
Abstract
Background
Very few longer term follow-up of unlinked elbow replacements have been published and most series are small.
Methods
Since 1994 87 Kudo 5 total elbow replacements in 70 patients were undertaken by two specialist elbow surgeons (LN and MT) for adult rheumatoid arthritis. These were evaluated at a mean follow-up of 79 months (29 months to 137 months) using the Mayo Clinic performance index. Post-operative radiographs were also reviewed for loosening using standard antero-posterior and lateral films.
Results
Eight patients were lost to follow-up and 16 patients had died leaving 62 total elbow replacements in 46 patients. Pre-operatively 6 had moderate pain and 56 had severe pain. Post-operatively the pain was rated as none by 58 and moderate by 4. The average Mayo elbow score improved from 37 pre-operatively to 86 post-operatively. The flexion extension arc improved from 60? to 99?, whilst pronation and supination improved by 18? and 20? respectively. The overall complication rate was 24% with ulnar neuropraxia being the commonest problem. Six cases were revised, four for aseptic loosening and two for sepsis. The ulnar component was the more commonly affected and appeared to be the cause of more problems. However with revision as the endpoint, the probability of survival of the Kudo 5 at 79 months using the Kaplan Meier method was 96% reducing to 86% at 100 months.
Conclusion
The results of the Kudo 5 total elbow replacement in patients with adult rheumatoid arthritis are acceptable and comparable with other reported series and to other unlinked implants with similar follow-up.
Introduction
The elbow joint is affected in a large proportion of patients with rheumatoid arthritis. After 15 years of the disease almost two out of three patients with rheumatoid arthritis show definite involvement of the elbow joint [1].
The options for surgical treatment include synovectomy with or without radial head excision, interposition and excision arthroplasty or total elbow replacement. Those joints that would be considered for elbow replacement due to severe erosions with Larsen grade four to five changes [2] are seen in 11% of adult rheumatoids, whilst such significant joint destruction, when it occurs is most often bilateral and therefore causes much disability [1].
Elbow prostheses can be classified as linked and unlinked. The Kudo 5 implant belongs to the unlinked group and has been in clinical use since 1994. It was developed by modification of the Kudo type 4, which had a reported complication of implant fracture at the shell stem junction of up to 31% [3], [4]. This area was therefore reinforced following which there have been no reports of fracture of the type 5 implant. The humeral component is made of cobalt chrome alloy whilst the ulnar component, which has a straight stem, is titanium; both are available in cemented and uncemented forms. The metal backed ulna has a 3 mm polyethylene bearing surface.
In an in vitro biomechanical study looking at the ulnotrochlear joint of five unlinked elbow prostheses it was found that implants that resemble the human elbow in appearance do not necessarily replicate its behaviour and that despite the Kudo type 5 not resembling the human elbow, it was one of only two implants that most closely approximated the normal elbow constraint behaviour [5].
Patients and Methods
Our study represents a long term follow-up of the Kudo 5 total elbow prosthesis in a group of patients with rheumatoid arthritis from two different hospitals, one teaching hospital and one District General hospital. Since 1994, 87 elbow replacements were performed in 70 patients with adult rheumatoid arthritis using this prosthesis. The indication for arthroplasty was intractable pain with reduction in movement resulting in significant loss of elbow function.
The mean age at the time of operation was 65 years (42 years to 87 years). Sixteen patients had died at the time of follow-up and 8 patients were untraceable leaving 62 total elbow replacements in 46 patients. These were reviewed at an average follow-up of 79 months (29 months to 137 months). There were 35 female and 11 male patients. Sixteen patients had bilateral elbow replacements, of which 12 were female and 4 male.
Six elbows had previously undergone synovectomy and radial head excision.
Patients were assessed pre- and post-operatively by the Mayo Clinic elbow performance index [6]. Pre-operatively elbows were also classified using antero-posterior radiographs into 48 type IV and 12 type V according to the Larsen grading [2]. Although the Kudo 5 prosthesis has been described for the treatment of mutilating rheumatoid arthritis where there is severe erosion [7], patients with gross instability and major bone loss are treated with linked implants in our units, due to the potential of instability in such cases. Antero-posterior and lateral radiographs were done at follow-up to assess the position of the implant and for any signs of loosening.
Survivorship analysis was also performed with the Kaplan Meier technique using revision as the endpoint.
Operative technique
Surgery was performed in all cases by the senior authors (LN and MT). The surgical approach was similar in the two units using a modified posterior approach. A tongue of triceps aponeurosis was raised from the underlying triceps muscle separating it from the triceps raphe. Extending this on the lateral side allowed the lateral head of triceps and anconeus to be mobilized and retracted as a single unit. The radial head if present was resected and the ulnar nerve was decompressed within the cubital tunnel and between the two heads of flexor carpi ulnaris. It was retracted during the surgery with its surrounding soft tissues and vessels so as not to devascularize the nerve. At the end of the procedure the nerve was restored to its original position and was not transposed. On the medial side the triceps raphe was incised 2 cm proximal to its insertion and the medial and deep heads of triceps were reflected medially exposing the distal humerus. The medial collateral ligament was released in its entirety to allow dislocation of the elbow. Releases were also done on the lateral side to balance the elbow which, as it was unlinked, relied on a balanced soft tissue envelope for the components to track correctly and therefore maintain joint stability.
