
Abstract
Background
Although the established measure of disability post stroke, the modified Rankin Scale emphasizes motor function and may underestimate the importance of cognitive impairment in more disabled patients. A subset of four items from the National Institutes of Health Stroke Scale has been proposed to assess cognitive function after stroke (Cog-4), and to correlate with modified Rankin Scale. Items correspond to orientation, executive function, language, and inattention. We investigated responsiveness of Cog-4 to treatment with thrombolysis and whether it offers information that supplements modified Rankin Scale.
Methods
We included 6268 patients from the Virtual International Stroke Trials Archive: 2734 received intravenous thrombolysis and 3534 were treated conservatively. We compared day 90 outcomes between treated and untreated groups, by modified Rankin Scale (illustrative) and by Cog-4 (primary measure) adjusting for age, baseline National Institutes of Health stroke scale, hemispheric lateralisation as well as baseline Cog-4 and baseline National Institutes of Health Stroke Scale excluding baseline Cog-4 separately. Analysis of Cog-4 was repeated within strata of 90 day modified Rankin Scale. Statistical analyses included proportional odds logistic regression and Cochran–Mantel–Haenszel test.
Results
Modified Rankin Scale showed a difference between treatment groups of expected magnitude (odds ratio 1·56; 95% confidence interval 1·43–1·72; P < 0·001). After adjustment for imbalance in baseline prognostic factors, the distribution of Cog-4 scores at 90 days was better in thrombolysed patients compared with nonthrombolysed patients (odds ratio 1·31; 95% confidence interval 1·18–1·47; P = 0·006). However, Cog-4 analysis stratified by 90-day modified Rankin Scale was neutral between treatment groups (OR 1·01; 95% CI 0·90–1·14), and Cog-4 was not responsive to treatment group even within modified Rankin Scale categories 4 and 5 despite substantial cognitive deficits in these patients.
Conclusion
Although Cog-4 may be responsive to treatment effects, it does not provide additional information beyond modified Rankin Scale assessment.
Introduction
Cognitive impairment is a common consequence of stroke (1–3). It is an independent predictor of adverse outcome and is closely associated with disability and dependency after stroke (3–6). To measure functional impairment as an outcome of stroke, the modified Rankin Scale (mRS) assessment is well established. This is the most prevalent outcome measurement in stroke trials investigating treatment effects with thrombolysis. However, its emphasis lies on the assessment of physical functions, whereas cognitive impairment might be underrepresented: a patient who after a stroke is still able to walk with a stick but cognitively severely impaired presumably would get a better (i.e. lower) mRS score than a wheelchair-ridden stroke patient who otherwise is mentally fit and capable of making his own decisions. In addition, the effects of stroke treatment with thrombolysis on cognitive impairment have been poorly explored, as common screening tools for assessment of cognitive function such as the Mini Mental Status Examination (MMSE) and the Montreal Cognitive Assessment are not routinely assessed during the acute phase of stroke: information about cognitive impairment as immediate consequence of stroke is often missing.
A tool routinely used to assess impairment in the acute phase of stroke is the National Institutes of Health Stroke Scale (NIHSS). Cumming et al. have suggested the use of a subset of the NIHSS to assess cognitive function after stroke based on four NIHSS items corresponding to orientation, executive function, language, and inattention, calling it Cog-4. They found it to be almost as good as the MMSE in detecting cognitive impairment and suitable for assessment of cognitive function in the absence of other dedicated measures of cognition (7).
Subsequently, Bath et al. used the Cog-4 subscale as a measurement of poststroke cognitive function, investigating its correlation to baseline clinical factors. They found post-stroke cognitive impairment at three-months was associated with increasing age, stroke severity and left hemispheric involvement (8).
As these findings imply that the Cog-4 subscale may be suitable for the assessment of cognitive function after stroke, we sought to address the question whether it is sensitive to effects of treatment with thrombolysis on functional outcome beyond those captured by the mRS assessment (9). Particular attention was paid to the more disabled patients, i.e. mRS subcategories 4 and 5: even severe motor deficits might be functionally less disabling in the absence of cognitive impairment. Assuming the Cog-4 adds information to the mRS assessment, it should then reveal treatment effects even within mRS subcategories. Our aim was to investigate if the Cog-4 is responsive to treatment with thrombolysis and whether significant differences can be observed comparing thrombolysed patients with nonthrombolysed patients within each mRS subcategory.
