
Abstract
Coracoid impingement syndrome is a rare cause of anterior shoulder pain. It is mainly a diagnosis of exclusion after considering the more common subacromial impingement. We describe a case of coracoid impingement and a novel approach to its management: coracoid osteotomy as opposed to the more commonly used technique of coracoplasty. A review of the literature is also presented in relation to this condition. Coracoid osteotomy with internal fixation allows good stability with reliable direct bone-to-bone healing. Coracoid osteotomy is a reliable and a satisfactory alternative to the more commonly-used technique of coracoplasty for the treatment of idiopathic coracoid impingement syndrome.
Introduction
Coracoid impingement syndrome is a rare cause of anterior shoulder pain. It is mainly a diagnosis of exclusion after considering the more common subacromial impingement. We describe a case of coracoid impingement and a novel approach to its management: coracoid osteotomy as opposed to the more commonly used technique of coracoplasty. A review of the literature is also presented in relation to this condition.
Case Report
A 48-year-old right hand dominant professional worker presented with a5-year history of pain and clicking sensations over the anterior aspect of the right shoulder. There was no significant history of trauma or surgery to the shoulder in the past. The pain was most obvious during sporting activities that required forward flexion and internal rotation of the shoulder. He also experienced rest pain when lying on his right side. Activity restriction and nonsteroidal anti-inflammatory medication gave some partial relief.
On examination, the coracoid process was prominent and focally tender. Active movements in the shoulder were: 170° forward flexion (with pain 100° –170°), 170° abduction (with pain from 90° –170°), 80° external rotation, and internal rotation up to the upper lumbar spine. There was evidence of biceps tendon subluxation with an obvious clicking sensation during shoulder movement. The coracoid impingement test with forward flexion of 90° with adduction and internal rotation of the shoulder elicited severe pain in the region of the coracoid process. Power in the rotator cuff muscles was normal.
Anteroposterior view plain radiographs of the shoulder revealed a prominent and curved coracoid process (Fig. 1). Magnetic resonance imaging (MRI) scans of the shoulder revealed a prominent coracoid process with narrowing of the coracohumeral distance, as well as a partial thickness tear of the inferior fibres of the underlying subscapularis tendon suggestive of subcoracoid impingement (Fig. 2). The long head of the biceps demonstrated intrasubstance signal irregularity and thickening suggestive of tendinosis. There was marked thickening of the superior glenohumeral ligament with tissue suggestive of synovitis in the rotator interval local anaesthetic injection into the coracoid area (~5 mls of 1% Lignocaine) temporarily relieved the symptoms. Because further conservative treatment with physiotherapy proved unsuccessful, it was decided to undertake surgery.

Preoperative X-ray of the right shoulder showing a prominent coracoid process.
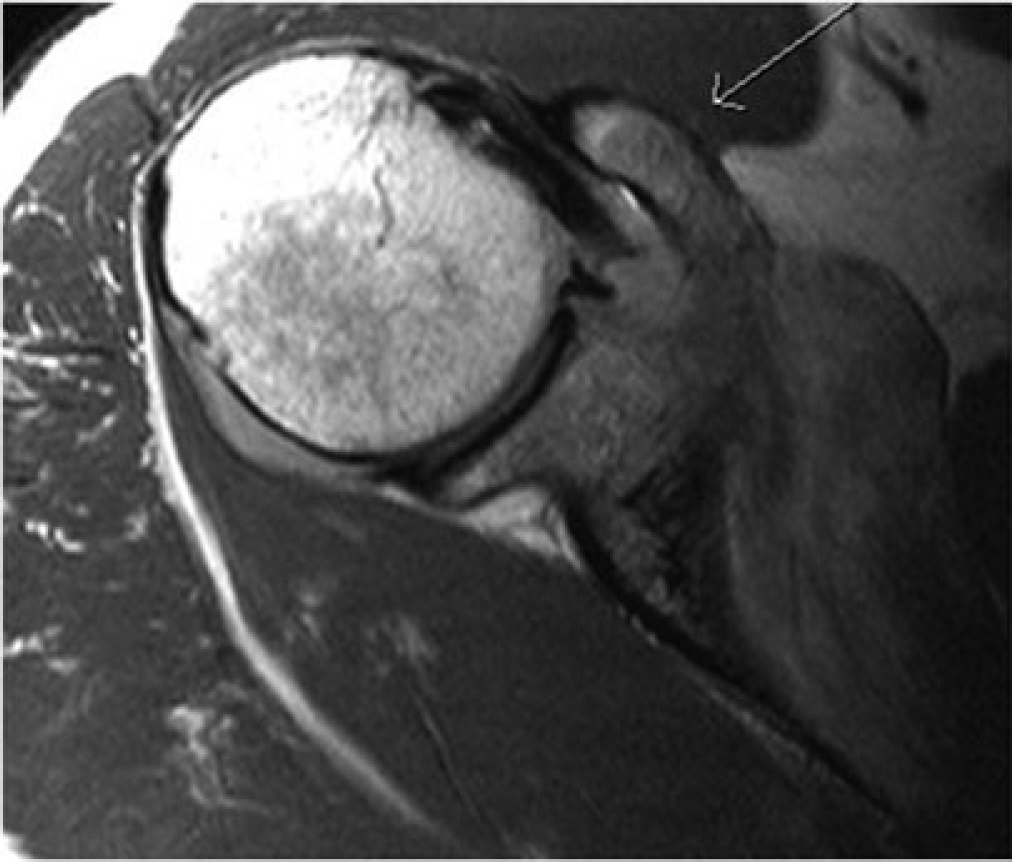
Intermediate weighted magnetic resonance scan in the axial plane of the shoulder demonstrates impingement by a prominent coracoid process over the subscapularis tendon at the musculotendinous junction.