All the ulna prostheses were cemented. Thirty five humeral components were inserted without cement and 27 were cemented.
Post-operatively an extension splint was used at night for 4 weeks in 32 elbows and 2 weeks in 30 elbows presenting the only difference in the management in the two units.
Results
Mayo elbow performance index
The average pre-operative score was 37 and this improved to 86 post-operatively. A score of ≥ –90 is considered an excellent result; 75 to 89 points, a good result; 60 to 74 points, a fair result; and ≤ –60, a poor result. On this basis 21 patients had an excellent result, 32 had a good result, 5 patients had a fair result and 4 patients had a poor result (Figs 1 and 2).
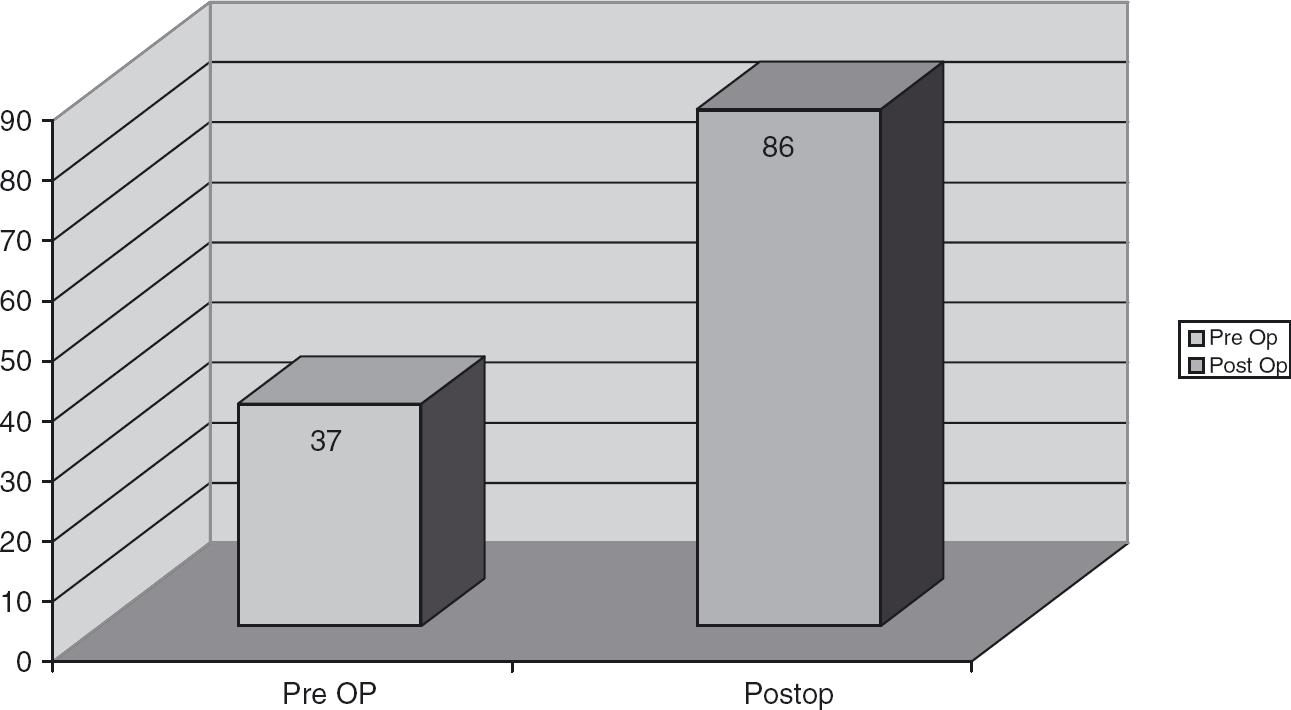
Kudo 5 total elbow arthroplasty results—overall Mayo Clinic performance.
