
Abstract
In order to improve results of shoulder arthroplasty in cuff deficient shoulders constrained or reverse arthroplasties were tried. However, the results were unpredictable until the unique design of the Delta reverse shoulder by Professor Grammont. This arthroplasty, with a large hemisphere on the glenoid side resulting in a medialized centre of rotation, has shown very good results in short- and mid-term follow-up studies. It is now routinely used for a variety of different shoulder pathologies where the function of the rotator cuff is lost. Active elevation and abduction is restored together with excellent pain relief. Active external rotation, however, is not restored and therefore the procedure has been combined with muscle transfer in selected patients. This is a review of the history, indications, results and complications of the reverse arthroplasty.
Introduction
Anatomical shoulder replacement, hemi or total, can give excellent pain relief and restore shoulder motion. However, when the rotator cuff is deficient the outcome of shoulder replacement is more unpredictable [1]–[13]. In order to compensate for the lost function of the rotator cuff constrained or reverse designs have been tried. Today reverse total shoulder arthroplasty is routinely used to restore function and relieve pain in rotator cuff deficient shoulders of various aetiologies.
History and Biomechanics of the Reverse Arthroplasty
When the function of the rotator cuff is lost the humeral head migrates superiorly. This reduces the tension in the deltoid muscle and the centre of rotation becomes unstable. Some patients completely lose their ability to raise their arm, while others maintain the capacity to flex above shoulder level. When these patients were treated with conventional arthroplasties the results were unpredictable [1], [2], [4]–[6], [10]–[15]. Therefore new designs were developed to overcome this biomechanical deficiency.
To counteract superior migration of the humeral head hooded glenoids were tried and abandoned due to high failure risk [16]–[18]. Several constrained arthroplasties were tried but a high failure rate was seen [19]–[25]. By reversing the joint i.e. placing the spherical part on the glenoid side and the cup on the humeral side it was possible to stabilize the centre of rotation and to control its position. However, fixation of the component on the glenoid side was difficult with high failure rates [23], [24]. These early designs were experimental and very few reports have been published [19], [20], [22], [23], [25]. Most of these designs were abandoned.
Professor Paul Grammont in Dijon, France, however, continued to work on a design to restore function in shoulders with rotator cuff deficiency. He advocated a large head on the glenoid side with a medialized centre of rotation to restore length and to improve the lever arm for the deltoid muscle [26]. His first reverse design was the trumpet prosthesis in 1985, which was modified into the Delta reverse arthroplasty, which became available in 1991 [27], [28]. The Delta reverse arthroplasty has a large hemispheric ball on the glenoid side (uncemented screw fixation) and a polyethylene cup on the humeral side. The centre of rotation is at the bone-implant interface reducing the shear forces and lowering the risk for glenoid loosening compared with earlier designs with a lateralized centre of rotation [19], [25]. The glenoid component has a hydroxyapatite covered central peg and four screws in different angles. Furthermore, he introduced a non-anatomical inclination angle of 155° on the humeral side. There were originally two sizes of the head, 36 mm and 42 mm, which have been changed to 38 mm and 42 mm in the latest design. A larger diameter of the head results in better stability and greater range of motion before the component impinges on the scapula bone. The original Delta reverse arthroplasty had one height of polyethylene insert, but different depths on the polyethylene cup to help the surgeon to create a stable articulation. To facilitate soft tissue balance polyethylene inserts with different heights were later introduced (3 mm, 6 mm and 9 mm).
There have been several modifications of the original Delta design to improve outcome and to make the procedure easier and the latest is the Delta Xtend (DePuy Ltd) introduced in 2007 (Fig. 1). However, the innovative and proven ideas of Grammont have been respected.

The modular cementless Delta Xtend reverse arthroplasty (DePuy Ltd) available since 2007.
