
Abstract
Background
Despite increasing socio-economic burden of stroke, few studies have investigated the costs associated with the stroke care in Korea. We estimated the two-year direct medical costs associated with stroke.
Methods
This was a multi-centre, incidence-based, retrospective observational study. We examined the records of all adult patients who were admitted in eight large hospitals throughout Korea due to acute stroke [I60: sub-arachnoid haemorrhage; I61: intracerebral haemorrhage; I62: other nontraumatic haemorrhage; I63: cerebral infarction, by The International Statistical Classification of Diseases and Related Health Problems (ICD)-10] between 1 November and 31 December 2006. Direct medical inpatient and outpatient cost of each patient was extracted from the medical record and the reimbursement claim data of the hospital.
Results
Out of 908 studied patients (14% diagnosed as I60, 18% as I61, 3% as I62, and 65% as I63), 460 (50·7%) were assessed for more than one-year. The annual average direct medical costs were Korean ₩ 8 114 471 US$8732) for the first year, and Korean ₩ 431 527 for the second year. The first year costs for haemorrhagic stroke (I60–I62) (Korean ₩ 13 090 179) were significantly higher than those associated with cerebral infarction (I63) (Korean ₩ 5 460 459), whereas the second year costs were not different. Factors independently associated with high cost were female gender, young age, and first stroke.
Conclusions
Direct medical costs for stroke in Korea were determined, which seem to be lower than those of other developed countries. Female gender, young age, and first stroke were factors related to higher stroke cost.
Stroke is a major cause of death and disability worldwide, and imposes significant economic burdens to many countries (1). Thus, healthcare plans must include adequate primary and secondary prevention strategies and quality control of treatments for stroke (2,3). In this regard, proper estimates of the cost-effectiveness of interventions are needed so that effective healthcare policies can be implemented, and this requires accurate assessment of total costs (4).
Many countries have investigated and published the healthcare costs for prevention and treatment of stroke (5,6), thereby providing a basis for cost-effective analysis and healthcare policy. In Korea, however, there have been few studies on stroke cost, one prevalence-based study (7) and, the other, a single hospital based study (8). So far, there have been no English-language reports of the costs associated with stroke in Korea, making international comparisons difficult.
Korea is a rapidly aging society with the aging index (proportion of people older than 65 years vs. those younger than 15 years) being 34·3 in 1999 and 63·5 in 2009 (9). As the elderly consumes more medical resources, there has been a sharp rise in healthcare expenditures in Korea, with an annual increase of 8·7% in the past 10 years, significantly higher than the 4·1% average of other Organization for Economic Cooperation and Development (OECD) countries (10). Therefore, there is an urgent need for more effective control of diseases occurring in the elderly in Korea.
Stroke, a typical neurological disease of the elderly, is the second leading cause of death in Korea. Considering the significance of stroke as a disabling disease exerting enormous socio-economic impact, the establishment of strategies for the prevention and treatment of stroke should be one of the most important healthcare priorities. The accurate assessment of the costs associated with stroke care could serve as the basis for such policymaking. We therefore attempted to assess the costs incurred for stroke treatment and care in Korea. We also wished to find factors related to the cost. For this purpose, we used an incidence-based approach to evaluate costs in eight tertiary hospitals of large Korean cities.
Methods
Subjects
A retrospective, incidence-based approach was used to determine all medical costs of patients during a certain period of time after onset of stroke. The subjects were all adults (>18 years.) who were admitted to participating hospitals during November and December of 2006 with a primary diagnosis of acute stroke within one-month of onset [ICD 10 code: I60, sub-arachnoid haemorrhage (SAH); I61, intracerebral haemorrhage (ICH); I62, other nontraumatic haemorrhage; I63, cerebral infarction]. Eight tertiary hospitals from six largest nationwide metropolitan cities (Seoul, Busan, Incheon, Daegu, Daejon, Kwangju, in the order of population; total population: 21 852 457 in 2009) were selected. These are well-known, representative hospitals covering population in each city.