Through a deltopectoral approach, the coracoid process with the attached conjoined tendon was explored. Coracoid osteotomy was performed 1 cm proximal to the tip of the coracoid. A medially-based bone wedge was excised from the body of the coracoid to shorten and re-orientate the coracoid process, thereby increasing the coracohumeral distance and relieving the impingement of the coracoid tip on the subscapularis (Fig. 3A). The osteotomy was fixed with a 4-cm partially threaded cancellous screw (Fig. 3B). Physiotherapy in the form of pendulum exercises was initiated the day after the operation. A full range of active motion exercises was initiated after 4 weeks. The patient regained normal muscle strength and a full range of motion 3 months after the operation. After 1 year of follow-up, the patient remained symptom free and had returned to sporting activities. He has subsequently been discharged from our care.
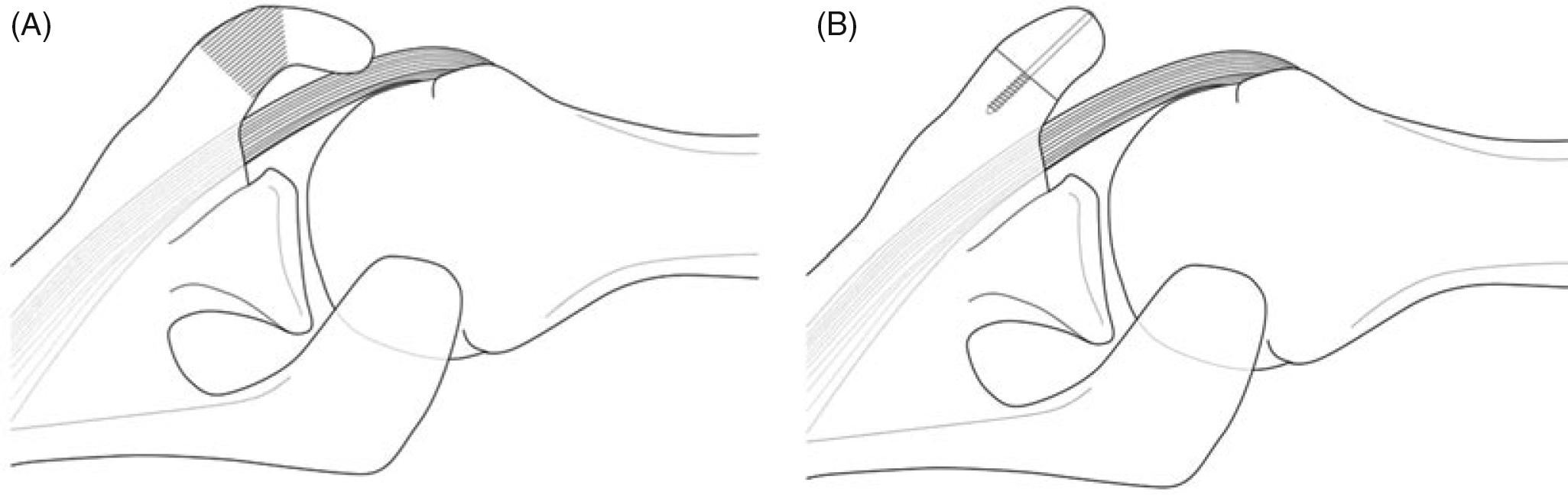
Coracoid shortening osteotomy showing medially-based wedge osteotomy, 1 cm proximal to tip of coracoid (A) and the use of a semi-threaded cancellous screw for fixation (B).
