
Abstract
Background
A feature of stroke is that it recurs (25% within five-years). Risk factors for stroke and recurrent stroke include smoking, alcohol consumption, poor diet, and physical inactivity.
Aim
To evaluate the effectiveness of secondary prevention lifestyle interventions designed to change lifestyle behavior following stroke. This short paper presents a summary of the systematic review process and findings.
Methods
Ten major databases were searched using subject headings and key words. Papers were screened using review-specific criteria. Critical appraisal and data extraction were conducted independently by two reviewers. Data were pooled in statistical meta-analysis; where this was not possible findings were presented in narrative form.
Results
Three studies involving 581 participants were reviewed. Two models of intervention delivery were reported: shared care and nurse-led. Interventions were delivered to groups or in one-to-one consultations. Metaanalyses of the pooled lifestyle data favored the interventions (2P = 0.02). In terms of physiological outcomes, while overall treatment effect was not significant, pooled results did approach statistical significance (2P = 0.08), however the test of heterogeneity was significant, suggesting differences in the variables that were pooled. Pooled secondary outcomes, including perceived health status and stroke knowledge, favored the interventions (2P #< 0.00001), however, the test for heterogeneity was highly significant.
Conclusion
Stroke secondary prevention lifestyle interventions are effective in terms of effecting positive change in lifestyle behaviors and secondary outcomes, and appear promising in relation to physiological outcomes. There was insufficient evidence to determine the effect of intervention on incidence of stroke recurrence.
Keywords
Background
Each year, approximately 15 million people worldwide have a stroke; of these, five million die and another five million are chronically disabled. One of the features of stroke is that it recurs (25% within five-years) (1). In the United States, for example, there are 795 000 strokes annually, of which approximately 30% are recurrent events (2). Consequences of recurrence include risk of death (15% at three-months poststroke), increased disability, and institutionalization (1). Ten risk factors for stroke have been identified (3), of which many are associated with lifestyle behaviors, including smoking, alcohol consumption, poor diet, and physical inactivity and may be addressed by means of behavioral health promotion interventions. Lifestyle risk factors for recurrence are the same as those for first-ever stroke (4,5). Recent improvements in the treatment and management of stroke have resulted in a decline in the incidence of stroke in many developed countries. However, the global incidence remains high and prevalence is rising due to the ageing demographic of the population (6,7). It is estimated that in 2030, stroke is likely to remain the second highest cause of death worldwide (8).
In light of the aforementioned, following stroke, it is essential that clinicians implement effective health promotion strategies and interventions that address modifiable lifestyle risk factors for recurrent stroke as well as other modifiable risk factors such as hypertension (9). Evidence-based guidelines recommend that secondary prevention interventions should be multimodal, i.e. they should combine prescription of appropriate medication with active provision of information and education (9,10). It is further recommended that interventions should be initiated while patients are in hospital and followed up in primary care (11,12). However, physician adherence to treatment guidelines is sub-optimal (13,14). For example, rates of prescription of combination therapy (i.e. antiplatelet, antihypertensive, and statin) are low (15), and this is compounded by high rates of noncompliance among patients (14). A recent Cochrane review highlighted the need for the development of strategies to assist patients to follow medication prescriptions for long-term conditions (16). Such strategies include educating patients about stroke, their prescription medication, and the importance of adherence. At present, evidence suggests that stroke patients' knowledge levels are low regarding stroke risk factors, medication, and the need to take immediate action if stroke is suspected (e.g. (17,18)), but that they want more information about how to avoid recurrence (19), findings that highlight the need for effective secondary prevention interventions.
Scoping searches undertaken in MEDLINE and CINAHL revealed a limited evidence base regarding the effectiveness of multimodal interventions designed to address recurrent stroke. Therefore, we undertook a systematic review, which sought to establish the current evidence regarding the effectiveness of secondary prevention behavioral interventions that address one or more modifiable lifestyle risk factors for recurrent stroke.
