
Abstract
Background
Frequency, factors associated with, and impact on outcome of haemorrhagic transformation in young adults with ischaemic stroke are unknown.
Methods
Consecutive young patients (age 15–49) with first-ever ischaemic stroke were included, having their first brain computed tomography/magnetic resonance imaging within seven-days of stroke onset, and second within seven-days from the first imaging. Haemorrhagic transformation in any imaging was classified as haemorrhagic infarct or parenchymal haemorrhage within or remote from the infarct. Symptomatic haemorrhagic transformation was defined according to the European Cooperative Acute Stroke Study II (ECASS II) criteria as any haemorrhage leading to a National Institutes of Health Stroke Scale score increase of ≥4 points or death. Unfavourable three-month outcome was defined as a modified Rankin Scale 2–6.
Results
In 636 eligible patients, any haemorrhagic transformation occurred in 79 patients (12·4%; 10·0–15·2%): 66 (10·4%; 8·24–12·9%) had haemorrhagic infarct, and 13 (2·04%; 1·19–3·46%) had parenchymal haemorrhage. Symptomatic haemorrhagic transformation occurred in 16 patients (2·5%; 4·04–1·55%). In logistic regression analysis, independent factors associated with haemorrhagic transformation were large anterior (18·70; 6·72–52·04), large posterior (9·41; 3·13–28·25), medium-sized (odds ratio 3·30; 95% confidence interval 1·14–9·57) lesions, higher low-density lipoprotein level (1·44 per unit increment; 1·10–1·90), and lower platelet count (1·005 per unit decrement; 1·009–1·001). Haemorrhagic infarct (1·76; 0·76–4·11) or parenchymal haemorrhage (2·39; 0·23–24·76) were not associated with unfavourable functional outcome or death at three-months.
Conclusions
In young adults, haemorrhagic transformation of ischaemic stroke occurred in comparable rates to haemorrhagic transformation in elderly patients. Although haemorrhagic transformation was more common in severe strokes, it was the lesion size and baseline stroke severity that were associated with three-month clinical outcome, not haemorrhagic transformation per se.
Introduction
Ischaemic stroke is an important cause of morbidity and mortality, and has long-lasting effects on young adults regarding quality of life and work ability (1). Some data exist on the occurrence of risk factors (2); however, the neuroimaging data on solely young stroke patients are scarce (3,4). Factors associated with, frequency, and impact on outcome of haemorrhagic transformation (HT) in young patients with ischaemic stroke are unknown.
In elderly patients, parenchymal haemorrhage (PH), but not any HT, has been associated with an increased risk for death or disability (5). Neurological deterioration has usually been detected in patients with a dense haemorrhage exceeding 30% of the infarcted area with a substantial space-occupying effect or HT remote from the infarcted area (6). However, earlier results in older patients suggest that also smaller haemorrhages can influence the outcome (7,8), and that, in children, increasing HT grade was associated with a worse outcome in unadjusted analysis, although not after taking the lesion size into account (4).
Bleeding into an ischaemic lesion is a natural consequence of cerebral infarction, and HT is seen within the first days, up to 1–2 weeks after stroke onset (9), with only 3% occurring during the third week (10). Good collateral circulation has been thought to be essential (10) and reperfusion time important for HT, as delayed recanalization is associated with HT (11). Stroke aetiology affects HT, and the frequencies have been high in cardioembolic (CE) patients: 40% in computed tomography (CT) studies (10) and even higher in autopsy findings (12) and magnetic resonance imaging (MRI) studies (13). Recanalization has also been reported to occur more often in CE than in atherothrombotic stroke (14).
The overall frequency of any HT in earlier study populations has been reported to be 8·5–13% with elderly stroke patients (5,15,16) and 30% in childhood strokes (4). Symptomatic HT (sHT) has been 0·6–4·6% in nonthrombolysed (15,17) and 5·9% in thrombolysed old patients (18), and 3% in childhood strokes (4). The risk of HT has been higher in patients on anticoagulation therapy increasing with the dose (5,16), although controversial reports exist (14,19). The HT risk factors analysed previously have concerned older stroke patients (5), or children (4), and the results have been partly controversial, due to small or heterogeneous study populations.
Aims
Our study was designed to investigate the HT rate and risk factors in young adults, and to determine its impact on the three-month outcome in a large homogenous ischaemic stroke population.
Methods
This retrospective study was approved by the relevant authorities, and carried out at the Department of Neurology, Helsinki University Central Hospital, Finland. Our hospital is the only comprehensive stroke centre with a neurological emergency room in the Helsinki and Uusimaa region serving a population of 1·5 million. The Helsinki Young Stroke Registry (n = 1008) includes all first-ever ischaemic stroke patients aged 15 to 49 years diagnosed and treated at our department from 1994 to 2007, including information on risk factors, aetiology, and detailed neuroimaging data (2).
