
Abstract
Background
We wish to demonstrate that osteoarthritis of the sternoclavicular joint can be a cause of tertiary subacromial impingement as a result of decreased motion of the clavicle.
Materials
We present a series of five patients with tertiary subacromial impingement caused by stiffness of the sternoclavicular joint. All five patients attended our upper limb clinic with what appeared to be subacromial impingement. Close examination revealed that they had an inability to shrug the affected shoulder as a result of reduced mobility of the sternoclavicular joint caused by osteoarthritis. None of the patients had symptoms localized to the sternoclavicular joint itself. After appropriate investigation, four patients underwent excision of the medial end of the clavicle and one responded well to physiotherapy.
Results
All patients regained full shoulder movements and resolution of the subacromial impingement pain.
Discussion
We recommend that the ‘shrug test’ should be part of routine shoulder examination so that sternoclavicular joint pathology can be recognized at an early stage and acted on appropriately. We conclude that subacromial impingement can be caused by impaired clavicle rotation as a result of osteoarthritic changes in the sternoclavicular joint.
Introduction
We wish to demonstrate that osteoarthritis of the sternoclavicular joint can be a cause of tertiary subacromial impingement as a result of decreased motion of the clavicle.
Different types of shoulder impingement have been described in the literature. In 1972, Neer described the impingement on the rotator cuff by the coraco-acromial ligament and the anterior third of the acromion (as a result of the intrinsic pathology of the cuff and bursa, and extrinsic factors: spur formation of the acromion) [1]. Walch presented an impingement occurring between the deep side of the supraspinatus tendon and the postero-superior edge of the glenoid cavity which he named ‘postero-superior glenoid impingement’ (internal impingement) [2]. Dines et al. described the subcoracoid impingement: impingement of the coracoid process against the greater tuberosity of the humerus during adduction, internal rotation and flexion [3].
We present a series of five patients with tertiary subacromial impingement, caused by stiffness of the sternoclavicular joint. All these cases presented initially with absence of any localized symptoms of the sternoclavicular joint. They had all undergone various treatments for subacromial impingement prior to the correct diagnosis being established.
Case Reports
Case 1
History.
A 29-year-old man was referred by his general practitioner with recurrence of left shoulder impingement pain. Five years previously, he had sustained an injury to the left shoulder, which was eventually treated by arthroscopic tenodesis of long head of biceps.
Examination.
The patient had well developed musculature of the shoulder girdle, with positive subacromial impingement signs and restriction of shoulder flexion to 130° (Fig. 1) and abduction to 150°. There was no bony tenderness over the shoulder girdle, including the sternoclavicular joint. Further detailed examination (by J.F.) noted stiffness of the sternoclavicular joint, as demonstrated by his inability to shrug the shoulder on the affected side (Fig. 2).

Preoperative shoulder flexion.

Preoperative shrug test.
Investigations.
Plain X-rays of the sternoclavicular joints appeared normal. A computed tomography (CT) scan of the sternoclavicular joints revealed erosive changes of the medial end of the left clavicle (Fig. 3).
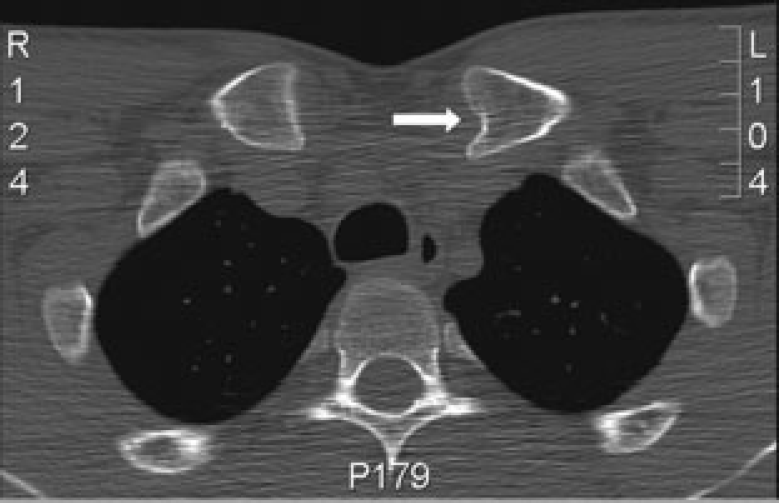
Computed tomography of sternoclavicular joint (patient 1).
Treatment.
The patient underwent left shoulder arthroscopy (which did not show any pathology) and excision of medial end of the clavicle. He was followed up for 12 months. He had full resolution of impingement symptoms and restoration of a full range of movements of the shoulder.