Methods
In August 2009, a systematic search for published literature was conducted of 10 key bibliographic databases including All EBM Reviews, CINAHL, Conference Proceedings Citation Index – Science, EMBASE, and MEDLINE. MeSH terms and keywords associated with ‘stroke', ‘secondary prevention’, and with the four-lifestyle behaviors, which formed the focus of the review were used to develop comprehensive searches. No currency or language delimiters were specified. Inclusion criteria specified experimental and nonexperimental study designs. Primary outcomes of interest included lifestyle behavior i.e. changes in behavior relating to tobacco use, physical activity, alcohol consumption and diet, and physiological outcomes, e.g. blood pressure, blood sugar, blood lipids, and body mass index (BMI). Secondary outcomes included psychological and learning outcomes, and recurrence of stroke and other vascular events.
Two reviewers independently assessed methodological quality using standardized critical appraisal instruments developed and used by the Joanna Briggs Institute (20). The instruments provide design-specific criteria against which to judge methodological quality, e.g. use of appropriate randomization techniques and use of appropriate analytic approaches. One point was awarded for each of the nine or 10 items listed in the individual appraisal instruments; papers scoring five or more were included in the review. Any discrepancies between reviewers were resolved consensually. Data were extracted using a review-specific data extraction form (21). Detail was sought regarding characteristics of the sample population, including information regarding the nature and severity of stroke and whether participants with aphasia were included, intervention design, delivery, and content, and primary and secondary outcomes and associated measures.
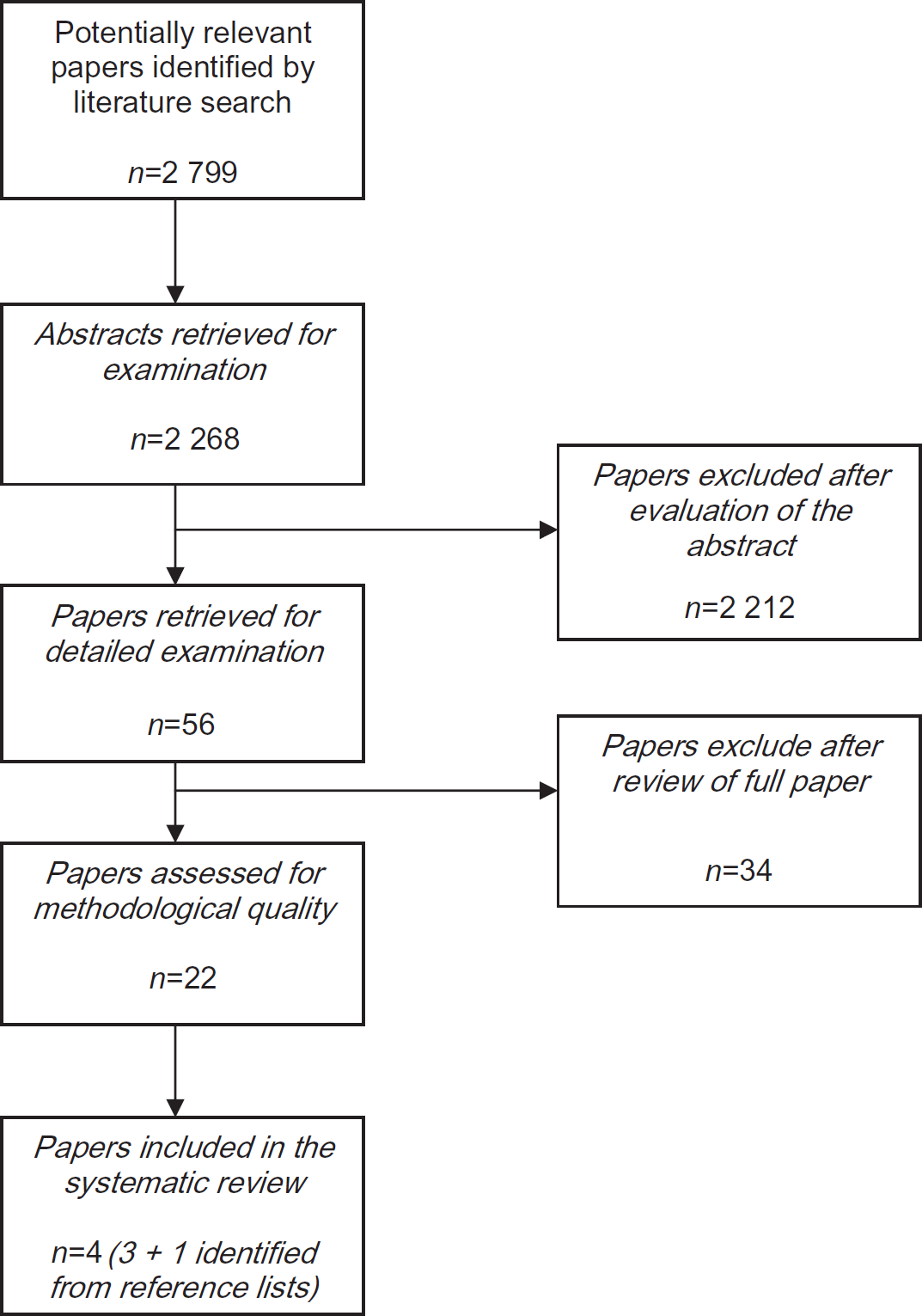
Flow chart of study selection.
Where possible, results from the studies included in the review were pooled in statistical meta-analysis. In some instances, studies reported more than one outcome for the same set of participants. These outcomes were reported independently; therefore, it was possible to pool the data as though drawn from separate populations. Where statistical pooling was not possible, findings were presented in narrative form.
Results
The searches identified 2268 unique references (Fig. 1). In stages 2 and 3, studies were excluded (n = 2246) because the study population did not meet the review inclusion criteria, e.g. the studies were concerned with cardiac or renal disease, they presented practice guidelines and recommendations, or they reported interventions that focused on motor recovery rather than secondary prevention.