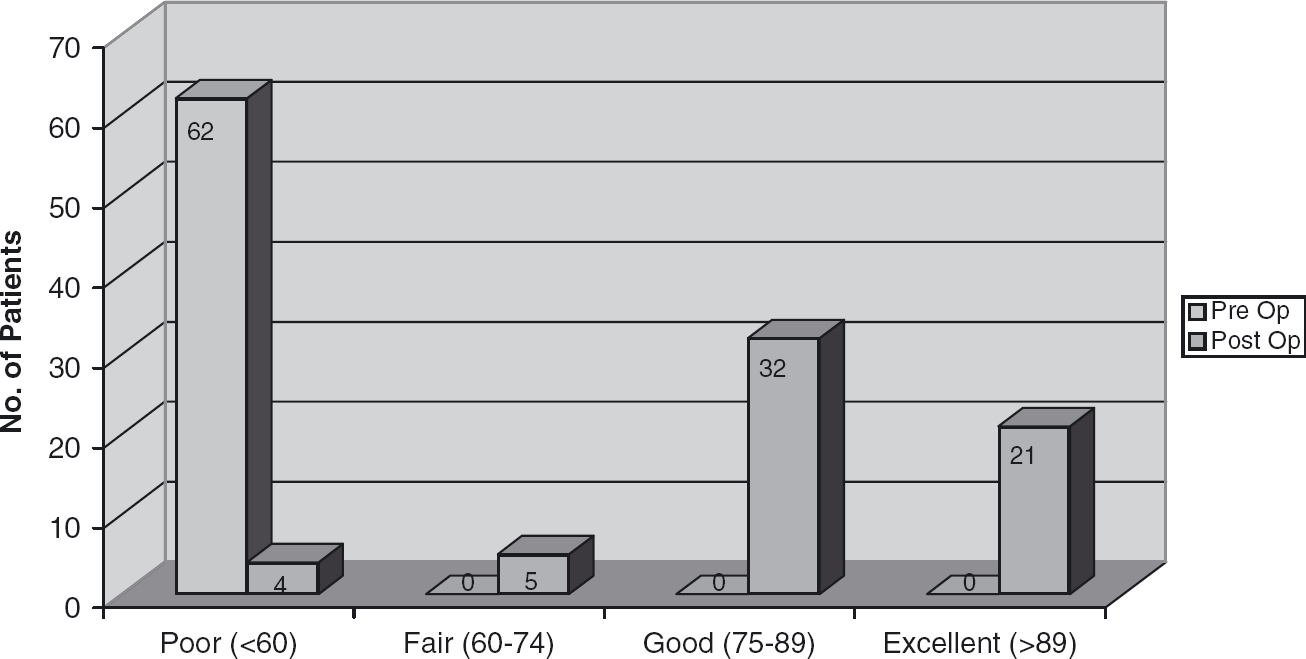
Results—breakdown of Mayo Clinic performance score.
Pain relief
Pre-operatively 56 patients had severe pain and 6 patients had moderate pain. Post-operatively the pain was rated as none by 57 patients and moderate by 5 patients. No patient had severe pain post-operatively (Fig. 3).
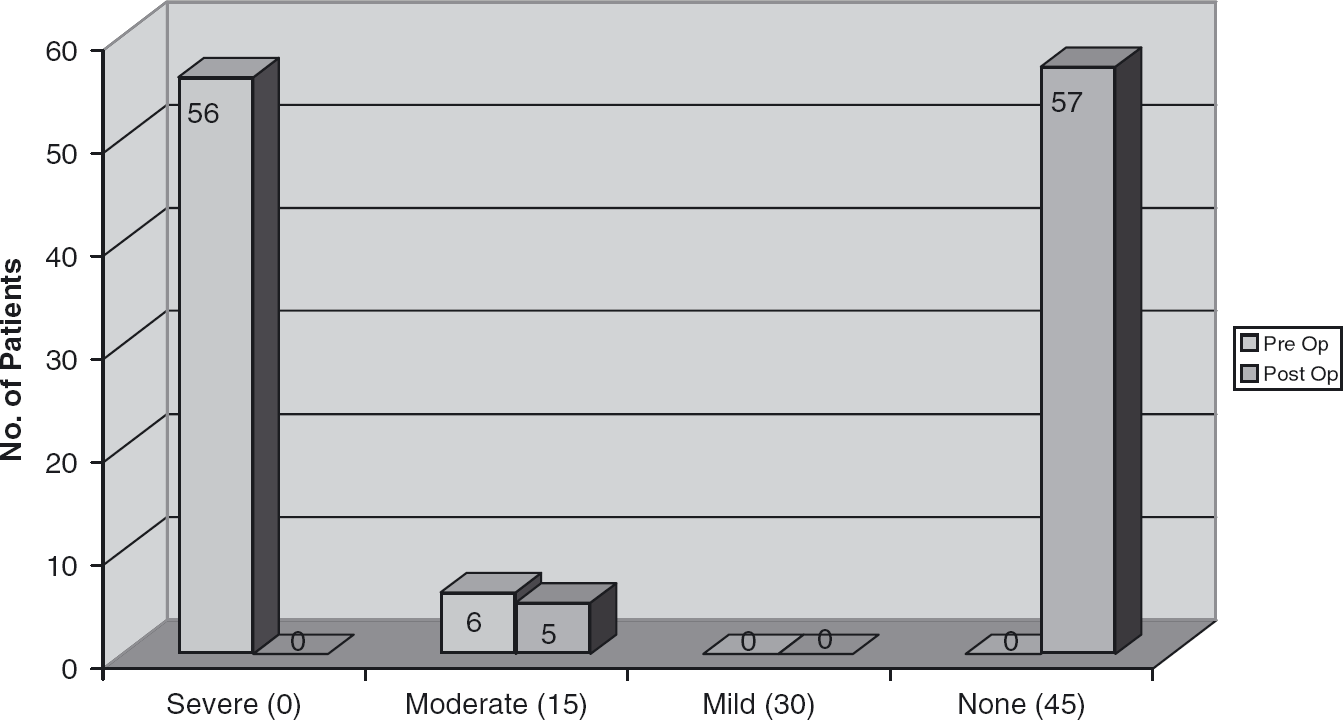
Results—Mayo Clinic performance pain score.