The unique design of the Delta reverse arthroplasty creates a stable centre of rotation at the bone-implant interface and the centre of rotation can be positioned low on the glenoid surface. This restores the length of the deltoid muscle (or slightly overstretches it) and provides a longer lever arm for the deltoid muscle. The medialization of the centre of rotation also results in more muscle fibres for active abduction. The rotational motion of a reverse arthroplasty is not rotation as in a normal joint, but rather the polyethylene cup gliding over the spherical surface until the edge of the cup reaches the scapula bone. Due to the medialization of the centre of rotation the remaining rotator cuff muscles have reduced tension after a reverse arthroplasty. This may result in weakened rotation, particularly external rotation.
The Delta reverse arthroplasty has shown very promising early results, with increased clinical use [28]–[32]. There are now more than 10 designs on the market which more or less are based on Grammont's design. However, there are some differences. Some have a lateralized centre of rotation of various degrees. The rationale is to reduce the risk for the humeral component to impinge on the inferior part of the scapula (notching) and also to give a better tension in the remaining rotator cuff muscle. However, it also results in a higher load on the fixation of the glenoid component which proved detrimental in the early designs of reverse arthroplasty. Long term follow-up studies are necessary to see whether there is an increased risk for glenoid loosening in these designs.
Indications
The Delta reverse arthroplasty was designed to treat patients with cuff tear arthropathy. However, the clinical consequences of cuff tear arthropathy vary. Some patients have good function (biomechanical balance) and can raise the arm above shoulder level. Others have lost the ability to actively raise their arm (pseudoparalysis). In patients with a biomechanical balance a hemi-arthroplasty can still be considered, particularly if the patient is younger. If the patient has pain and pseudoparalysis a reverse arthroplasty is indicated. It is important to test the ability to raise the arm with a weight in the hand(1 kg to 2 kg) to see the functional biomechanical balance. If the arm is very painful it can be very helpful to inject a local anaesthetic in the subacromial space to eliminate pain as a cause for the poor range of motion. In order to consider a reverse arthroplasty the patient needs to have a functioning deltoid muscle and enough bone stock on the glenoid side to fix a glenoid component with or without a bone graft.
There are many disease processes that result in a loss of function in the rotator cuff and biomechanical deficiency. Over the last 20 years the indications have widened and today the reverse arthroplasty is used in patients who have pain and irreparable cuff deficiency due to cuff tear arthopathy, massive irreparable cuff tear with or without osteoarthritis, rheumatoid arthritits and other inflammatory joint diseases, failed anatomical arthroplasties, tumours, acute complex fractures in the elderly and post-traumatic conditions (malunited fractures, non-unions, chronic locked dislocations in the elderly) [30]–[45]. It is an evolving process to define the proper indications for the reverse arthroplasty and more studies are needed. It has predominately been used in elderly patients (over 70 years) and there is a lack of long term follow-up data. Therefore it is recommended to be used only in older patients. However, there are younger patients with severe pain and pseudoparalysis where no other procedure can help, and in such cases a reverse arthroplasty may be indicated.
When do I consider doing a reverse arthroplasty in a younger patient? I consider doing the procedure if the shoulder is very painful and so bad that even after failure and removal of the implant after several years, the patient will not be worse off than the pre-operative status. However, based on the current literature the use of a reverse arthroplasty in younger patients should be very restricted.
Surgical Technique
The surgical technique is important since many complications can be avoided by proper implantation of the reverse arthroplasty. Plain radiographs and a CT scan are recommended pre-operatively. The surgical technique varies between different prosthetic systems, but some important general principles can be defined.
The patient should be in the beach chair position. There are two possible approaches. One is the classic delto-pectoral approach and the other a superior deltoid split. Grammont advocated a superior deltoid split with an osteotomy of the acromion, but today this is not used [28]. There are pro and cons for both approaches. I prefer the superior deltoid split in standard primary cases and in acute fractures, and the deltopectoral approach in revisions and more complex primary cases.
There is no absolute agreement on the version of the humeral cut in reverse arthroplasty. A retroverted cut favours external rotation, while a cut in more neutral or slight anteversion favours internal rotation. Since it has proven difficult to restore internal rotation in patients undergoing reverse arthroplasty, I place the cut in neutral to optimize the capacity for internal rotation.