Patients extracted from the database for the current study were imaged at least twice, with the first brain imaging performed within seven-days of stroke onset, and the second within seven-days from the first imaging. When clinically deemed necessary, patients included in the study were imaged more than twice. Brain imaging data are shown up to 35 days. The stroke aetiology was based on medical and radiological data, and was assessed by stroke physicians according to the Trial of Org 10172 in Acute Stroke Treatment (TOAST) criteria (20). All patients underwent routinely a wide range of blood tests at admission, and fasting blood tests were performed the following working day within 72 h.
Brain imaging was performed using either CT (n = 634) or MRI (n = 472), or both. Infarct size was classified based on documented templates (5) with slight modifications: (1) small <1·5 cm lesion: in anterior or posterior circulation; (2) medium lesion: in a cortical superficial branch of the anterior cerebral artery (ACA), middle cerebral artery (MCA), or posterior cerebral artery (PCA), or deep branch of MCA or PCA, or in internal border-zone territories; (3) large anterior lesion: complete territory of ACA or MCA; two branches of MCA; or >1 artery territory; and (4) large >1·5 cm posterior lesion: involving brain stem, cerebellum, or complete territory of PCA together with border-zone territories.
HT classification was carried out blinded to outcome data involving all brain imaging. HT was defined radiologically as a haemorrhagic infarct (HI), parenchymal haemorrhage (PH) within, or remote (PHr) (21) from the actual infarct area. Due to the small number of PHs and PHrs, these were merged into one group for statistical analysis. Symptomatic HT (sHT) was defined in both thrombolysed and nonthrombolysed patients according to the European Cooperative Acute Stroke Study II (ECASS II) criteria as blood at any site in the brain, clinical deterioration, or adverse events indicating clinical worsening (e.g., drowsiness, increase of hemiparesis) or causing an increase in a National Institutes of Health Stroke Scale (NIHSS) score of 4 or more points (22).
Patients were routinely evaluated at three-months at the outpatient clinic by a neurologist or at a rehabilitation site by the treating physician. In a few patients, outcome information was obtained by a telephone interview. One patient was lost to follow-up at three-months. Three-month modified Rankin Scale (mRS) with a score of 2 to 6 represented unfavourable outcome for the young adults, as defined before (23).
Statistical analyses
Chi-square and Fisher's exact tests were used to compare categorical variables. Student's t-test and Mann–Whitney U-test allowed comparisons of normally distributed continuous and non-normally distributed or noncontinuous variables, respectively. Age, laboratory parameters, and NIHSS score were analysed as continuous variables. Detection of HT was depicted graphically by means of Kaplan–Meier curves with comparisons between sub-groups by log-rank tests. A multivariate logistic regression model was constructed to investigate factors associated with HT detected in any brain imaging. In addition to age and gender, variables in this model were selected based on their univariate significance (P < 0·10). In the regression model studying the associations with the three-month outcome, covariates included demographics, those showing a univariate association with unfavourable outcome and those with a significant association with HT development. As all risk factors meeting the univariate criterion for multivariable models (congestive heart failure, history of myocardial infarction, and atrial fibrillation) had significant collinearity with the TOAST category high-risk CE source, they were not entered in the models, A two-sided P value <0·05 was considered statistically significant. All statistical analyses were performed on SPSS 19·0 (SPSS Inc., Chicago, IL, USA).
Results
A total of 636 eligible patients were included in the study with more men (n = 365, 60·5%) than women. The median age was 42·9 years [interquartile range (IQR), 37–47], including seven paediatric patients (15–18 years) and half of the patients being ≤40 years. Median delay to first imaging was zero-days (IQR, 0–1) and to second imaging one-day (IQR, 1–3). There were 79 patients (12·4%; 95% CI 10·0–15·2%) with HT, of which 47 (60%) were detected with CT and 32 (40%) with MRI. Median delay to HT detection was three-days (IQR, 2–8), and HT was detected in 10 patients (1·6%) in the first brain imaging. The majority (n = 66) of HTs were HI1 or HI2 (10·4%; 8·24–12·9%), and 13 patients had PH or PHr (2·04%; 1·19–3·46%). Sixteen (2·5%; 95% CI 4·04–1·55%) had sHT according to the ECASS II criteria. The case fatality rate was 24% in 35 days.
Table 1 shows univariate comparison between patients having any or no HT, and Fig. 1 depicts the timing of HT detection in the entire cohort (Fig. 1a) and in sub-groups (Fig. 1b–e). Mean age or gender distribution did not differ between patients having any or no HT. Patients with any HT had significantly higher baseline NIHSS and larger infarcts (Table 2), located in most cases in the anterior circulation (Fig. 1b). Pre-hospital oral anticoagulant, antiplatelet, or statin therapy did not increase the risk of HT. Among the laboratory parameters, higher levels of baseline low-density lipoprotein (LDL) (Fig. 1c), lower high-density lipoprotein (HDL) levels, and significantly lower platelet counts (Fig. 1d) appeared in patients with HT. High-risk source of CE, carotid artery dissection (CAD) (Fig. 1e), heart failure, and myocardial infarction were more frequent among these patients. They were less often anticoagulated or treated with antiplatelets during hospitalization, but received more frequently a prophylactic dose of low-molecular-weight heparin. Intravenous thrombolysis treatment was equally frequent in both groups. Lipid profiles according to aetiologic sub-groups are given in Table 3.