Case 2
History.
A 45-year-old lady presented with ongoing pain in her right shoulder over many years. She was complaining of two different types of pain: one localized around the anterior aspect of the shoulder radiating down the arm and in the trapezius muscle and the other one around mid-shaft of the clavicle.
Examination.
She had a nontender prominent right sternoclavicular joint. There was no tenderness over the insertion of the rotator cuff and the acromioclavicular joint. The range of movements was limited: flexion to 140° and abduction to 160° with a painful arc between 70° and 160°. Hawkins test was mildly positive. She was also unable to shrug the affected shoulder.
Investigations.
Plain X-rays of the shoulder showed minimal arthritic changes in the acromioclavicular joint without any other abnormalities. An ultrasound scan did not show any pathology of the rotator cuff or biceps tendon and there were no signs of bursitis. A CT scan of the prominent sternoclavicular joint was then performed and revealed an abnormal medial end of the clavicle with a bony protrusion, which had formed a pseudoarthrosis with the first rib (Figs 4 and 5).
Computed tomography of sternoclavicular joint (patient 2): osteoarthritis and pseudarthrosis with first rib.
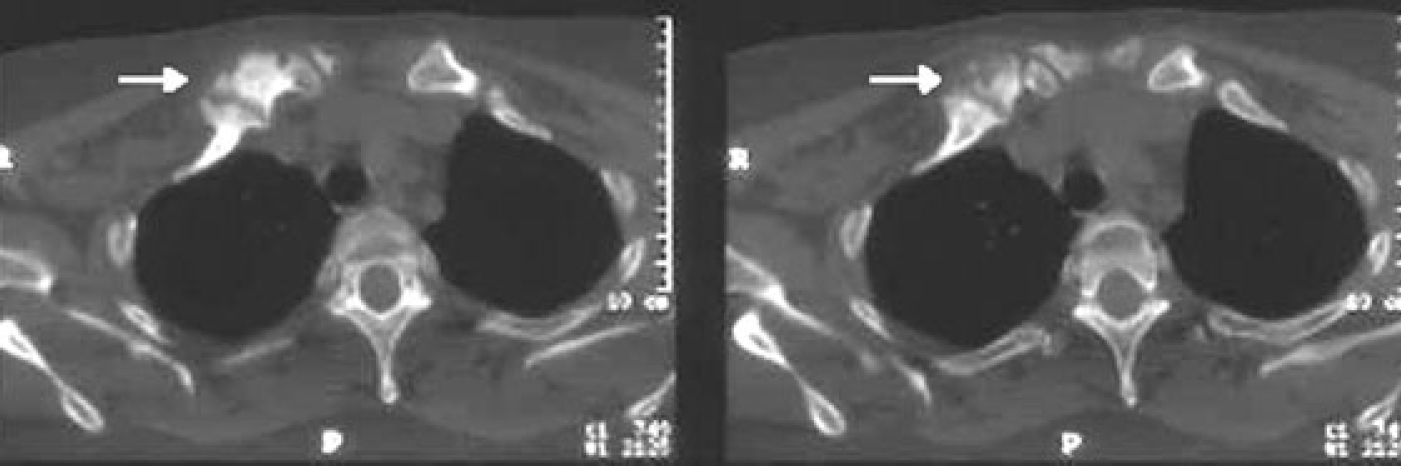
Computed tomography of sternoclavicular joint (patient 2): osteoarthritis and pseudoarthrosis with first rib.
Treatment.
Patient had physiotherapy and two subacromial steroid injections with little effect. The patient underwent excision of medial end of the clavicle and, 12 months later, she was fully asymptomatic when she was discharged from the clinic.
Case 3
History.
A 33-year-old lady presented with a history of left shoulder pain for three years. She described a previous direct injury to her left shoulder, although the pain settled soon after that and restarted just after the birth of her second child. Two previous subacromial injections did not relieve the pain.
Examination.
She had normal shoulder silhouette, no muscle wasting and no tenderness over the shoulder girdle. She also had a nontender prominent left sternoclavicular joint. Her range of movements was restricted, with flexion to 140° and abduction to 110°. Subacromial impingement signs were positive, in conjunction with an inability to shrug the affected shoulder.
Investigations.
An ultrasound scan of the affected shoulder was completely normal. A CT scan of the prominent sternoclavicular joint showed osteoarthritis with hypertrophy of the medial end of the clavicle.
Treatment.
The patient was initially referred for physiotherapy, which did not improve the range of movements. She then underwent excision of the medial end of the clavicle. Twelve months after surgery, she was discharged from the clinic with full resolution of symptoms.
