
Abstract
Background
The proximal radio-ulnar joint (PRUJ)-plasty is a new biologic procedure devised to restore an elbow joint after the humero-ulnar joint is destroyed by trauma or infection, or after the distal humerus is resected for tumour.
Methods
After osteotomies on either side of the PRUJ, the joint is rotated 90° and fixed to the distal humerus and the proximal ulna, and functions as a vascularized, innervated synovial elbow joint.
Results
Four young patients had the procedure: one after tumour resection of the distal humerus, another for non-union of the distal humerus and an ankylosed elbow, and two for an old arthrodesis of the elbow after an infection years before.
Conclusion
Postoperatively, three patients had an active elbow joint range of movement from 70° to 120°, and one failed and ankylosed again.
Introduction
We present a new salvage procedure, using the proximal radial ulna joint, to restore elbow joint motion when the ulno-humeral joint is destroyed. This proximal radio-ulnar joint (PRUJ)-plasty can also be used to restore function following ankylosis of the elbow.
Resection of the distal humerus for benign or malignant tumour is rare, although loss of the ulno-humeral joint is more common after trauma or infection. The loss of the elbow joint presents a difficult reconstruction problem, particularly in a young patient. Total elbow replacement is considered in appropriate in the young, and arthrodesis of the elbow is less than optimum because of the loss of motion and the lack of an ideal position. Other arthroplasties such as dermal or fascial lata interposition techniques can also result in a variable outcome.
Materials and Methods
The PRUJ is a relatively expendable joint because radial head excision for fracture in a stable joint is known to leave little deficit. We have devised a simple technique to turn the PRUJ as a block and use it to replace the elbow joint.
The PRUJ is mobilized by osteotomies on either side of it, rotated 90°, and fixed to the humerus and ulna (Figs 1 to 5).
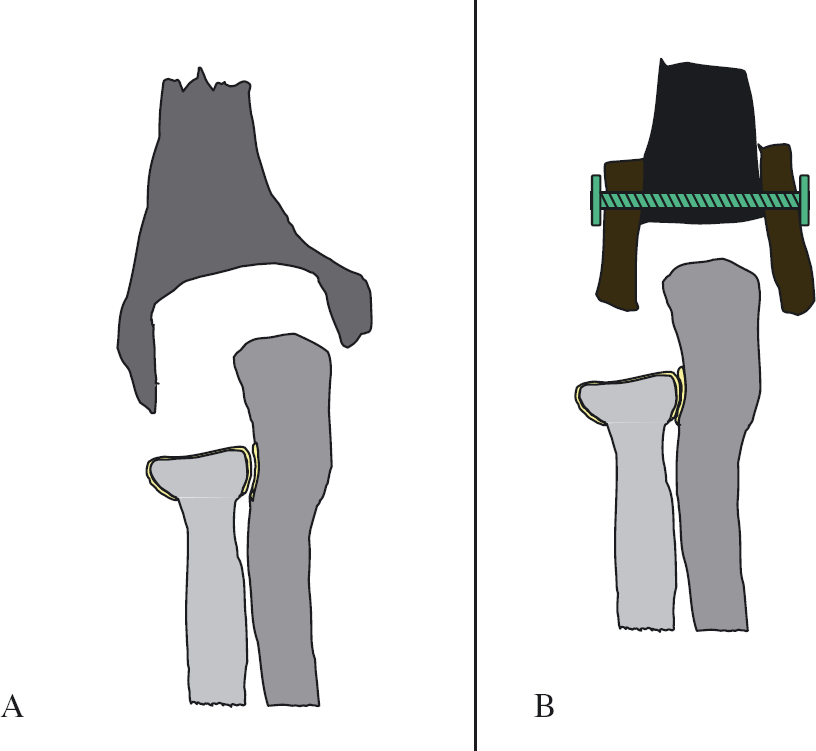
Step 1 of technique for the destroyed joint. The distal humerus is hollowed out as in A, or reconstructed as in B.