Demographics, prestroke, and in-hospital medication, and stroke risk factors in the study cohort and stratified by occurrence of any haemorrhagic transformation (HT)
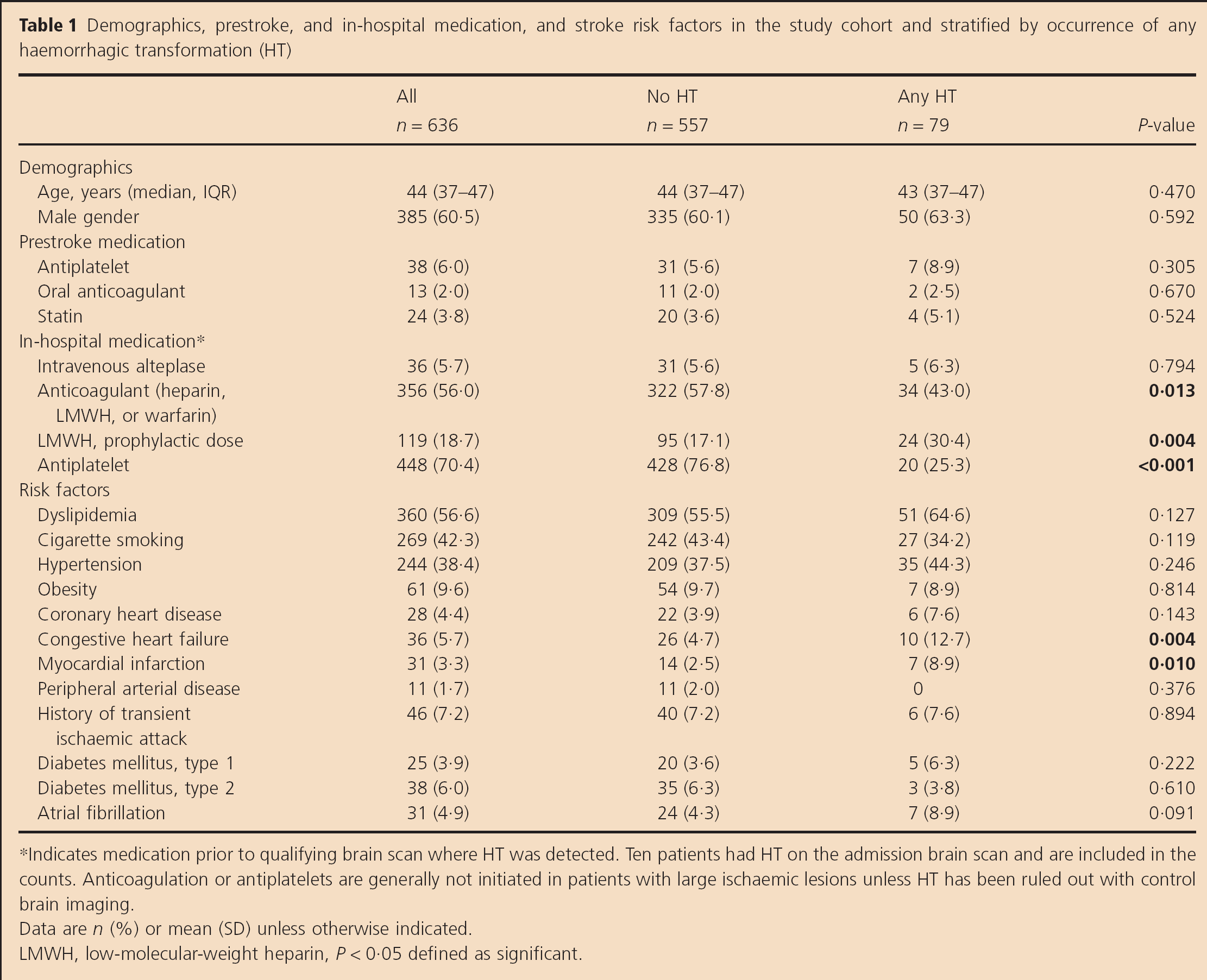
Indicates medication prior to qualifying brain scan where HT was detected. Ten patients had HT on the admission brain scan and are included in the counts. Anticoagulation or antiplatelets are generally not initiated in patients with large ischaemic lesions unless HT has been ruled out with control brain imaging.
Data are n (%) or mean (SD) unless otherwise indicated.
LMWH, low-molecular-weight heparin, P < 0·05 defined as significant.
