
Abstract
Background
The current European license for alteplase in acute ischemic stroke excludes from treatment large groups of patients. Nevertheless, in everyday practice, many patients receive off-label thrombolysis at the physician's discretion.
Aim
Our aim was to evaluate safety and effectiveness of intravenous alteplase in patients not fully adhering to the drug license compared with those treated strictly according to the license in Central and Eastern Europe.
Methods
We analyzed the data contributed to Safe Implementation of Thrombolysis in Stroke registry from nine countries between February 2003 and February 2010. Statistical analysis included multivariate logistic regression.
Results
Of 5594 consecutive patients, 1919 patients (34·3%) not fully adhered to the license. The most frequent deviations were: time-to-treatment >3 h (13·1%), use of intravenous antihypertensives (8·3%), age >80 years (7·3%), oral anticoagulation (4·2%), a previous stroke with concomitant diabetes (3·9%), and previous stroke <three-months (2·7%). The off-label group showed a significantly higher rate of symptomatic intracranial haemorrhage, which was not confirmed in the multivariate analysis. License nonadherence significantly increased the risk of death or dependency (odds ratio 1·26; 95% confidence interval: 1·08–1·48), with a trend for increased mortality (odds ratio 1·17; 95% confidence interval: 0·97–1·42). Isolated time-to-treatment >3 h was an independent predictor of unfavorable outcome (odds ratio 1·32; 95% confidence interval: 1·01–1·71).
Conclusion
Our findings show that patients not fully adhering to the European license are not at increased risk of symptomatic intracranial haemorrhage but achieve less favorable outcome. Some contraindications appear more redundant than others. However, the final conclusions about safety and effectiveness should be based on the results of ongoing randomized trials.
Introduction
Thrombolytic treatment with recombinant tissue plasminogen activator (rt-PA, alteplase) is currently administered to approximately 5% of all ischemic stroke patients and up to 20% in thrombolysis-oriented centers (1,2). Such low proportion may be because of organizational issues and also numerous contraindications listed in the European drug license (3). Nonetheless, in everyday practice, some patients receive off-label thrombolysis according to the clinical judgment of the attending physician (2,45). Treatment between 3 and 4·5 h from the stroke onset has already been proved safe and effective (6,7). There is also a growing body of evidence supporting thrombolysis in the elderly (8,–11). However, still little is known about treatment outcome in other groups of patients not fully adhering to the current drug license. Besides, the management of preexisting comorbidities and peristroke care in Central and Eastern Europe is still less effective than in the Western countries. Therefore, to obtain accurate and reliable estimates, we should prefer direct analyses for the region instead of extrapolating the Western findings.
Our aim was to evaluate the safety and effectiveness of intravenous rt-PA in patients treated outside the European drug license in Central and Eastern Europe.
Materials and methods
The original European labeling was reflected in Safe Implementation of Thrombolysis in Stroke-Monitoring Study (SITS-MOST) inclusion/exclusion criteria (3). SITS-MOST was based on the platform of the Safe Implementation of Thrombolysis in Stroke – International Registry of Thrombolysis in Stroke (SITS-ISTR). Although SITS-MOST addressed only the European Union member countries by 2003, cases of thrombolysis have been reported to the SITS-ISTR by many Central and Eastern European stroke centers. Our study is based on the data of all patients contributed to the registry by nine SITS-EAST participating countries (Croatia, Czech Republic, Estonia, Hungary, Lithuania, Poland, Slovakia, Slovenia, and Turkey) between February 28, 2003 and February 28, 2010. The methodology of SITS registry has been described in details elsewhere (12).
Data were acquired with the approval of the SITS-EAST Steering Committee and the international coordinator, checked for internal validity, and processed for statistical analysis.
According to all relevant variables reported in the registry, patients defined as treated outside the European license fulfilled at least one of the following: age >80 years, onset of symptoms >3 h before administration of rt-PA, use of oral anticoagulants, previous stroke within three months, a history of previous stroke and concomitant diabetes, treatment with unfractioned heparins, use of intravenous antihypertensives before thrombolysis, systolic blood pressure >185 mmHg or diastolic blood pressure >110 mmHg despite antihypertensive treatment, stroke severity >25 points in the National Institute of Health Stroke Scale (NIHSS), and blood glucose concentration <2·8 or >22·2 mmol/l.
Our end points were: symptomatic intracranial haemorrhage (sICH), three-month mortality, and unfavorable outcome (disability or death, modified Rankin Scale score (mRS) 3–6). We distinguished between sICH definitions according to SITS (12) and European Cooperative Acute Stroke Study (ECASS) (13), described in detail later on.
Statistical analysis
Comparative analyses were planned for the off-label patients as a whole and in subgroups. To minimize the influence of potential confounders, we analyzed particular license deviations only in patients with isolated deviations. In sensitivity analysis, we also evaluated nonadherence to modified protocol, allowing for treatment ≤4·5 h, use of intravenous antihypertensives and oral anticoagulants with INR < 1·7. As the reference, we always used patients fully adhering to the European license.
Proportions were calculated after exclusion of unknown values from the denominator. Continuous variables because of non-normal distribution were presented as medians with interquartile ranges (IQRs) and compared with Mann–Whitney U-tests.