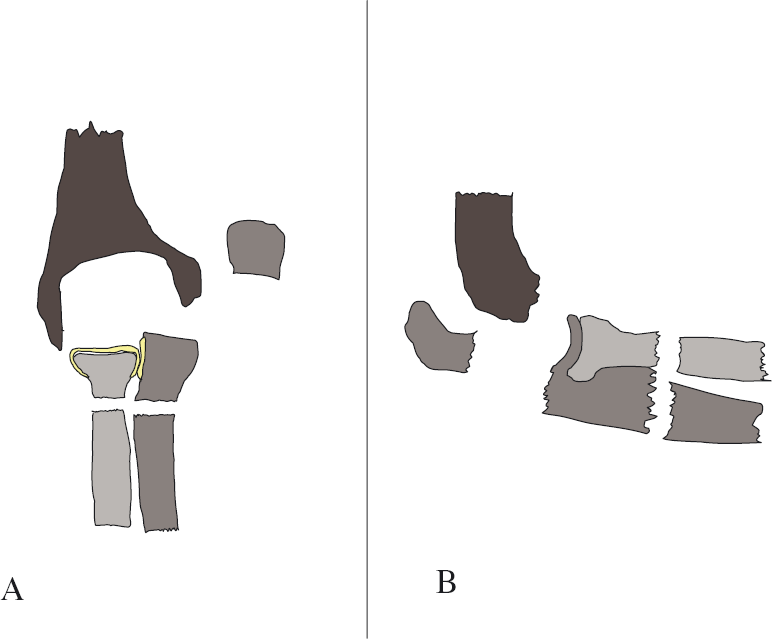
Step 2 of technique, AP and lateral views: posterior approach via olecranon osteotomy, then osteotomy of proximal radius and ulna.
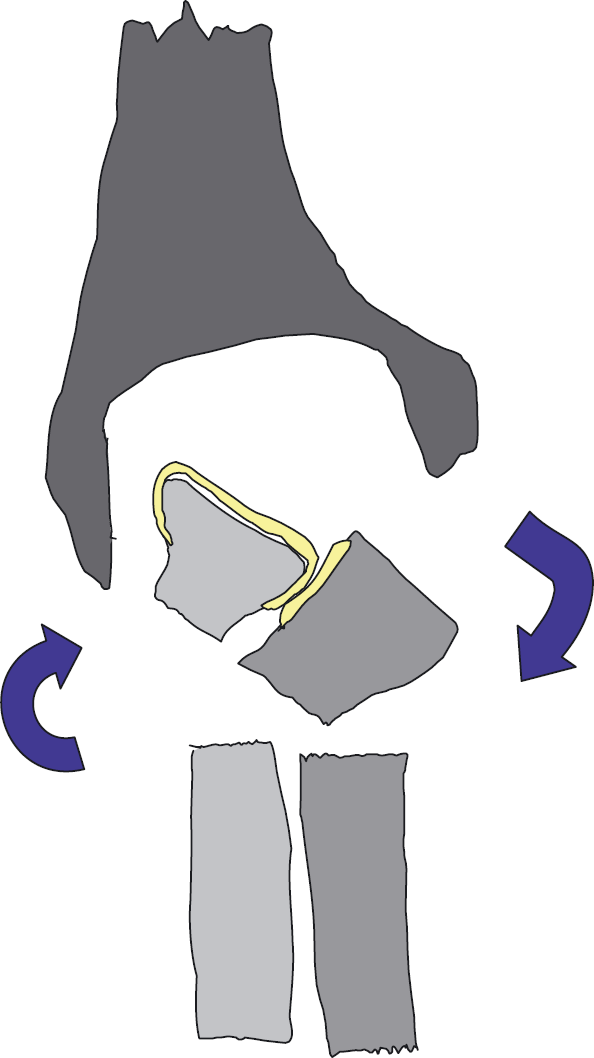
Step 3 of technique: rotation 90 degrees of PRU joint as a unit.
New position of PRU joint for use as elblowjoint.