Baseline laboratory parameters, stroke characteristics, and aetiology in the study cohort and stratified by occurrence of any haemorrhagic transformation (HT)
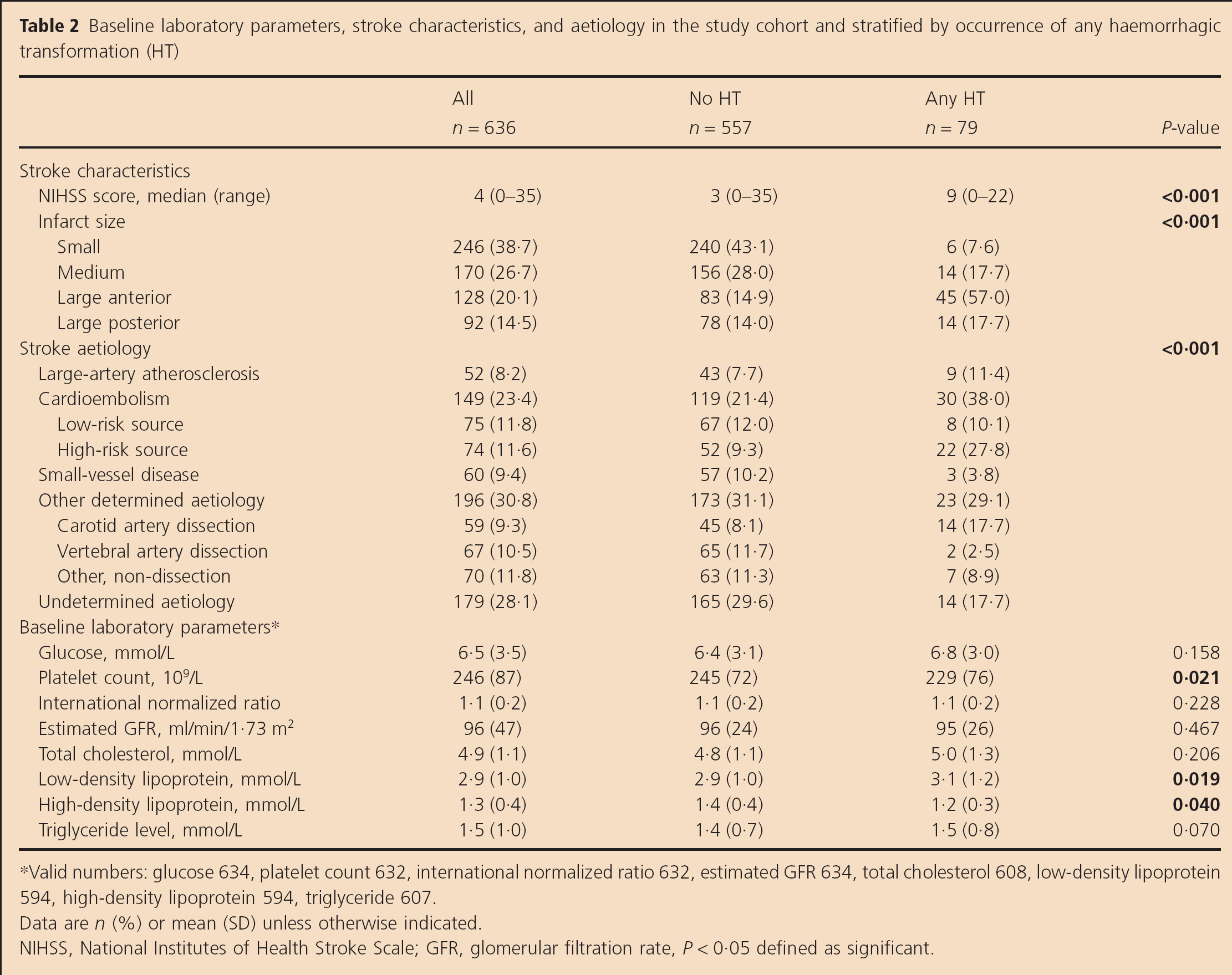
Valid numbers: glucose 634, platelet count 632, international normalized ratio 632, estimated GFR 634, total cholesterol 608, low-density lipoprotein 594, high-density lipoprotein 594, triglyceride 607.
Data are n (%) or mean (SD) unless otherwise indicated.
NIHSS, National Institutes of Health Stroke Scale; GFR, glomerular filtration rate, P < 0·05 defined as significant.