Methods
We collected anonymized data from 6268 stroke patients held within the Virtual International Stroke Trials Archive (VISTA) (10). This is a collaborative, not-for-profit compilation of stroke trial datasets. Analysis included 2734 patients who received treatment with intravenous thrombolysis and 3534 patients who were treated conservatively. Reasons for conservative treatment could include absence of marketing approval for alteplase at the time and in the location of treatment or clinical factors that militated against use of alteplase. A subset of four items corresponding to orientation, executive function, language, and inattention was extracted from the 90-day NIHSS recording to generate the Cog-4 score as a cognitive outcome measure [Cog-4 at 90 days (Cog4_90)]. Patients who did not survive until follow-up visit at 90 days after stroke onset (score of 6 at the mRS at 90 days; Cog4_90 missing) were excluded. Ranging from a minimum score of 0 to a maximum score of 9, the Cog-4 scale was considered ordinal (i.e. the lower the score the better the cognitive outcome) rather than categorical (i.e. uncertain order of better versus worse). However, we recognize there is not a strict relation between degree of impairment and the final score: The Cog4 score is not normally distributed, being skewed toward low scores.
We compared baseline clinical factors between the thrombolysed and the conservatively treated group. To investigate the effect of thrombolysis treatment on outcome, we used proportional odds logistic regression and expressed results as odds of better outcome with treatment, with 95% confidence intervals. Cochran–Mantel–Haenszel statistics were applied to define P values for the comparison of ordinal distributions. To validate our dataset, we confirmed the direction and extent of the difference between treatment groups on mRS score at 90 days [mRS at 90 days (mRS90)]. Our primary analyses of group differences in cognitive outcome were based on the Cog4_90, after adjustment for age, baseline stroke severity (baseline National Institutes of Health Stroke Scale = BNIHSS, continuous variable), side of stroke [left hemispheric involvement (LHI)], and both baseline Cog-4 (COG4_BASE) and baseline NIHSS excluding baseline Cog-4 (BNIH_SUB). Analyses of cognitive outcome were first conducted in the entire dataset and then repeated with stratification for mRS90 and examined independently within each separate mRS outcome subcategory to investigate whether treatment group differences on Cog4_90 supplement those reflected by mRS.