The records of patients who were admitted with primary diagnoses of the corresponding ICD codes during the study period were extracted from the hospital databases. Patients with first-ever and recurrent stroke were both included. Patients were excluded if:
stroke was not the main reason for admission
they were transferred to another hospital within 24 h of visiting a hospital as only the emergency costs are likely to be incurred in these patients
they had other conditions that might have significantly influenced medical costs, such as concomitant active cancer (ICD-10 C00∼C97, D00∼D09, D37∼D48), or
they were enrolled in clinical trials that supported some of the costs (i.e., costs of magnetic resonance imaging). However, patients who were enrolled in observational studies with no cost support were included.
One stroke neurologist from each hospital reviewed the medical records to confirm the primary diagnosis and to examine whether enrolled patients met inclusion/exclusion criteria.
Cost categories and assessment
The clinical profiles of patients, including primary and secondary diagnoses, investigation and treatment profiles, death, and direct medical costs for admission and outpatient visits for two-years after onset, were derived from hospital records. It was assumed that all costs were due to primary stroke management and prevention, regardless of the department of admission or concomitant diagnosis. When patients were transferred to another hospital or lost to follow-up after discharge, costs were calculated assuming that they remained in the same hospital and had the same visitation frequency as other stroke patients, unless they died.
Direct medical costs were assessed from the health insurance claim electronic database of each hospital. In the mainly socialized healthcare system of Korea, the government is the only health insurance supplier, and all the Korean people are obligated to subscribe to this health insurance system. The government determines not only which service items to be covered by insurance but also the price of those items, which is uniform in all the hospitals in Korea including large referring hospitals or family clinics. Thus, reimbursement claim data from each hospital virtually cover all direct medical costs, and each claim data are investigated and approved by the Health Insurance Review and Assessment service, which is a subdivision of Ministry of Health and Welfare of Korea (11). The total direct medical costs were classified as inpatient or outpatient (based on admission status) and reimbursed or nonreimbursed (based on insurance coverage). This study was approved by the Institutional Review Board of each hospital.
For statistical analysis, SPSS v.17·0 (SPSS Inc., Chicago, IL, USA) was used. For comparisons of the costs of groups, t-tests and analysis of variance, with the significance level of 0·05, were performed.
Results