Motion
Pre-operatively the elbows had an average arc of flexion from 46° to 106°, with 53° of pronation and 39° of supination. Post-operatively the average flexion arc was 31° to 130°, with 71° of pronation and 59° of supination. This therefore represented an average improvement in the flexion extension arc from 60° pre-operatively to 99° post-operatively with an 18° and 20° increase in pronation and supination respectively (Figs 4–6).
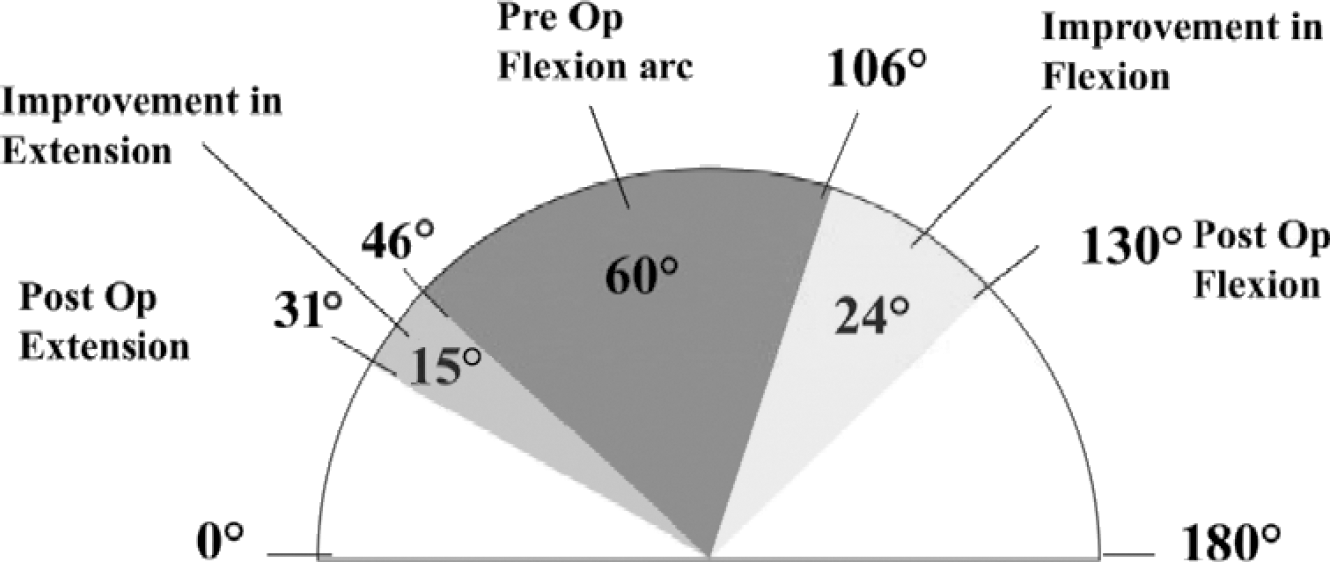
Results—arc of movement.
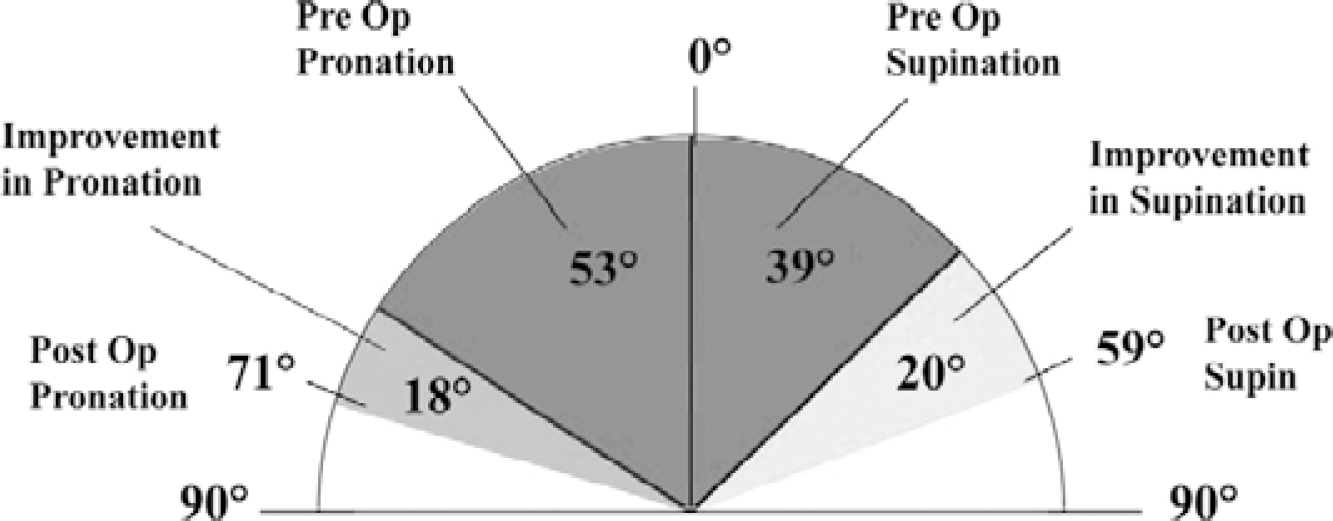
Results—forearm rotation.