Papers in languages other than English
The searches retrieved records of several papers written in languages other than English, e.g. French, Korean, Polish, and Russian. Bibliographic records included English translations of the title and abstract, which provided sufficient information to enable screening in stages 2 and 3 of the review process. No papers in languages other than English met all of the review inclusion criteria; consequently, only English language papers were included in stage 4 of the review.
In stage 4, 22 papers were assessed for methodological quality; sixteen were excluded because they failed to meet five or more design-specific methodological criteria or because the reported interventions were not designed to address behavioral change. Therefore, six papers were eligible for data extraction. At this stage, the reviewers noted that the paper by McManus et al. (22) reported follow-up trial data (42-month mean) but provided no baseline data. Rather, baseline and five-month follow-up data had been reported in a research letter by Ellis et al. (23), which had not been retrieved by the stage 1 searches. A decision was made to include both documents in the review but to treat them as one for purposes of quality appraisal, data extraction, data analysis, and reporting.
Following the data extraction process, authors of these resultant seven papers (22–28) were asked for additional information. Authors of three papers (26–28) were unable to provide the data requested, and as it was not possible to extract sufficient review-specific data to enable meaningful analysis and reporting, these papers were excluded from the review. Therefore, four papers reporting three studies (two randomized control trials (RCTs) and one quasi-experimental study) were included in the review, i.e. Joubert et al. (25), Ellis et al. (23)/McManus et al. (22), and Sit et al. (24).
The methodological quality of the three included studies (22–25) was good as they scored six or more using Joanna Briggs Institute critical appraisal instruments, although some limitations were noted. For example, Joubert et al. (25) highlighted a limitation in the random allocation to groups. Joubert et al. (25) also noted that differences between intervention group and the control group may have influenced differences in some of the 12-month outcomes. In terms of sample size, the small number of participants (n = 102) in McManus et al.'s study meant that the study was ‘relatively underpowered’ (p. 103) (22). Attrition was also a feature of the studies; however, only Sit et al. (24) and Ellis et al. (23) used intention to treat analysis.