All statistics were conducted with SAS 9·2 (SAS Institute Inc., Cary, North Carolina, USA) and Minitab 15 (Minitab Inc., State College, Pennsylvania, USA) software.
Results
Stroke patients collected from VISTA had been managed according to stroke guidelines acceptable at the point of their treatment. NIHSS scores at 90 days and thus the derived Cog-4 scores were available for all 6268 surviving patients.
Baseline factors favored untreated patients (Table 1).
Baseline clinical factors for treated vs. untreated patients
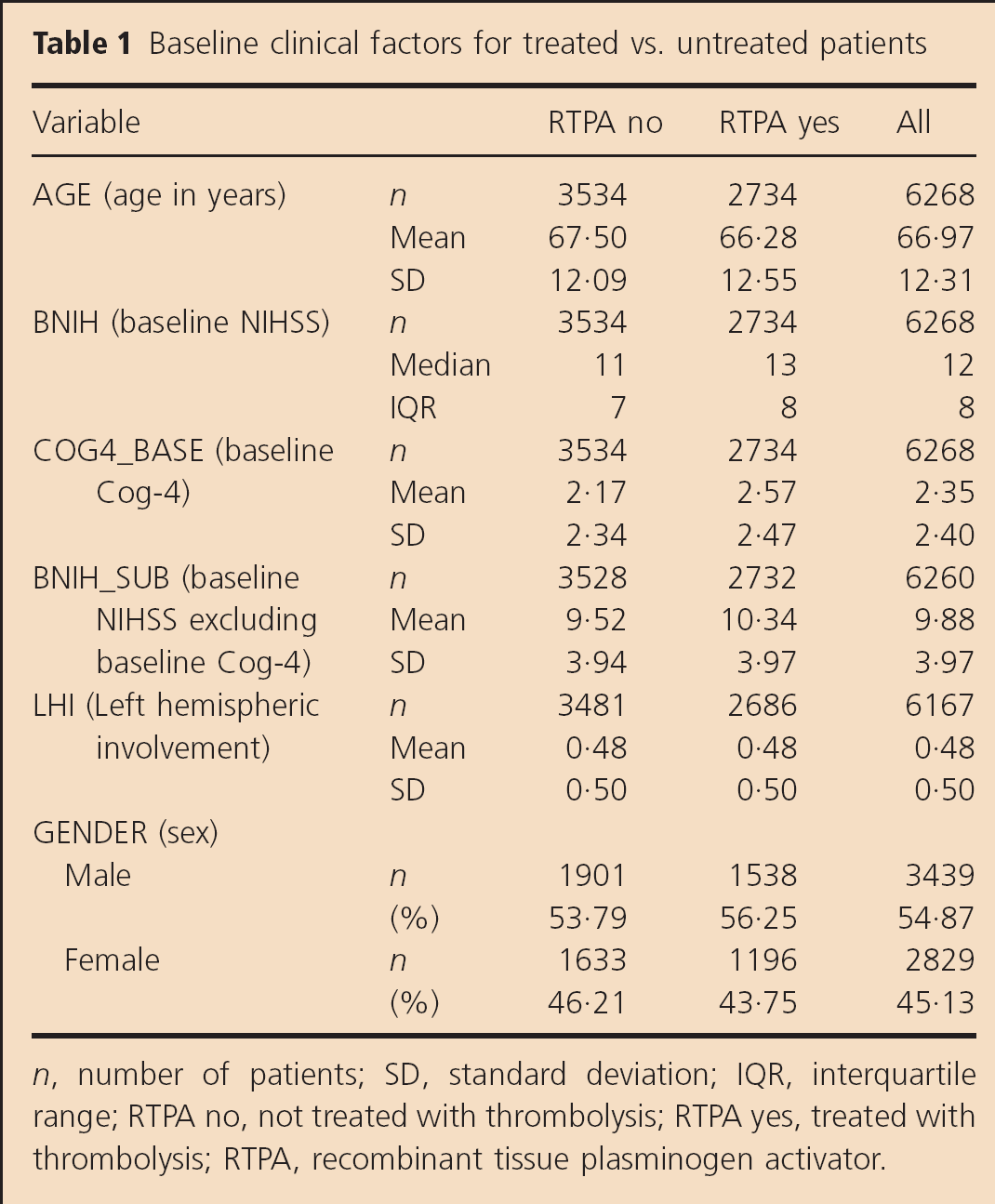
n, number of patients; SD, standard deviation; IQR, interquartile range; RTPA no, not treated with thrombolysis; RTPA yes, treated with thrombolysis; RTPA, recombinant tissue plasminogen activator.
For analyses of functional outcome, both unadjusted and adjusted analyses showed favorable outcome (i.e. lower mRS90 scores) with thrombolysis [unadjusted: odds ratio (OR) 1·24; 95% confidence interval (CI): 1·13–1·35; P < 0·001; adjusted: OR 1·57; 95% CI: 1·43–1·72; P < 0·001].
Unadjusted analysis of Cog4_90 across all patients (mRS90 = 0–5) was equal for the thrombolysed and the conservatively treated groups (OR 0·99; 95% CI: 0·90–1·09; P = 0·73). However, after adjustment for baseline imbalance in prognostic factors, Cog4_90 was better among thrombolysed than comparator group patients (OR 1·31; 95% CI: 1·18–1·47; P = 0·006). Within the stratified analysis, testing for a supplemental contribution of Cog-4 beyond that detected by mRS, there was no difference in Cog4_90 between the thrombolysed and the conservatively treated groups (OR 1·01; 95% CI: 0·90–1·14; P = 0·669). Cog-4 showed a ceiling effect, with mainly normal scores among patients with mRS 0–2, and the underlying hypothesis was that mRS categories 4 and 5 emphasize motor functions over cognitive deficits. We therefore examined intergroup Cog-4 distributions within each mRS outcome category. There was no evidence of a treatment group difference in Cog-4 at any level of mRS (Table 2, Fig. 1).
