
Abstract
Background
The present study reports a retrospective case series detailing our experience of the use of Copeland surface replacement hemiarthroplasty (CSRA) for the treatment of rheumatoid arthritis (RA) of the shoulder.
Methods
Fifty-three CSRAs were performed in 45 patients between 1994 and 2004. Forty-six shoulders were followed up at a mean of 62.5 months (range 24 months to 150 months). Assessment included a Constant score, patient satisfaction score, and plain radiographs.
Results
The Constant score improved in all shoulders, from a pre-operative mean of 15.2 to 46.3. Mean abduction improved from 27° to 78°, mean flexion from 47° to 92°, and mean external rotation from 9° to 34°. Fifty-two percent of shoulders showed superior subluxation on plain radiographs. Seven shoulders had over 2 mm of glenoid erosion, of which one underwent reoperation. No implants were loose or required revision. One humeral neck fracture was successfully treated non-operatively. Four shoulders required arthroscopic subacromial decompression.
Discussion
CSRA provides satisfactory results in RA compared to more conventional stemmed implants and total shoulder arthroplasty.
Introduction
Almost two-thirds of adults with rheumatoid arthritis (RA) complain of shoulder pain. The disease initially affects the glenohumeral joint; when the rotator cuff becomes trapped between rheumatoid pannus inferiorly and a swollen subacromial bursa superiorly, severe cuff thinning and deterioration occurs [1]. The gradual progression of disease leads to end-stage joint destruction with severe pain and loss of function [2], [3]. Initial medical management includes the use of analgesia, anti-inflammatory and disease-modifying drugs, and localized steroid injections [1], [4]. Suprascapular nerve blocks and radiosynoviorthesis have also been used with demonstrable benefit [5], [6]. Once medical management of the condition has failed, the surgical options include synovectomy, osteotomy, arthrodesis, and resection and interposition arthroplasty [7][8][9][10][11]–[12]. Prosthetic shoulder arthroplasty is now an established treatment for RA of the shoulder. However, there is still some controversy over which prosthetic option provides the best functional results and long-term survivorship; both total shoulder arthroplasty (TSA) and hemiarthroplasty have been advocated, using conventional or reverse-geometry designs, as well as stemmed or surface replacement humeral implants [13]–[19].
The present study reports our own experience of surface replacement hemiarthroplasty for the treatment of rheumatoid arthritis of the shoulder.
Materials and Methods
Between 1994 and 2004, 53 Copeland surface replacement hemiarthroplasties (CSRAs) were performed by the senior author in 45 patients for the treatment of symptomatic rheumatoid arthritis of the shoulder. All of the patients had severe pain that could not be controlled with medical therapy or conservative measures and had Larsen grade IV or V changes on plain radiographs [2]. All procedures were performed via a standard deltopectoral approach, together with routine excision of the outer end of the clavicle [20]. The uncemented mark-3 hydroxyapatite-coated prosthesis was used in all cases. At the time of the study, four patients had died from unrelated causes, including one with bilateral hemiarthroplasties, and one patient was lost to follow-up, also with bilateral hemiarthroplasties. This left 46 shoulders (19 left, 27 right) in 40 patients (11 males and 29 females) as being available for assessment. The mean age at operation was 64.0 years (range 40 years to 80 years). The shoulders were reviewed at a mean follow-up of 62.5 months (range 24 months to 150 months).
All patients had been assessed pre-operatively by the senior author in a standardized fashion, including history, clinical examination and radiographic evaluation, together with documentation of a Constant score [21], [22]. A subjective preoperative rating of the shoulder was scored on a scale from 0 to 10. Postoperative review was performed by independent observers. Clinical assessment included range of motion, pain assessment using a visual analogue score (VAS), and a Constant score: patients who were unable to abduct their shoulder to 90° scored zero points for power, which otherwise was assessed using an isometric dynamometer (Isobex Engineering, Tokyo, Japan). Plain radiographs were compared with immediate postoperative films. Patients were also asked to rate their satisfaction with their shoulder using a VAS.
Statistical analysis
The outcome data were tested for normality of distribution using the Shapiro–Wilk W-test, which revealed that the data were unlikely to come from a normal distribution (W = 0.854483; p < 0.0001). Therefore, the differences between pre- and postoperative data were analysed for statistical significance using the two-sided Wilcoxon signed ranks test. p = 0.05 was considered statistically significant.