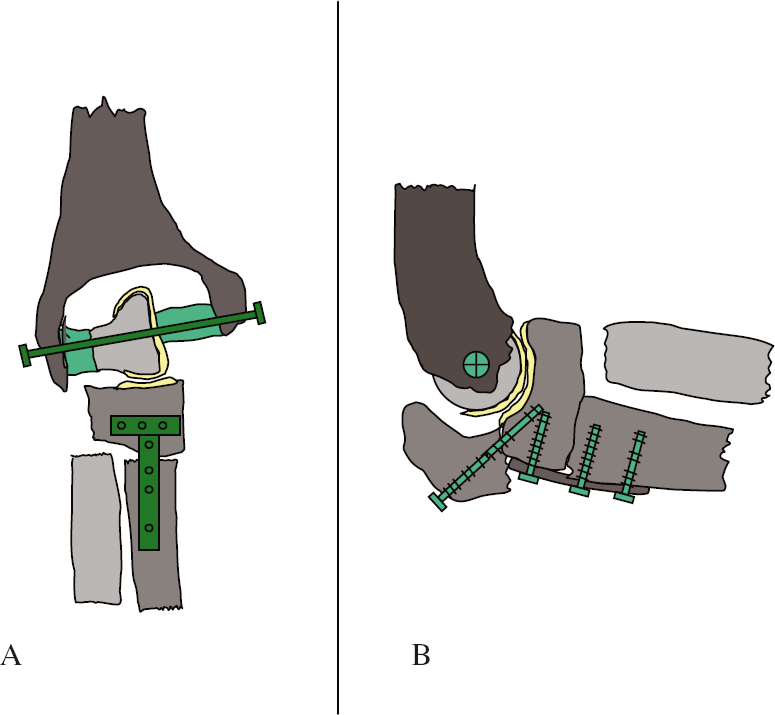
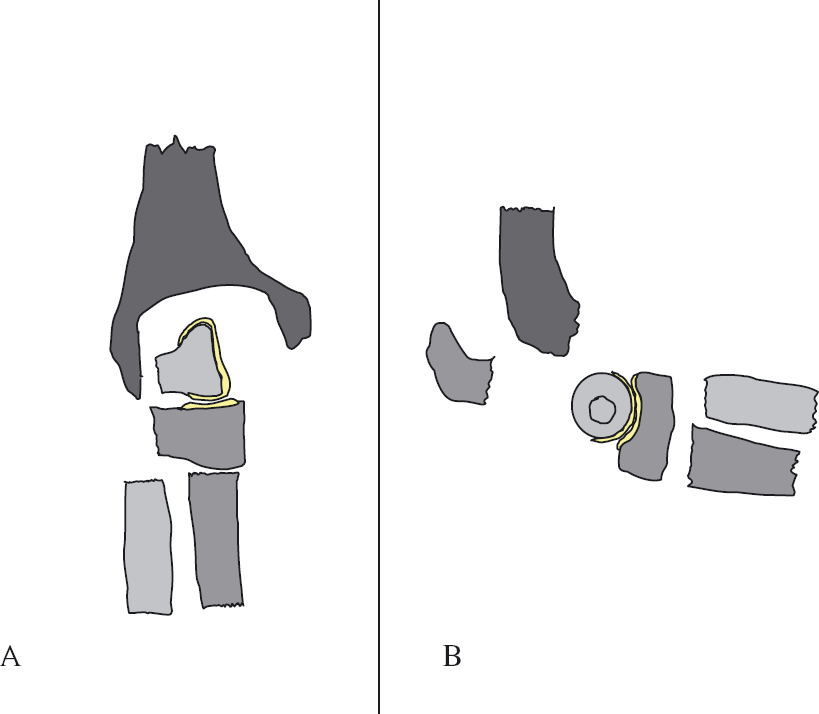
Step 4 of technique, AP and lateral: internal fixation of PRU joint in new position, using bone grafts to fix radial head to humerus. The annular ligament of the radial head is not shown, but the hollowed out humerus leaves room for it.