Odds ratios (ORs), 95% confidence interval (CI) limits, and P values for functional outcome [modified Rankin Score at 90 days (mRS90)] or cognitive outcome (Cog-4 at 90 days) for analysis in whole sample (mRS90 = 0–5) and in each mRS subcategory
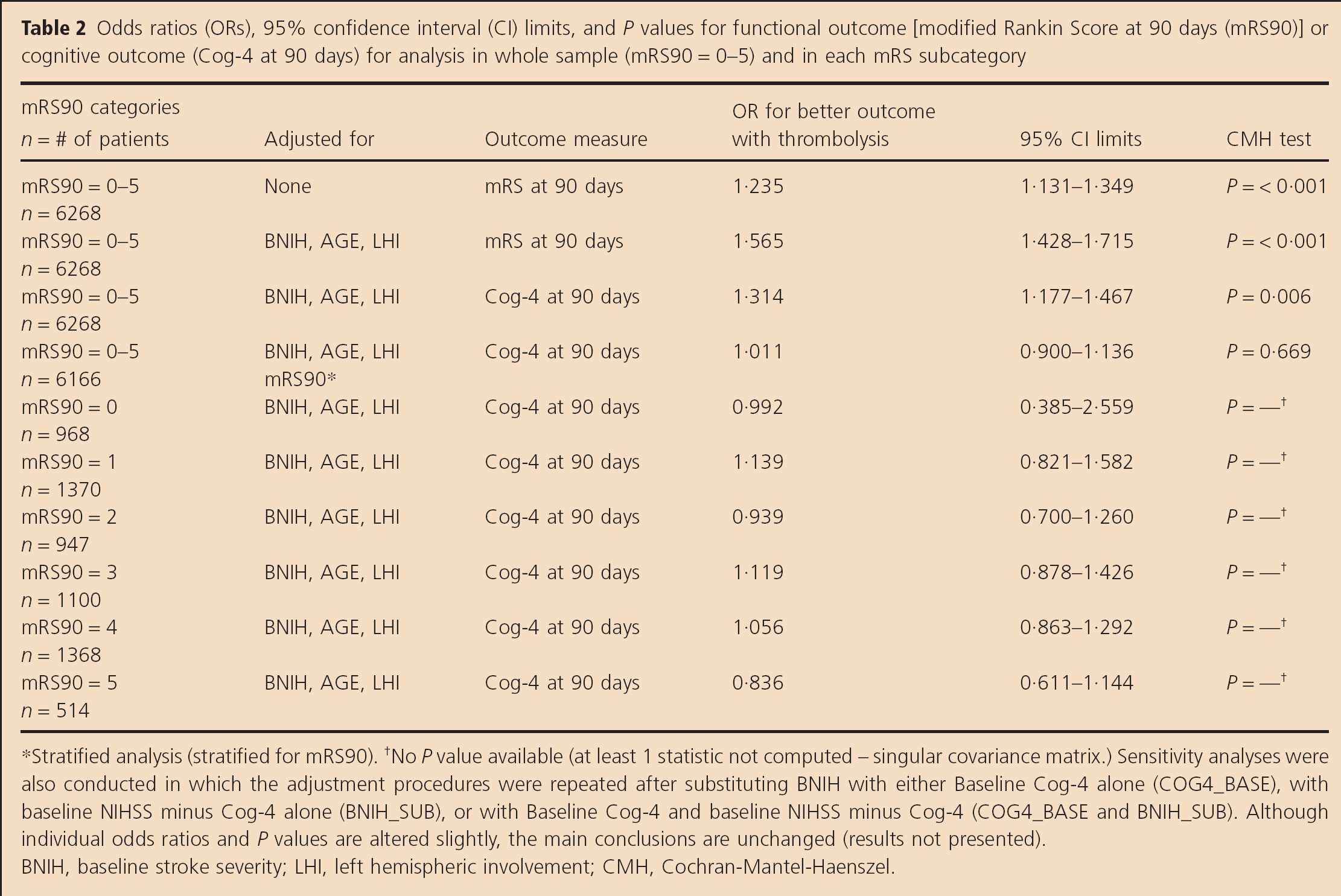
Stratified analysis (stratified for mRS90).