To avoid variable selection caused by spurious correlations, only variables showing a relationship to the outcome (defined as P < 0·10) in the univariate model were included as potential predictors for constructing multivariate models. The final multivariate model for each outcome was identified using an interactive backward stepwise approach and included only independent (P < 0·05) outcome predictors. It was subsequently used to verify the influence of particular variables.
All tests were two sided, and P < 0·05 was considered statistically significant. Calculations were carried out in STATISTICA 8·0 (StatSoft, Inc. 2008, Tulusa, Oklahoma, USA).
Results
In the study period, 5594 cases were entered into the SITS registry in 124 centers. Patients were predominantly male (58·6%), with median age 68 years (IQR: 59–75), median onset-to-treatment time 150 mins (IQR: 125–175), median door-to-needle time 71 mins (IQR: 52–95), and median NIHSS score 12 (IQR: 8–17). Overall three-month mortality was 20·9%, while favorable (mRS 0–2) and excellent (mRS 0–1) outcomes were observed in 51·2% and in 35·7% of cases, respectively. The sICH according to the SITS definition occurred in 1·8% of cases.
We found at least one license deviation in 1919 patients (34·3%), including 371 cases (6·6%) with at least two deviations and 69 cases (1·2%) with at least three deviations. Definite on-label treatment was administered in 3428 (61·3%) patients. Due to incomplete data on license adherence, we were not able to clearly classify the remaining 247 patients.
The most frequent deviations were: onset-to-treatment time >3 h (13·1%), including onset-to-treatment time >4·5 h (2·4%), use of intravenous antihypertensives before rt-PA (8·3%), age >80 years (7·3%), a history of previous stroke and concomitant diabetes (3·9%), oral anticoagulation (3·8%), including cases with INR >l·7 (0·8%), and a previous stroke >3 months (2·7%). Other deviations were infrequent (Table 1).
Deviations from the European license
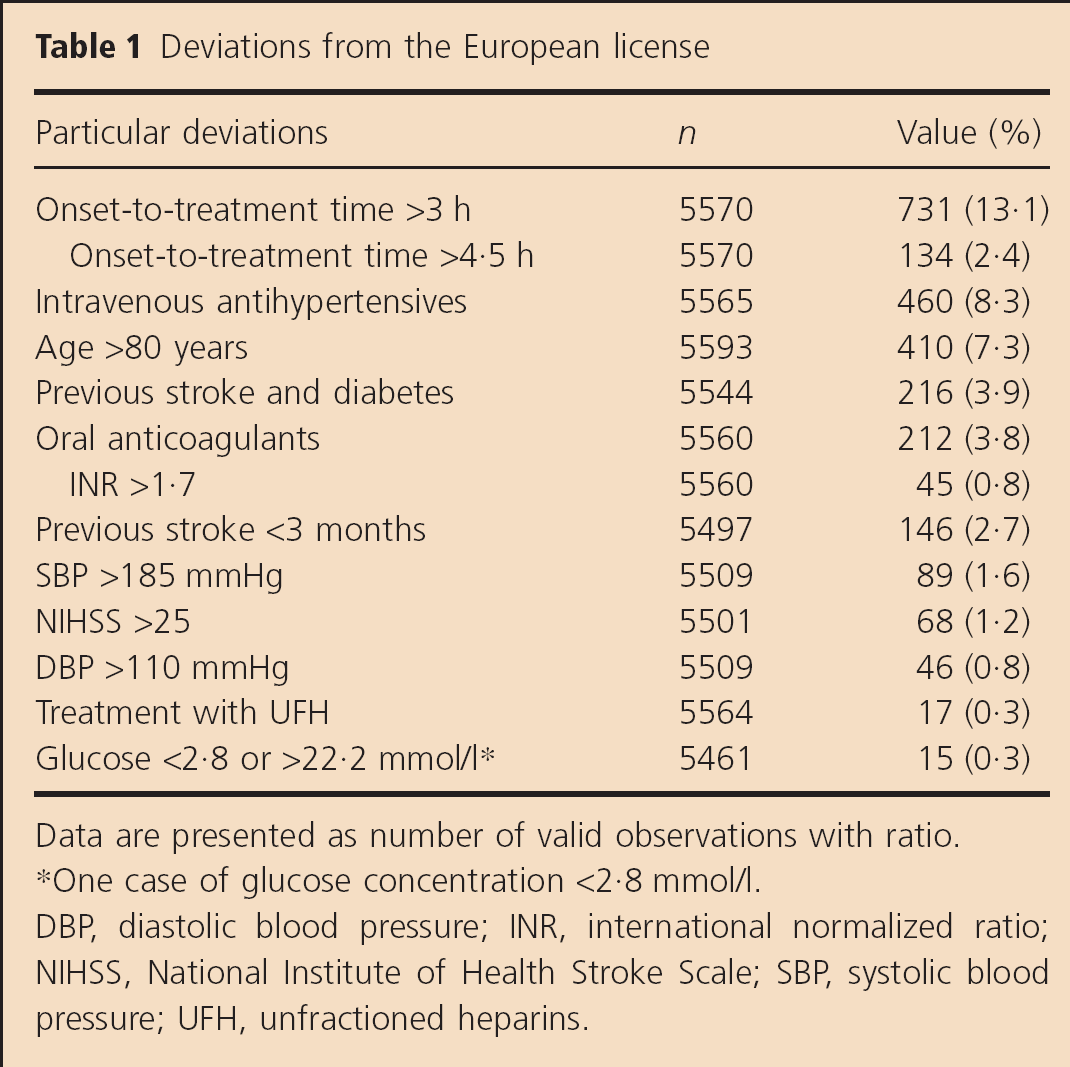
Data are presented as number of valid observations with ratio.
