
Abstract
Background
Dementia is a frequent condition in stroke patients.
Aims
To investigate the effect of dementia on access to diagnostic procedures in ischaemic stroke patients.
Methods
All cases of ischaemic stroke from 2006 to 2010 were identified from the population-based Stroke Registry of Dijon, France. Patients' characteristics were recorded, as was the use of brain computed tomography scans, brain magnetic resonance imaging, electrocardiogram, echocardiography, and Doppler ultrasonography of the cervical arteries. Dementia was diagnosed according to Diagnostic and Statistical Manual of Mental Disorders-IV criteria. Logistic regression models were used to evaluate the associations between dementia and the use of the diagnostic procedures.
Results
Of the 907 patients recorded, 104 were excluded because of death and inability to test cognition. Among the remaining 803 patients, 149 (18·5%) had dementia. Almost all of the patients underwent a brain computed tomography scan and an electrocardiogram during their stay. In contrast, the use of both Doppler ultrasonography of the cervical arteries (79·2% versus 90·2%, P < 0·001), echocardiography (32·9% versus 43·6%, P = 0·02), and brain magnetic resonance imaging (21·5% versus 34·4%, P < 0·001) were significantly lower in stroke patients with dementia than in those without. In multivariate logistic regression, dementia was associated with a lower use of both Doppler ultrasonography (odds ratio = 0·49; 95% confidence interval: 0·29–0·81, P = 0·005), echocardiography (odds ratio = 0·57; 95% confidence interval: 0·37–0·89, P = 0·012), brain magnetic resonance imaging (odds ratio = 0·55; 95% confidence interval: 0·34–0·89, P = 0·015), and a comprehensive assessment (odds ratio = 0·62; 95% confidence interval: 0·40–0·96, P = 0·033).
Conclusion
Demented patients were less likely to undergo diagnostic procedures after ischaemic stroke. Further studies are needed to determine whether this lower utilization could account for the reported excess in recurrent events in these patients.
Introduction
Dementia is a frequent condition in patients suffering from ischaemic stroke (1,2), and the current trend is towards an expected increase because of the ageing population (3,4). Access to standard diagnostic procedures is restricted in demented patients for various diseases such as acute myocardial infarction (5), or cancer (6,7), with, as a result, a poorer prognosis in these individuals. However, data about ischaemic stroke are scarce (8). As the efficacy of the prevention of recurrent events is greatly dependent on a reliable diagnosis of the ischaemic stroke subtype, identifying the factors that could limit access to diagnostic procedures could be of a particular interest.
Aim
The present study aims to investigate the effect of dementia on access to diagnostic investigations in ischaemic stroke patients.
Methods
Study population
This study was based on data obtained from the prospective population-based stroke registry of Dijon, France (152 000 inhabitants). Multiple overlapping sources of information were used to identify fatal and nonfatal stroke in hospitalized and nonhospitalized patients (2,9). For this study, we included patients with a diagnosis of ischaemic stroke defined according to World Health Organization recommendations (10), from 1 January 2006 to 31 December 2010. Patients who died during the acute stage of stroke and those who were not testable for cognitive function were excluded from the analyses.
Data collected
Vascular risk factors and prestroke treatments were collected (2,9). Clinical severity was assessed at admission using the National Institutes of Health Stroke Scale (NIHSS) score, as well as decreased consciousness. We recorded length of stay and the use of the following diagnostic resources: brain computed tomography (CT) scan, brain magnetic resonance imaging (MRI), electrocardiogram (ECG), echocardiography, and Doppler ultrasonography (US) of the cervical arteries. Patients were considered to have had a comprehensive diagnostic assessment if they had undergone all of the following investigations: brain imaging (either CT scan or MRI), an ECG, Doppler US, and echocardiography. Dementia was assessed by a neurologist immediately after the acute stage of stroke, thanks to a simple standardized clinical approach using Diagnostic and Statistical Manual of Mental Disorders (DSM)-IV (11), as previously described (2). Hence, both patients with prestroke dementia and those who developed dementia soon after their stroke were identified.