Discussion
Mechanical impingement on the rotator cuff by the overlying acromial arch including the coracoid process was postulated as early as 1909 [1] and, subsequently, in 1937 [2] and in 1941 [3]. Dines et al. coined the term ‘coracoid impingement syndrome’ in 1990 [4].
Coracoid impingement syndrome is an infrequent cause of anterior shoulder pain. Symptoms are presumed to occur when the subscapularis tendon impinges between the coracoid and lesser tuberosity of the humerus [5]. Repetitive overuse with multiple episodes of microtrauma, especially when the shoulder is persistently in forward flexion, adduction and internally rotation results in anterior shoulder pain [6].
The causes are classified as idiopathic, traumatic or iatrogenic [6]–[8]. Secondary causes include previous fractures of the lesser tuberosity, calcification within the subscapularis tendon, and abnormal glenoid orientation secondary to glenoid osteotomy [4]. Gerber et al. reported coracoid impingement in 1985 in a series with a high percentage of iatrogenic cases secondary to Trillat procedure [7]. The diagnosis of itself has not been extensively studied, and it remains a diagnosis of exclusion based on the findings of the physical examination, the results of local anaesthetic injections, and radiographic features [7].
The coracoid impingement test is performed with the patient's shoulder placed in a position of cross-arm adduction, forward elevation, and internal rotation to bring the lesser tuberosity in contact with the coracoid [4]. Another method of evaluation is to inject lignocaine into the subcoracoid region, as was performed in this instance [4]. Although it has been suggested that relief of pain with this injection can help to establish the diagnosis, this test has not been studied to determine either its validity or its accuracy [9]. The proximity of multiple structures in the subcoracoid region, including the joint itself, makes the accuracy of these injections questionable.
Plain radiographs of the shoulder, in particular an anteroposterior view and an axillary view perpendicular to the plane of the scapula can detect anatomical aberrations that may contribute to the impingement. Coracoid index measurement of the lateral projection of the coracoid process beyond a line tangential to the articular surface of the glenoid on axial computed tomography is helpful [4]. The average index in 67 normal shoulders was 8.2 mm [4]. Gerber et al. observed that the average coracohumeral space in normal shoulders is 6.7 mm with the arm flexed and medially rotated, but only 5.5 mm in patients with coracoid impingement syndrome [10]. The sensitivity of this particular position in detecting coracoid impingement on MRI is only 5.3% with a specificity of 97.6%. [11]. This suggests that subcoracoid impingement appears to be largely a clinical diagnosis that may be supported or suggested, but not established, by MRI [11].
A final way of making a diagnosis of coracoid impingement is direct arthroscopic observation of the contact [12]. This case report on patients with a partial rupture of the subscapularis tendon noted contact between the subscapularis tendon and the lesser tuberosity with the arm in a position simulating that used to elicit the coracoid impingement sign. The fact that the subscapularis tendon was torn in this instance made the observation of the contact more likely similar to the MRI scan findings reported in the present case.
Controversies exist regarding the therapeutic options for the resolution of symptoms and a return to optimal shoulder function. The first line of treatment for coracoid impingement should be a programme of activity modification, with avoidance of the provocative positions of forward flexion and medial rotation, as well as physical therapy to strengthen the rotator cuff muscles and stabilize the scapula [6], [7].
Surgical decompression of the subcoracoid space is undertaken if non-operative measures fail. Various surgical procedures, including open coracoplasty, a combination of coracoacromial ligament resection and acromioplasty, anterior shoulder stabilization and arthroscopic treatment, have been described in the literature [4], [7], [13]. There is no consensus regarding the best operative procedure for coracoid impingement.
We have described a new technique of coracoid osteotomy (Fig. 3A, B). Figure 4 shows the postoperative X-ray radiographs. Unlike the coracoplasty technique where a successful outcome depends on healing of soft tissues (conjoined tendon) to bone, coracoid osteotomy with internal fixation allows good stability with reliable direct bone-to-bone healing. Osteotomy also allows the surgeon to resect as much bone as possible and re-orientate the coracoid process to relieve impingement on the subscapularis by the tip of the coracoid process.