One case of glucose concentration <2·8 mmol/l.
DBP, diastolic blood pressure; INR, international normalized ratio; NIHSS, National Institute of Health Stroke Scale; SBP, systolic blood pressure; UFH, unfractioned heparins.
Patients from the off-label group were significantly older and had a higher proportion of all stroke relevant comorbidities and prestroke disability. Their median delay from onset to treatment was significantly longer, but there were no differences in stroke severity. Detailed comparative characteristics are shown in Table 2.
Baseline characteristics and three-month outcomes according to the license adherence
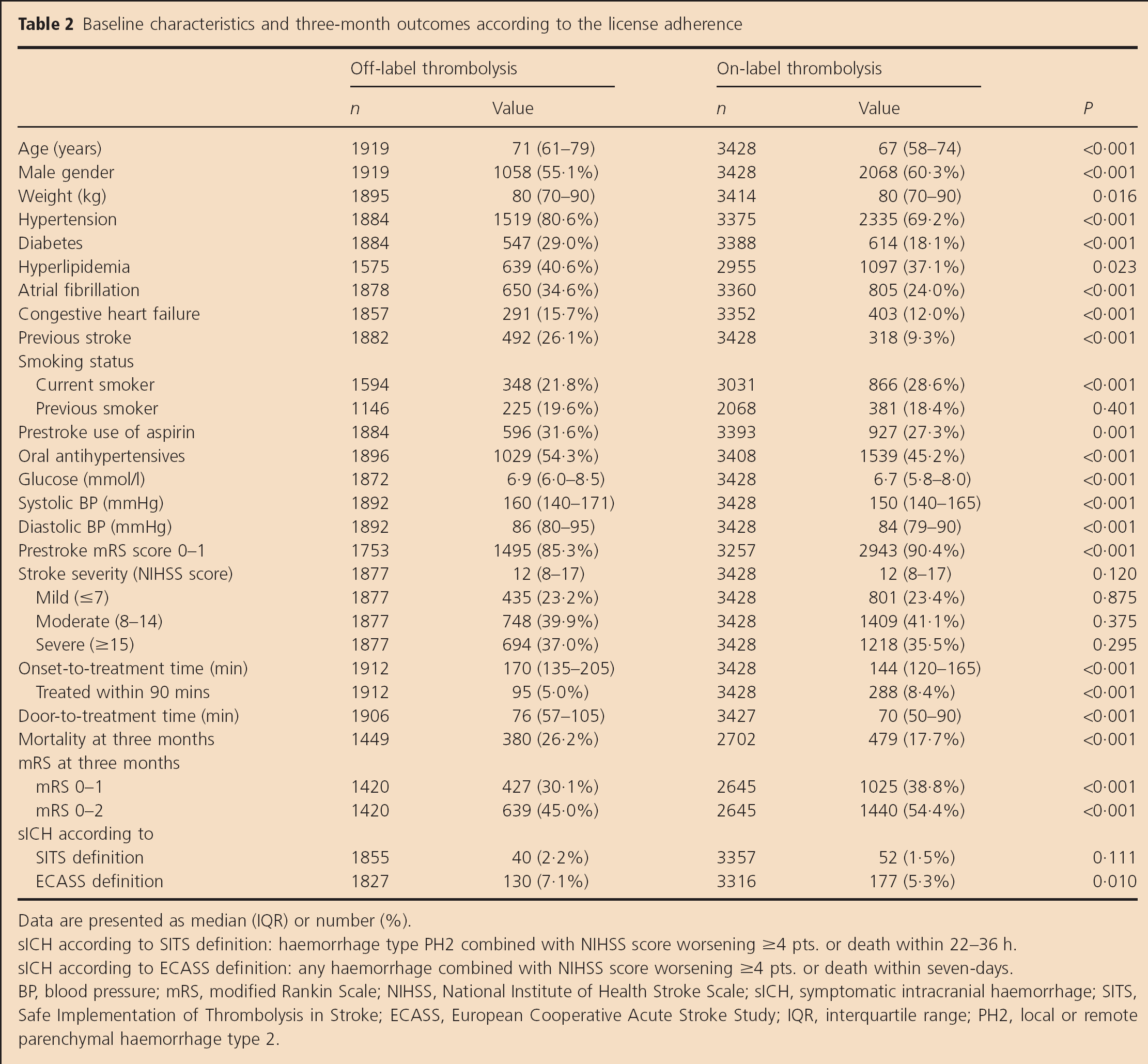
Data are presented as median (IQR) or number (%).
sICH according to SITS definition: haemorrhage type PH2 combined with NIHSS score worsening ≥4 pts. or death within 22–36 h.
sICH according to ECASS definition: any haemorrhage combined with NIHSS score worsening ≥4 pts. or death within seven-days.
BP, blood pressure; mRS, modified Rankin Scale; NIHSS, National Institute of Health Stroke Scale; sICH, symptomatic intracranial haemorrhage; SITS, Safe Implementation of Thrombolysis in Stroke; ECASS, European Cooperative Acute Stroke Study; IQR, interquartile range; PH2, local or remote parenchymal haemorrhage type 2.
