
Abstract
We investigated around 100 patients for one-year and then registered the information about the possible etiology of the stroke, type of disease, treatment, localization of the clot, age, as well as gender distribution of stroke patients' population. This general overview of risk factors, ways of treatment, diagnostics, care and monitoring of the stroke patients in Armenia might serve as a cornerstone work for further highlighting of new avenues for stroke treatment.
Introduction
Total population of Armenia is 3 215 800. The country is situated in Caucasus, which is located in the heart of Western Asia and Eastern Europe.
The health policies are leaded by the Armenian Ministry of Health.
Stroke is one of the leading cause of mortality and morbidity in Armenia.
In 2011 there was created specialized stroke center in the Clinic N1, in the capital city of Armenia, Yerevan.
In accordance with the results from Department of Epidemiology and Medical Informatics of Health Ministry the percentiles of diseases related with the abnormalities of hemo circulation is equal to 8% (including stroke).
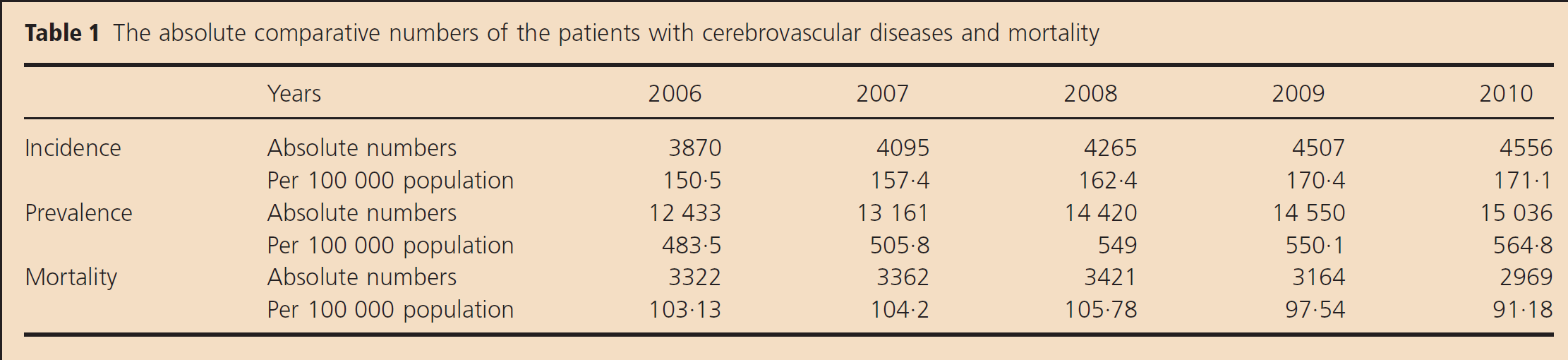
This generalization is composed from ischemic diseases of the heart (30%), others (25%), and the diseases related with the hypertension (45%). The numbers of the incidences, mortality as the absolute, as well as calculated per 100 000 population, are presented for the years 2006–2010 in Table 1 (1).
The absolute comparative numbers of the patients with cerebrovascular diseases and mortality
No modifiable (2) primary risk factor for stroke in Armenia is the age.
Age doubles the risk of stroke each decade after 50–55 years of age (3). Our experimental group of stroke patient was aged between 50 and 85 years old.
The frequency of stroke occurrence is higher in men than in women (3). Men also have generally higher age-specific stroke incidences than woman (4).
Our study group consisted from 62,9% of male patients and 37,1% of females (Fig. 1). It is necessary to mention that age dependence of male patients was broader in comparison with the female patients. The age of female stroke patients varied from 65 to 78 years old, whereas for male stroke patients it was between 52 and 85. At this point of the analysis, we acknowledge controversy with the literature, most likely due to ethnicity.
