
Abstract
Background
Irreversible damage may occur at reperfusion after sustained cerebral ischaemia.
Aims
We investigated the value of cyclosporine A for reducing the infarct size in a model of transient middle cerebral artery occlusion.
Methods
Twenty-seven Sprague-Dawley rats sustained a middle cerebral artery occlusion of one-hour. Acute multimodal Magnetic Resonance Imaging (MRI) was used during occlusion to confirm the success of surgery and measure baseline lesion size. Animals were randomly treated by: (i) intracarotid cyclosporine A (10 mg/kg) 20 mins before middle cerebral artery occlusion (pretreatment group); (ii) intracarotid cyclosporine A (10 mg/kg) immediately after reperfusion (post-treatment group); and (iii) intracarotid saline immediately after reperfusion.
Results
Histopathological measurements on day 1 showed a significant reduction of infarct size in the pretreatment group compared to the post-treatment (percentage values of ipsilateral hemispheres: 16 ± 5% vs. 29 ± 11%, P= 0·004) and saline groups (16 ± 5% vs. 42 ± 12%, P= 0·015). No significant difference was observed between the post-treatment and saline groups (P = 0·065). Behavioural examinations on day 1 showed no significant difference between groups. Immunohistochemistry showed a statistically significant reduction of microglial cell count in the pretreatment group compared to either saline or cyclosporine A post-treatment groups.
Conclusions
We conclude that intracarotid cyclosporine A is effective in reducing infarct size when given prior to ischaemia, but not when administered at reperfusion.
Introduction
Timely reperfusion to limit the final infarct size remains the only validated therapeutic strategy for acute ischaemic stroke (1). Reperfusion can nonetheless induce additional injury following prolonged periods of ischaemia, through multiple mechanistic pathways: oxidative stress, calcium overload, inflammation, mitochondrial permeability transition pore (MPTP) opening, and apoptosis (2,3).
Accumulating evidence from both myocardial and cerebral ischaemia research fields indicates that reperfusion injury can be reduced by ischaemic preconditioning (a brief ischaemia that limits the damage from a subsequent prolonged ischaemia) (4,5) and postconditioning (serial interruptions of blood flow conducted at reperfusion) (6–10). Pharmacological interventions emulating the effects of ischaemic conditioning would have considerable clinical relevance. Cyclosporine A (CsA), in addition to its immunosuppressant effects, is a potent inhibitor of MPTP opening. A recent proof-of-concept trial showed that a single intravenous injection of CsA at reperfusion reduced the infarct size in patients with acute myocardial infarction (11). Conversely, no clinical trial has evaluated the impact of CsA in ischaemic stroke. Experimental data investigating the effects of CsA in models of focal cerebral ischaemia-reperfusion remain limited and conflicting (12–21).
Objectives
The present study aimed to assess the effectiveness of CsA in limiting the infarct size when administered as a pre-or post-treatment (i.e. pre- or post-reperfusion) drug, using a rat model of transient middle cerebral artery occlusion (MCAO). All animals were screened with multimodal magnetic
resonance imaging (MRI) in order to assess the success of surgery and to reduce the lesion size variability.
Materials and methods
All procedures used in this study were performed after approval by our institutional review board. Animals were housed in Plexiglas cages in groups of six in a colony room maintained on a 12/12 h light/dark cycle (07:00–19:00).
Animal model
Male Sprague-Dawley rats (Janvier, France), weighing 240–330 g, were anaesthetized with isoflurane (1–2%) in ambient air and underwent transient MCAO for 60 mins. The intraluminal suture model was used, except that the common carotid artery was permanently ligated for catheterization and treatment administration (see later) (22). The external carotid artery was electrocoagulated and transected to enable insertion of a coated monofilament (0·37 mm diameter, Doccol Corporation, Redlands, CA, USA). The suture placement at the MCA origin was monitored by transcranial laser Doppler flowmetry (PeriFlux System 5000, Perimed, Järfälla-Stockholm, Sweden). The probe was positioned 5 mm lateral and 2 mm posterior to the bregma. Reperfusion was achieved by withdrawing the monofilament. To alleviate pain, animals received 0·05 mg/kg subcutaneous buprenorphine immediately after reperfusion anaesthesia. During surgery, body temperature was monitored continuously with a rectal probe and maintained at 37·0 ± 0·5°C by a feedback-regulated heating pad.