In patients treated off-label, there was a trend for higher incidence of sICH according to SITS (2·2% vs. 1·5%, P = 0·111), and a significant difference in sICHs according to ECASS definition (7·1% vs. 5·3%, P = 0·010). Both were not confirmed in multivariate analyses. However, we observed a trend for increased odds of sICH according to SITS in patients with time-to-treatment >3 h (OR 1·87; 95% CI: 0·96–3·66). The adverse association between NIHSS >25 and sICH according to ECASS was significant after excluding NIHSS as continuous covariable from the model (Table 3). Negative influence of INR >l·7 (sICH according to SITS), previous stroke with concomitant diabetes, and inappropriate glucose concentration (sICH according to ECASS) was significant only in univariate analyses (Table 4).
Adjusted odds ratio (OR) for sICH adjusted for independent predictors
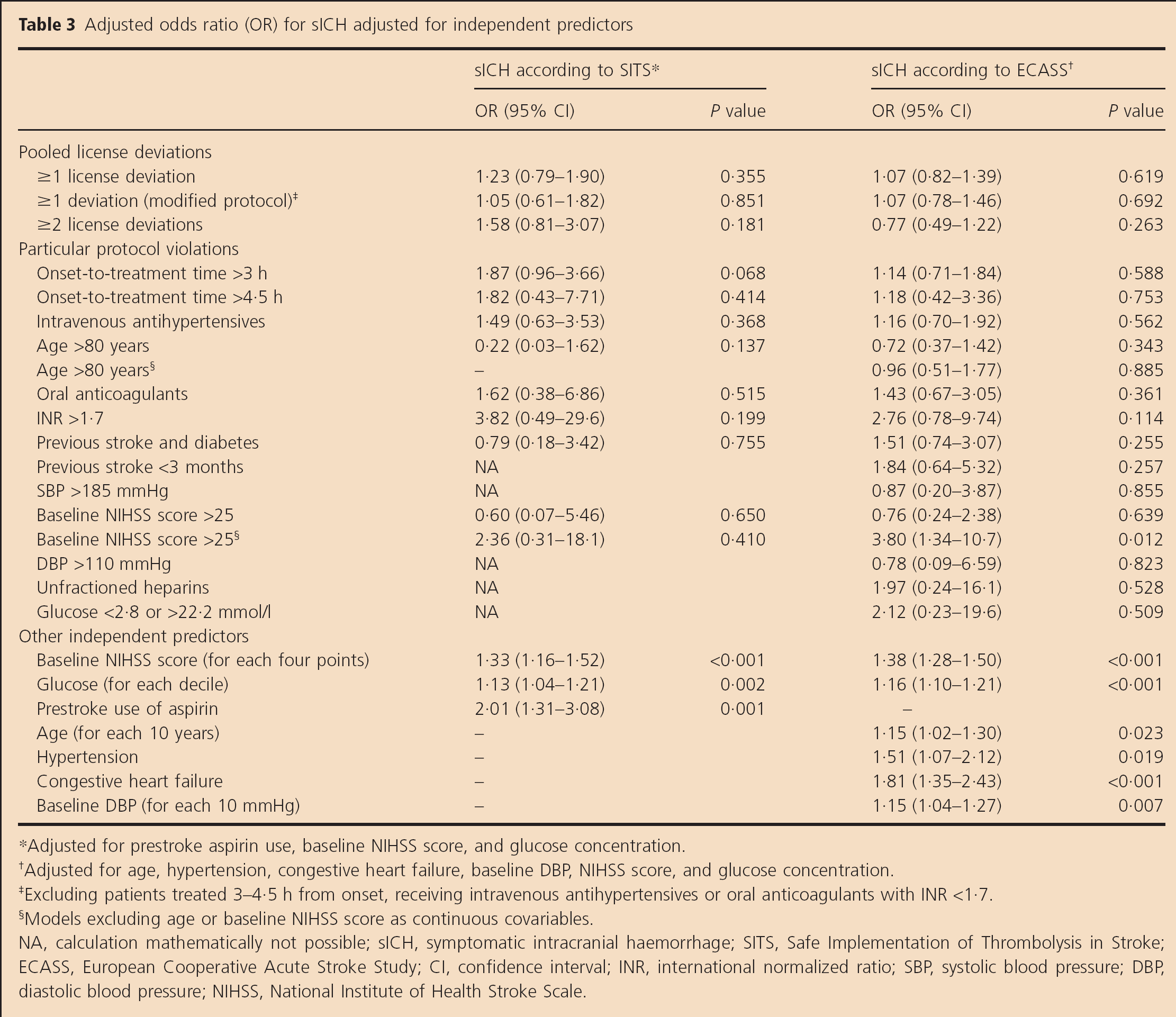
Adjusted for prestroke aspirin use, baseline NIHSS score, and glucose concentration.
Adjusted for age, hypertension, congestive heart failure, baseline DBP, NIHSS score, and glucose concentration.
Excluding patients treated 3–1·5 h from onset, receiving intravenous antihypertensives or oral anticoagulants with INR <1·7.
Models excluding age or baseline NIHSS score as continuous covariables.
NA, calculation mathematically not possible; sICH, symptomatic intracranial haemorrhage; SITS, Safe Implementation of Thrombolysis in Stroke; ECASS, European Cooperative Acute Stroke Study; CI, confidence interval; INR, international normalized ratio; SBP, systolic blood pressure; DBP, diastolic blood pressure; NIHSS, National Institute of Health Stroke Scale.