Lipid profiles in various stroke aetiology groups
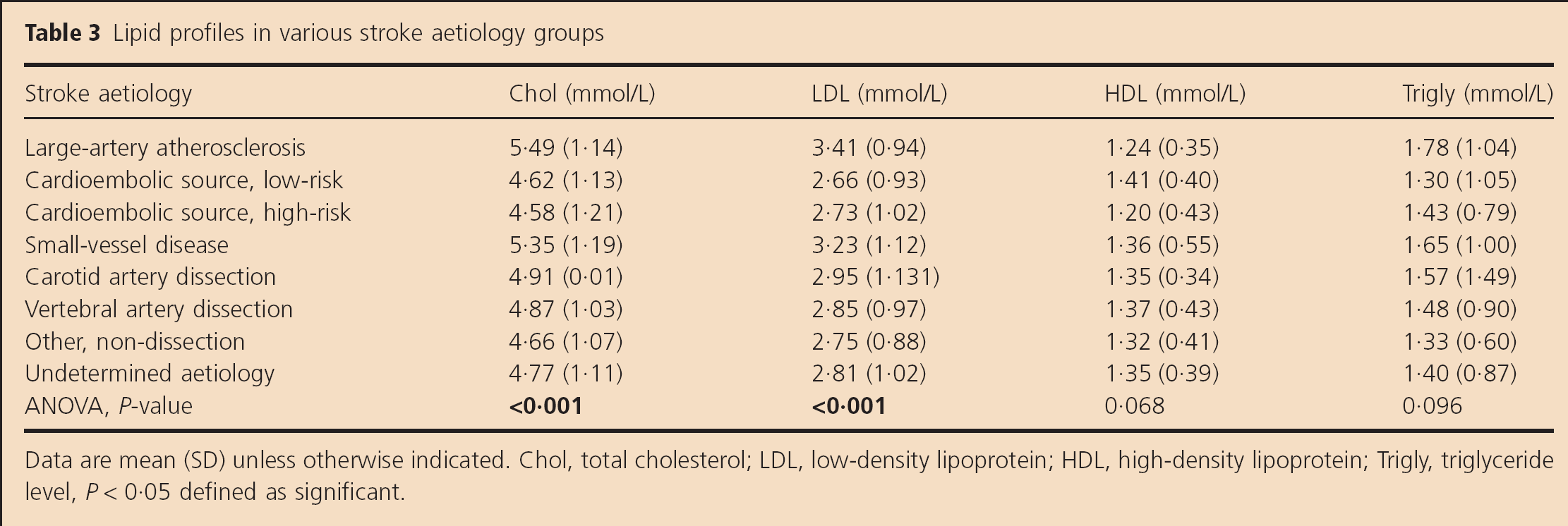
Data are mean (SD) unless otherwise indicated. Chol, total cholesterol; LDL, low-density lipoprotein; HDL, high-density lipoprotein; Trigly, triglyceride level, P < 0·05 defined as significant.
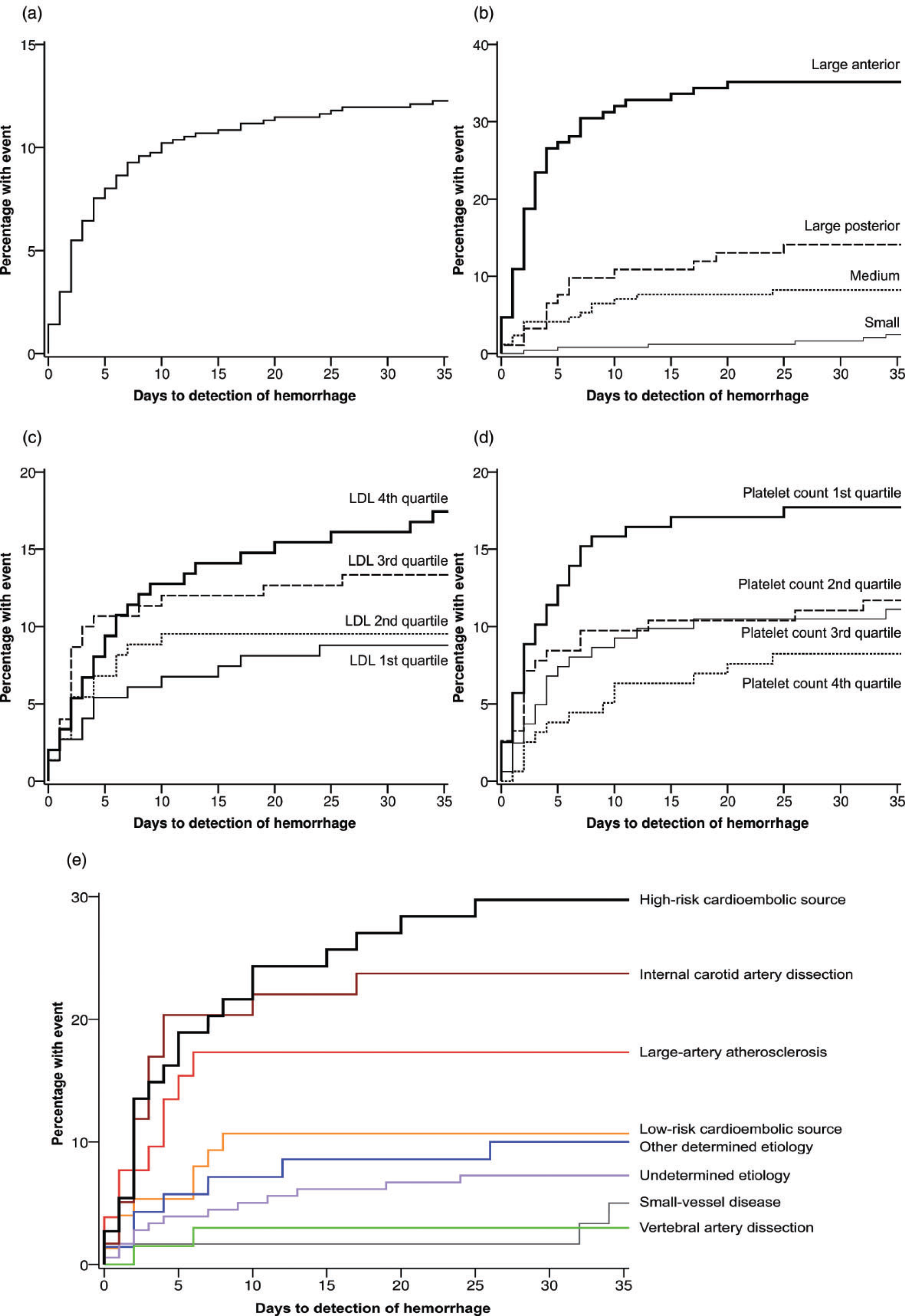
Kaplan–Meier curves showing timing and rate of the detection of haemorrhagic transformation (a) in the entire cohort and stratified by (b) infarct size (log rank P < 0·001), (c) low-density lipoprotein quartiles (P = 0·089), (d) platelet count quartiles (P = 0·062), and (e) aetiologic sub-group (P < 0·001). The analyses considered all brain imaging studies.