No P value available (at least 1 statistic not computed – singular covariance matrix.) Sensitivity analyses were also conducted in which the adjustment procedures were repeated after substituting BNIH with either Baseline Cog-4 alone (COG4_BASE), with baseline NIHSS minus Cog-4 alone (BNIH_SUB), or with Baseline Cog-4 and baseline NIHSS minus Cog-4 (COG4_BASE and BNIH_SUB). Although individual odds ratios and P values are altered slightly, the main conclusions are unchanged (results not presented). BNIH, baseline stroke severity; LHI, left hemispheric involvement; CMH, Cochran-Mantel-Haenszel.
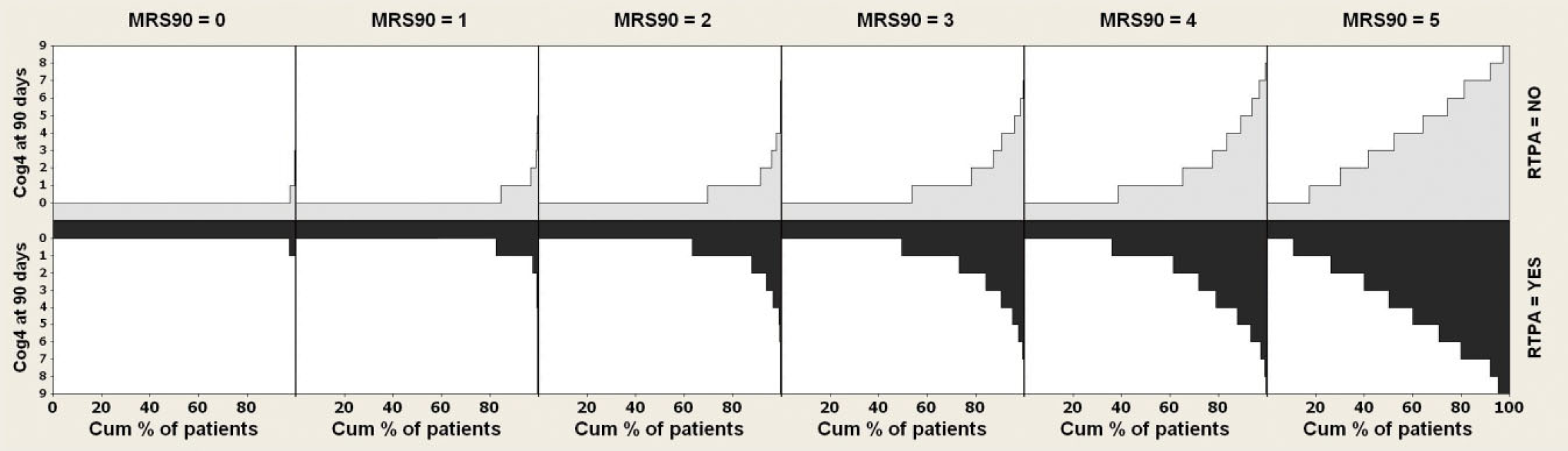
Distribution of Cog-4 at 90 days (y-axis) by cumulative percentage of patients (x-axis), nonthrombolysed (above) vs. thrombolysed (below), for each mRS subcategory (mRS90 0–5). MRS, modified Rankin Scale; RTPA, recombinant tissue plasminogen activator.
Discussion
The mRS has become the standard outcome measure for stroke trials but attracts criticism for emphasizing mobility at the expense of cognitive function. The Cog-4 subset of NIHSS terms has been proposed as a simple means to assess cognitive function and has the attraction of being already available in many previous trial datasets. Cog-4 correlates with mRS (8). We could justify adding Cog-4 as a routine outcome measure for trials only if it is shown responsive to treatment effects and to contribute additional information beyond that already assessed within the mRS (9). Our analysis gives an indirect answer because it relies on nonrandomized data to tackle these questions. Our treatment groups are not perfectly matched at baseline, prognostic factors favoring the nonthrombolysed group. Despite this, the mRS outcome favored the thrombolysed patients, and after adjustment for baseline imbalance, the estimate of the intergroup difference matches the known treatment effect on mRS of intravenous alteplase. This gives a reasonable basis for the examination of Cog-4.