Technique
A posterior approach is used with an olecranon osteotomy. The distal humerus is hollowed out (Fig. 1A) or, if absent, bone grafts can be used to restore the shape (Fig. 1B). If an ankylosis or fusion between humerus and ulna is present, osteotomy at the level of the ankylosis is undertaken. A second more distal osteotomy of both the radius and ulna is performed just proximal to the biceps insertion on the radius (Fig. 2). A segment of proximal radius and ulna including the PRUJ is thereby created. This block containing the PRUJ is then rotated 90° (Fig. 3), and then fixed to the distal end of the humeral shaft and the proximal end of the ulna shaft as shown in Fig. 4. This enables the proximal radius to be fitted to the distal humerus, with room for the annular ligament of the radial head to rotate around the fixed radial head, rather like a pulley. This PRUJ, now between the humerus and ulna, functions as a vascularized, innervated synovial elbow joint.
The pre-requisite for the procedure is an intact PRUJ. The range of motion (ROM) of this joint in its new position at the elbow is potentially the same as the PRUJ (i.e. as much as 160°).
Results
Three young adults who had lost elbow function as a result of a tumour, trauma or infection underwent a PRUJ-plasty with a satisfactory outcome. A fourth case involving a fused ulno-humeral joint from an old infection was not successful.
Case report 1
A 16-year-old female had undergone resection of the distal two-thirds of the humerus for a chondrosarcoma (Fig. 6). This was reconstructed initially using the removed distal humerus shaft as a bone graft following autoclaving. There was no reconstruction for the elbow at the time of the surgery. Although the tumour did not recur, unfortunately, the bone ‘autograft’ graft re-absorbed over the next 2 years. The humeral shaft was then successfully replaced using a vascularized fibula graft (Fig. 6B), although this still left the patient with no elbow joint function. The patient had to wear a sling because of instability. Six years after resection of the tumour, reconstruction of the joint was finally carried out using the PRUJ rotated to replace the ulno-humeral joint. In this case, the radial head was fixed to the distal end of the humerus (Fig. 6C) without regard for the annular ligament. The ROM was 75° after healing, with good joint stability.
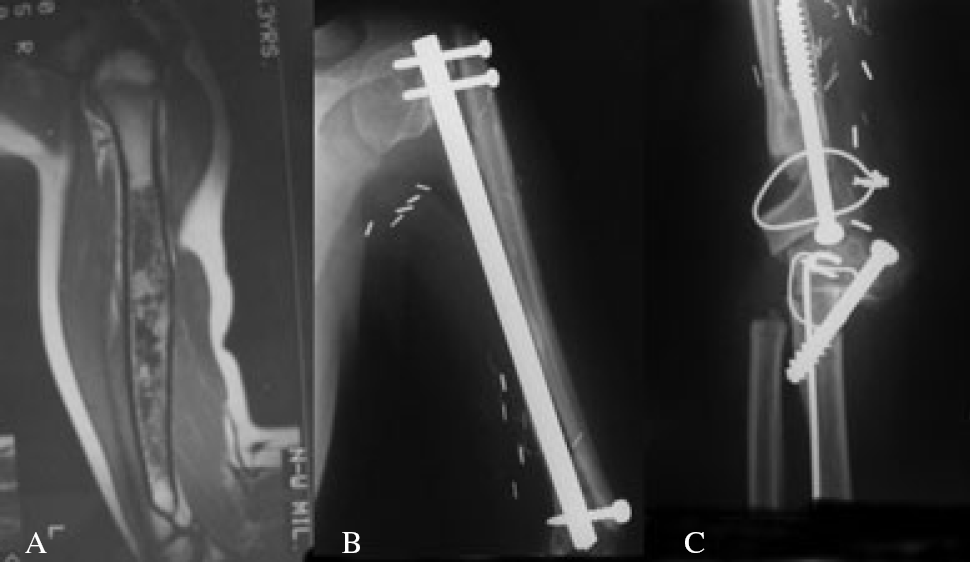
Case 1: (A) Chondrosarcoma before resection of four-fifths of the distal humeral shaft. (B) Fibular graft, but no distal humerus. (C) After PRUJ-plasty, in this first case, the radius was fixed to the humerus.