Unadjusted odds ratio (OR) for sICH
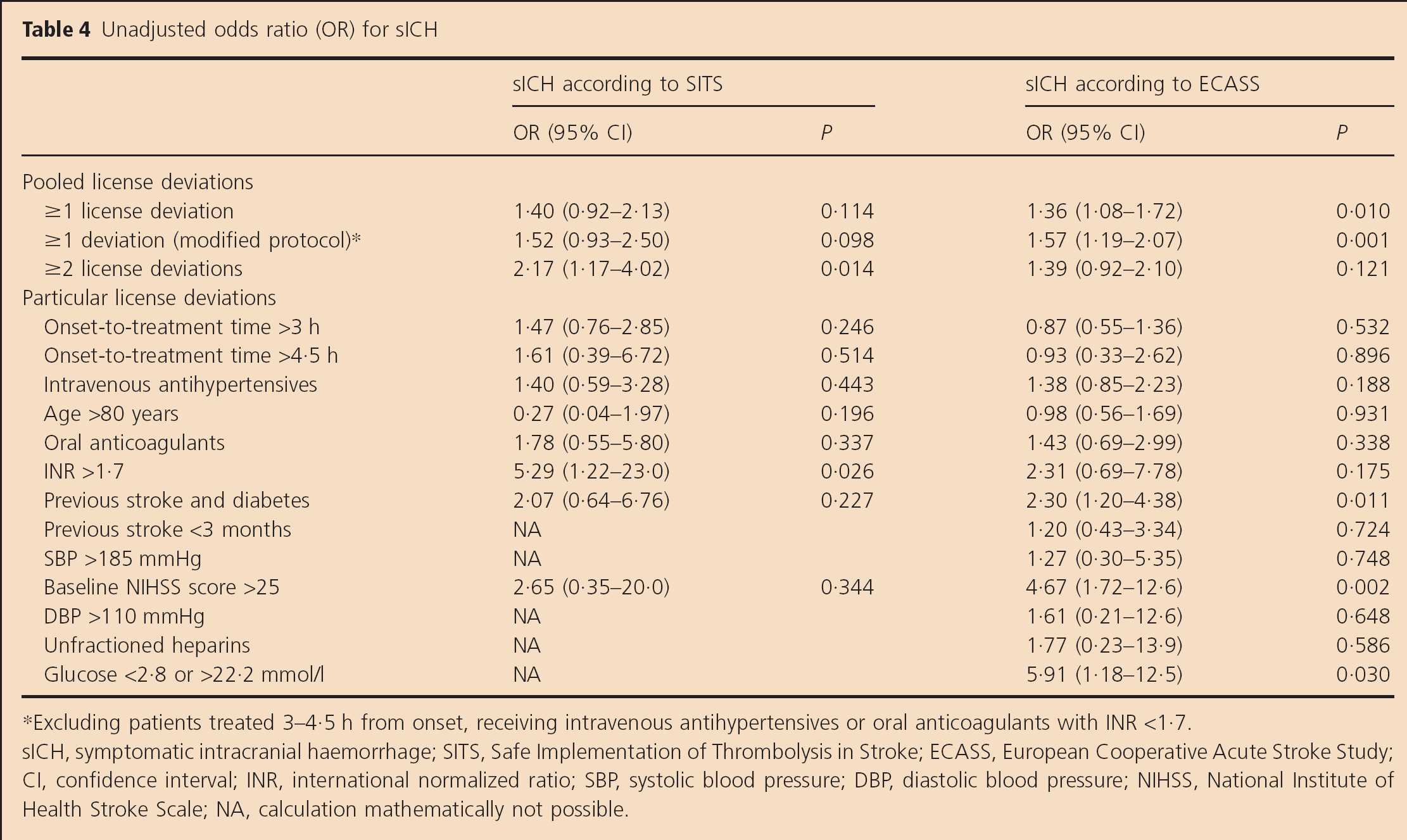
Excluding patients treated 3–4·5 h from onset, receiving intravenous antihypertensives or oral anticoagulants with INR <1·7.
sICH, symptomatic intracranial haemorrhage; SITS, Safe Implementation of Thrombolysis in Stroke; ECASS, European Cooperative Acute Stroke Study; CI, confidence interval; INR, international normalized ratio; SBP, systolic blood pressure; DBP, diastolic blood pressure; NIHSS, National Institute of Health Stroke Scale; NA, calculation mathematically not possible.
In the off-label group, we also observed a significantly higher three-month mortality (26·2% vs. 17·7%, OR 1·64; 95% CI: 1·41–1·92) and a higher proportion of three-month unfavorable outcome (55·0% vs. 45·6%, OR 1·46; 95% CI: 1·28–1·66) (Table 2). The distribution of mRS scores at three months is presented in Fig. 1.
In multivariate analysis adjusted for independent predictors (i.e. age, diabetes, congestive heart failure, oral antihypertensive treatment, prestroke mRS 0–1, and baseline NIHSS score), the association between any protocol nonadherence and the risk of death was not significant (OR 1·17; 95% CI: 0·97–1·42 for ≥1 deviation). However, it was significant in the sensitivity analysis after excluding from the nonprotocol group patients with INR <l·7, treated 3–4·5 h from the onset or receiving intravenous antihypertensives. Considering particular deviations, we found an adverse trend for age >80 years (OR 1·41; 95% CI: 0·92–2·18), which was significant after excluding age as an independent continuous covariable from the model (Table 5).
