
Abstract
Rationale
Copeptin independently predicts functional outcome and mortality at 90 days and one-year after ischemic stroke. In patients with transient ischemic attack, elevated copeptin values indicate an increased risk of further cerebrovascular events.
Aims
The Copeptin Risk Stratification (CoRisk) study aims to validate the predictive value of copeptin in patients with ischemic stroke and transient ischemic attack. In patients with ischemic stroke, the CoRisk study aims to further explore the effect of treatment (i.e. thrombolysis) on the predictive value of copeptin.
Design
Prospective observational multicenter study analyzing three groups of patients, i.e. patients with ischemic stroke treated with and without thrombolysis and patients with transient ischemic attack.
Outcomes Primary end-point:
In patients with ischemic stroke, the primary end-point includes disability (modified Rankin scale from 3 to 5) and mortality (modified Rankin scale 6) at three-months after stroke. In patients with transient ischemic attack, the primary end-point is a recurrent ischemic cerebrovascular event (i.e. ischemic stroke or recurrent transient ischemic attack). Secondary end-point: In patients with ischemic stroke, the secondary end-points include in-house complications (i.e. symptomatic intracerebral hemorrhage, malignant edema, aspiration pneumonia or seizures during hospitalization, and in-house mortality).
Introduction
In patients with ischemic stroke, age and stroke severity assessed by the National Institute of Health Stroke Scale (NIHSS) are the main clinical variables predicting functional outcome and mortality (1). Time from stroke onset to thrombolysis represents an additional prognostic factor in patients treated with intravenous thrombolysis within the first 4·5 h (2). However, predictive models based on simple clinical variables do not necessarily make better predictions of functional outcome as compared with experienced stroke physicians (3). In patients with transient ischemic attack (TIA), the age, blood pressure, clinic, duration & diabetes mellitus (ABCD2) score helps stratifying the risk for subsequent ischemic stroke (4). Improvement of these predictive models is relevant to patients, their families, and treating physicians. With an accurate prognosis, treating physicians could individualize treatment and optimally allocate our limited healthcare resources. Biomarkers, which accurately and reliably discriminate between favorable and unfavorable outcome and which are readily available, are needed to improve the current prognostic models in clinical routine. Even though many blood biomarkers have been associated with poor outcome after ischemic stroke, the majority of the studies did not report whether the evaluated biomarkers improved outcome prediction beyond clinical evaluation and neuroimaging (5). Recently, it has been demonstrated that copeptin, a fragment of the vasopressin precursor hormone, independently predicts functional outcome and mortality in patients with ischemic stroke as well as recurrent cerebrovascular events in patients with TIA (6,7). Importantly, copeptin improved risk stratification beyond the clinical severity of stroke or TIA, assessed by established clinical scores (i.e. National Institute of Stroke Health Score and the ABCD2 score, respectively). To provide all the information needed to assess a novel marker, measures of discrimination (e.g. C-statistics), accuracy (e.g. calibration by a goodness of fit test (8)), and improvement of risk classification (integrated discrimination improvement (9)) should be reported (10).
Before implementing any marker such as copeptin in the routine clinical practice, it is crucial to validate its prognostic value in an independent cohort of patients (11). Moreover, it is relevant to further explore the predictive properties of copeptin in patients undergoing thrombolysis. The Copeptin and Risk Stratifiction in ischemic stroke and TIA patients study aims to validate copeptin as prognostic marker of outcome in patients with ischemic stroke, assessing patients treated with and without thrombolysis separately, and as marker for recurrent cerebrovascular events in patients with TIAs.
Methods
This study is registered in ClinicalTrials.gov under the number NCT00878813.
Study design
The CoRisk study is a prospective observational multicenter study to evaluate three groups of patients:
patients with ischemic stroke treated with thrombolysis;
patients with ischemic stroke treated without thrombolysis; and
patients with TIA.
We defined ischemic stroke according to the World Health Organization criteria as an acute focal neurological deficit lasting longer than 24 h (12), and we included patients with symptom onset within 24 h before admission but no sign of acute intracranial bleeding on imaging. We defined TIA as a transient episode of neurological dysfunction caused by a focal brain injury with symptoms lasting 24 h or less, irrespective whether diffusion weighted magnetic resonance imaging (MRI) showed a lesion or not. We chose this time instead of tissue-based definition of TIA to give the participating neurologists the liberty to choose the ancillary investigations as they feel appropriate.