It is important to expose the glenoid and define the bony anatomy. The inferior part of the glenoid is a circle and the goal is to place the glenoid component in that circle. The glenoid component should be placed as low as possible to minimize the risk for inferior impingement (notching) [31], [46]–[48]. The goal is to have the metaglene plate in line with the inferior border of the scapula. When the glenosphere is attached an overhang is created, which reduces the risk for notching. The low placement of the glenoid component improves the biomechanics. If there is a bone deficiency, grafting is necessary to have good support for the metaglene plate. I prefer to use the resected head or autologous iliac crest bone.
The metaglene plate is in most cases fixed to the scapula with a central peg and screws. The inferior screw is placed first and then the top screw followed by the anterior and posterior. The number of screws varies between different designs. Polyaxial locking screws are a big advantage since they give the surgeon a better chance of low positioning of the metaglene plate and still have a long inferior screw inside the scapula. Locking screws give better fixation compared with non-locking and are recommended.
The humeral component can be uncemented or cemented. If there is proximal bone loss of the humerus a monobloc is recommended. Unscrewing of a two component humeral component has been seen in the author's institution. When the humerus is prepared care should be taken to protect the remnants of the rotator cuff.
Trial components are placed to check range of motion and stability. A large glenosphere gives better stability and less risk for notching and is recommended if possible. The deeper polyethylene cups result in a more constrained joint and a risk of more polyethylene wear and should be avoided.
If a deltoid split is used it is important to re-attach the deltoid with non-absorbable sutures and tailor the post-operative rehabilitation accordingly.
Results
In 1993 Grammont published the results in 14 patients with cuff tear arthropathy. Function improved significantly, but there was a high percentage of complications, such as acromial fractures, humeral fractures, superficial infection and deep infection [28]. In 1995 Baulot et al. reported the early results of 16 cases [29]. Their conclusion was that the Delta reverse shoulder was effective in restoring function in the cuff deficient shoulder. During the following years the early results of several series of Delta reverse arthroplasty were presented at different meetings (Fig. 2A, B). In 2004 Sirveaux et al. published a multicentre study of 80 shoulders (77 patients) with massive rotator cuff tears and osteoarthritis which were treated with a Delta reverse arthroplasty with a mean follow-up 44 months [31]. The Constant score increased from 23 points pre-operatively to 66 points post-operatively. In 96% of the shoulders there was no or only minimal pain. The active elevation increased from 73° to 138°. There were five cases of glenoid loosening (6%). A scapular notch was seen in 64% of the cases. An extensive notch was associated with a lower Constant score. They also reported that an intact teres minor resulted in a better outcome and higher Constant score (p = 0.01). A low position of the metaglene baseplate was recommended. If revision of the implant was considered the end point, the chances of not having a revision within 97 months was 95% (92 to 97). Werner et al. reported on 58 patients who had pseudoparalysis due to rotator cuff deficiency [32]. Of these 58 patients 21 were revisions of other prostheses. The relative Constant score increased from 29 to 64 and mean active forward elevation from 42° to 100°. A complication occurred in 50% of the patients and 19 patients (33%) underwent a revision procedure. The most common complications were a haematoma (12 patients) and dislocation (5 patients). Notching was seen in 96% of the radiographs, but could not be correlated to outcome. In 2005 Frankle et al. reported early results from another reverse arthroplasty design in 60 patients [36]. The mean American Shoulder and Elbow score increased from 34 to 68. Mean active forward flexion increased from 41° to 102°. Forty-one of the 60 patients rated the results as good or excellent. There were 17% complications.