Adjusted odds ratio (OR) for three-month mortality and unfavorable outcome (mRS 3–6) adjusted for independent predictors
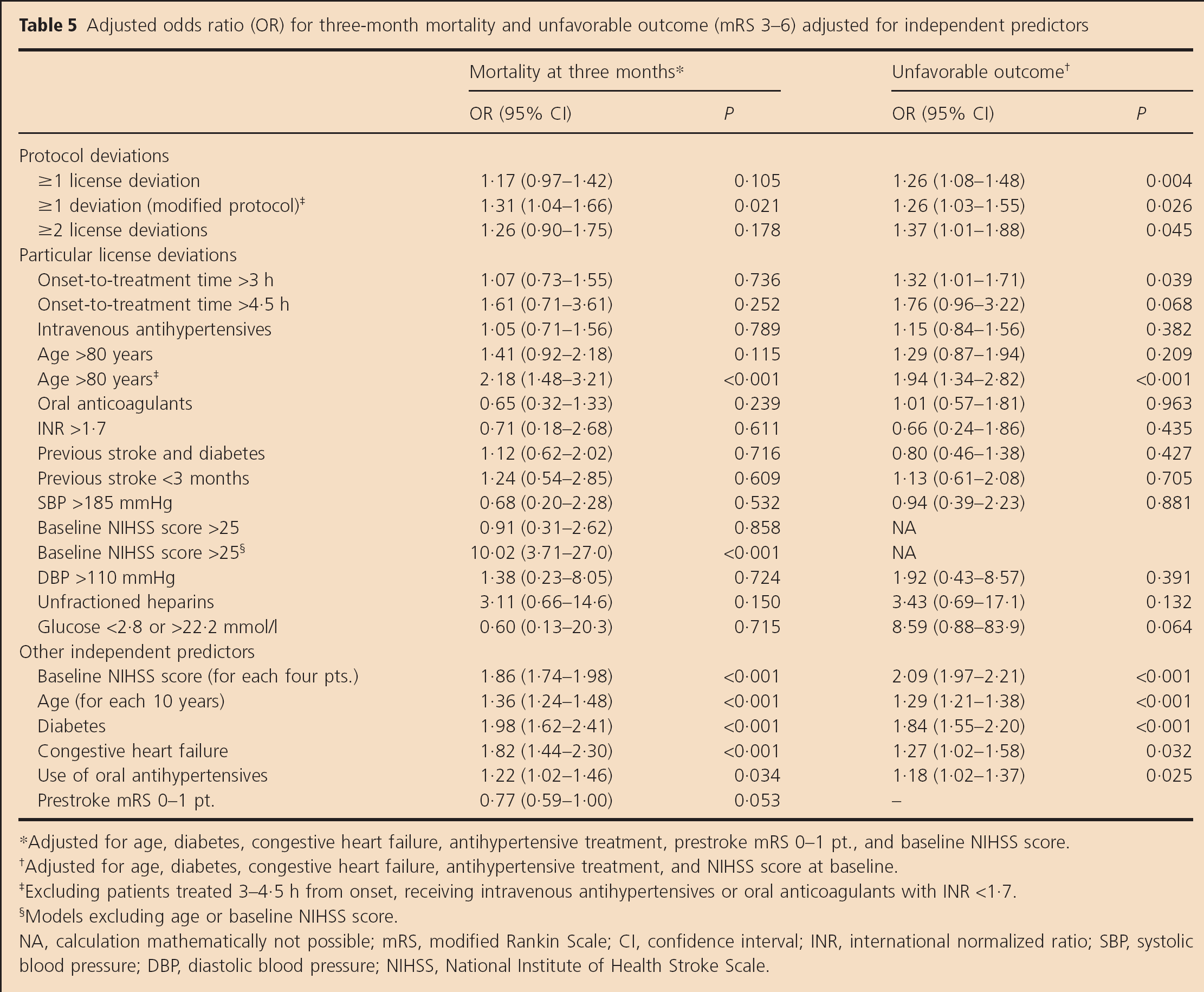
Adjusted for age, diabetes, congestive heart failure, antihypertensive treatment, prestroke mRS 0–1 pt., and baseline NIHSS score.
Adjusted for age, diabetes, congestive heart failure, antihypertensive treatment, and NIHSS score at baseline.
Excluding patients treated 3–4·5 h from onset, receiving intravenous antihypertensives or oral anticoagulants with INR <1·7.
Models excluding age or baseline NIHSS score.
NA, calculation mathematically not possible; mRS, modified Rankin Scale; CI, confidence interval; INR, international normalized ratio; SBP, systolic blood pressure; DBP, diastolic blood pressure; NIHSS, National Institute of Health Stroke Scale.
In multivariate analysis adjusted for independent predictors (i.e. age, diabetes, congestive heart failure, oral antihypertensive treatment, and baseline NIHSS score), any protocol nonadherence significantly affected the risk of unfavorable three-month outcome (OR 1·26; 95% CI: 1·08–1·48 for ≥1 deviation). Considering particular deviations, we observed a significant association with time-to-treatment >3 h (OR 1·32, 95% CI: 1·01–1·71) and a trend for hyperglycemia (only one case with glucose concentration <2·8 mmol/l)(OR 8·59, 95% CI: 0·88–83·9). The influence of age >80 years was significant after excluding age as an independent continuous covariable (Table 5).