During the two-month study period, a total of 1103 patients were admitted to the participating hospitals with primary diagnoses of stroke, 195 patients were excluded based on the criteria described above, and direct medical costs were assessed for the remaining 908 patients. Table 1 shows the characteristics of enrolled patients, which were comparable to those of previously published Korean stroke registry data (12). The mean age was 62·9 years, and 507 of the patients (55·8%) were male. A total of 460 patients (50·7%) were followed more than a year, and 81 patients (8·9%) died during the study period. A total of 594 patients (65·4%) had ischaemic stroke, and 137 patients (15·1%) had recurrent stroke. Most patients (89·3%) were admitted via the emergency room.
Demographic and clinical characteristics of patients, number and (%)
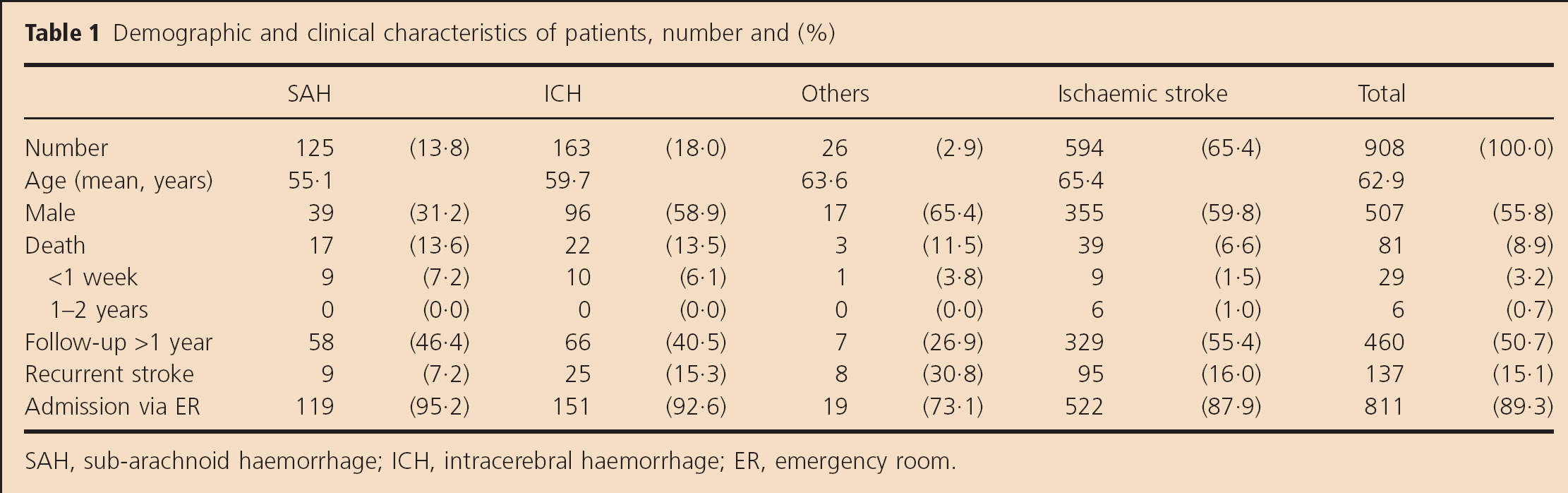
SAH, sub-arachnoid haemorrhage; ICH, intracerebral haemorrhage; ER, emergency room.
Table 2 presents the direct medical costs for stroke, based on patient characteristics. The total two-year cost was Korean ₩ 8 545 998 (US$9196 by the 2007 currency exchange rate and US$12 289 by the 2007 purchasing power parity). The cost was Korean ₩ 8 114 471 for the first year and Korean ₩ 431 527 for the second year. Between the stroke sub-types, SAH was associated with the highest cost, followed by ICH, others, and ischaemic stroke.
Direct medical costs of different sub-groups of stroke patients, in Korean ₩
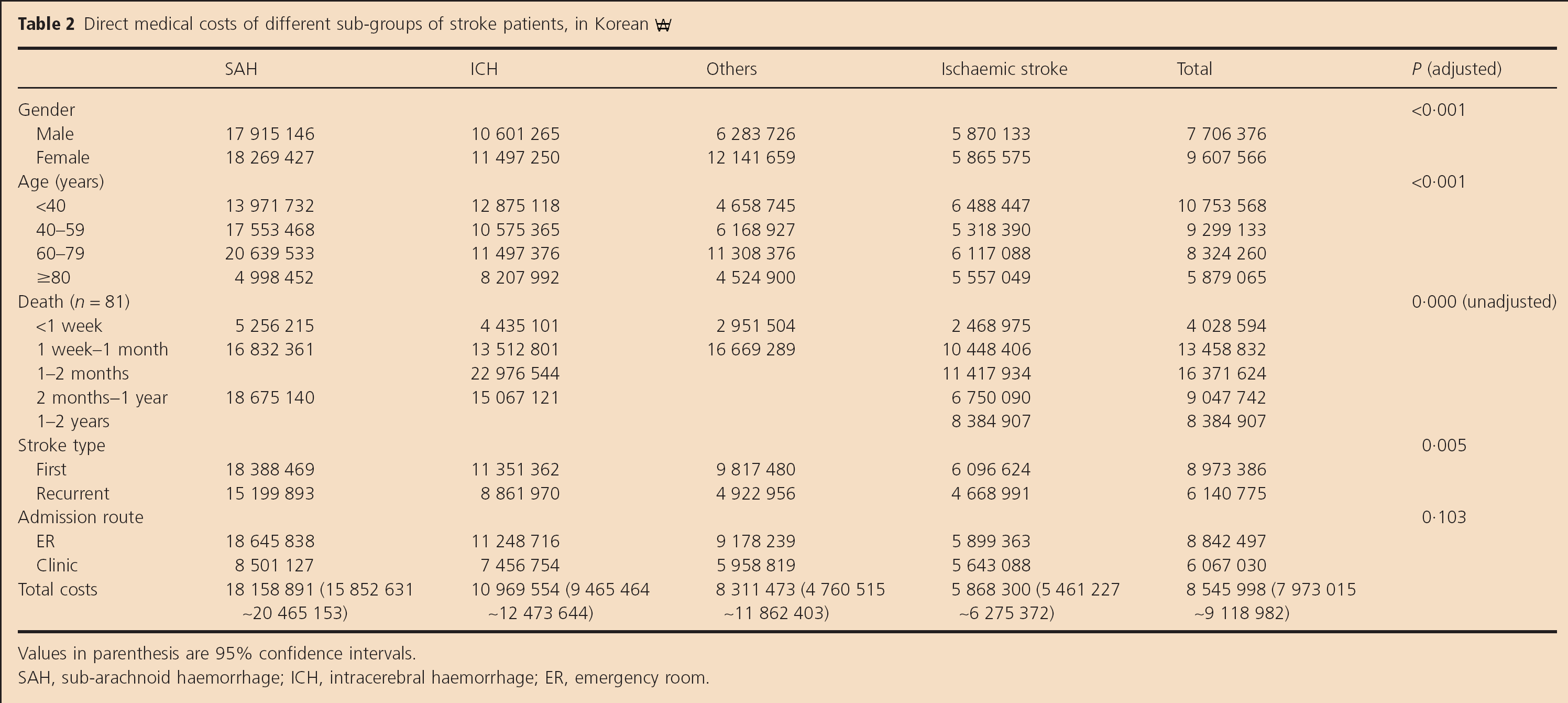
Values in parenthesis are 95% confidence intervals.
SAH, sub-arachnoid haemorrhage; ICH, intracerebral haemorrhage; ER, emergency room.