Study setting
Leading center: Emergency and Neurological Department of Inselspital, University Hospital of Bern (Switzerland). Col-laborating centers: Emergency and Neurological Departments of the University Hospital of Basel (Switzerland)/Charité – Campus Benjamin Franklin, Berlin (Germany)/Johann Wolfgang Goethe-University, Frankfurt am Main (Germany).
Inclusion and exclusion criteria
Inclusion criteria
All consecutive patients who are admitted to the neurological emergency department or the neurological ward with a suspected ischemic stroke or TIA within 24 h of symptom onset. For each study participant, informed consent is obtained.
Exclusion criteria
No informed consent. Patients discharged from hospital with a diagnosis different from ischemic stroke or TIA (stroke mimics). Data regarding patients with stroke mimics will be kept in the database and used for potential future analysis.
Study plan
Enrolment
All eligible patients in the neurological emergency department or the neurological ward will be enrolled into the study. On admission, during the first routine blood sampling, 15 ml of blood will be drawn for the study, with 7·5 ml being filled in an ethylenediaminetetraacetic acid-containing tube and 7·5 ml in a plasma tube. In patients undergoing thrombolysis, an additional and identical blood sample will be taken at the first routine venipuncture on the day after thrombolysis. Copeptin levels will be assessed in plasma in two intermediate and one final blinded batch analysis. A new chemiluminescence sandwich immunoassay will be used. The lower detection limit is 0·4 pmol/l and the functional assay sensitivity is <1 pmol/l (<20% inter assay coefficient of variation, defined as the ratio of the standard deviation (SD) to the mean). Median copeptin levels in 200 healthy individuals was 3·7 pmol/l and the 97·5 percentile is 16·4 pmol/l (13).
Data sampling
On admission and during hospital stay, clinical items including weight, blood pressure, pulse rate, and body temperature will be assessed by chart review until discharge. Computed tomography (CT) or MRI will be performed on admission and 24–36 h after intravenous (IV) or intra-arterial (IA) thrombolysis. In all patients, additional CT/MRI studies will be performed at the discretion of the treating physicians. The clinical stroke severity will be assessed by the NIHSS on admission (14). The clinical stroke type will be defined as stroke in the anterior circulation or posterior circulation as previously defined (15). Comorbidities will be assessed on admission by the Charlson Comorbidity Index (16,17). Detailed information such as results of brain imaging, cardiac ultrasound, vascular imaging, 24-h electrocardiogram will be collected to define stroke etiology according to the Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification (17). The TOAST classification denotes five subtypes of ischemic stroke:
large-artery atherosclerosis;
cardioembolism;
small-vessel occlusion;
stroke of other determined etiology and
stroke of undetermined etiology.
Selected medical complication defined according to published criteria will be assessed until discharge (see secondary end-point) (18).
In patients undergoing any form of vessel imaging after thrombolysis, namely angio-CT/-MR or digital substraction angiograpgy, vessel recanalization will be documented and graded according to the Thrombolysis in Myocardial Infarction (TIMI) classification. The TIMI classification encompasses four grades of recanalization: no recanalization (TIMI 0), minimal (TIMI 1), partial (TIMI 2), and complete (TIMI 3) (19). The recanalization degree will be analyzed in association with the copeptin level on day one and its change from day zero.
Follow-up
Outcome will be assessed three-months after the index stroke or TIA by stroke physicians and study nurses through a structured interview. The outcome of patients not returning to the planned outpatient visit will be assessed by phone through the same structured interview. In order to avoid biases, the end-point evaluators will be blinded to the copeptin levels.
Primary end-point
In patients with ischemic stroke, the primary end-point is death or disability (modified Rankin Scale score 3–6), in patients with TIA, it is a recurrent ischemic stroke or TIA (20).
Secondary end-point
In patients with ischemic stroke, the secondary outcomes include symptomatic intracerebral hemorrhage, space occupying cerebral edema, pneumonia (defined as auscultatory respiratory crackles combined with body temperature ≥38°C, purulent sputum, or positive chest X-ray), seizures (clinical diagnosis of focal and/or generalized seizure in a previously nonepileptic patient), or mortality during hospitalization (18). Intracerebral hemorrhage will be classified as ‘symptomatic’ if a parenchymal hematoma type 2 is accompanied by a four-point increase in the NIHSS score or leading to death -according to the Safe Implementation of Thrombolysis in Stroke-Monitoring Study (SITS-MOST) criteria (21) – otherwise it was defined as ‘asymptomatic’ intracerebral hemorrhage.