Statistical analysis
Baseline characteristics were compared using the chi-square test and the Wilcoxon test when appropriate. Associations between dementia and the use of each diagnostic procedure were analysed using logistic regression to obtain odds ratios (OR) and 95% confidence intervals. Age, length of stay, and NIHSS scores that did not satisfy the log-linearity assumption were included in the models as stratified variables. In multivariate models, we introduced dementia, age, gender, and all variables with a P-value <0·20 in unadjusted models. A backward elimination procedure was performed using the likelihood ratio test to obtain the final models that included the significant confounders, as well as dementia, age, and gender. Stratum-specific analyses were performed within categories according to the identification of significant statistical interaction terms along with dementia. P-values <0·05 were considered statistically significant. Statistical analysis was performed with STATA ® 10·0 software (StataCorp LP, College Station, TX, USA).
Ethics
Our registry was approved by the National Ethics Committee and the French Institute for Public Health Surveillance.
Results
Nine hundred seven patients with ischaemic stroke were recorded, and 104 were excluded from the analyses because they died soon after the acute event, or because cognitive function could not be tested. Among the remaining 803 patients, 149 (18·5%) had dementia. Characteristics of patients are shown in Table 1.
Characteristics of ischaemic stroke patients according to dementia
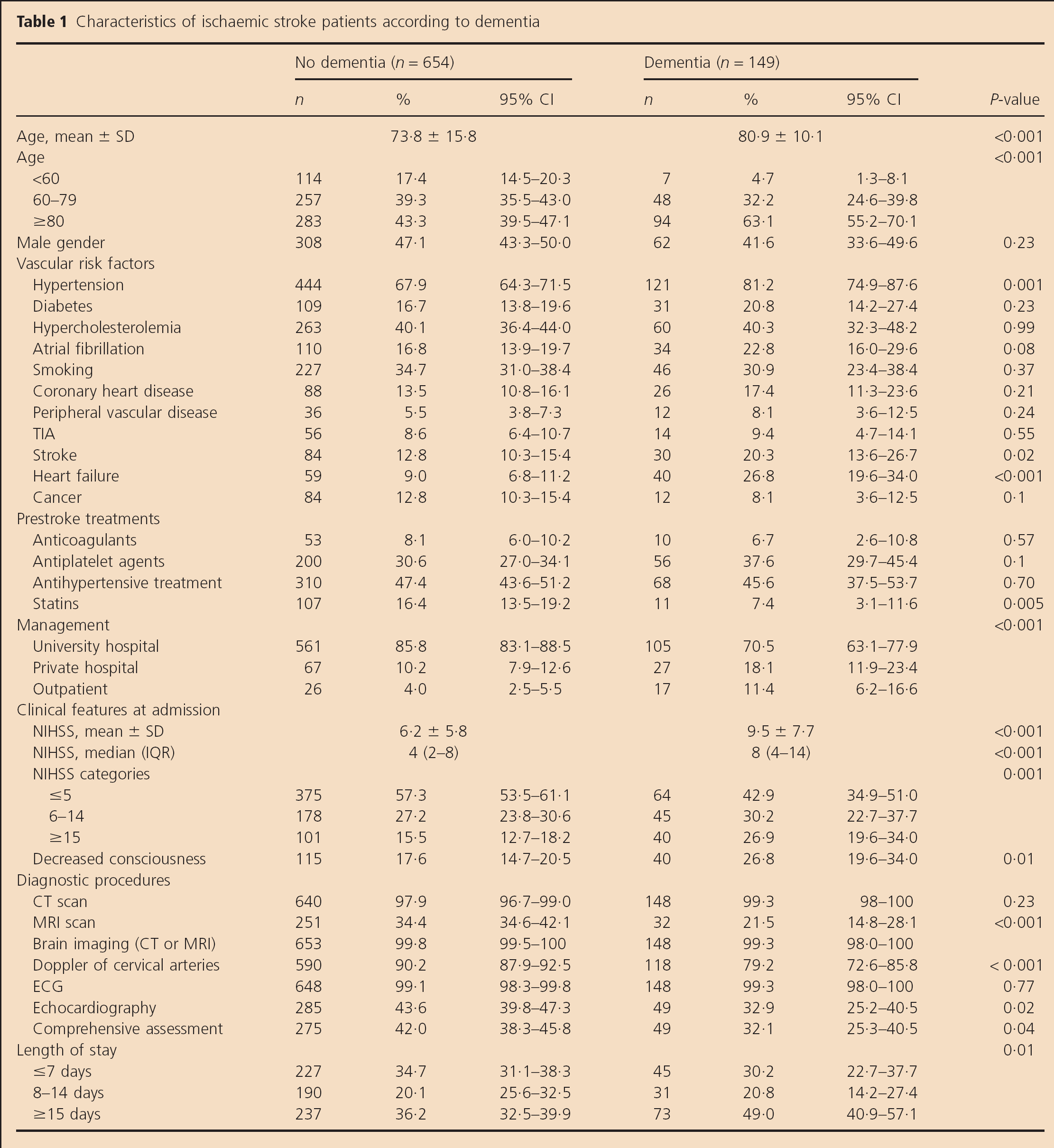
Almost all of the patients underwent a brain CT scan and an ECG during their stay. In contrast, the use of Doppler US of the cervical arteries, echocardiography, and brain MRI were lower in stroke patients with dementia than in those without. After multivariate logistic regression (Table 2), dementia was independently associated with a lower use of Doppler US (OR = 0·49, P = 0·005). In stratum-specific analyses, this