Univariate analysis showed that factors associated with high cost were: female gender, young age, and death about one-month from onset, first stroke, and admission via an emergency room. Multivariable analysis adjusted for these factors (age, gender, first stroke, and admission route), indicated that female gender, young age, and first stroke were independently associated with high costs. The first year cost was mostly caused by admission (96·1%), and this admission cost in the second year decreased to 43·8% (Table 3). The percentage of nonreimbursed costs was 25·2% in the first year and 22·5% in the second year. These nonreimbursed items are determined by the government as described earlier, especially when the costs are too high to afford, such as ultrasonography or off-label use of expensive treatments. In those cases, the patients or relatives have to pay for the costs. The mean number of admissions and in-hospital duration was 1·1 per year and 20·5 days for the first year, and the mean number of outpatient visit was 5·2 per year.
Direct medical costs according to stroke sub-type, year, management type, and health insurance coverage (in Korean ₩)
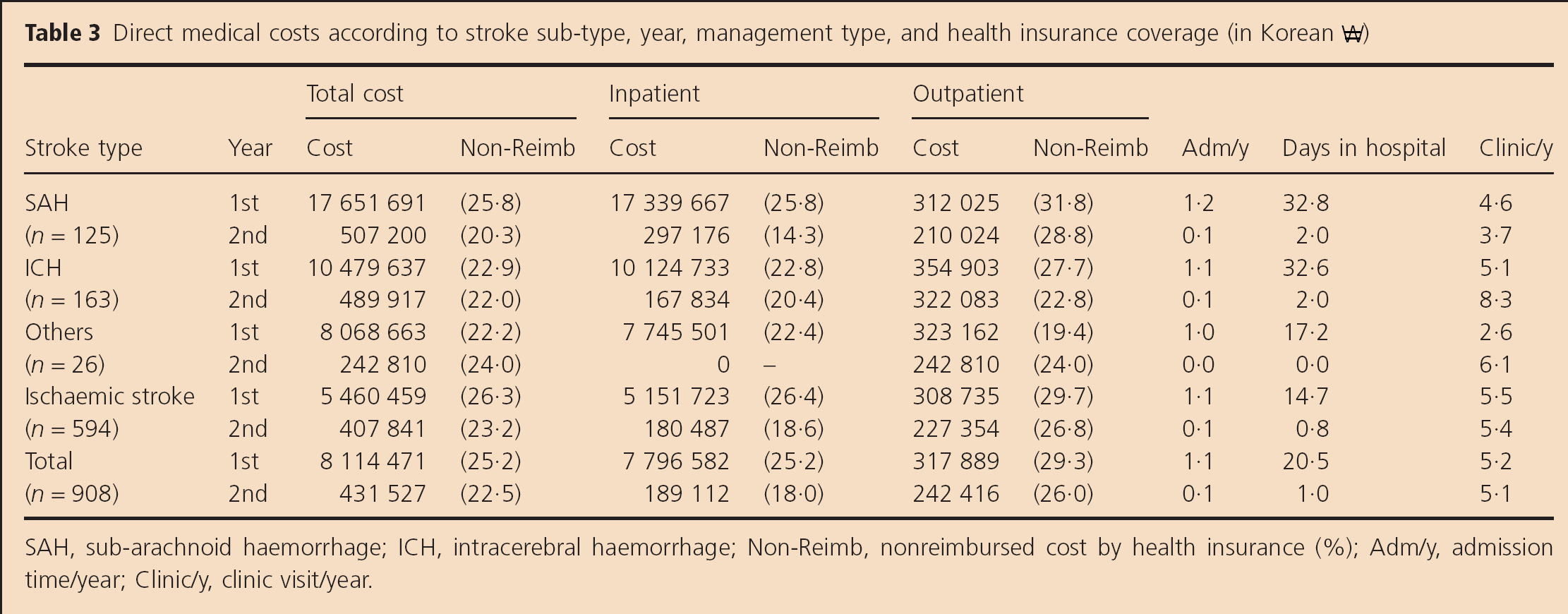
SAH, sub-arachnoid haemorrhage; ICH, intracerebral haemorrhage; Non-Reimb, nonreimbursed cost by health insurance (%); Adm/y, admission time/year; Clinic/y, clinic visit/year.