Unlike mRS, Cog-4 showed no intergroup difference on unadjusted analysis; indeed, the trend favored the nonthrombolysed patients. However, after adjustment for baseline imbalance, this reversed and there was a significant difference favoring the thrombolysis group. To this extent, Cog-4 appears responsive to treatment effects but perhaps less responsive than mRS.
Modified Rankin assessment considers cognitive symptoms and effects of cognitive deficits on usual activities or aspects of daily living. It is thus unlikely that Cog-4 will diverge from mRS scores in the range 0–3. At more severe grades of disability, with mRS scores of 4 or 5, there may be some patients with normal cognitive abilities as well as some with severe dysphasia or cognitive impairment. We tested whether Cog-4 scores showed an intergroup difference after stratifying our sample by mRS at 90 days, because this approach examines if there is a contribution of Cog-4 beyond that of mRS in the whole sample and retains the statistical power of our large sample. There was no intergroup difference in Cog-4: routine addition of this scale to mRS would not be justified.
Because the emphasis of mRS on mobility applies only at grades 4 and 5, and because abnormalities of Cog-4 are primarily restricted to mRS grades 4–5 (Figs 1 and 2), we also examined the intergroup difference in Cog-4 within these independent subgroups. Even allowing for the smaller sample size and associated restriction in statistical power, there was no indication that Cog-4 could detect subtle treatment effects on cognitive function that are missed by mRS.
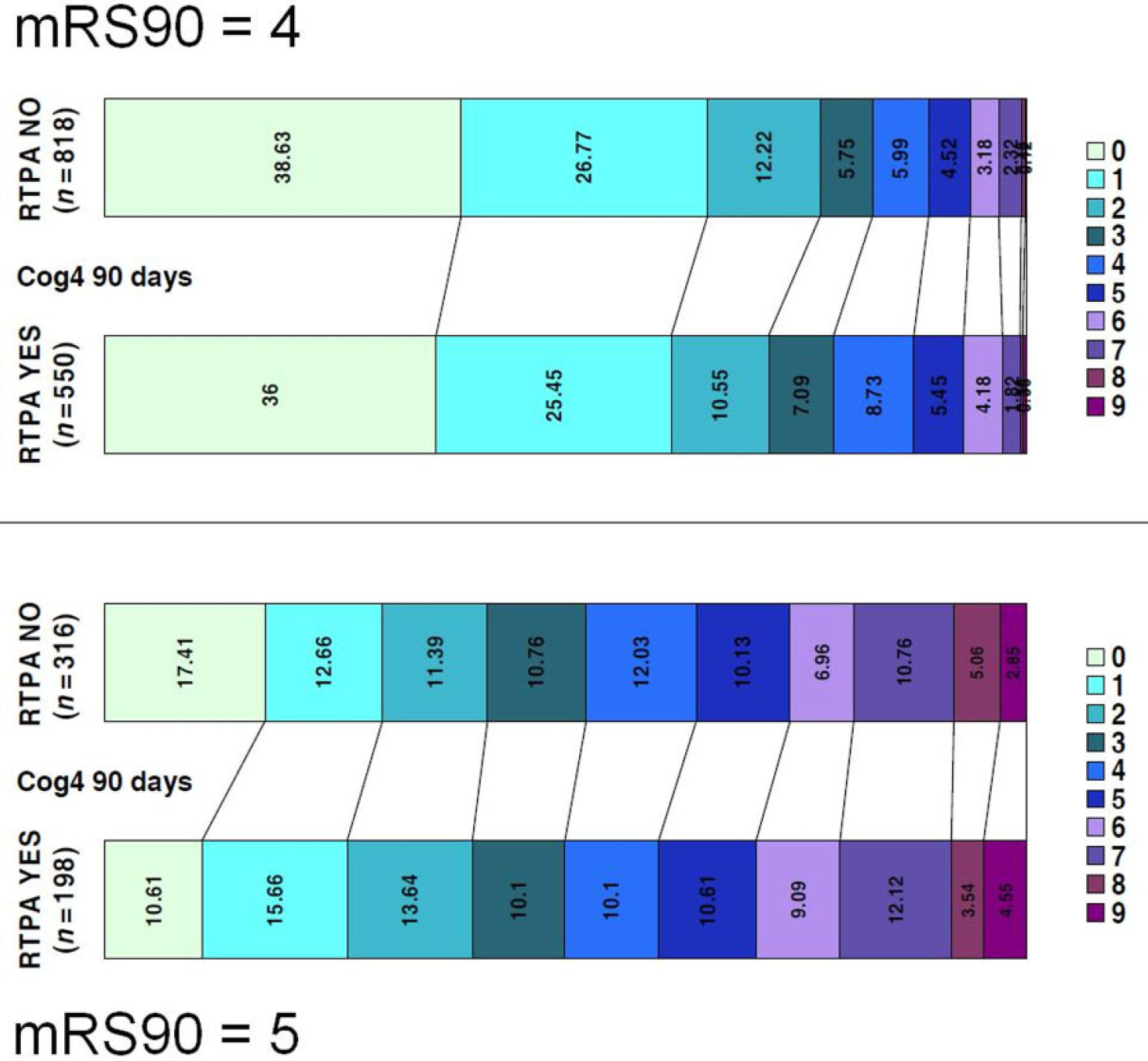
Distribution of Cog-4 at 90 days within the mRS subcategories 4 (above) and 5 (below), compared between non-thrombolysed (RTPA NO) and thrombolysed patients (RTPA YES). Figures represent raw data that showed a trend in cognitive outcome that favors the non-thrombolysed group: mRS4: OR 0·85, 95% CI 0·70–1·03; mRS5: OR 0·84, 95% CI 0·62–1·15. After adjustment for imbalance in baseline prognostic factors, no difference between groups was apparent: mRS4: OR 1·06, 95% CI 0·86–1·29; mRS5: OR 0·84, 95% CI 0·61–1·14. OR, odds ratio; mRS, modified Rankin Score; CI, confidence interval; RTPA, recombinant tissue plasminogen activator.