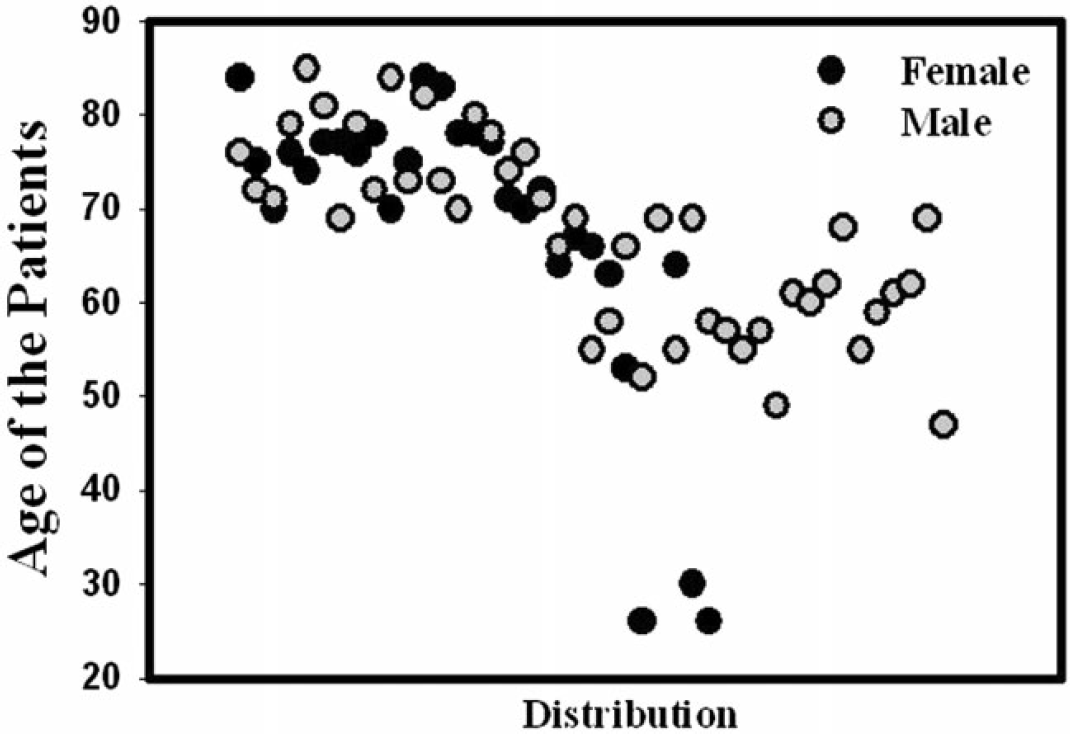
Representation of the age of stroke patients. Black cycles represent female stroke patients, whereas the grey cycles points to the age of the male patients. The age of the main population of the stroke patients varies from 27 to 83 years old.
One of the well-documented risk factors is atherosclerotic vascular disease. We included into the experimental group patients with hemorrhagic (26.76%) and ischemic strokes (73.24%) (2). The main complication in both groups was atherosclerosis (84.79%) of the cerebral and peripheral vessels (Table Table 2).
The presence of cerebrovascular disease is strongly associated with the presence of symptomatic (5) and asymptomatic (6) cardiac disease. Moreover, myocardial infarction is associated with the development of atrial fibrillation and is a source of cardiogenic emboli (7). There are other cardiac diseases, documented during investigation in Armenian population of stroke patients, which can contribute to the risk of thromboembolic stroke. It is cardiomyopathy, valvular heart disease (mitral valve prolapse, endocarditis, prosthetic cardiac valves), and intracardiac congenital defects (patent foramen ovale, atrial septal defect, atrial septal aneurysm). Investigations of patients' histories highlighted that 90,15% of the stroke patients had developed different types of cardiac diseases.
Correlation between blood pressure, cardiovascular, and stroke risk is highly significant and independent of other risk factors (9). Blood pressure, particularly systolic blood pressure, increases with the elevation of age (8). Hypertension in our study was documented in 69,01% of the patients. (Table 2).
Distribution of risk factors for stroke

Patients with hemorrhagic (26·76%) and ischemic stroke (73·24%) were included. The main complications in both groups were atherosclerosis (84·79%), diabetes (22·54%), hypertension (69·01%), pulmonary dysfunction (42·25%), and cardiac impairment (90·15%).
The lowest percentile of documented risk factor in our study belongs to diabetes mellitus and it was equal to 22.54% (Table 2).
Pulmonary infections and impairments are the other risk factors for stroke occurrence. The percentile frequency of pulmonary impairment in stroke patients was 42.25% (Table 2).
Poststroke treatment in Armenia includes the utility of drugs influencing the rennin-angiotensine system (Ramipril), calcium channels (Amilodipine), antibiotics (Ceftriaxone), analgetics (Analgin, Dimedrol), aspirin (Cardiomagnyl), compounds improving the metabolic processes (Cerebrolisyn), antioxidants (Mexidol), and drugs for the diabetic patients with stroke (Diabeton) as well as compounds minimizing blood glucose, etc. There is no treatment with the plasminogen activators including tPA (tissue type Plasminogen activator), Urokinase, Alteplase, etc.
Diagnostic imaging is generally based on the utility of computer tomography. Hopefully, in the nearest future, there will arise new possibilities for treatment of stroke patients with safer and improved thrombolytics, which will posses with the highest level of efficiency.
Acknowledgement
We are thankful to PhD students Arakelova E. and Tsakanova G. for their help in the collecting of the data. The work was supported by ANSEF biochem-2381 award.