Case report 2
A 21-year-old female presented with a 10-year-old arthrodesis of the elbow following a childhood infection (Fig. 7). The humerus and ulna were one bone, although the PRUJ joint was intact, giving her normal prono-supination. Osteotomies were carried out above and below the joint and this bone segment, containing the joint, was rotated as a unit to be interposed between the humerus and ulna. The radial head was fixed to the humerus as in the first case, and the side of the proximal ulna to the distal ulna shaft, using a tension band type of technique. This resulted in 120° of movement (Fig. 8).

Case 2: A fused ulno-humeral joint after a childhood infection; note the intact proximal radio-ulnar joint.

Case 2 at 6 months post-op. Final motion was more with near normal pro-suppination.
Case report 3
A 20-year-old male presented with an ankylosed elbow joint along with non-union of the distal humerus through the olecranon fossa following an automobile accident (Fig. 9). He only had motion through the non-union, which was painful enough for him to have to wear a sling. A computed tomography scan confirmed complete ankylosis between the distal humerus and the ulna. The PRUJ was rotated as in the other two cases, although, in this case, the non-united distal humeral fragment was removed and used as bone graft to provide a Y-shaped end of the humerus to accommodate the rotated radial head. This technique preserves the annular ligament and allows it to rotate around the radial head (Fig. 10A, B). His resulting ROM was approximately 100° of flexion.

Non-union distal humerus fracture, screw from failed surgery. Post-traumatic fusion of the ulno-humeral joint was confirmed by CT scan.
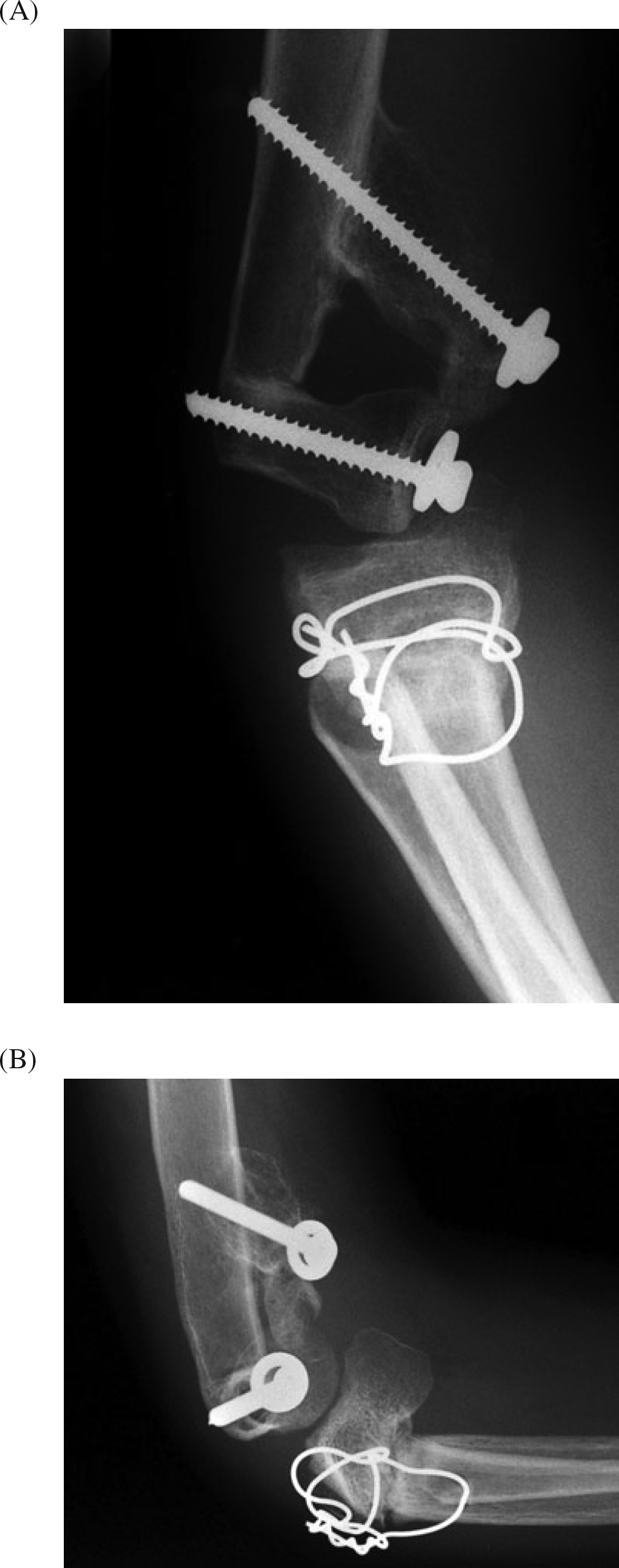
Case 3: (A) Anteroposterior view. Radius fixed to humerus, ulnar fragment fixed to distal ulnar shaft. (B) Lateral view at 2 years, showing the radio-ulnar joint functioning as an elbow joint. Total movement was 90°.