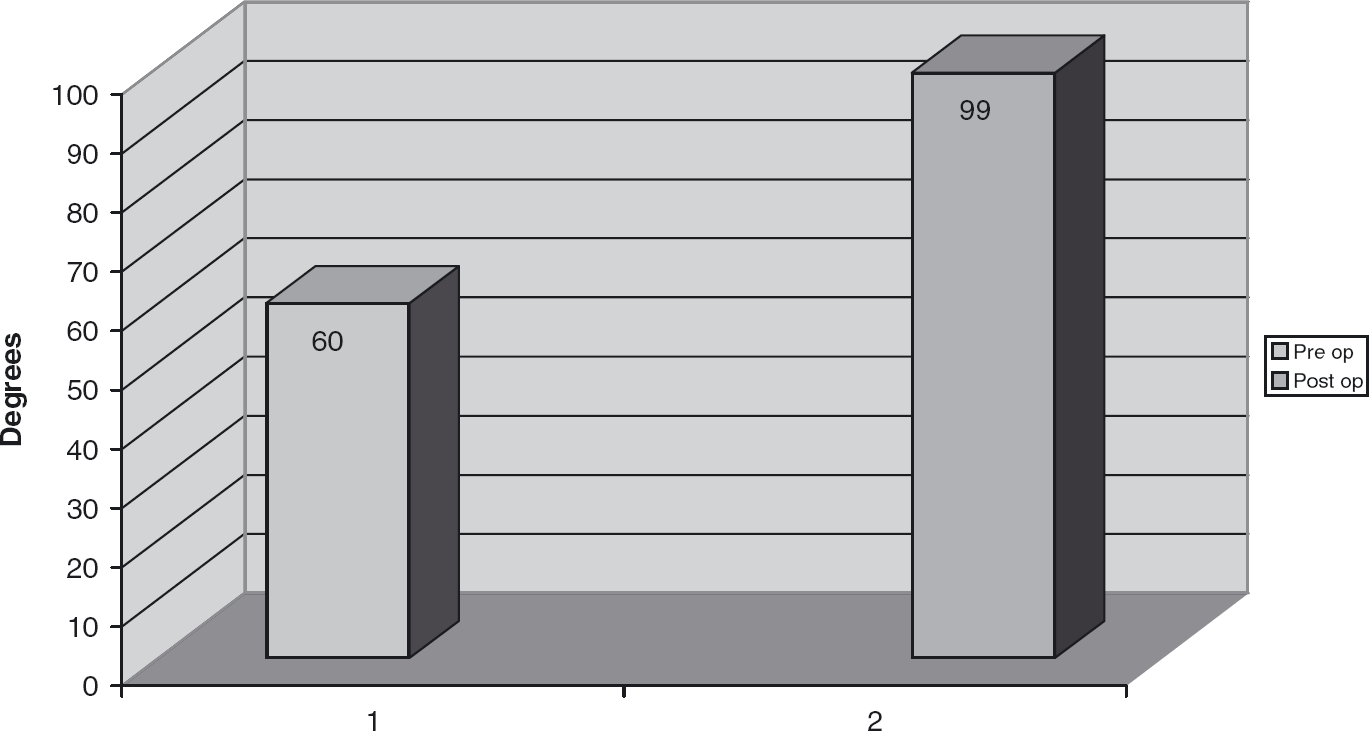
Results—Mayo Clinic performance score—arc of flexion.
Activities of daily living
Activities of daily living are scored to a maximum of 25 in the Mayo index. This improved dramatically from 3 patients with a score of 21 to 25 pre-operatively to 35 patients with the same score post-operatively. The other patients' scores are shown in Fig. 7.
