a more aggressive approach to complex lesions. During the analysis of our data, we noticed that due to the improved flexibility and the low rate of angiographic and clinical complications in our first 27 patients treated with the Wingspan system, the indication for IACS expanded from simple target lesions in the posterior circulation with easy access to more complex lesions in the posterior and the anterior circulation. Thus, the unexpected high rate of clinical adverse events in the SES group might be explained by the increasing proportion of patients with a recent stroke as QE, the higher number of patients with complex type C lesions, and the higher proportion of MCA stenoses (Table 4). The high fraction of individuals with increased procedural risk is illustrated when comparing our SES data with the baseline characteristics of the Wingspan registry (20): while gender, age, and lesion site are comparable, the proportion of patients with high-grade stenoses >70% (91% vs. 81%) and with stroke as QE (69% vs. 59%) was considerably higher in our SES group. A potential source for vascular injury and subsequent complications with the SES is the use of a long exchange wire to introduce the stent after balloon angioplasty: vessel perforations with subsequent subarachnoid hemorrhage were noted in three SES patients; this complication was absent in patients treated with the BES models.
The high rate of clinical adverse events in our study is supported by a recent publication from Costalat et al., who reported an overall of 21·4% procedural complications after treatment of symptomatic intracranial stenosis with isolated angioplasty, balloon-expandable coronary stents, and the Wingspan Stent System (18). In the Wingspan group, the authors observed six major procedural complications (31·6%), including one case of subarachnoid hemorrhage after stent deployment, one case of delayed in-stent thrombosis, one embolic occlusion of the PCA, and three occlusions of brain stem perforators. These results are in line with the most recent communication from the stenting and aggressive medical management for preventing recurrent stroke in intracranial stenosis (SAMMPRIS) trial that reported a 14% death and stroke rate at 30-day follow-up in the stenting arm. Due to these findings, enrolment to the SAMMPRIS trial has been stopped in April 2011 (21).
Nahab et al. analyzed risk factors associated with major cerebrovascular complications after intracranial stenting in 160 patients that underwent ICAS with the Wingspan Stent System (22). The authors found that lesions in the posterior circulation, stenting soon after a QE, stroke as a QE, and a low number of treated patients (low-volume sites) were correlated with a higher risk for cerebrovascular complications. Morphological factors were not analyzed in this study. In contrast, we found lesion morphology and degree of stenosis to be the most important predictors of a clinical adverse event during or after ICAS (Table 3). However, similar to the results of Nahab et al., the RR for neurological complications was moderately elevated for patients with stroke as the QE than for those with TIA and in patients who underwent ICAS soon after the QE. Interestingly, we did not find a relevant correlation for the site of the lesion (anterior circulation, 22·5% vs. posterior circulation, 26·5%; RR 1·2).
This study has several technical and systematic limitations that might explain in parts the surprising results especially for the SES group. As stated earlier, it is very probable that there has been a change in patient selection, which is difficult to verify within a retrospective analysis. Moreover, changes in technical approaches, learning curves, and the relatively low number of cases per year might have influenced in part the results of this study. On the other hand, this series of patients might represent clinical reality as all patients who underwent ICAS were reviewed without further selection criteria.
In conclusion, despite a high technical success rate, ICAS is associated with a substantial risk for stroke and death at 30 days independent of the stent design. The procedural risk is related to the angiographic access and lesion morphology. New and less traumatic stent devices may lower the procedure related complication rate.
Footnotes
Acknowledgements
We thank all participating physicians, nurses, and neuroradiological technicians for their constant effort in this study.