In terms of the validity and reliability of outcome measures, smoking status was not biochemically validated in any of the studies (29). Further, participant self-report, which is known to be prone to misreporting (30), was used by Sit et al. (24) and McManus et al. (22) to measure outcomes including number of cigarettes smoked, dietary intake, medical history, and vascular recurrence.
The studies were conducted in three different countries, i.e. China (Hong Kong) (24), Australia (25), and Scotland (22,23) and involved 581 participants (baseline). Interventions were delivered to groups or in one-to-one consultations.
Joubert et al. (25) described a shared-care model (hospital and community); Sit et al. (24) and Ellis et al. (23)/McManus et al. (22) reported nurse-led models, which were delivered in the community (24) and in a hospital-based outpatient clinic (22, 23). All three interventions were of short duration; however, the length and intensity of therapeutic follow-up varied. Sit et al. (24) delivered their educational intervention in two-hourly sessions conducted weekly over the course of eight-weeks. Joubert et al. (25) evaluated a multimodal intervention that included prescription of appropriate medication, education delivered by a hospital-based stroke nurse coordinator, and frequent (five times in 12 months) follow-up with a family doctor. Ellis et al. (23)/McManus et al. (22) delivered their educational and counseling intervention in 30-min consultations held at monthly intervals over the course of three-months.
The pooled lifestyle behavior data results are significant and favor the interventions (treatment effect 2P = 0.02; note: here and throughout, 2P represents the two-tailed probability), particularly those designed to increase the frequency of deliberate walks taken for exercise (28,29) and to improve diet (28) (Fig. 2). The chi-square test for heterogeneity was not significant, which suggests similarities in the pooled variables. In terms of clinical significance, the meta-analysis demonstrates that intervention is better than no intervention and as the beneficial effect is likely to be additive, multiple interventions might be better than a single one.
In terms of physiological outcomes, the pooled results are significant (2P = 0.05) and favor the interventions, particularly those aiming to reduce blood pressure, cholesterol levels, and BMI (22,23,25) (Fig. 2). The chi-square test for heterogeneity was not significant. In terms of clinical significance, meta-analysis demonstrates that intervention is better than no intervention and because the beneficial effect is likely to be additive, multiple interventions might be better than a single one.
The pooled secondary outcomes data, including quality of life and stroke knowledge are highly significant (2P #< 0.00001) and favor the interventions (Fig. 2). The chi-square test for heterogeneity was also highly significant, which suggests large differences in the variables that have been pooled. However, as the evidence base is small and the numbers in the individual trials are limited, there is insufficient statistical power to consider them in sub-groups.
Limitations
Two methodological limitations are noted. In terms of currency, only papers published before August 2009 were included, and in terms of publication bias, searches of the gray literature were limited to only two databases, i.e. Conference Proceedings Citation Index – Science and ProQuest Dissertation & Theses. Finally, only three studies with a small number of participants were included in the review; therefore, the results reported here should be interpreted with caution.