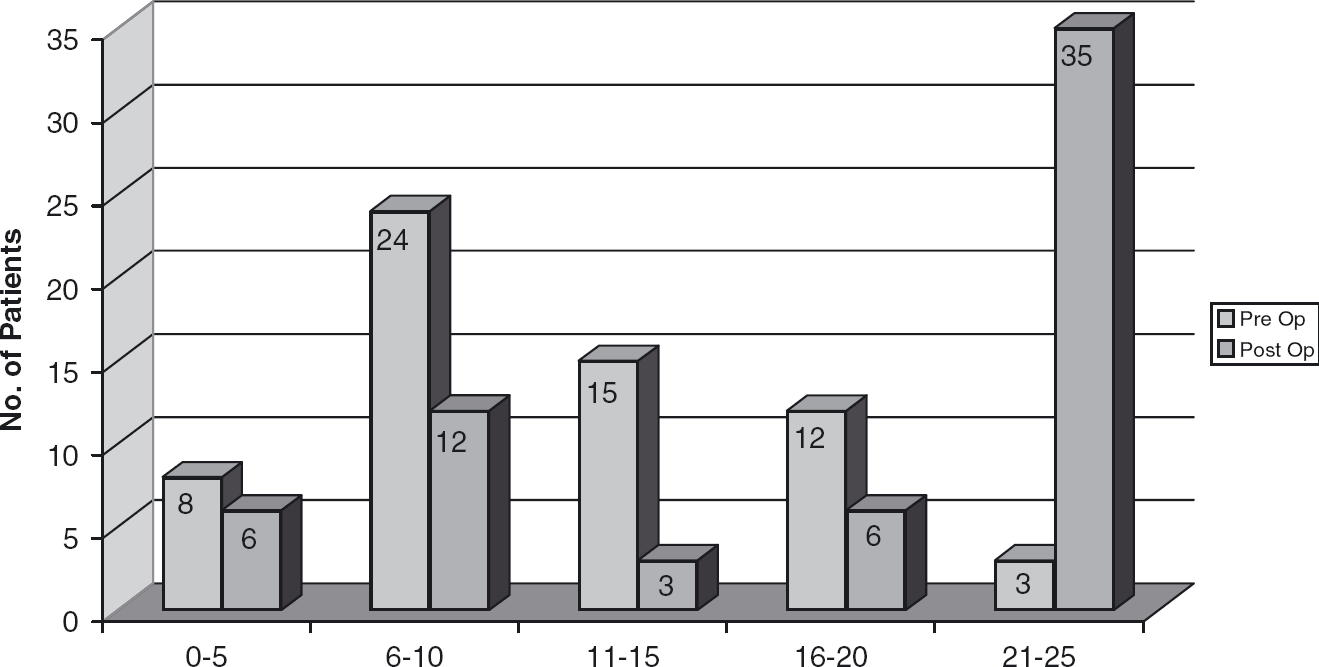
Results—daily function (25/100) (combing, feeding, hygiene, shirt, shoes).
Overall Results
There was no difference in results between patients who had cemented or uncemented humeral components and the results were similar in patients with previous synovectomy and radial head excision.
There was no difference in the extension gain between those patients using night extension splints for 2 as apposed to 4 weeks.
Radiographic analysis
Post-operatively no significant radiological changes were seen in 44 elbows. Thirteen elbows showed radioluscent lines of less than 1 mm. Five ulna components and two humeral components showed lucent lines of greater than 1 mm signifying loosening. All but one of these components was revised. Valgus tilting of the ulna component was seen in eight elbows.
Survivorship analysis
The survivorship curve is shown in Fig. 8. This showed that using revision as an end point overall survivorship of the Kudo 5 prosthesis was 96% at 79 months and 86% at 100 months. Further predictions about longer survival become unreliable as there were small numbers of patients at risk beyond 8.3 years.
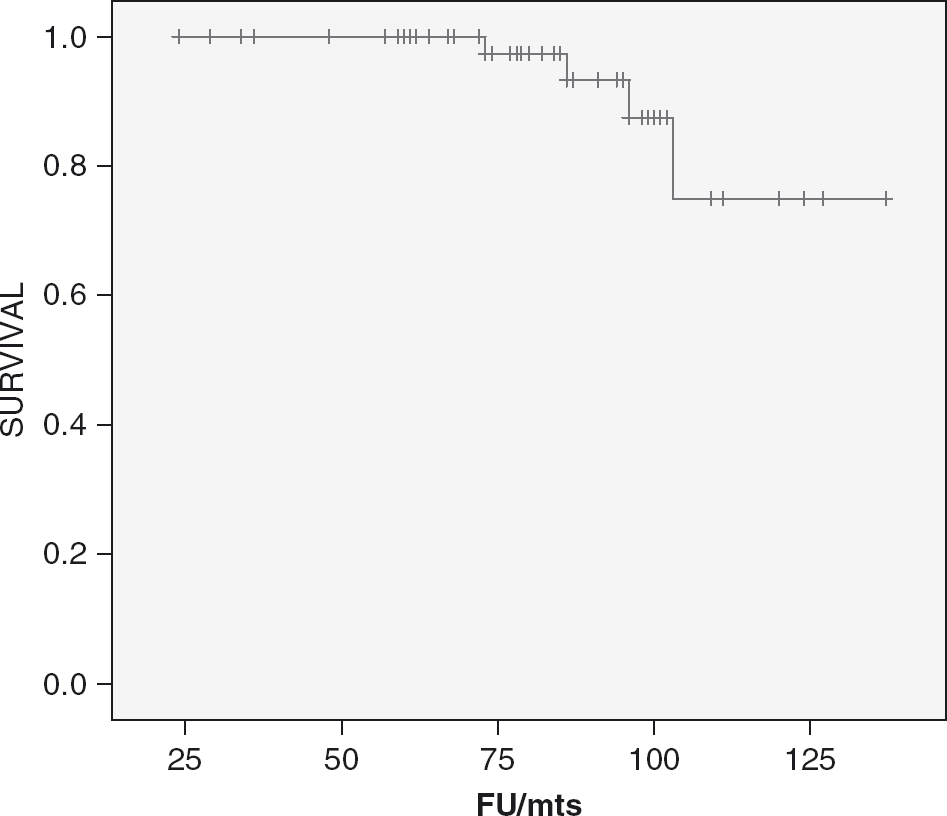
Kaplan Meier survival rate using survivorship with revision as the endpoint.
