
Abstract

Small artery infarction, which is particularly prevalent among Asians (1), carries a lower risk of recurrent stroke at one-month compared with other stroke subtypes, but long-term findings are inconsistent (2, 3). Data on subsequent myocardial infarction risk after small artery stroke are limited. We compared the incidence of vascular events following ischemic stroke due to small artery disease vs. other etiologies among prospectively recruited Asian patients admitted to the Singapore General Hospital from 2005 to 2007. Telephone follow-up at a median of 30 months (IQR 24–34) masked to clinical information was obtained for 89% of the cohort.
Among the 731 patients with known stroke etiology, 49% had small artery infarction, 38% had large artery infarction, 12% had cardioembolic, and 1% had other etiology. Figure 1 shows the cumulative incidence of subsequent vascular events. Using Cox regression adjusted for age, gender, hypertension, diabetes, hyperlipidemia, smoking, and atrial fibrillation, small artery infarction was associated with a lower incidence of recurrent stroke [hazard ratio (HR) 0·62; P = 0·047], myocardial infarction (HR 0·45; P = 0·031), vascular death (HR 0·18; P = 0·002), and composite vascular events (HR 0·59, P = 0·007) compared with nonsmall artery stroke.
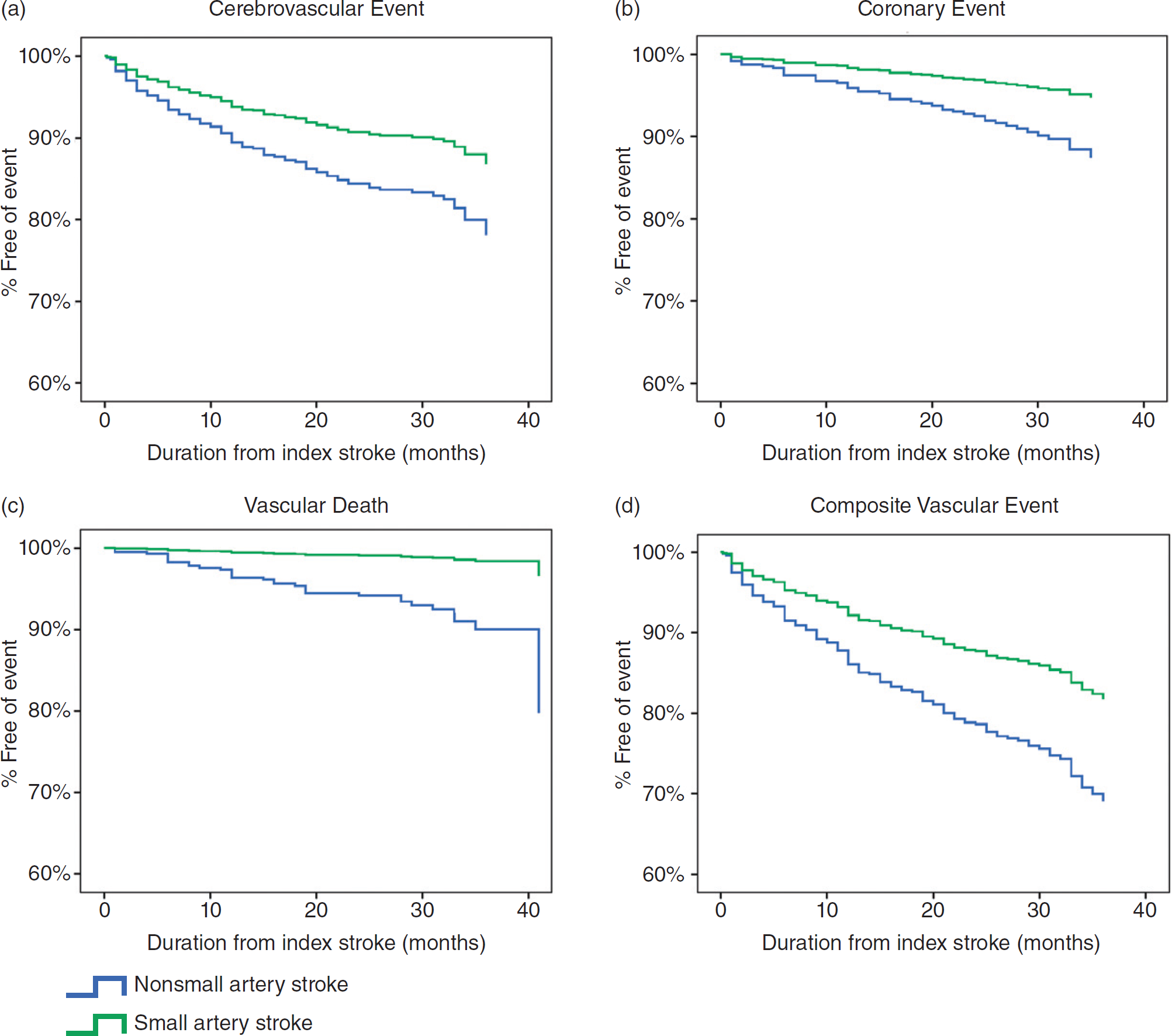
Survival-free incidence of subsequent vascular events from index stroke.
The lower risk of subsequent vascular events following small artery infarction may be explained by a differing underlying pathology from large artery and cardioembolic stroke, as suggested by autopsy (4) and retinal microvascular studies (5). Our findings provide evidence for more accurate prognostication for ischemic stroke patients based on index stroke etiology. The dissimilar prognostic profile and postulated differing pathology of small artery infarction compared with other subtypes suggest the need for targeted secondary prevention strategies. As risk reduction with secondary vascular prevention strategies may vary between small artery and nonsmall artery strokes, secondary prevention trials should consider the distribution of index stroke subtypes. Understanding the specific underlying pathogenesis of small artery infarction may lead to novel treatments targeting small artery disease.