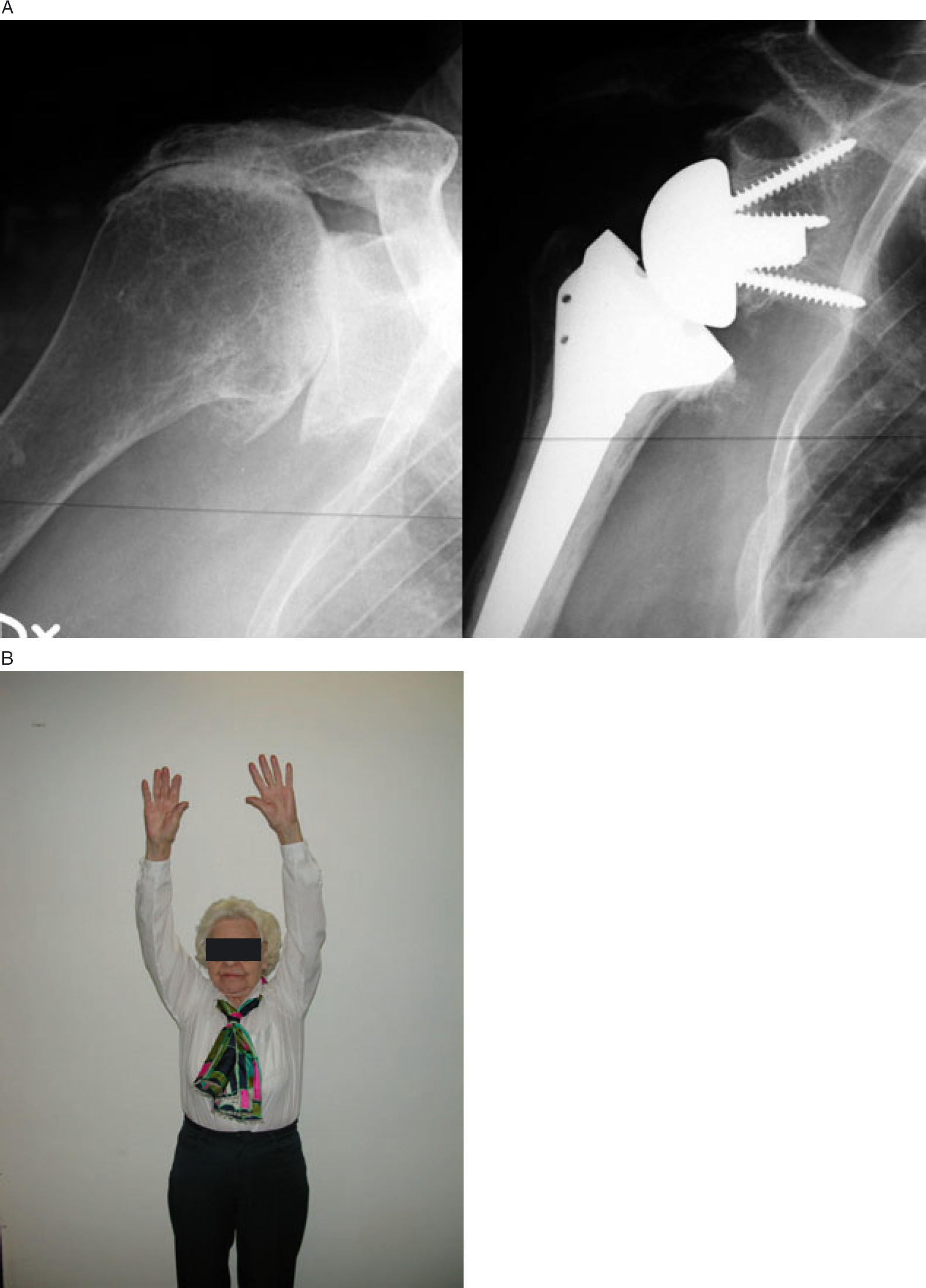
(A) Eighty-five year old patient with cuff tear arthropathy. Pre- and post-operative X-rays. (B) Functional outcome in the same patient.