Data monitoring body
The Ethical Committee of the Canton Bern (Switzerland) gave its consent to this study and represents the official data monitoring body of this investigator-driven study.
Sample size estimation
Sample size
The relation of copeptin with end-points will be assessed using univariate comparisons and multivariate logistic regression models adjusted for significant outcome predictors. It has been demonstrated that multiple regression models with about 10–15 observations per predictor variable reveal good estimates (22). Considering five predictor variables, about 65 patients should present an unfavorable outcome three-months after the index event in order to provide reliable estimates in the multivariate model (Table 1).
Estimated sample size per subgroup of the CoRisk study
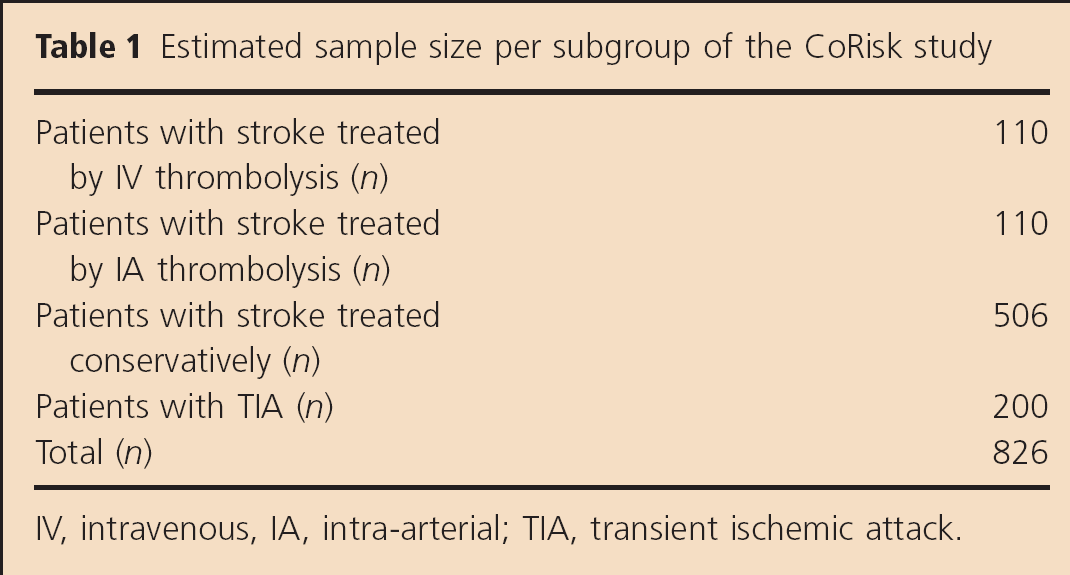
IV, intravenous, IA, intra-arterial; TIA, transient ischemic attack.
Sample size of patients undergoing IV thrombolysis (IVT)
In the National Institute of Neurological Disorders and Stroke (NINDS) trial, 40% of the patients treated with IVT had an unfavorable outcome three-months after the stroke (23). We will need to include at least 110 patients treated with IVT for a reliable multivariate analysis with four covariates.
Sample size of patients undergoing IA thrombolysis (IAT)
In the Prolyse in Acute Cerebral Thromboembolism II (PROACT-II) trial, 60% of the patients treated with IAT had an unfavorable outcome three-months after the stroke. We will need to include at least 110 patients treated with IA therapy for a reliable multivariate analysis with five covariates.
Sample size of the stroke patients treated conservatively
Because blood for copeptin analysis is drawn in an urgent setting in all patients admitted with an acute cerebrovascular event, we will include patients for the whole length of the study consecutively.
Based on the statistics of the enrolling neurological emergency department, the ratio of patients treated conservatively vs. thrombolysis is of approximately 2·3/1. Hence, we plan to include at least 506 patients with stroke treated conservatively, considered a minimum sample size of 220 patients treated with thrombolysis.