Case 4
History.
A 36-year-old man was referred to our clinic with right shoulder pain for 10 months. The pain was radiating over right clavicle, trapezius muscle and lateral arm. There was no history of trauma. A previous course of physiotherapy and subacromial injection had provided very little benefit.
Examination.
There was reduced right shoulder forward flexion and abduction to 120°. Impingement signs were positive. There was no tenderness over the sternoclavicular joint. On the basis of clinical findings, the patient underwent arthroscopic subacromial decompression and excision of distal clavicle. His symptoms improved to some extent postoperatively, although shoulder pain continued to be an issue 12 months after surgery. During routine follow-up, it was noticed that the patient could not shrug the affected shoulder. There was no tenderness over the sternoclavicular joint.
Investigations.
Plain shoulder X-rays did not reveal any abnormality. A CT scan of the sternoclavicular joint revealed osteoarthritic changes.
Treatment.
Because physiotherapy failed to improve the symptoms, the patient underwent excision of medial clavicle and, 2 months postoperatively, he was completely asymptomatic and regained full range of movements. He was followed up for 9 months.
Case 5
History.
A 30-year-old lady presented to our clinic with a 11-year history of pain in her left shoulder, which started after lifting another person. She had several courses of physiotherapy with little benefit. She was also given one subacromial injection that relieved the pain for approximately 6 months.
Examination.
There was no obvious muscle wasting and no swelling over the shoulder girdle, including the sternoclavicular joint. There was minimal tenderness on palpation over the sternoclavicular joint and also along the clavicle. Impingement tests were negative. Flexion was restricted to 140° and abduction to 100°. The patient was unable to shrug the affected shoulder.
Investigations.
Plain X-rays of the affected shoulder did not reveal any abnormality. An ultrasound scan showed a normal rotator cuff and moderate subacromial bursitis. ACT scan of the sternoclavicular joints suggested arthritic changes on the left side.
Treatment.
The patient responded very well to a course of physiotherapy. Three months later, she regained a full range of movements and was completely asymptomatic. She was also able to shrug her left shoulder normally. She was followed up for 9 months.
Results
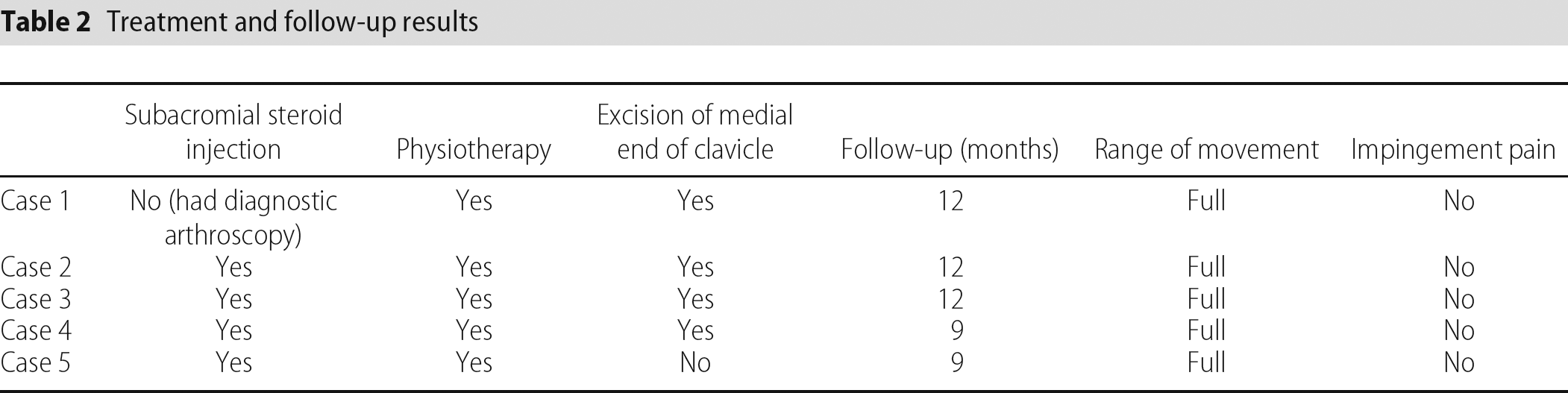
The results obtained are summarized in Tables 1 and 2.