Among the patients who were followed for more than one-year (n = 460, 50·7%), 320 patients (35·2%) were followed at the first hospital for full two-years. Patients with ischaemic stroke had the highest follow-up rate (41·2%), followed by those with ICH, SAH, and other types of stroke (Fig. 1). When we compared the related factors (age, gender, first stroke, stroke sub-type, admission route) between the patients who were followed more than one-year and those who were not, there were no differences in the gender (male 58 vs. 53·6%), first stroke (83·9 vs. 85·9%), and admission via emergency room (87·6 vs. 91·1%). However, patients followed more than one-year were younger (61·0- vs. 64·9-year-old, P < 0·001) and more often had ischaemic stroke (71·5% vs. 59·2%, P < 0·001).
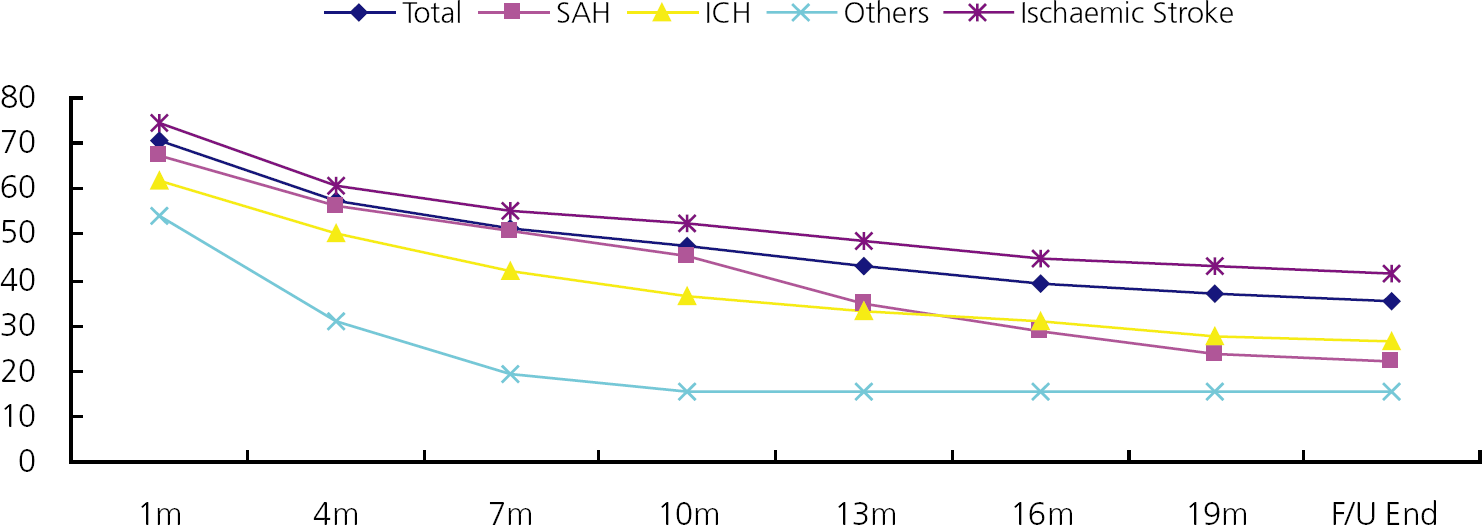
Duration of follow-up for different sub-types of stroke. ICH, intracerebral haemorrhage; SAH, sub-arachnoid haemorrhage.
Costs according to service provided in the first year were due to surgical procedure (23·5%), admission fee (22·7%), imaging (17·7%), injections (13·6%), laboratory services (12·8%), rehabilitation (3·9%), and clinical examination (1·8%). In the second year, the most significant costs were for imaging (20·4%), clinical examination (20·3%), laboratory services (16·5%), admission fee (11·1%), injections (10·3%), rehabilitation (8·2%), and surgical procedure (6·2%). The different stroke sub-types were associated with different patterns of resource use (Fig. 2).
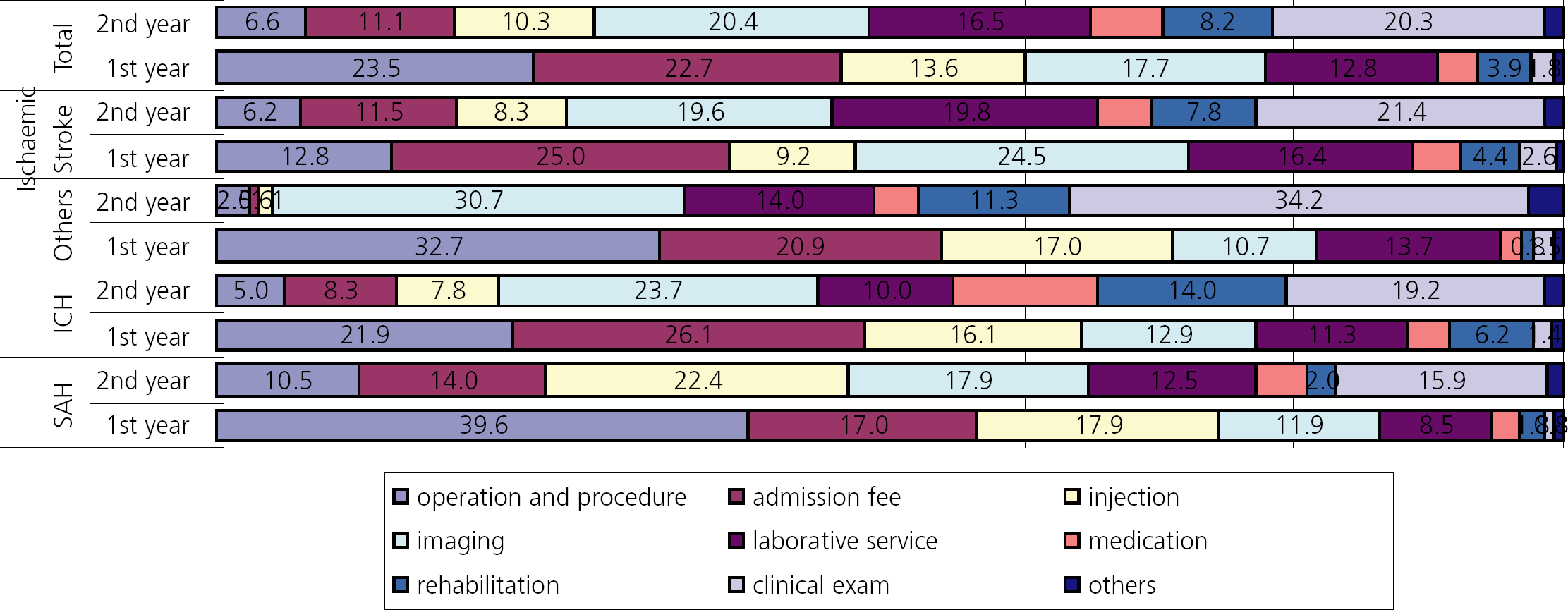
Costs associated with stroke care according to services provided (in percentage). ICH, intracerebral haemorrhage; SAH, sub-arachnoid haemorrhage.