Guery et al. reported on survivorship analysis of 80 Delta reverse arthroplasty followed for 5 years to 10 years [38]. At the time of review 60 shoulders were available for follow-up. If failure was defined as revision of the implant there was a 91% survival at 120 months. However, if the endpoint was loosening of the implant the survivorship dropped to 84% at 120 months. Furthermore, if the endpoint was a Constant score of <30% the survivorship was 58% at 120 months. The authors noted two breaks in the survival curve. The first was at 3 years representing early loosening and the second at around 6 years indicating progressive deterioration of the functional results. The conclusion from this study was that the reverse arthroplasty should only be used in patients over 70 years old with low functional demand.
Boileau et al. reported on midterm results of 45 patients after implanting a Delta reverse arthroplasty with a mean follow-up of 40 months [30]. The indications were cuff tear arthropathy (21), fracture sequel (5) and revision arthroplasty (19). There was significant improvement regarding active forward elevation and Constant score (17 to 58). There was, however, no change in external or internal rotation. The results were best in cuff tear arthropathy and significantly worse in revisions. In revisions a complication rate of 47% was seen compared with 5% in the cuff tear arthopathy group. Scapula notching was seen in 68% of the patients. Patients with atrophy or severe fatty infiltration of the teres minor had worse external rotation and a lower Constant score (p < 0.007).
Wall et al. reported on similar results in 240 consecutive cases of reverse arthroplasties in 232 patients [44]. Of these 196 arthroplasties were followed for an average of 40 months. The indications were cuff tear arthropathy (59), revision arthroplasty (45), massive cuff tear (34), primary osteoarthritis (25), post-traumatic osteoarthritis (28) and others (5). The overall mean Constant score increased from 23 to 60. The best outcome was seen in cuff tear arthropathy, massive cuff tears and primary osteoarthritis. Inferior results were seen in patients with post-traumatic osteoarthritis and revision arthroplasties. Scapular notching was seen in 51% of the cases with adequate radiographs (77/152 patients). The notching did not affect outcome. Overall complication rate was 19%.
Several authors have reported that the clinical results depend on the integrity of the teres minor. In many cases of cuff tear arthropathy the only external rotator left is the teres minor [30], [31], [49]. If this tendon is torn or the muscle atrophic, the patient has a lower Constant score and less external rotation. A latissimus dorsi transfer has been advocated to improve the results in these patients [50], [51]. Gerber et al. reported on 12 patients who had a combination of latissimus dorsi transfer and a reverse arthroplasty performed [51]. The latissimus dorsi tendon was released through a separate incision. The active flexion improved but the absolute external rotation with the arm at the side did not change significantly (from 12° to 19°). However, the score for functional external rotation according to Constant increased from 4.6 to 8.2 (out of 10). The score for activity of daily living increased from 2.3 to 7.9 (out of 10). In 2008 Boileau et al. reported on 11 patients who had a latissimus dorsi and teres major transfer in combination with a reverse arthroplasty performed through a single deltopectoral approach [50]. The combination restored active elevation and external rotation in all patients.
The development of a scapular notch has been reported by many authors [30]–[32], [38], [42]–[44], [48]–[52] (Fig. 3). It starts as a mechanical contact between the humeral component and the scapular neck. However, due to polyethylene wear particles it can also cause an osteolytic response. In the large French multicentre study the frequency of a scapular notch increased with longer follow-up. It was 41% at 1 year and 87% at 6 years to 10 years follow-up [43]. No correlation was found between the scapular notch and pain, mobility, and activity score. Wall et al. in a study of 186 patients with a 2 year follow-up radiograph found a notch in 51% of the patients but no significant difference in results in patients with or without a scapular notch [44]. The patients with a notch had a Constant score of 59 and patients without a Constant score of 61. However, Simovitch et al. reported that an inferior scapular notch was associated with significantly poorer clinical outcome [48].