In multivariate logistic regression model that investigated factors associated with HT, female gender, lesion size, high-risk source of CE, higher LDL level, and lower platelet counts were associated with HT (Table 4).
Logistic regression analysis exploring association between baseline variables and haemorrhagic transformation
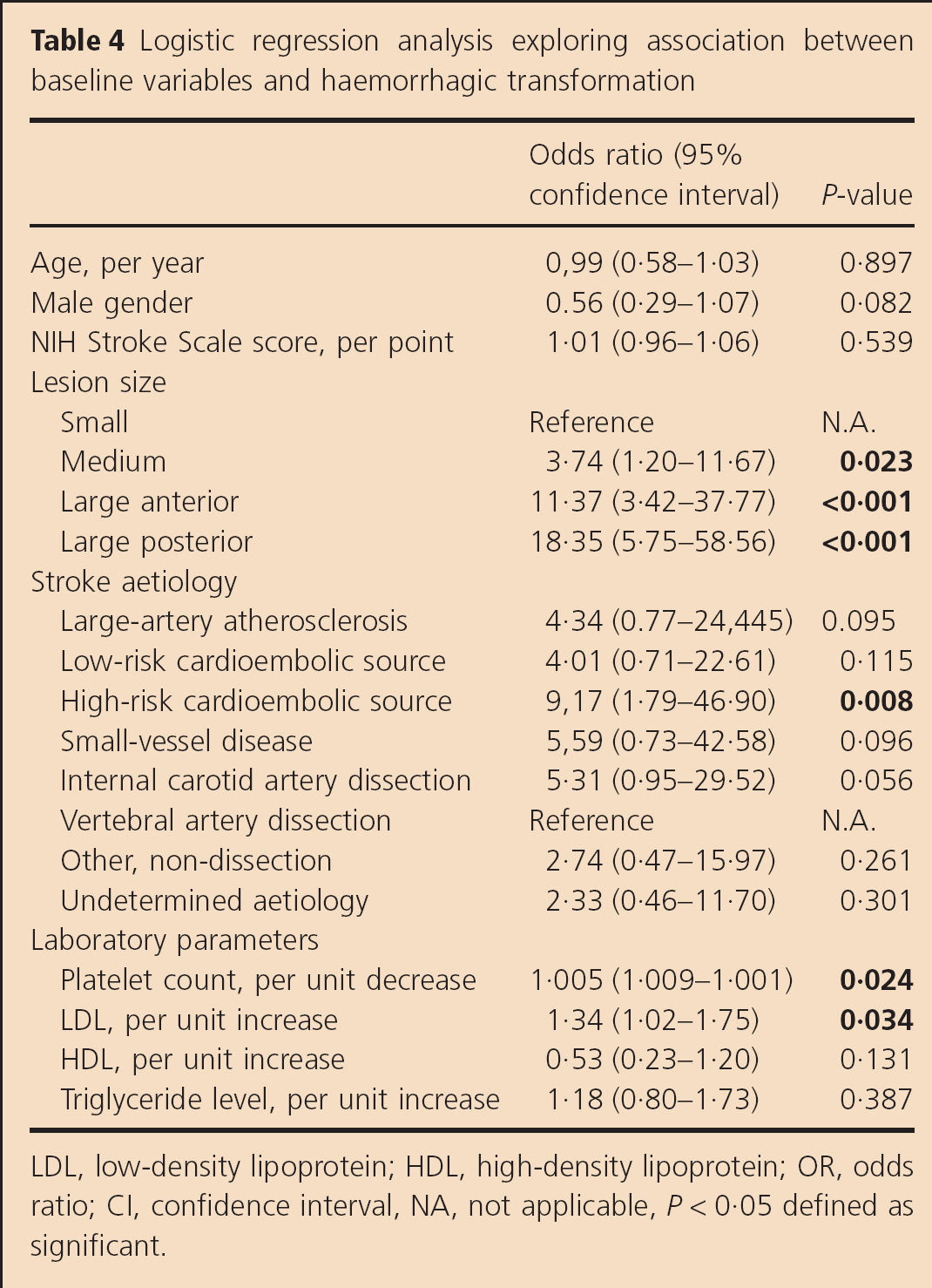
LDL, low-density lipoprotein; HDL, high-density lipoprotein; OR, odds ratio; CI, confidence interval, NA, not applicable, P < 0·05 defined as significant.