Treatment
Animals (n = 27) were randomly assigned into three treatment groups (n = 9 each):
pretreatment group: intracarotid injection of CsA (Sandimmun® 50 mg/ml, Novartis, Basel, Switzerland: 10 mg/kg) 20 mins before ischaemia onset
post-treatment group: intracarotid injection of CsA (10 mg/kg) within one-minute following reperfusion, and
saline group: intracarotid injection of NaCl 0·9% within one-minute following reperfusion.
All examiners assessing MRI, behavioural, and histopathological data were blinded to treatment allocation.
Magnetic resonance imaging
MRI was performed in all animals during the 60-min MCAO, using a Bruker Biospec 7T/12 cm horizontal magnet equipped with Paravision 5·0. A birdcage head-coil of 72 mm inner diameter was used for radiofrequency transmission and a 25 mm diameter surface coil for reception. The rats were placed in a cradle equipped with a stereotaxic holder, an integrated heating system to maintain body temperature at 37 ± 1°C, and a pressure probe to monitor respiration. Time-of-flight magnetic resonance angiography (MRA) was performed using a two-dimensional multislice gradient echo sequence with matrix = 256 × 128, field of view (FOV) = 3·7 × 2·5 cm2 80 contiguous slices with slice thickness 0·3 mm and interslice overlap 0·15 mm, TE/TR = 5/25 ms, and two averages. T2-weighted images were acquired using a RARE sequence with matrix =256 × 256, FOV = 4×4 cm2 five noncontiguous slices with slice thickness 1·5 mm and interslice gap 0·5 mm, covering the entire MCA territory, TE/TR = 75/3000 ms, and two averages. Diffusion-weighted imaging was performed 40 mins after ischaemia onset in all animals, using echo planar imaging (EPI) with the same FOV and slice characteristics as T2-weighted images, with matrix = 128 × 128, TE/TR =25/2000 ms and 3 b-values (0,1500, and 3000 s/mm2). Perfusion weighted imaging was performed with multislice dynamic susceptibility contrast-enhanced MRI, using an EPI gradient echo sequence with the same FOV and slice characteristics (matrix = 96×96, zero-filled to 128 × 128 and TE/TR 4·84/100 ms). One hundred consecutive images were acquired per slice with a time resolution of 0·6 s during which a 0·2-ml bolus of gadolinium (Dotarem, Guerbet Aulnay-sous-Bois, France) was injected intravenously after acquisition of the 15th image.
Image analysis
MRI analysis was performed by an investigator (P. A.) blinded to treatment allocation, behavioural, and histological data. Source images and maximum intensity projection of MRA were used to assess MCA occlusion. A qualitative angiographic score was defined: complete occlusion (undetectable flow along the whole MCA route), partial occlusion (decreased flow signal), and no occlusion (normal flow signal). Apparent diffusion coefficient (ADC) maps (mm2/s) were calculated by fitting MR signal curves to a monoexponential model function on a pixel-by-pixel basis, using in-house software written in Matlab 2009 (MathWorks, Natick, MA, USA). Contrast agent-induced signal intensity changes from Dynamic Susceptibility Contrast-enhanced MRI (DSC-MRI) images were converted to changes in the transverse relaxation rate 1/T2* (i.e., AR2*) according to the formula AR2* = −1/TE.lnS(t)/S0, where S0 is the precontrast baseline signal intensity and S(t) is the signal intensity at time t. Time-to-peak maps are commonly used clinically to assess hypoperfusion (23); however, the low temporal resolution compared to bolus first-pass duration hampered their use in the present rodent study, and perfusion maps were therefore generated using the image corresponding to the AR2* time-curve peak, or maximum peak concentration (MPC) (24). Acute diffusion and perfusion lesions were manually outlined on ADC and MPC maps, respectively, using ImageJ software (Image Processing and Analysis in Java, NIH, Bethesda, MD, USA; http://rsb.info.nih.gov/ij/). Lesion volumes were expressed as a percentage value of ipsilateral hemisphere.
Animal inclusion criteria
To reduce the intrinsic variability of lesion size in this model, operated animals were included in the analysis only if they fulfilled the following criteria based on their acute MRI:
Behavioural examination
Behavioural evaluation was performed 24 h after MCAO (F. C., blinded to treatment allocation and MRI data), using a previously reported neuroscoring scale: 0–9 (27) These scales consist in simple sensorimotor tasks (gait, parachute reflex, lateral resistance, limb placing) for assessment of the extent of lateralized neurological deficits. Higher scores reflect greater deficits.