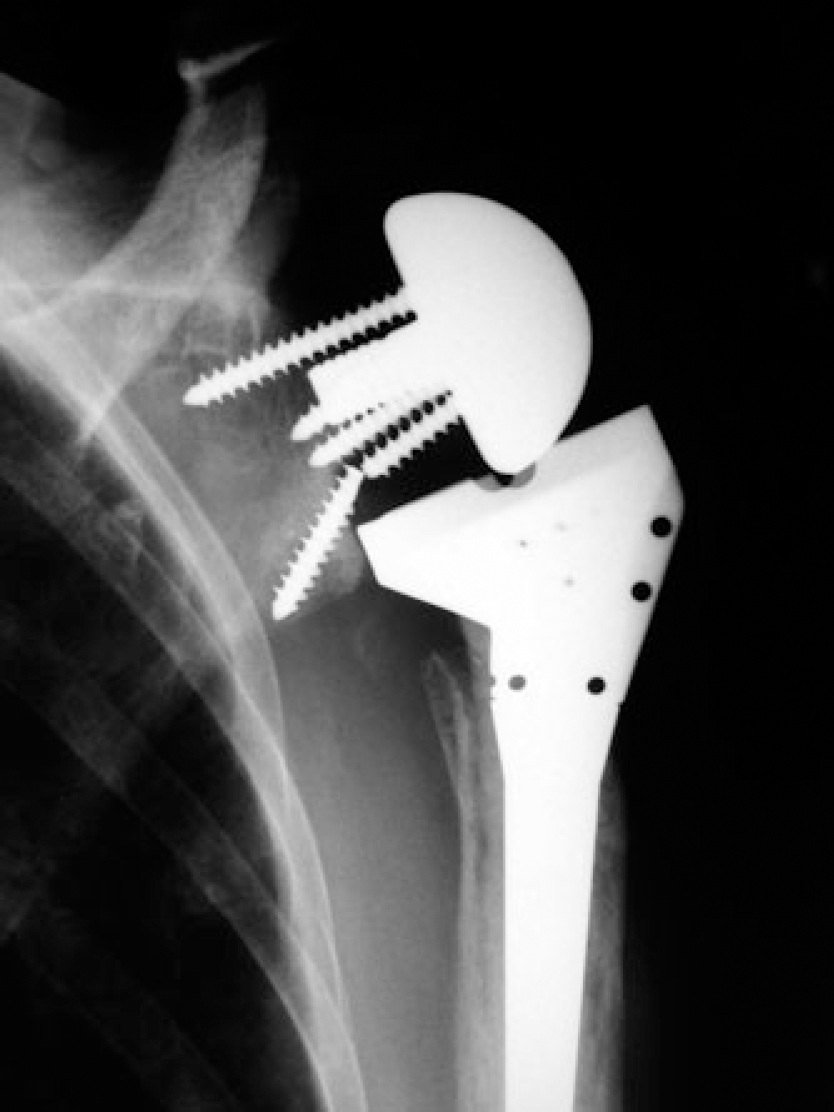
Scapular notch with a broken screw.
Reverse arthroplasty for acute four part fracture in the elderly is still controversial. The author started to use the reverse for this indication 1997 (Fig. 4A, B). In 2006 Cazeneuve & Cristofari reported on 23 cases of acute complex fracture of the proximal humerus treated with a Delta reverse arthroplasty [34]. At a mean follow-up of 86 months the Constant score was 60 points. Bufquin et al. reported on 43 patients with a mean Constant score of 44 [33]. They concluded that satisfactory mobility was obtained despite frequent migration of the tuberosities. More recently Klein et al. reported on 20 patients with a mean Constant score of 68 [39]. Mean flexion was 123° and abduction 113°. Gallinet et al. compared reverse arthroplasty with hemi-arthroplasty in acute complex fractures of the proximal humerus [37]. The reverse arthroplasty group showed better abduction, anterior elevation and Constant score, but the rotation was worse. Further studies are needed in order to define the proper indication and surgical technique for using reverse arthroplasty in acute complex fractures of the proximal humerus.

(A) Pre- and post-operative radiographs of a 82 year old female with a fourpart proximal humeral fracture treated with a Delta Xtend reverse arthroplasty. (B) Functional outcome after 1 year.