Discussion
Our study is the first large multinational study directly addressing the issue of off-label thrombolysis. Although the gap in the access to health care between East and West is gradually closing, the management of preexisting comorbidities and poststroke care in the region is still less effective and may affect the recovery (14). For example, in Poland between 2003 and 2007, the onset-to-treatment time and door-to-treatment time were significantly longer, and the three-month mortality was significantly higher than reported in SITS-MOST (15). It seems reasonable to be cautious about extrapolating the Western European findings directly to the Central/ Eastern population. On the other hand, the non-Western results may be considered a surrogate worst-case scenario for safety evaluations in the Western countries. Therefore, our findings are both region specific and generalizable.
According to our data, patients not adhering to the current license are at increased risk of unfavorable outcome, especially those treated >3 hours from onset and probably aged >80 years or with glucose concentration >22·2 mmol/l. Nonadherence to the modified protocol (i.e. allowing treatment <4·5 h, use of intravenous antihypertensives and oral anticoagulants with INR <1·7) was independently associated with increased mortality. Apart from the adverse trend for time-to-treatment >3 h, we found no clear associations with the risk of sICH.
In a recent study, Meretoja et al. evaluated safety and effectiveness of thrombolysis outside the European license in a group of 985 consecutive patients treated in Helsinki. At least one deviation was observed in 499 cases (51%). The most frequent were: age >80 years (16%), mild stroke (13%), use of intravenous antihypertensives (11%), onset-to-treatment time >3 h (10%), blood pressure >185/110 mmHg (5%), and oral anticoagulation (4%). Pooled off-label thrombolysis was associated with a trend for unfavorable outcome (OR 1·37; 95% CI: 0·95–1·97) but did not affect the risk of sICH according to the ECASS definition (OR 0·80; 95% CI: 0·43–1·48). The only contraindication independently associated with unfavorable outcome was age >80 years (OR 2·18; 95% CI: 1·27–3·73). It partially concurs with our findings. The differences may be attributed to a lower number of participants, better organization of acute care (34–min median door-to-treatment time), better overall outcome (8·7% on-label mortality, 39·6% unfavorable outcome), and methodological differences. The above-mentioned study did not examine factors influencing mortality. Patients with basilar artery occlusion were not included, and treatment in patients with NIHSS 0–4 (not formally defined as minor stroke) was considered off-label. The OR were calculated without exclusion of patients with multiple deviations, and a 21-variable model was not limited to independent outcome predictors (16).
Treatment outcome outside SITS-MOST protocol was evaluated also by Rubiera et al. They included 369 nonlacunar stroke patients with a documented intracranial artery occlusion, INR <1·8 and mismatch on MRI if treated >3 h from the onset. The non-SITS-MOST group consisted of patients aged >80 years (n = 91), treated 3–6 h from onset (n = 124), with stroke severity >25 NIHSS (n = 16), and previous stroke with concomitant diabetes (n = 12). Although there were no differences in the rate of sICH, the non-SITS-MOST group demonstrated a trend for higher three-month mortality (16·1% vs. 10·5%; P = 0·084) and higher ratio of unfavorable outcome (60·4% vs. 51·7%; P = 0·082). After excluding patients aged >80 years, the proportion of unfavorable outcome was comparable with the per-protocol group (5). Despite methodological differences (narrow inclusion criteria, median NIHSS score of 17, and a large number of patients thrombolyzed >3 h from onset), these results are generally consistent with ours.
Those two studies as well as our study show that patients not fully adhering to the SITS protocol/European license may achieve less favorable outcome. Importantly, it does not allow concluding that those patients do not benefit from the treatment. Indirect controlled comparisons of treated vs. untreated patients offer reassurance that intravenous thrombolysis is beneficial in certain groups of off-label patients (e.g. the elderly or those with concomitant diabetes and prior stroke) (11,17). However, in other groups (i.e. NIHSS <4 or >25), it appears to be dubious (18). Final conclusions can be provided only by controlled clinical trials (e.g. Third International Stroke Trial, Thrombolysis in Elderly Stroke Patients in Italy) (19). Until then, we need to rely on registry-based analyses and other pooled studies.
Intravenous thrombolysis ≤4·5 h from the stroke onset or even beyond this time window has already been proved safe and effective (6,7,12,13). In our study, patients treated <3 h from the onset achieved worse outcome and demonstrated trend for higher incidence of sICH according to SITS definition, which is partially consistent with the analysis of the whole SITS-ISTR population (20).
There is no direct evidence against aggressive management of elevated blood pressure with intravenous antihypertensives to achieve values <185/110 mmHg before thrombolysis (21). Withholding antihypertensive treatment in patients with a history of hypertension is associated with worse outcome (22). Therefore, using effective and easily reversible intravenous treatment for the optimal control of very high blood pressure should not be considered a contraindication for rt-PA. Our results support this thesis.
