
Abstract
Background
Surgical approaches have been developed to enhance exposure and facilitate operative procedures. Some approaches are not commonly used or preferred due to prolonged learning curves and higher risk of iatrogenic injuries, which can be distressing to both the patient and the surgeon. The antero-superior approach provides good exposure to the rotator cuff, the anterior and posterior aspects of the shoulder and the glenoid. This approach is gaining popularity as a preferred exposure for shoulder arthroplasty as well as trauma surgery. Knowledge of the axillary nerve anatomy, however, is vital in this approach; in order to avoid injury.
Method
We have dissected the axillary nerve in six cadavers and measured its distance from inferior reflection of the subdeltoid bursa.
Results
The axillary nerve was at least 1.5 cm distal to the bursa in all cases.
Conclusion
The deltoid muscle can safely be split to the level indicated by a finger placed into the inferior recess of the subdeltoid bursa. This method uses the patient's own anatomy, and does not rely on nonstandard data, or unreliable points of reference such as the acromion and offers a reliable guide for the use of this approach safely.
Introduction
Surgical exposures of the shoulder are guided by internervous planes and limited by the vascular and nervous structures. The antero-superior or Neviaser-Mackenzie approach [1] has gained popularity in shoulder surgery for its use in arthroplasty, open rotator cuff surgery and, occasionally, fracture fixation.
The approach does, however, threaten the axillary nerve over its course as well as branches innervating the deltoid. This paper investigates the relationship of the inferior reflection of the subdeltoid bursa (Fig. 1), and the position of the axillary nerve as it courses around the proximal humerus.

Finger tip in the subdeltoid bursal reflection.
Standard texts relating to surgical approaches to the lateral aspect of the proximal humerus describe the limit of permissible splitting of deltoid muscle to avoid axillary nerve injury to 5 cm distal to the acromion [2], [3]. Vathana et al. [4], however, concluded that the acromion is not a reliable reference point with respect to the position of the axillary nerve. Patient morphology and size also vary enormously, making a standard distance measured from the acromion invalid [5].
With this uncertainty as to the position of the nerve, the options seem to be to dissect out the nerve on each approach, or limit the dissection with safety margins.