Case report 4
A 19-year-old female presented with an ankylosed ulno-humeral joint with a normal PRUJ after a childhood infection. Her case was almost identical to Case 2. The distal humerus was hollowed out and the PRUJ as a block was rotated and fixed between the humerus and ulna (Figs 1 to 5). Unfortunately, after the procedure, she had exuberant bone formation which refused her elbow joint completely.
Discussion
Many cases of trauma or infection cause global joint damage to the elbow. Sometimes, however, only the ulno-humeral joint is destroyed, leaving the PRUJ intact. This procedure can be used whenever the PRUJ joint is intact and normal.
Reconstruction of the distal humerus for tumour is rare enough for it not to be mentioned in most major text-books on limb-salvage surgery [1], [2]. Malignant bone tumours most often involve the pelvis, knee or shoulder. Destruction of the distal humerus from trauma or infection, however, is relatively more common. After resection of the distal humerus, most tumour surgeons will insert a distal humerus prosthesis [3]–[5], using a hinge type of joint. Although good long-term results have been reported [4], we believe that the lifespan of these prostheses in young people will be limited and, in the cases that we did, loosening developed early.
Resection arthroplasty usually results in either instability or marked stiffness. Arthrodesis of the elbow is not like the knee, ankle or wrist, each of which has an accepted ‘position of function’. There is no position of the elbow that is ideal. Not being able to eat with the right hand is particularly disabling in the Arab world.
When the distal humerus is resected for tumour, the PRUJ is usually intact. After infection of the elbow joint, the PRUJ can be intact because it is a separate joint. The survival of the PRUJ after severe trauma is variable. Unfortunately, patients with osteoarthritis or rheumatoid arthritis usually have involvement of both joints and, as a consequence, are not good candidates for this procedure.
Following restoration of the distal humeral shaft by bone graft if required, the PRUJ can be used to replace the ulno-humeral joint. Although this joint is not quite as stable as the normal ulno-humeral joint, it does have a good ROM and does not dislocate. It is also a real biological joint, with cartilage and ligaments, as well as a blood and nerve supply. This should result in good long-term results.
Following the fourth case, which failed because of bone callus of flexion filling the gap created in the distal humerus, we now suggest staging the procedure. Initially, the distal humerus should be prepared by hollowing it out or using a bone graft to give it the shape required (Fig. 1A, B). Once healing of the distal humerus is complete, the osteotomies of the ulna and radius can be carried out and the PRUJ as a unit turned into place and fixed as shown in Fig. 4(A, B).
Conclusions
The PRUJ, if intact, can be mobilized by osteotomies on either side, rotated as a block, and interposed between the humerus and ulna to replace the ulno-humeral joint. This has the advantage of being both an innervated and vascularized synovial joint. As such, it may survive longer than the current metal or plastic joint prosthesis. Three patients who had no elbow joint pre-operatively had a useful ROM after this procedure. A fourth failed because of spontaneous fusion. In at least three patients, this has been a good salvage procedure.