Measurement of final infarct volume
After the behavioural evaluation, animals were sacrificed with an overdose of pentobarbital. Brains were fixed immediately in 4% formalin and remained in this solution for five-days. Following paraffin embedding, 20-mm coronal sections were obtained and stained with cresyl violet. Five sections taken at equally spaced 2-mm intervals, corresponding to MRI slices, were selected and digitized. Infarct volumes were expressed as a percentage of the ipsilateral hemisphere volume. Normalization to the entire ipsilateral hemisphere copes with tissue deformation of various sources (oedema, fixation, histological processing) and enables a comparison between in vivo and post-mortem data. Finally, the evolution of lesion size between day 0 ADC map and day 1 histological sections (expressed as percentage values of ipsilateral hemispheres) was assessed: evolution = (day 1 – day 0)/day 0 × 100.
Microglial cells detection
Coronal sections at bregma 0·84 mm (n = 6 for each condition) were first incubated for 30 mins with 5% normal horse serum in phosphate-buffered saline with 0·5% triton X-100, then overnight at 4°C with biotinylated Ricinus communis (tomato lectin, dilution 1:500) and revealed with streptavidin coupled to the red fluorescent marker Cy3 (Jackson ImmunorRes Laboratories, Interchim, Asnieres, France). Stained cells were counted in the cortex at the periphery of the infarct.
Statistical analysis
Data analysis was performed using SPSS software (Version 15.0, SPSS Inc., Chicago, IL, USA), with statistical significance set at P < 0·05. Nominal parameters (ADC, MPC, and histological volumes, as well as cell counts) are reported as mean ± standard deviation, while neuroscores are reported as median and range. Comparisons between treatment groups were performed with nonparametric Kruskal–Wallis tests. Mann-Whitney tests were used for post hoc paired comparisons, with Bonferroni's adjustment for the P-value (P < 0·017 for three groups).
Results
From the 27 rats that underwent randomization and surgery, 21 fulfilled inclusion criteria and were included in the study. Three animals were excluded because of subarachnoid haemorrhage (two in the saline group, one in the pretreatment group), while three other animals had an incomplete occlusion and/or an ADC lesion restricted to striatum (one in the saline group, two in the pretreatment group). Three rats in the post-treatment group died within minutes of CsA injection and thus could not be assessed on day 1. No significant difference in ADC (P= 0·559) or MPC (P= 0·717) lesion size was observed between treatment groups on day 0 (Table 1).
Ischaemic lesion volumes (ADC maps), hypoperfusion volumes (MPC maps) and mortality on day 0
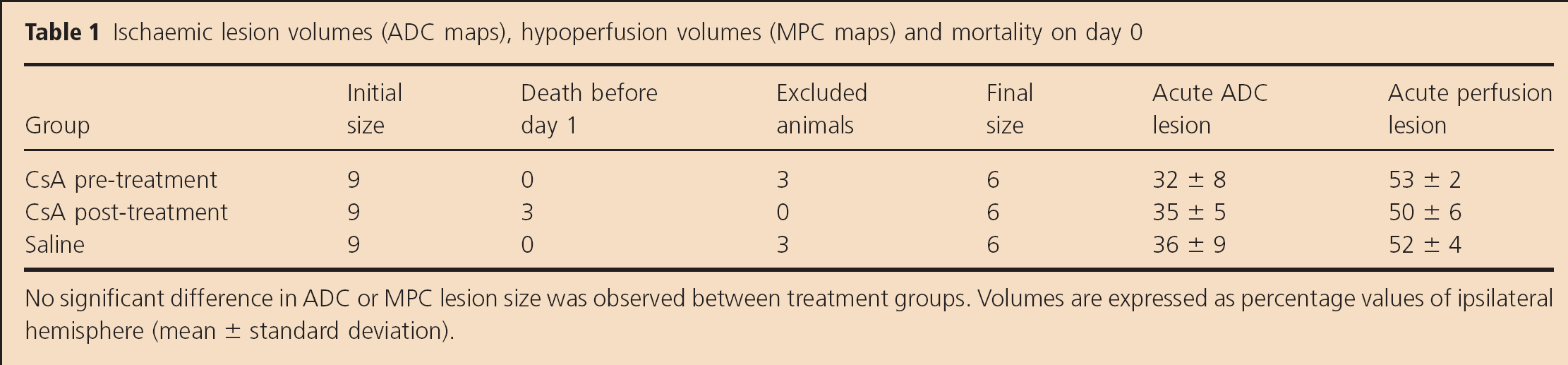
No significant difference in ADC or MPC lesion size was observed between treatment groups. Volumes are expressed as percentage values of ipsilateral hemisphere (mean ± standard deviation).