Discussion
This is the first nationwide multi-centre study to investigate the direct medical costs of stroke in Korea using an incidence-based approach. We found that the cost for the first year (Korean ₩ 8 114 471) was significantly higher than that for the second year (Korean ₩ 431 527), and that the cost for haemorrhagic stroke (Korean ₩ 18 158 891 for the SAH and 10 969 554 for ICH) was higher than that for ischaemic stroke (Korean ₩ 5 868 300). This overall pattern is similar to previous studies (5,6). Most medical resources are consumed during the first year, especially during hospitalization for evaluation, acute care, and rehabilitation. After the first year, the annual medical costs, which are mostly related to secondary prevention, became lower.
The higher cost for haemorrhagic stroke may be related to the fact that strokes in this sub-group are more severe and more often treated by surgery than ischaemic strokes. However, the difference in cost was not significant for the second year. A recent Australian study (North-East Melbourne Stroke Incidence Study) reported that when the cost of stroke is measured for more than three-years, the annual medical costs associated with ischaemic stroke exceed those associated with haemorrhagic stroke (13), suggesting that the lifetime costs associated with ischaemic stroke may exceed those associated with haemorrhagic stroke. The relative increase in cost after the first year in ischaemic stroke may be related to the fact that patients need more expensive secondary preventive measures such as antithrombotic or antidiabetic agents.
Our results are somewhat different from those of a recent prevalence-based Korean study that analysed national health insurance claim data (7). This study included direct and indirect medical costs and reported that the total national cost of stroke care (882 143 patients) was Korean ₩ 3737 billion in 2005, which is 2·2% of the total national healthcare costs. This corresponds to a per capita annual cost of Korean ₩ 2 685 559 (Korean ₩ 6 847 128 for haemorrhagic stroke and Korean ₩ 2 632 593 for ischaemic stroke). As it was estimated that the indirect medical costs were more than double the direct medical costs, the direct annual medical cost per patient would be less than Korean ₩ 1 000 000. In this study, the ICD 10 code system used for claim data could not discriminate between acute and chronic stages of stroke, and only average annual costs were calculated. Thus, the data are not comparable with our incidence-based study results. Another Korean study using an incidence-based approach in a single hospital in 2002 reported that the first year cost after acute ischaemic stroke was Korean ₩ 5 235 000 (8) which is similar to our calculated first year cost for ischaemic stroke (Korean ₩ 5 444 505).
A comparison of our results with those of other countries indicates that the first year cost of stroke in Korea (Korean ₩ 8 114 471, equivalent to US$8732 in 2007), is much lower than the international mean cost of stroke (US$19 018) determined from 71 studies (6). Although direct comparison would be difficult owing to differences in methodology (i.e., follow-up period, stroke type, and cost categories), the following costs have been reported for stroke in other OECD countries/regions: Western Europe US$9438, Japan US$12 883, and USA US$28 253. After consideration of per capita income (US$19 751 in 2007) and purchasing power parity (US$757 in 2007), stroke cost in Korean patients seems still low.