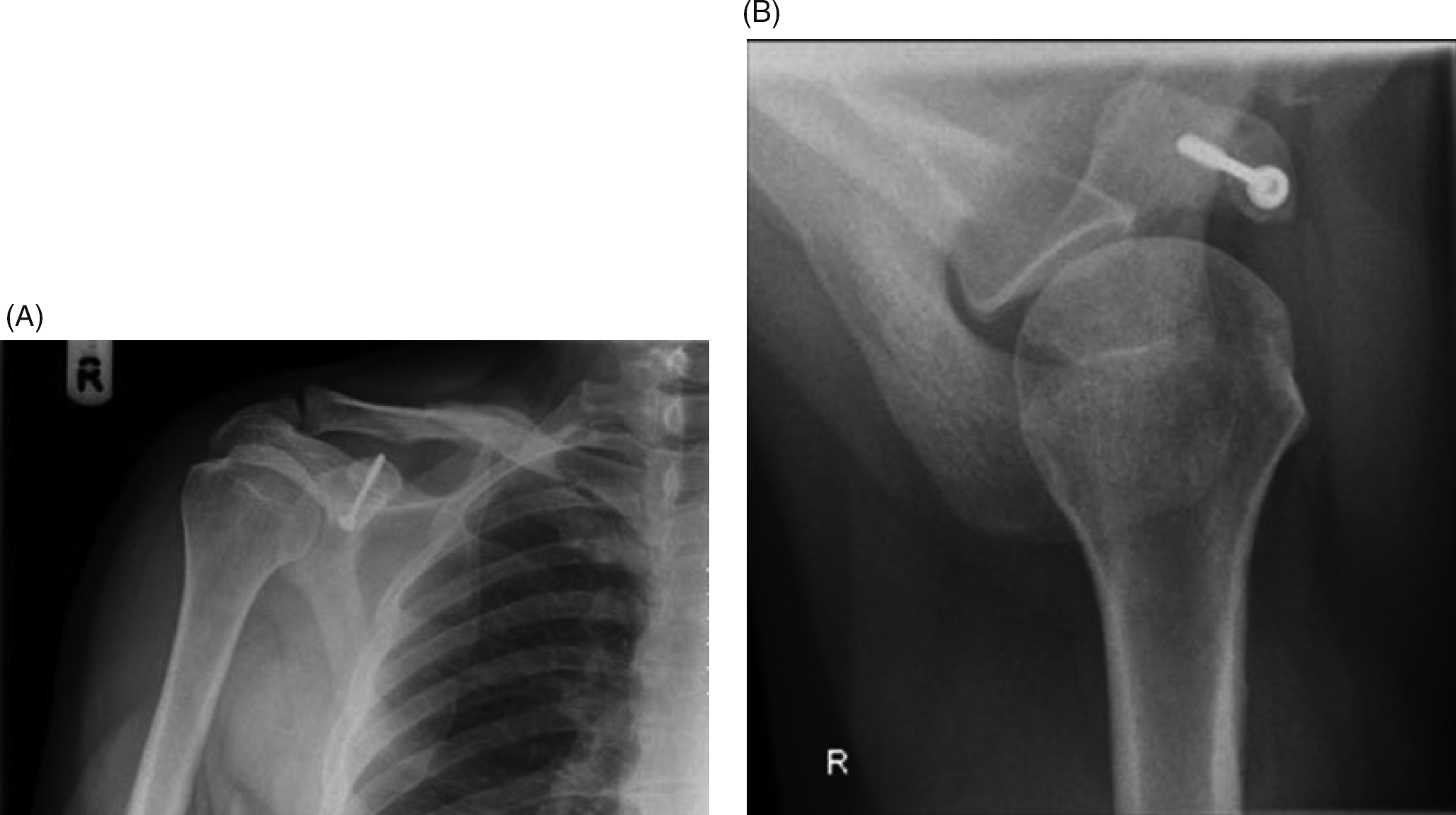
Postoperative antero-posterior (A) and axillary (B) radiographs showing the corrective coracoid shortening osteotomy.
Conclusions
It is important to include a diagnosis of coracoid impingement in the differential diagnosis of activity-related anterior shoulder pain. Coracoid osteotomy is a reliable and satisfactory alternative to the more commonly used technique of coracoplasty for the treatment of this commonly idiopathic syndrome.
Footnotes
Acknowledgements
We thank Jackie Withycombe of the Medical Illustration Department at University Hospitals Leicester for providing the line diagrams depicting the coracoid osteotomy.