Behavioural examinations on day 1 showed no significant difference between groups (P= 0·264) (Fig. 1). CsA injection before induction of ischaemia significantly reduced the infarct size on day 1, compared to post-treatment with either saline (16 ± 5% vs. 42 ± 12%, P = 0·004) or CsA (16 ± 5% vs. 29 ± 11%, P = 0·015). CsA administered after reperfusion did not significantly affect lesion size compared to saline (P = 0·065). From day 0 to day 1, a significant reduction in lesion volume was observed in the pretreatment group when compared to either saline (−49 ± 11% vs. +16 ± 20%, P = 0·002) or CsA post-treatment group (−49 ± 11% vs. −20 ± 24%, P = 0·004). Conversely, no significant difference was noted between the saline and CsA post-treatment groups (P = 0·026). These results are summarized in Fig. 2. Immunohistochemistry showed that the microglial cell count was significantly reduced in the pre-treatment group, compared to saline or CsA post-treatment groups (Fig. 3).
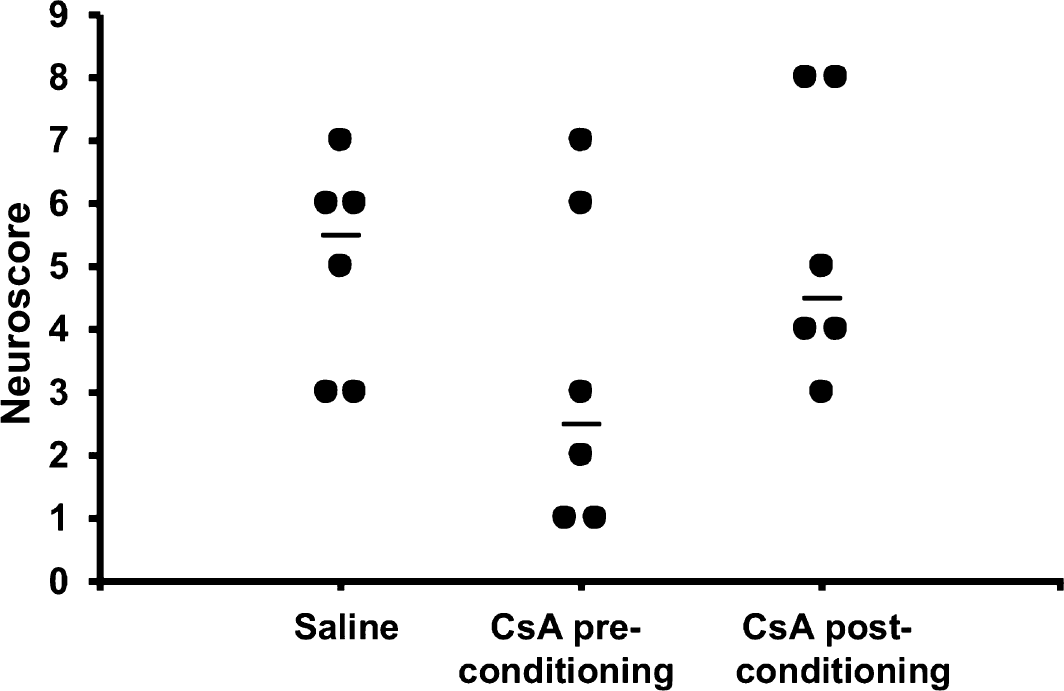
Blinded behavioural evaluation 24 h after ischaemia onset in the saline, preconditioning and postconditioning groups, using the 0–9 neuroscore (27). No significant difference was noted between groups (horizontal bars represent median values).