association was significant in men (OR = 0·23, P < 0·001), and in patients with previous atrial fibrillation (OR = 0·22, P = 0·003) and those without heart failure (OR = 0·33, P < 0·001). Dementia was also associated with reduced access to both echocardiography (OR = 0·57, P = 0·012), especially in patients with decreased consciousness (OR = 0·37, P = 0·038), and brain MRI (OR = 0·55, P = 0·015). In stratum-specific analyses, the negative association between dementia and the use of brain MRI was observed in patients <80 years old. Finally, dementia was a predictor of not benefiting from a comprehensive diagnostic assessment after ischaemic stroke (OR = 0·62, P = 0·033).
Multivariate analyses of predictors of the use of diagnostic procedures in ischaemic stroke patients
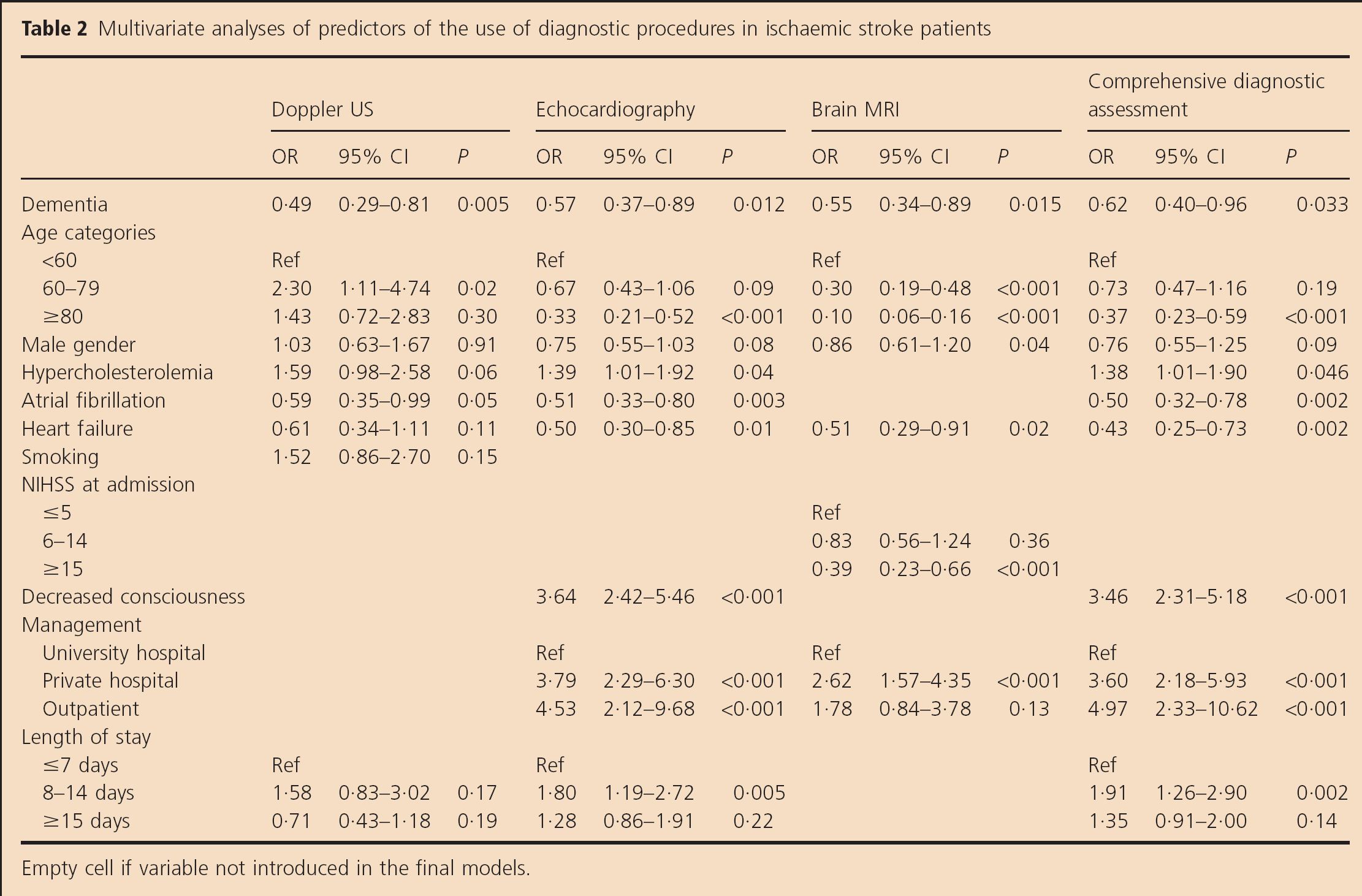
Empty cell if variable not introduced in the final models.
Discussion
Dementia was associated with a lower utilization of most of the diagnostic procedures for the assessment of ischaemic stroke subtypes.
There was no difference between patients with dementia and those without with regard to the utilization of brain CT scans and ECGs, which were both performed in about 99% of cases. This rate appeared to be much higher than that reported elsewhere (8,12,13), and may reflect easier access to these exams in our community, which is probably related to particularities in the local organization of health care. In contrast, the use of other procedures was considerably lower in patients with dementia, and only one-third of them benefited from a comprehensive diagnostic assessment, which is required to establish an accurate classification of patients according to the underlying stroke mechanism. These findings are consistent with those from a recent hospital-based study that reported a lower frequency of the use of both carotid imaging and cardiac investigations in ischaemic stroke patients with preexisting dementia (8).