Complications
In a large French multicentre study of 457 reverse arthroplasties 25.6% of the patients had a least one intra- or post-operative complication [43]. However there was a significant difference between primary and revision arthroplasty. Fifteen percent experienced a complication after primary arthroplasty compared with 65% after revision arthroplasty. Thirty-nine intra-operative complications were recorded. The most common intra-operative complications were humeral (28) or glenoid (11) fracture. Instability was the most common post-operative complication in the entire patient group and was seen in 4.8% (22 cases) followed by infection in 3%. In the group of 94 revision arthroplasties instability occurred in 11% and infection in 6%.
Other complications were periprosthetic fractures 2.6%, glenoid loosening or disassembling 2.1%, humeral loosening 0.9%, haematoma 0.7%, and scapular spine fracture 0.7%.
These results are in accordance with Wall et al. who reported an incidence of dislocations of 7.5% and infection of 4% [44].
Recently Wierks et al. reported on 20 patients with a complication rate of 75% [53]. This was higher than results from 12 published series of in a total of 417 patients. The mean complication rate in these series was 25% (95% confidence interval 13.5% to 35.9%). The great variation in reported rates of complications may be due to lack of an accepted definition of a complication.
Between 1995 and 2002 118 reverse arthroplasties were performed by the author. Forty-five were revisions. Dislocation was seen in 8% and infection in 8%. Twelve (10%) patients experienced two or more complications. However, the rate of complications has dropped significantly over the last years. In the last 200 cases of reverse arthroplasty in our institution we have not seen any infection and only two dislocations (both in revision). There are several reasons for this improvement in results such as better implants, more modularity (different height of inserts), surgery now being performed in less complex cases, and improved knowledge about the surgical technique.
Instability of a reverse arthroplasty can occur without pain (Fig. 5). Several of our cases were detected on routine radiographic follow-up. The patient usually experiences a drop in active flexion and abduction. If the dislocation occurs early (within the first days) we perform a closed reduction and immobilization for 3 weeks. However, most dislocations occur later (within 3 months) and our approach in all these cases is revision and removal of scar tissue and lengthening of the system. All our cases have been stable after revision. Dislocation is more common after the deltopectoral approach compared with a superior deltoid split [43]. A larger glenosphere is more stable and therefore preferred.

Post-operative dislocation of a reverse arthroplasty.
Infections are treated like other infected arthroplasties. Early infection can sometimes be saved by early debridement. Deep infection occurring later is normally treated with a two stage revision with an antibiotic impregnated spacer in-between. It is particularly important in revision arthroplasty to rule out low grade infection before revision to a reverse. Severe pain at rest should raise the suspicion of an existing infection.
Summary
Traditional shoulder replacement is a very successful procedure and is routinely performed. However, the results have been unpredictable in cuff deficient shoulders. Therefore reverse designs were tried since they improve the biomechanics in the cuff deficient shoulder. At the time when many early designs of reverse shoulder arthroplasty were abandoned, Grammont in France continued to work on his reverse arthroplasty design, which lead to the Delta reverse arthroplasty. The first procedure in the author's institution was performed 1995 and since then it has been possible to treat patients who were considered non-treatable. The design has proven to be reliable with very low risk for loosening in mid-term follow-up studies [30], [31], [38], [42]–[44]. It is now routinely used all over the world for patients with cuff deficiency of various aetiologies. However, the rate of reported complications has been high, but there are indications that the incidence has dropped significantly during the last few years. Correct indications and surgical technique is crucial to obtain the best results. An additional latissimus dorsi transfer is now recommended in patients who have complete lack of external rotation pre-operatively (no infraspinatus or teres minor) and/or severe atrophy and fatty infiltration of the teres minor. The radiographic finding of a glenoid notch is a concern and one of the reasons why this implant is recommended only in the elderly. New designs and specific surgical guidelines have been advocated to reduce the incidence of notching. Long term follow-up studies are needed to ascertain the clinical consequences of the glenoid notch and to evaluate the survival of the implant.