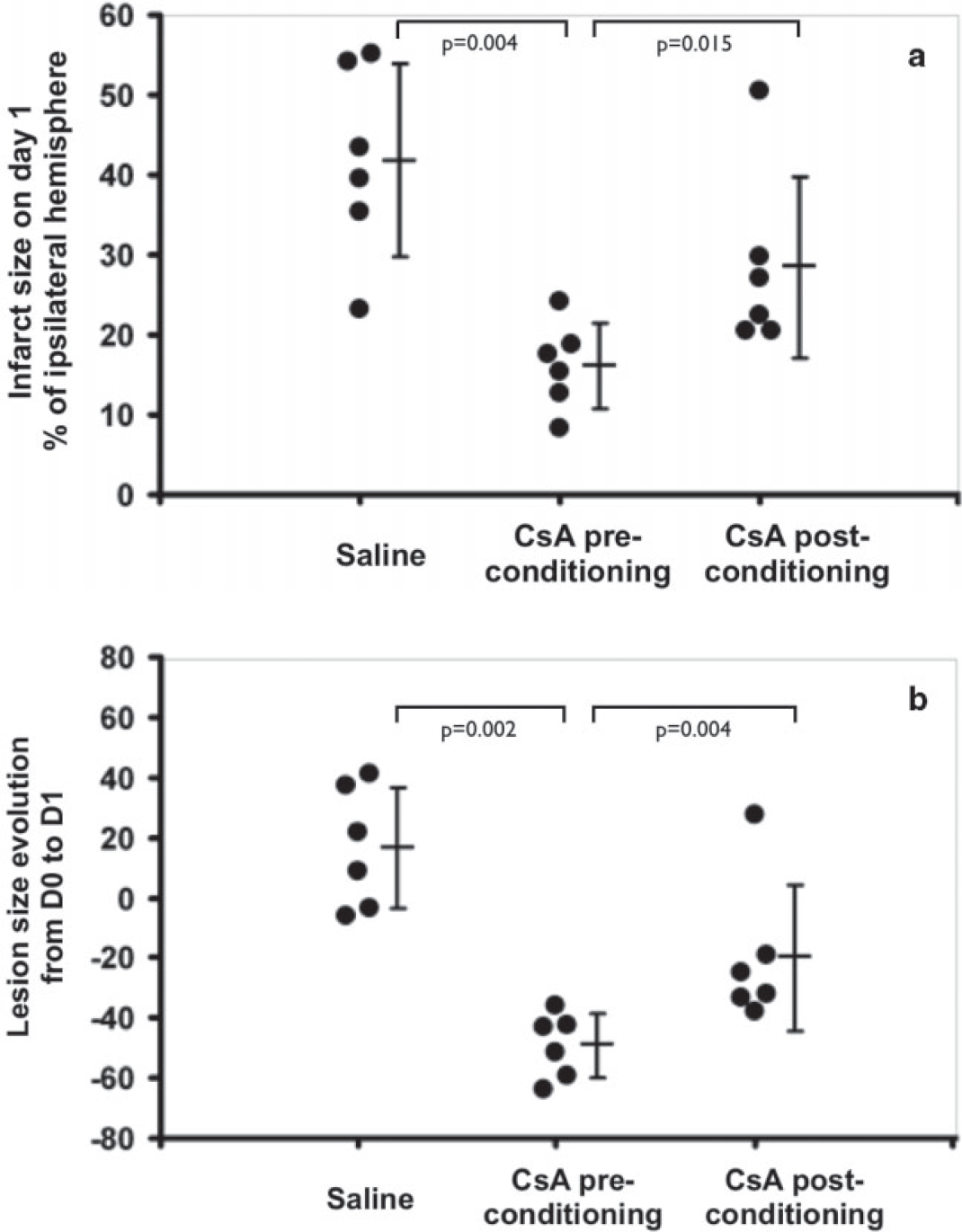
Infarct size on day 1 (a): lesion size was reduced in the pretreatment group compared to the saline (16 ± 5% vs. 42 ± 12%, P= 0·004) and post-treatment group (16 ± 5% vs. 29 ±11%, P= 0·015). No significant difference was observed between the post-treatment and saline groups (P = 0·065). Lesion size evolution between day 0 and day 1 (b) yielded the same conclusions.