In univariate analysis, patients with unfavourable outcome (mRS 2–6, n = 359) were significantly older, had more severe symptoms, more often large anterior circulation strokes, and more frequently any HT. The stroke aetiologies associated with an unfavourable outcome were large-artery atherosclerosis (LAA) and CAD. Of the baseline laboratory values, lower levels of HDL cholesterol were attributed to an unfavourable outcome (Table 5).
Comparison of patients with favourable and unfavourable three-month outcome
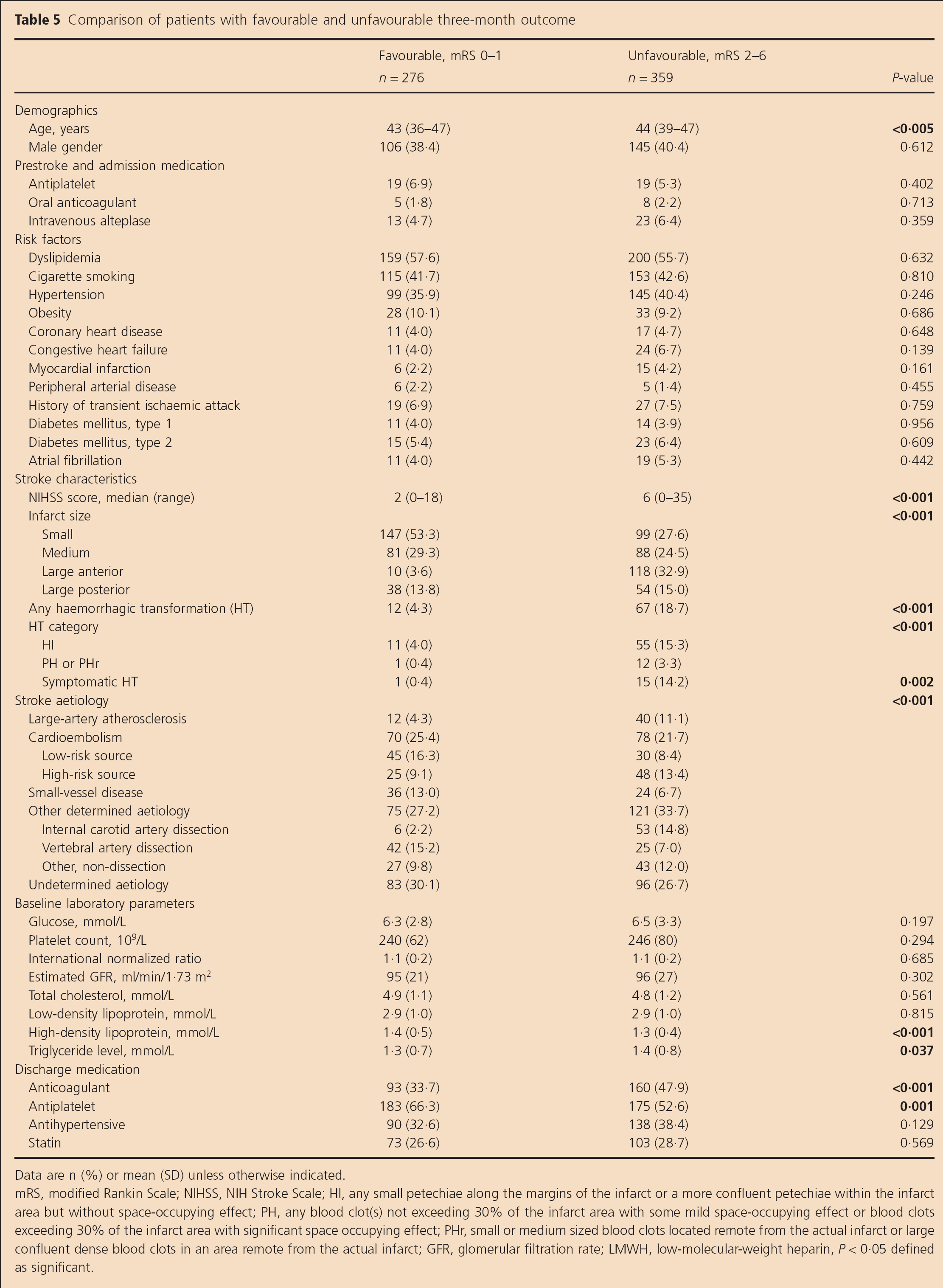
Data are n (%) or mean (SD) unless otherwise indicated.
mRS, modified Rankin Scale; NIHSS, NIH Stroke Scale; HI, any small petechiae along the margins of the infarct or a more confluent petechiae within the infarct area but without space-occupying effect; PH, any blood clot(s) not exceeding 30% of the infarct area with some mild space-occupying effect or blood clots exceeding 30% of the infarct area with significant space occupying effect; PHr, small or medium sized blood clots located remote from the actual infarct or large confluent dense blood clots in an area remote from the actual infarct; GFR, glomerular filtration rate; LMWH, low-molecular-weight heparin, P < 0·05 defined as significant.