Several explanations could account for these results. The medical attitude towards demented patients could differ from that towards nondemented patients, and a practical approach in the management of these patients could be more usual, as suggested by the fact that invasive procedures and treatments are less frequently prescribed for them in various diseases (5,14–16). Such an attitude may result from the assumption according to which both the application and the impact of the possible interventions arising from the findings of these procedures on the prognosis of demented patients could be limited. Another explanation could be the occurrence of delirium during the acute stage of ischaemic stroke, which is more frequent in stroke patients with cognitive impairment (17), and could make the doctor reluctant to perform various investigations that require the patient to be calm and compliant.
The population-based design of our study avoided selection biases related to a hospital-based methodology, and consequently ensured a clear representation of the ‘real life’ care of stroke patients. As diagnosis of dementia was always made in the early stages of stroke, we think that it could have influenced the attitude of the primary care physicians regarding further investigations. However, as it was only based on DSM-IV criteria (11), several cases may have been missed, all the more so as patients who died soon after the acute event were excluded. Nevertheless, it can be assumed that it would have resulted in an underestimation of our findings.
Conclusion
Demented patients were less likely to undergo diagnostic procedures after ischaemic stroke. Further studies are needed to determine whether or not this lower utilization is clinically relevant or whether it represents discrimination on the basis of dementia. Moreover, another challenge would be to establish whether these differing rates of utilization of diagnostic procedures could account for the previously reported excess in recurrent events in these patients (18,19), and whether improving the diagnostic assessment could reduce this trend.