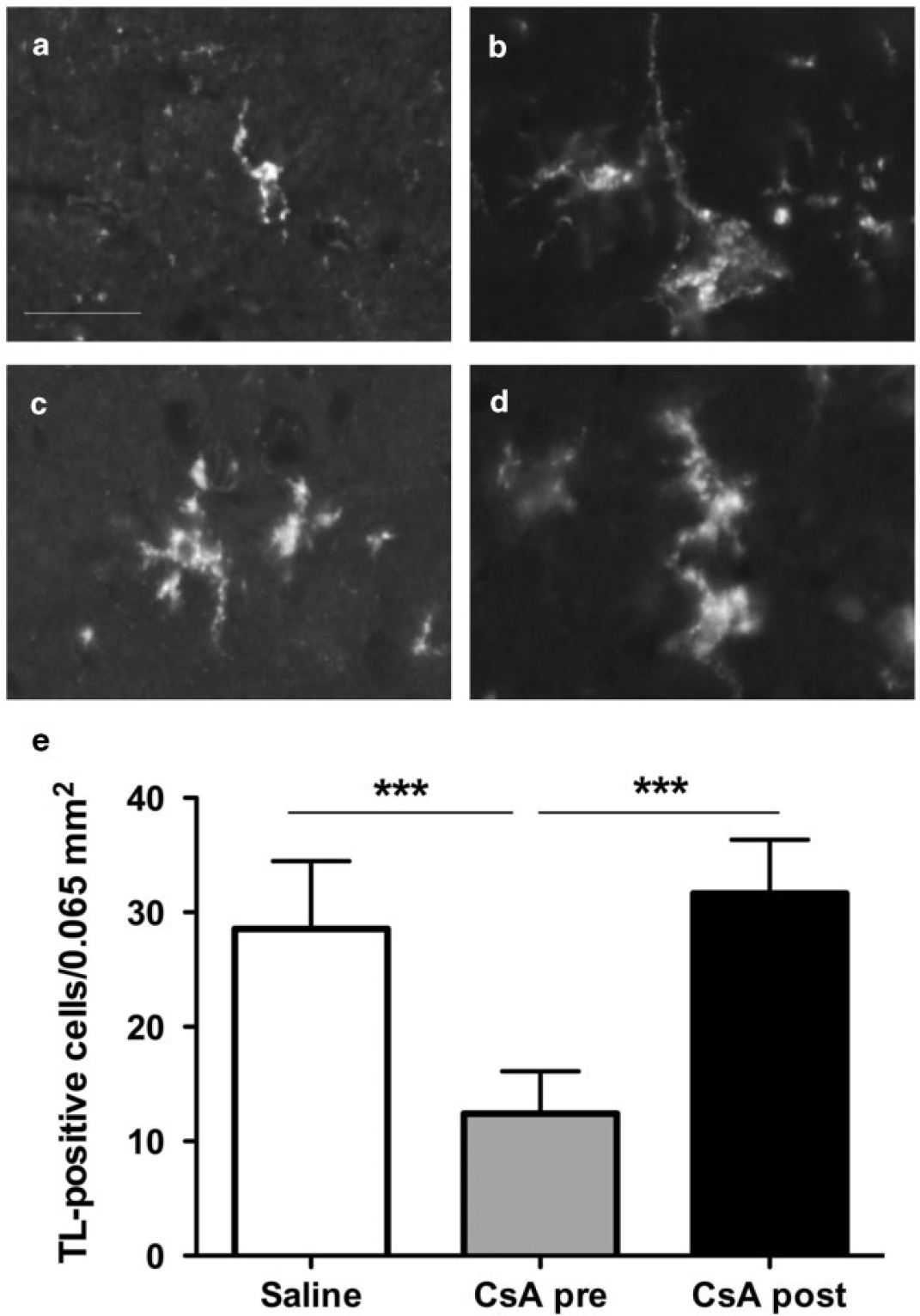
CsA given before ischaemia reduces microglial responses at 24 h of reperfusion. Microglial cells were detected using tomato lectin (TL) immunostaining. (a,b) Example of resting (a) and reactive (b) microglia in the contralateral and ipsilateral hemisphere, respectively, in an ischaemic animal receiving the saline solution. (c,d) Example of reactive (c) and ameboid (d) microglia in animals receiving CsA either before (c) or after (d) the ischaemic onset. Note the intermediate (between resting and activated) microglia morphology in a CsA-pretreated animal. Scale bar represents 20 mm. (e) Quantitative analysis of reactive TL-positive microglial cells density in the cortex at the periphery of the infarct (***P < 0·001).