Clinical examination and investigations of shoulder
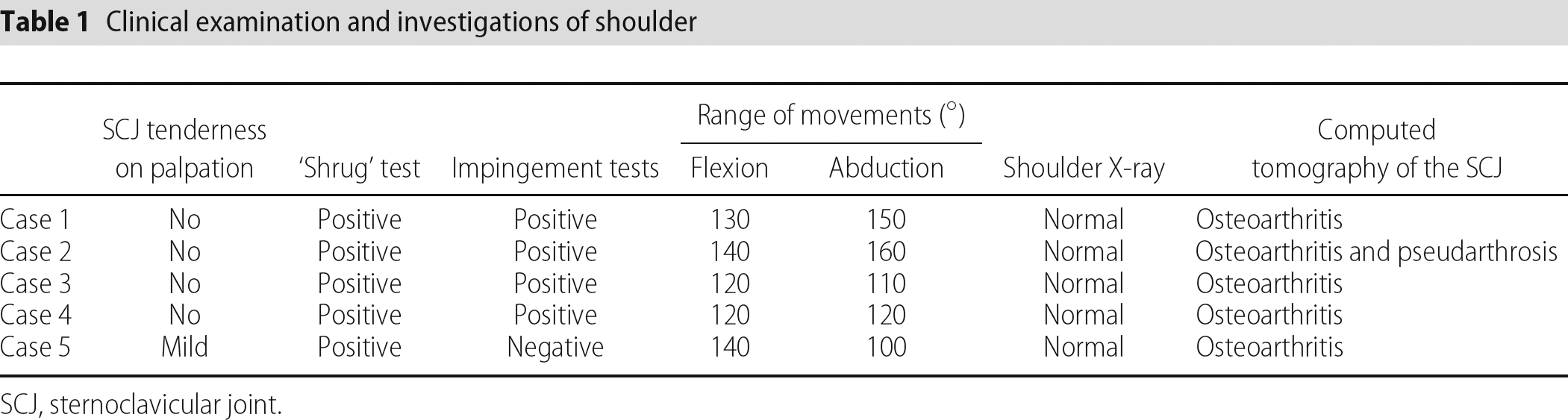
SCJ, sternoclavicular joint.
Treatment and follow-up results
Discussion
The sternoclavicular joint plays an important role in the biomechanics of the shoulder girdle, allowing the clavicle to elevate approximately 35°, rotate forward 10° and rotate around its longitudinal axis 45° during the arm elevation [4].
Osteoarthritis of the sternoclavicular joint is a common condition with increasing age, usually affecting the joint bilaterally [5]. Postmortem examinations have demonstrated minimal degenerative changes in some patients in their third decade, whereas these changes were present in almost all patients by the fifth decade [5]. Unilateral osteoarthritis is normally associated with local tenderness, which can lead to restricted movements in the affected shoulder [5].
Sternoclavicular joint pathology can be clinically evaluated by the ‘shrug test’ [6], which has also been described for accessory nerve palsy [7]. Patients with massive rotator cuff tears have a positive ‘shrug sign’ as a result of their inability to actively initiate abduction of the arm [8], [9]. During the shrug test, the corresponding shoulder is elevated and, subsequently, the clavicle elevates approximately 35°. This movement arises from the sternoclavicular joint. Any restriction in sternoclavicular joint mobility results in decreased shoulder elevation and a positive ‘shrug test’. This is compared with the unaffected side. We have demonstrated that, in these five cases, subacromial impingement was caused by the inability of the clavicle to elevate and rotate during arm elevation as a result of degenerative changes in the sternoclavicular joint. This leads to reduced mobility of the scapula and therefore the acromion will impinge on the subacromial bursa and rotator cuff. The results of the present study show decreased forward flexion and abduction of the shoulder but normal external and internal rotation, which demonstrates that scapula rotation is impaired.
All five cases were referred to our clinic with shoulder subacromial impingement pain. Close examination revealed that they had an inability to shrug the affected shoulder as a result of a reduced mobility of the corresponding sternoclavicular joint caused by osteoarthritis. None of the patients had any initial symptoms localized to the arthritic sternoclavicular joint. All patients underwent appropriate investigations, including a CT scan of the sternoclavicular joint, which confirmed erosive changes at the medial end of the clavicle. All patients had a course of physiotherapy but only one had improvement of symptoms after conservative management. The other four patients underwent excision of medial clavicle and were asymptomatic 6 weeks postoperatively.
We recommend that the ‘shrug test’ should be part of routine shoulder examination so that sternoclavicular joint pathology can be recognized at an early stage and acted on appropriately. We have designed an algorithm that could help to identify a pathological sternoclavicular joint as being the cause of shoulder impingement (Fig. 6). To our knowledge, tertiary shoulder impingement as a result of sternoclavicular joint arthritis in the absence of any localized symptoms to the sternoclavicular joint has not been reported in the literature.