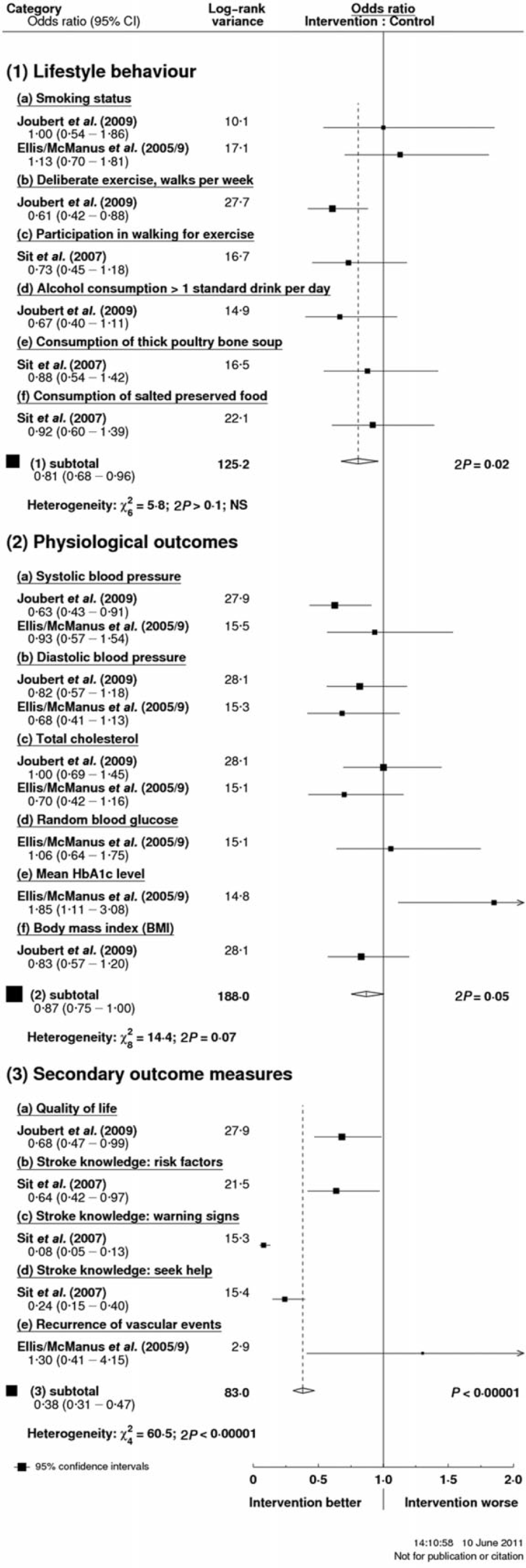
Secondary prevention lifestyle interventions: forest plots.
Conclusions
Stroke secondary prevention lifestyle interventions are effective in terms of effecting positive change in relation to lifestyle behaviors, physiological outcomes, and secondary outcomes. In particular, behavioral interventions were found to be effective in relation to increasing physical activity and improving dietary intake. In terms of physiological outcomes, interventions were found to be effective, particularly those aiming to reduce blood pressure, cholesterol levels, and BMI. In relation to secondary outcomes, intervention was seen to exert a highly significant beneficial effect, in particular with regard to improving perceived quality of life and stroke knowledge. There was insufficient evidence to determine the effect of intervention on incidence of stroke recurrence.
Recommendations for practice
Following stroke, clinicians should implement interventions to address behavior change in relation to physical inactivity, excessive alcohol consumption, and unhealthy diet, lifestyle behaviors that represent risk factors for recurrent stroke. Note that although the review evidence does not show that intervention to change smoking behavior is effective, there is strong evidence in the wider tobacco literature to indicate that clinicians should encourage patients to quit smoking and refer them to specialist smoking cessation services (31).
Following stroke, clinicians should implement interventions to address blood pressure management, cholesterol management, and BMI, physiological factors associated with lifestyle risk factors for recurrent stroke.
Note that although the review evidence does not support intervention to improve diabetic control, there is strong evidence in the wider literature, which indicates that clinicians should implement interventions that address diabetic management (32,33).
Following stroke, clinicians should implement behavioral/educational secondary prevention interventions to improve quality of life, self-perceived health status, and stroke knowledge.
Implications for research
Further large-scale, well-designed RCTs, which use appropriate objective outcome measures, are required to determine a range of issues relating to the secondary prevention of stroke, including frequency/intensity of interventions, the most effective time for initiation of secondary prevention strategies, cost-effective models of delivery, and determining whether such interventions are effective in the long term. In particular, longitudinal studies are required to determine whether secondary prevention interventions effectively reduce the recurrence of stroke and other vascular events.