Despite the general trend to widen the access of elderly stroke patients to rt-PA, the debate remains open. A meta-analysis of cohort studies by Engelter et al. indicates that elderly patients had higher three-month mortality and were less likely to achieve favorable outcome (mRS ≤1) (8). In a more recent meta-analysis by Meseguer et al., mortality was not assessed, but the likelihood of unfavorable outcome similarly increased (9). However, both analyses were not adjusted for other outcome predictors. In the most recent study of the whole SITS-ISTR population, Ford et al. demonstrated that the risk of sICH was not increased. However, the elderly had a higher three-month mortality rate and reduced independence (10). It partially concurs with our findings showing that age >80 years may affect mortality and less likely the functional outcome.
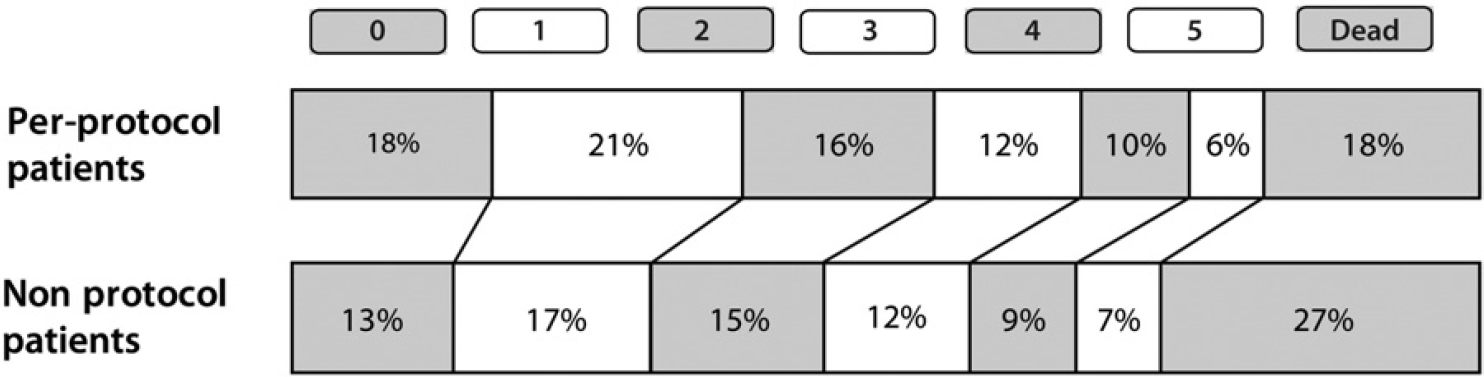
Distribution of mRS scores at three-months. mRs, modified Rankin Scale.
Our results show that ineffective oral anticoagulation probably does not increase the risk of death or unfavorable outcome. We found a slight trend for higher incidence of sICH, especially in the subgroup with INR >1·7. Concerns about sICH has also been raised by Prabhakaran et al. (23), but we think that presently there is not enough evidence to discourage thrombolysis in patients with subtherapeutic INR.
Previous stroke ≤3 months and stroke with concomitant diabetes did not significantly affect the outcome. However, the confidence intervals were not narrow enough to conclude that those contraindications are irrelevant. The evidence is still limited (4,1617), but withholding treatment in those patients may not be justified.
Elevated blood glucose concentration is associated with worse prognosis irrespectively of thrombolysis (24). It also increases the odds for sICH after treatment (24,25). Together with our findings, this supports the need for extreme caution while considering alteplase in patients with glucose concentration >22·2 mmol/l.
Our study is based on a voluntary registry and therefore has certain limitations. It is not possible to identify how many patients from both groups and due to what reasons were not reported to the registry. We may not exclude that some of them died early, had an sICH, received rt-PA despite other severe license deviations, or were admitted during the weekend. As the sampling in the off-label group was not random, it is also not possible to clearly distinguish between poor outcomes caused by underlying conditions and the effect of treatment itself. Patients in the off-label group had significantly worse comorbidity state. To minimize the influence of confounders, we used multivariate models adjusted for all independent outcome predictors. However, it does not eliminate their influence completely. To make particular estimates more precise we, decided to include cases with isolated missing values. We managed to perform separate calculations for each license deviation, but the number of valid cases was often low and the confidence intervals not narrow enough for drawing strong conclusions.
Nonetheless, our findings show that in Central and Eastern Europe one-third of ischemic stroke patients treated with intravenous alteplase have not fully adhered to the drug license. They achieved significantly worse outcome but were not at clearly increased risk of sICH. The study demonstrates that some exclusion criteria seem particularly relevant (>4·5 h time-to-treatment, glucose concentration >22·2 mmol/l), while other (aggressive blood pressure management with intravenous medication or oral anticoagulation with INR > 1·7) appear more redundant. In our everyday clinical decision making, we should rely on available evidence and guidelines. Therefore, we should not deny treatment to those patients only because of license limitations. However, for final conclusions, we still need results of ongoing randomized trials and other controlled studies.
Footnotes
Appendix
Countries participating in SITS-EAST with national coordinators and number of contributed patients: Czech Republic (Robert Mikulik – 3073), Poland (Anna Czlonkowska – 1016), Slovakia (Miroslav Brozman – 414), Slovenia (Viktor Svigelj – 307), Hungary (Laszlo Csiba – 303), Estonia (Janika Korv – 194), Croatia (Vida Demarin – 148), Lithuania (Dalius Jatuzis, Alexandras Vilionskis – 93), and Turkey (Yakup Krespi – 46).
Acknowledgements
We would like to thank Professor Peter Sandercock and Dr William Whiteley from the University of Edinburgh for their valuable advice while preparing the manuscript.