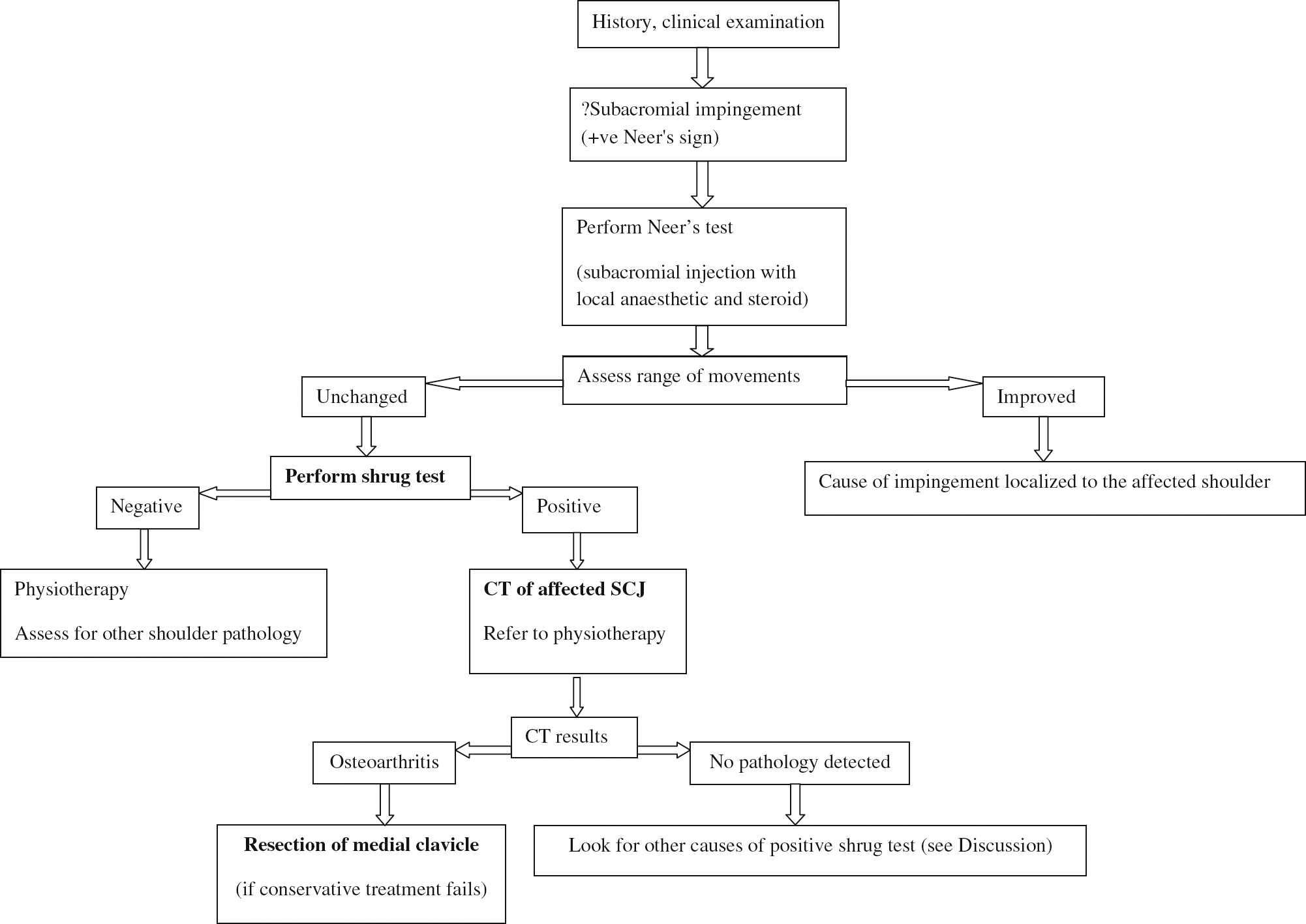
Diagnosis and treatment algorithm of sternoclavicular joint osteoarthritis.
We would like to emphasize that excision of medial clavicle should only be performed when osteoarthritis of sternoclavicular joint has been identified as the cause of shoulder pain/restricted mobility and conservative treatment has failed to improve the symptoms. Excision of medial clavicle should not be considered an option in failed subacromial decompressions in the absence of clear sternoclavicular joint pathology.
The limitation of the present study is the small number of cases but, in our experience, asymptomatic sternoclavicular joint arthritis leading to shoulder impingement is very rare. We have further identified two patients with similar pathology, although they are currently awaiting surgical treatment and the long term follow-up results are not available.