Following the clinical observation that the inferior reflection of the subdeltoid bursa does not extend to a level that would compromise the axillary nerve [6] and that the axillary nerve lies distal to the reflection, a cadaveric study was set up to explore the relations between the subdeltoid bursal reflection and the axillary nerve.
Methods
Six cadaveric specimens were dissected to identify the axillary nerve coursing through the quadrangular space, around the humerus applied to the deep surface of the deltoid muscle. There were two female and four male cadavers. Three left shoulders and three right shoulders were examined. The arms were placed in neutral by the side of the trunk to correspond with the arm in the beach chair position. The subdeltoid bursa was opened superiorly, and a finger placed into its most distal reflection, without applying any pressure (Fig. 1). The vertical distance from finger tip to the nearest portion of the nerve was then measured using calipers (Fig. 2).
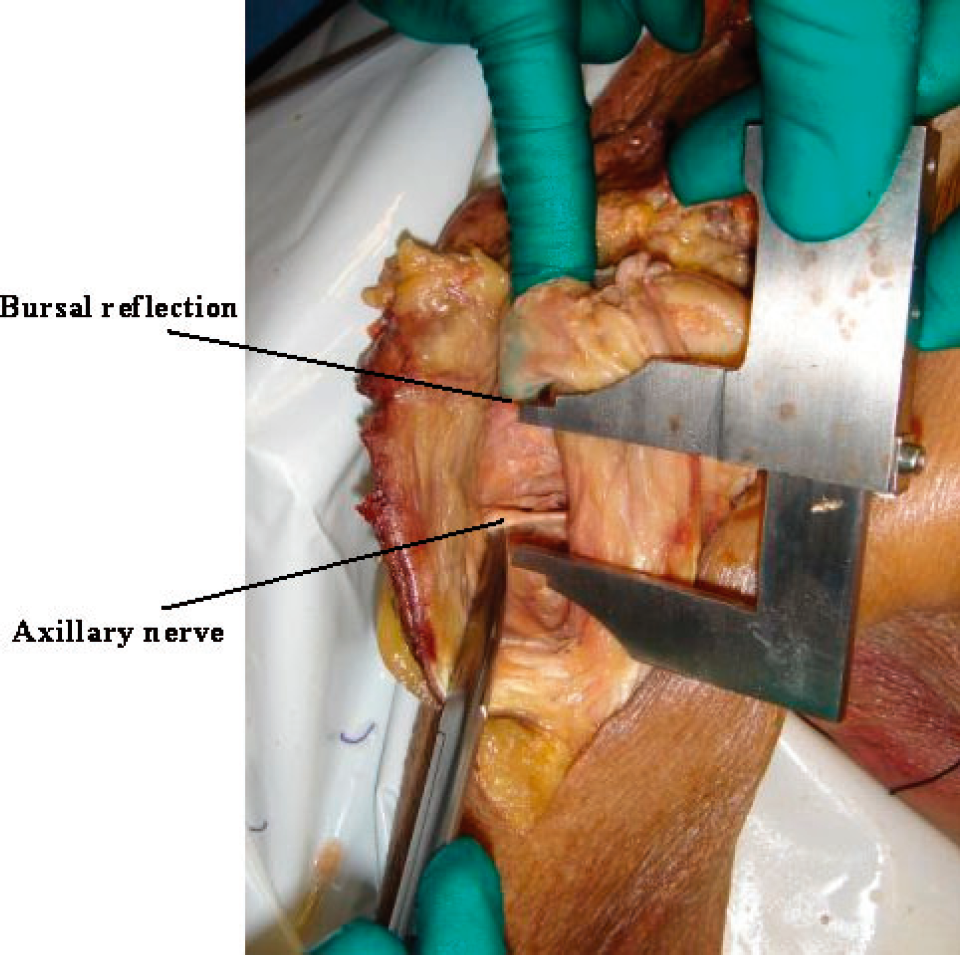
This demonstrates the distance between the inferior extent of the bursa and the axillary nerve.
Results
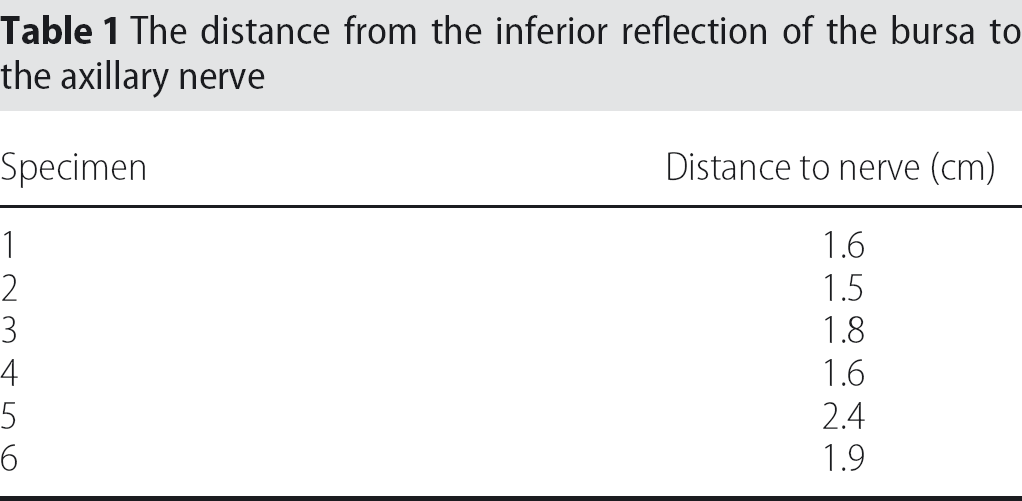
In all the cadaveric specimens, the axillary nerve was distal to the inferior reflection of the bursa. The average distance between the bursal reflection and the axillary nerve was 1.8 cm (1.5 cm to 2.4 cm), and no finger was closer than 1.5 cm (Table 1).
The distance from the inferior reflection of the bursa to the axillary nerve
Discussion
Beals et al. [6] have previously described the relationship of the axillary nerve to the bursa. Based on this, our surgical experience, and this anatomical study, we found that palpating the inferior reflection of the subdeltoid bursa was a reliable and safe indicator for the distance allowable to split deltoid muscle during shoulder surgery, without causing injury to the axillary nerve. We have found that this marker is easily recognized and reliable, even in trauma cases.
At surgery, using the Neviaser-Makenzie approach, the deltoid can safely be split to the level indicated by a finger placed into the inferior recess of the subdeltoid bursa. This method uses the patient's own anatomy, and does not rely on non-standard data, or unreliable points of reference such as the acromion.
To our knowledge this finding is not commonly appreciated by orthopaedic surgeons. Utilizing this technique and using the inferior extent of the bursal reflection as a landmark of the distal extent of the deltoid split, improves the safety of deltoid splitting approaches to the shoulder.