Discussion
Using MRI-based criteria for animal inclusion, we showed that CsA given shortly before reperfusion provided a robust reduction of lesion size after transient MCAO. As CsA poorly crosses the blood brain barrier, we used intracarotid injections which increase cerebral concentration two- to threefold compared to intravenous administration (28,29). Our results expand previous data: only three studies had evaluated pretreatment with CsA in models of focal cerebral ischaemia, using different models and treatment regimen (13,14,21). No significant behavioural benefit was associated with this reduction of infarct size. A prolonged follow-up may yield additional data for neurobehavioural analysis; our assessment was performed on day 1, and may have lacked sensitivity.
CsA is thought to limit reperfusion injury by antagonizing MPTP opening and thus preventing the resulting collapse of the mitochondrial membrane potential, uncoupling of the respiratory chain, efflux of proapoptotic factors, and adenosine triphosphate (ATP) hydrolysis (30). Modulation of inflammatory processes such as oxidative stress may mediate the effects of preconditioning (31). The reduced number of microglial cells in the pretreatment group indicates that CsA may also regulate the activation of phagocytes. It may otherwise be the result of a smaller lesion, and the role of microglial cells in reperfusion injury remains currently unclear.
We observed no significant benefit from intracarotid CsA when administered at reperfusion. Previous studies reported both positive and negative results, using various CsA dosages and administration routes. Yoshimoto et al. showed that an intracarotid injection of CsA (10mg/kg) five-minutes after reperfusion reduced the infarct size to 10% of the volume in control animals, but this study included animals with virtually no lesion after 90 mins of ischaemia; intravenous injections conferred no protection, unless a needle lesion had disrupted the blood brain barrier before ischaemia (16). Conversely, another group demonstrated effective neuroprotection using intravenous injections, despite using the same animal model and CsA dosage (20). Positive results were reported after intraperitoneal infusions, although the optimal treatment regimen remains uncertain (15,17–19). Our results clearly showed a difference in the effects of CsA when given before or after reperfusion onset. In intraluminal MCAO models, interspecies variability and interlaboratory differences in protocols are the source of significant variability in success and complication rates, and lesion volume (32). We minimized inter-animal lesion size variability by using MRI criteria for inclusion, allowing us to detect the protective effects of a pretreatment by CsA.
Furthermore, three out of nine animals died within minutes of CsA injection in the post-treatment group, whereas no mortality was observed in the other groups. Cerebral toxicity with increased rates of seizure and mortality was previously reported with intravenous or intraperitoneal injections exceeding 30–50 mg/kg of CsA (16,17). The biochemical mechanisms underlying CsA neurotoxicity remain unclear. Clinical and radiological analogies between mitochondrial encephalopathies and CsA-related posterior reversible encephalopathy syndrome, as well as studies using magnetic resonance spectroscopy, point to the central role of mitochondrial dysfunction resulting in cerebral ATP depletion, anaerobic glycolysis, increased levels of lactate, and reactive oxygen species (33). CsA may also cause endothelial cell dysfunction and vasoconstriction through decreased production of nitric oxide, and thus compound the vascular lesions observed during ischaemia (34). CsA was solubilized in its usual vehicle,
Cremophor® a synthetic surfactant with a potential toxicity on the peripheral nervous system (35). Conversely, its possible cerebral toxicity is less documented. Having used saline in the control group, the present work cannot fully address this issue. Our results suggest that CsA may have deleterious effects when administered after reperfusion. Although the presence of an acute cerebral lesion may have exacerbated neurotoxicity in the post-treatment group, no definite explanation has been validated.
In conclusion, pretreatment with intracarotid injection of CsA proved effective in a rat model of MCA ischaemia-reperfusion. After reperfusion, the margin between the potential neuroprotective and toxic effects of CsA appears to be narrow.
Footnotes
Acknowledgements
Imaging experiments were performed on the ‘Animage’ platform of CERMEP-Imagerie du Vivant, Lyon, France. The authors would like to thank Olivier Beuf and Denis Grenier of Creatis for help with EPI sequence optimization, as well as Jean-Baptiste Langlois of CERMEP for technical assistance during imaging experiments.