Complications
Ulnar nerve neuropraxia was seen in four patients (6.4%) post-operatively but had resolved at the time of follow-up.
There were two fractures (3.2%) of the medial condyle intra-operatively which were secured with k wires. The fractures united without further complication (Fig. 9).

Intra-operative fracture of the medial column fixed with two k wires.
Two elbows dislocated post-operatively (3.2%), one of which was reduced closed whereas one required open reduction. Both cases stabilized after treatment with no symptoms of further instability.
There was one post-operative triceps rupture (1.6%) occurring at 1 year which required repair. This patient made a good recovery achieving a functional 100° arc of flexion within 3 months of surgery.
Six elbows underwent revision procedures (9.6%).
Two were done for sepsis (3.2%), of which one elbow, with septic loosening of both components, was revised to a further Kudo prosthesis by a two stage operation. The other infected elbow was salvaged to an excision arthroplasty following a deep infection secondary to an insect bite over the elbow. Both components were found to be solidly fixed but were removed because of systemic sepsis and the potential to cause infection in the patient's other multiple joint replacements. The patient continues to have good painless function from his excision arthroplasty and has declined further surgery.
Four elbows were revised for aseptic loosening (6.4%) involving three ulna components and one humeral component. All the ulna components revised showed valgus tilting. One long stem humerus (Fig. 10) was used to revise an uncemented standard component which loosened early. At operation the ulna was solidly fixed without evidence of wear while there was no evidence of bony in growth to fix the humeral stem. Revision with a long uncemented stem was successful and at 8 years the patient has a pain free and functional joint. One long stem ulna component (Fig. 11) was used whilst the other two ulnas were revised with standard components. In revisions for aseptic loosening of the ulna components it was noted that the implant had consistently worn more on the radial side of the implant. Two components had eroded through the relatively thin polyethylene into the metal base plate resulting in instability of the elbow as shown in Figs 12 and 13. This occurred in one of the patients who had sustained an intra-operative fracture of the medial condyle but this had not compromised the humeral fixation which was solid at the time of the revision. All elbows revised for aseptic loosening have made good recoveries without complications and have regained functional elbow movement with Mayo performance index scores above 80.

Revision using long stem humeral component.

Revision using long stem ulna component.

Ulna component—showing valgus tilt with severe erosion on radial side of implant causing instability.

Ulnar component retrieved from elbow in Fig. 12.
The overall complication rate in this series was 24%, but 12.8% were significant requiring further surgery.
Discussion
The inventor reported his results using the Kudo type 5 prosthesis in patients with rheumatoid arthritis in 1999 [8]. There were 43 elbows in 37 patients with a mean follow up of 46 months. All humeral components and 32 ulnar components were uncemented. He reported excellent pain relief with improved flexion but without any increase in extension. One patient dislocated but no other complications were recorded and no elbow showed any evidence of loosening. These results have not been replicated in other units reporting their results using this implant.
Dislocation
Most series reporting the use of this elbow replacement record cases of dislocation [4], [8]–[11] which is a complication of unlinked implants. The incidence of two cases in our series is, therefore, no greater than reported by others using this prosthesis.
Cemented vs uncemented humerus
Ours is the only comparative study of cemented vs uncemented humeral implants but it failed to show any difference in results, complications or survival.
Ulnar component
Kudo is the only author who has reported no loosening in using the uncemented ulnar component [8]. Van de Heide et al. [12] in a comparative study of cemented and uncemented ulnar components showed a significant loosening rate of the latter with a revision rate of 7 out of 49 cases and a further 7 cases showing progressive radiolucencies. They concluded that the ulnar should always be cemented, which we have done exclusively in our patients. However, even if cemented, the ulnar component is both more commonly the site of radiological loosening and is revised for aseptic loosening [3], [9], [10], [13]. The concern with this ulna component is the thickness of the polyethylene which is only 3 mm. This metal backed ulna component has, however, been found to be superior to an all polyethylene cemented component of the same shape in a long-term study (10 years to 13 years) using the Kudo 5 humeral stem [14].