Sample size of the patients with TIA
Based on the statistics of the enrolling neurological emergency department, the ratio of patients with stroke vs. TIA is of approximately 3·5/1. Hence, we will include at least 200 patients with TIA, considered a minimum sample size of 706 of patients with stroke. In a similar study conducted at the University Hospital of Basel (Switzerland), about 10% of patients with TIA experienced a recurrent cerebrovascular event within three-months (6). Therefore, a number of 200 patients with TIA will suffice for a reliable analysis adjusting for the ABCD2 score as main known clinical predictor.
Power calculations
Based on previously published data [mean logCopeptin in patients with favorable outcome = 0·95, SD = 0·45, and 1·34, SD = 0·57 with unfavorable outcome (6)] with the estimation of 44 patients with an unfavorable outcome and 66 patients with a favorable outcome undergoing thrombolysis we would have a 96·8% power to detect a significant difference in average copeptin levels when in fact there is a true difference at a 5% level of significance.
Based on a pilot study in patients with TIA (i.e. mean of logCopeptin in patients with no re-event = 0·70, SD = 0·40; mean of logCopeptin 1·1, SD = 0·49 in patients with a re-event), we similarly calculated a power of 97% to detect a significant difference in means when in fact there is a true difference at a 5% level of significance (7). If event rates are lower than expected, the sample sizes will be increased by expanding the enrollment period or number of centers recruiting.
Statistical analysis
Discrete variables will be expressed as counts (percentage) and continuous variables as means ± SD or median (interquartile range), unless stated otherwise. Frequency comparison will be done by Fisher's exact test. Two-group comparison of data will be performed by the Mann–Whitney U-test. The Kruskal–Wallis one-way analysis of variance with Bonferroni's multiple post hoc test will be used if more than two groups are compared. Correlation analyses will be performed by using Spearman rank correlation. We will evaluate known predictors (e.g. age, gender, and NIHSS), comorbidities according to the Charlson Comorbidity Index, clinical stroke type, stroke etiology, routine laboratory parameters [i.e. with blood cell count, hemoglobin, thrombocytes, international normalized ratio (INR), C-reactive protein, glucose, Hemoglobin A1c (HbA1c) and creatinine], vital signs, medical history, and copeptin levels in multivariate logistic regression analysis if a significant association with the primary outcome was found in the univariate regression model. In addition, in TIA patients, we will also perform multivariable Cox proportional hazard regression modeling to estimate hazard ratios for the effect of copeptin levels on risk of recurrent cerebrovascular events. Receiver-operating-characteristic (ROC) curves will be calculated with the area under the ROC curve as an overall discriminatory measure to compare different outcome predictors. To assess the calibration of the predictive models, we will compare the number of observed events with those that are expected on the basis of estimation from the models within different a priori risk groups based on data by Goldstein et al. (1,24).
To further estimate the additive benefit of copeptin levels to traditional outcome predictors (i.e. NIHSS), we will calculate the net reclassification improvement as recently shown (25).
Finally, to study the ability of copeptin for mortality prediction, we will also calculate Kaplan–Meier survival curves and stratify patients by copeptin tertiles. Observations will be censored at the time of last follow-up. In addition to the final analysis, two evenly spaced interim analyses will be performed after 50% and 75% of the estimated events will have occurred, and appropriate statistical corrections will account for them to hold the overall significance level for the final analysis to P < 0·05.
All testing will be two-tailed, and P values less than 0·05 will be considered to indicate statistical significance.
Discussion
The use of blood biomarkers is becoming increasingly popular in different fields of medicine. Potential clinical applications have been considered for biomarkers in vascular neurology, including: characterizing stroke size and clinical severity, identifying stroke etiology, estimating short-term risk of progression or worsening, risk of mortality, and long-term functional outcome. At present, only few studies have shown additional information beyond that gained from standard clinical evaluation and imaging. Incorporating different statistical methods to address this question, we describe the design of a prospective multicenter biomarker study to address the question whether copeptin as the marker of interest independently predicts stroke outcome or recurrence after TIA and, importantly, whether copeptin will provide information beyond the available routine clinical information to finally improve risk stratification.
Footnotes
Acknowledgements
We would like to thank the study nurses Susanne von Kaenel and Marianne Kormann, Inselspital Bern (Switzerland) for their practical help.