There are several possible explanations for this. First, the total national health expenditures of Korea (Korean ₩ 50 990 billion, which corresponds to US$42 billion) and its proportion of the gross domestic product (5·6% compared with an OECD average of 8·1%) (10) are smaller than those in other OECD countries partly due to the socialized medical insurance system of Korea, which strictly regulates the healthcare budget. Second, care after a stroke in Korea is generally provided by family caregivers and this cost was not counted as a direct medical cost, whereas caregivers in many other OECD countries belong to institutes and the cost can be included in the direct medical cost. Unfortunately, direct nonmedical costs were not analysed in our study due to poor response rate as described later. Finally, for the loss of patients during follow-up, we developed simulation model under the assumption that lost patients were not re-admitted to another hospital during the follow-up period and consumed only average monthly cost of the other follow-up patients. This conservative approach might have resulted in an underestimation of the true cost.
In the present study, costs were greater for females than male patients. Previous studies reported similar results and attributed this difference to the greater severity of stroke in women (14,15). However, there also were contradictory results (16). In our study, the gender difference in costs was not evident in those with ischaemic or haemorrhagic stroke, but was evident in those with other stroke sub-types. The reason for this observed gender difference remains unclear. Our study also showed greater costs for young stroke patients. This may be due to the relatively extensive investigation for aetiology identification and the aggressive treatment of young stroke patients. In agreement with our results, an Italian study investigating the six-month cost for stroke reported that costs were higher for young vs. elderly patients (17). The reason for the higher cost in the first vs. recurred stroke could also be related to more extensive aetiological work-up in patients with first stroke. In addition, our analysis showed tendency of higher costs for patients who died about one-month from onset and who were admitted via emergency room. Both of these items could be indicators of more severe stroke, which is known to be associated with greater cost (15,18,–20). As we could not precisely analyse stroke severity with this retrospective design, we were not able to demonstrate this association clearly here.
There are several limitations in our study. First, many patients were lost to follow-up during the study, and cost assessment for more than one-year was available for 50·6% of patients only and the costs for the other patients were based on the simulation model as described earlier. As those patients who were followed more than one-year were younger and more often had ischaemic stroke, these differences might have influenced the total costs. However, young age and ischaemic stroke sub-types were factors influencing the cost to the opposite direction, and, indeed, the resulting costs (Korean ₩ 8 433 536 for those who were followed >1 year vs. 8 661 473 for those who were not) were not significantly different. Also, the difference of costs between the simulation model and the original observation was only 2·8% (Korean ₩ 8 545 998 for the simulation vs. 8 307 830 for the observation). Therefore, it seems that potential cost difference caused by different follow-up duration is not great.
Second, we could not analyse direct nonmedical and indirect medical costs. Actually, we initially attempted to assess those costs by using a structured questionnaire performed by trained clinical research coordinators, and about 50% of patients or family members agreed to be interviewed. However, as this research was conducted three-years after the index stroke, most of them could not precisely remember cost details, and only 29 patients (6·0%) gave reliable responses. Thus, the direct nonmedical costs and indirect medical costs could not be analysed.
Third, our study was conducted in tertiary hospitals in large cities, and the costs may have been overestimated due to extensive investigation, strict secondary prevention strategies, or admission of patients with relatively severe strokes. However, this bias may not be great because a recent survey indicated that more than 90% of the population of Korea now live in urban areas (9), and it is very unusual for the family doctors or community clinics to care for the acute stroke patients in Korea. Therefore, the participating hospitals can be regarded as typical setting of stroke care. Fourth, patients were enrolled during a specific time of the year, and may not represent stroke patients in general. Although we admit this limitation, we found that general characteristics of patients (sub-types, age, gender) were comparable to Korean stroke registry data (12) and national statistics (9). Finally, in this retrospective study, we could not evaluate certain clinical factors related to increased cost, such as neurologic severity or spasticity (21). Further prospective studies that also consider clinical factors and indirect costs are needed for more comprehensive evaluation of the cost of care for stroke.
Despite these limitations, our study provided first reliable data of stroke cost in Korea through multi-centre, incidence-based approach. These results may be used in cost-effectiveness analysis and implementation of healthcare policies by the government, health administrators, or clinicians in this country.