Ulnar tilting/malalignment
Valgus tilting of the ulnar component has previously been noted by Little et al. [11]. In their series of 33 Kudo implants such tilting was seen in six cases of which four were revised for loosening. They postulated that such tilting led to point loading of the polyethylene and wear which had previously been suggested by Potter et al. [9], although they did not give an incidence of such tilting in their series and no patients had undergone revision to retrieve any ulnar components. We have seen eight cases of tilting with three requiring revision. In all three cases of ulnar component revision for aseptic loosening, wear of the polyethylene on the radial side was noted which supports this theory as to the mode of failure (Fig. 12). The cause of the valgus tilt may be due to the natural history of the rheumatoid elbow which seems to turn into valgus during rheumatoid destruction. Excision of the radial head, however, may speed up this process [15] by accelerating the weakening of the medial capsuloligamentous complex [3]. Component malpositioning may also be a factor in that the humeral component requires the stem and the shell to be aligned so that the articular axis is correctly orientated to the anatomical axis of movement [9]. At the same time the ulnar component needs accurately placing especially in a rotational plane [12] which if not correct will result in tilting. Being an unlinked implant correct soft tissue balancing is also required to achieve correct alignment and stability.
Synovectomy vs nosynovectomy
Previous synovectomy and radial head excision was performed on 6 patients out of 87 in our series but the results, complication rate and survival was similar to those who had not had such surgery. This has previously been reported both for the Souter-Strathclyde [16] and the Kudo [10] prostheses. Our series, therefore, supports the latter and disagrees with the view that those patients who have had synovectomy and radial head excision fair worse with total elbow replacement [17] or that the post-operative complication rate is higher [18], [19].
Survivorship
Survival of this implant has been shown to be good with 86% surviving at just over 8 years in our series. This survival is also similar to that reported from other centres using this implant [9], [11]–[14]. We still, however, have only a mean follow up of 6 years and 7 months and whilst this is the longest so far reported for the Kudo type 5 implant, it is much less than for other prostheses.
Results of elbow arthroplasty in excess of 10 years are now available for linked and unlinked implants [20]–[23]. These show survivorship figures of 92.4% at 10 years for the Coonrad-Morrey (Zimmer) and 87.7% at 13.5 years for the GSB III (Sulzer) linked implants [20], [21]. Similar results are reported for the unlinked Souter-Strathclyde (Howmedica) with an 87% survival at 12 years. These figures have all been surpassed by the Kudo type 3 implant, which is no longer available. Its design was similar to the current Kudo 5 except that the humerus was made of stainless steel and the ulnar component was entirely polyethylene, with both components being cemented. Its inventor has reported an overall survival rate of 90% at 16 years. However 100% of the humeral components showed evidence of progressive radiolucency indicating loosening although the mean Mayo performance index scores were still 77 at 11 years to 16 years follow up. Interestingly in this series only 4 out of 50 ulnar components showed evidence of radiolucency which is in contrast to when the all polyethylene component is used with the uncemented Kudo type 5 humeral stem [14]. It is our assumption that there has been an improvement in the fixation of the type 5 stem into the humerus, whether cemented or uncemented, and that forces are then transmitted to the less well fixed ulnar component resulting in loosening, especially if there is any abnormal ulnohumeral orientation.
Complication rate
The complication rates quoted for elbow arthroplasty in the rheumatoid vary considerably. Gschwend et al. [24] reported an overall rate of 43% on reviewing the literature from 1986 to 1992 whilst Little et al. [25] extended their review of the literature in the English language to 2003 and found rates reported from 14% to 80% with a median of 33%. A recent large series in the German literature of over 170 cases of primarily linked but also unlinked implants performed between 1987 and 2005 still recorded a complication rate of 34.4% [26] which would support Little's figures and would suggest that even with the development of implants and techniques improvement in complication rate has been marginal over the last 20 years. Our figure of 24% is therefore slightly lower than the average reported.
In conclusion the Kudo elbow prosthesis has undergone considerable modification since the prototype was developed in 1972 culminating in the introduction of the Kudo type 5 in 1994 when it started to be used in our two units. The reason for its use to us was that it requires minimal bone resection for its insertion and thus theoretically is bone sparing in this rheumatoid group of patients, where maintenance of bone stock has advantages. We have shown similar results, complications and survival using this implant despite using both cemented and uncemented humeral components. The ulnar component remains the problematical part of this prosthesis being more commonly affected by aseptic loosening and malalignment (tilting). The results achieved are comparable to other series of unlinked implants currently being used [16], [22], [27] but longer follow up is required.