We treated Cog-4 score as an ordinal scale, not least due to better comparability with the ordinal mRS score. This assumption implies that a higher score is always keeping with more severe cognitive impairment. This may not be valid. The Cog-4 score comprises four sub-items that each represents a discrete aspect of cognitive function. Two patients with equal Cog-4 total scores need not present with cognitive impairment of the same nature, whereas patients with differing scores may have share a similar type of cognitive dysfunction.
Strengths of our study include the size of our sample, 10 times greater than the influential acute thrombolysis trials to date, and the robustly collected data due to the onsite monitoring and source data verification associated with the quality control measures for trials within VISTA. By restricting analysis to survivors, we also favored detection of a treatment group difference with Cog-4. Weaknesses include the nonrandomized allocation to thrombolysis treatment and imbalance in prognostic factors at baseline that represent only the visible evidence of selection bias, the case mix since over half of our patients had mRS of 0–3 by 90 days, and analytic issues regarding statistical handling of Cog-4.
The attraction of a simple, valid response measure of cognitive function after stroke is acknowledged; however, while Cog-4 is a simple measure, it lacks precision and has suboptimal statistical properties. Although it may be responsive to treatment, we conclude that the Cog-4 score does not provide additional information beyond mRS assessment and that its introduction as a trial outcome measure would not be justified. We acknowledge that neither mRS nor Cog4 is a powerful tool for assessing cognitive function and that the search for a better measure of cognitive recovery after stroke should continue.
Footnotes
Acknowledgements
The VISTA steering committee members were Alexandrov A, Bath PMW, Bluhmki E, Claesson L, Curram J, Davis SM, Donnan G, Diener HC, Fisher M, Gregson B, Grotta J, Hacke W, Hennerici MG, Hommel M, Kaste M, Lees KR (chair), Lyden P, Marler J, Muir K, Sacco R, Shuaib A, Teal P, Wahlgren NG, Warach S, and Weimar C. KH, RLF, and KRL had access to the VISTA data. KH and KRL designed and interpreted the analysis and drafted the manuscript. The manuscript was reviewed and approved by the VISTA steering committee. No commercial organization was involved in the origination, execution, or reporting of this work.