In logistic regression adjusted for demographics, stroke severity, lesion size, stroke aetiology, platelet count, and lipid panel components, neither HI (OR 1·76; 95% CI 0·76–4·11; P = 0·190) nor PH or PHr (2·39; 0·23–24·76; P = 0·465) were associated with unfavourable three-month outcome. Increasing age, NIHSS score, lesion size, aetiology of internal CAD, and lower HDL cholesterol levels independently associated with unfavourable outcome (data not shown).
Discussion
This study is the first to report the frequency, factors associated with, and impact on outcome of HT in young adults suffering from first-ever ischaemic stroke. The 12·4% HT rate was similar to that seen in older adults (15), and lower than seen in childhood strokes (4). Any grade of HT (HI, PH, or sHT) was more frequent in patients having unfavourable outcome in our young adults, but not after adjusting for the infarct size, stroke severity, and aetiology. This is in line with some earlier observations (24), although in one study, mild HT was associated with clinical improvement (6) and most trials have found PH2 (6,25) and HI1, PH1, and PH2 to worsen the prognosis (26) in general stroke patients after adjusting for age, stroke severity, and extent of initial focal hypodensity.
In our study population, infarct size and stroke severity were associated with HT and an unfavourable three-month outcome, consistent with previous studies (5,6,27). Age had no effect on HT, like in most studies, where the HT rates have been found to increase only after age of 70 to 75 years in CE infarcts, but not in other aetiologies (14,28) or all study populations (9).
LAA and CAD patients had more often an unfavourable outcome, and small vessel disease (SVD) and vertebral artery dissection patients a favourable outcome. However, only CE of high-risk source was independently associated with HT. Such CE was the most common aetiology of HT in our patients, and although the size of the lesion is not necessarily related to the presence of CE, HT is mostly seen in medium-sized and large CE infarcts (28), as was the case in our study. In earlier studies, CE from a high-risk source, in addition to M1 MCA occlusion, absence of collateral flow (15), baseline NIHSS > 14, and a hypodensity >33% MCA territory have helped to identify the risk of HT, but only delayed recanalization >6 h in CE stroke was associated independently with any HT (11).
Low platelet count is extremely rare (0·3%) in patients with acute ischaemic stroke (29), and is considered as an index of haemostasis. Low platelet count increases the risk of bleeding, and was independently associated with HT in our study in concordance with previous results (5). Although significantly higher levels of total cholesterol and LDL were found in LAA and SVD patients, higher levels of LDL were, independently from the aetiology, in the multivariate analyses associated with HT. Lower HDL levels were in turn associated more often with an unfavourable outcome at three-months. The association of cholesterol levels, acute stroke, and the risk of HT is unclear due to controversial results in different study set-ups. Cholesterol levels have been shown to change in the acute phase (30). Low LDL levels have been associated as HT risk factors in the univariate (31) but not in the multivariate analyses in nonthrombolysed patients (5). sHT instead has been independently associated with low LDL levels, after thrombolysis therapy or thrombectomy (26). Furthermore, in the young stroke patients, low HDL has been associated with an increased stroke risk (32).
The novel finding that high LDL levels are associated with any HT in young adult strokes, and that a low HDL level has more often an unfavourable outcome in the HT patients, could indicate the different risk factor profile in younger stroke patients, who have less generalized atherosclerosis, diagnosed hyperlipidaemia, and statin use. Although high-doses of statin have previously increased the risk of HT (33), it did not have an effect in our study, probably due to the small 3·8% percentage of statin users among the patients. Many of the earlier studies have not only analysed older patients but also smaller and more heterogeneous study populations, and, for instance, the cholesterol levels have differed in timing.
The study has several limitations. It was conducted in a retrospective manner, and the number of patients with HT was relatively small especially with regards to sHT, thereby restricting our ability to evaluate multiple factors. The high level of LDL in the young stroke patients with HT differs from the results seen in older patients, and also requires further confirmational studies in a prospective cohort.
To conclude, in young adults, HT of ischaemic stroke occurred in comparable rates to HT reported in elderly patients. Although HT was more common in severe strokes, it was the lesion size and baseline stroke severity that in this cohort were associated with three-month clinical outcome, not HT per se. However, the small numbers of sHT and the retrospective nature of the study demand further studies to confirm the result.