Results
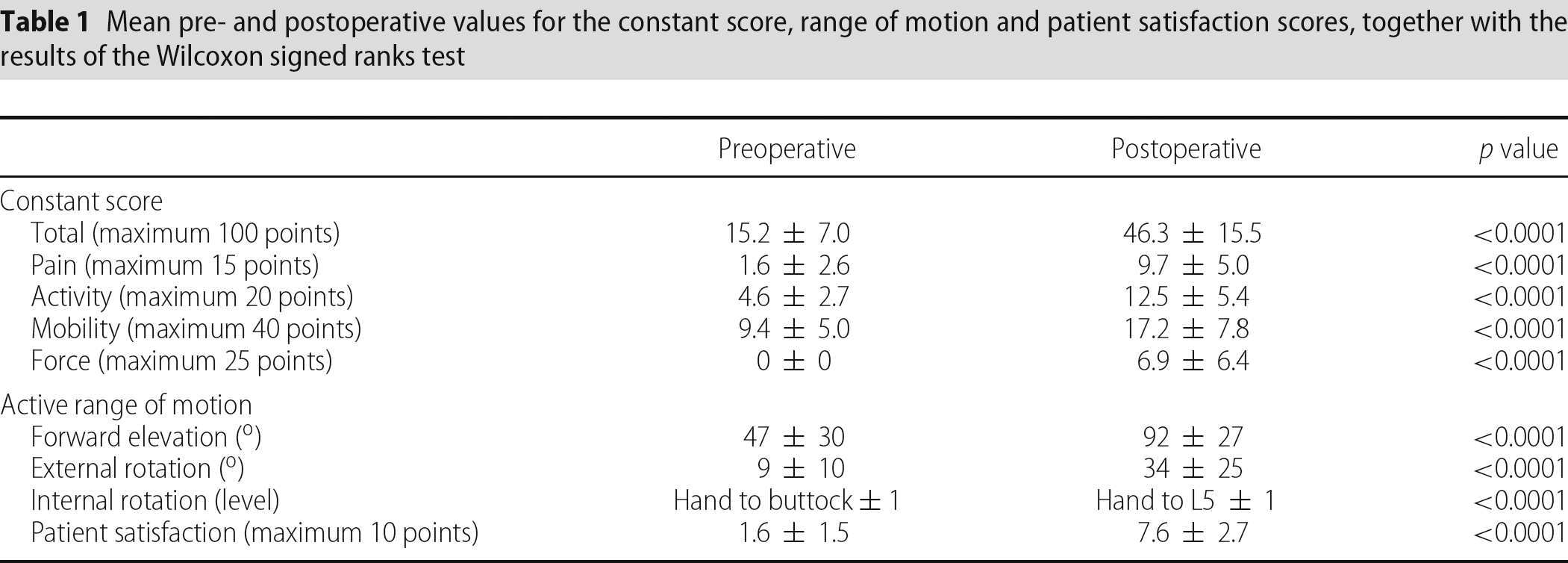
The mean pre- and postoperative values for the Constant score, range of motion and patient satisfaction scores are reported in Table 1.
Mean pre- and postoperative values for the constant score, range of motion and patient satisfaction scores, together with the results of the Wilcoxon signed ranks test
Functional results
There was a highly significant difference between the pre- and postoperative scores for all parameters of the Constant score. The mean improvement in total Constant score was 31.1 points. Mean forward elevation improved by 45° and external rotation improved by 25°.
Pain.
Pre-operatively, 32 shoulders (70%) scored less than 5 points (severe pain), 13 shoulders (28%) scored between 5 points and 9 points (moderate pain), and one shoulder scored 10 points (mild pain). Postoperatively, five shoulders (11%) scored less than 5 points, nine shoulders (20%) scored between 5 points and 9 points, 16 shoulders (35%) scored between 10 points and 14 points, and 16 shoulders (35%) scored 15 points (no pain).
Patient satisfaction
In a subjective assessment by the patient, only four shoulders (8.7%) were reported as being no better compared to pre-operatively. However, all four shoulders had an improvement in Constant score in all parameters. No shoulders were reported to be worse. Forty-two (91.3%) shoulders were reported as being better or much better. Overall, there was a significant increase in the satisfaction score from a pre-operative mean of 1.6 to 7.6 postoperatively.
Complications and re-operations
No shoulder required revision. One humeral neck fracture distal to the prosthesis, sustained during a fall, was treated non-operatively and united within 3 months. Four shoulders had symptoms of impingement with a painful arc of motion that was alleviated by diagnostic injection, which required arthroscopic subacromial decompression. However, one shoulder failed to improve. Marked glenoid erosion was noted on plain radiographs with medial migration of the humeral head. This was causing impingement of the humeral head against the coracoid process, with pain that was abolished by diagnostic injection. A coracoid osteotomy was subsequently performed, with good relief of symptoms. The results reported in the present study include data from all these shoulders.
Radiographic results
Three shoulders showed nonprogressive radiolucent lines of 1 mm width around the peg of the humeral component. No implants were deemed to be loose (i.e. no change in position compared to immediate postoperative films). Fifty-two percent of shoulders showed proximal migration on plain radiographs compared to postoperative films. Seven shoulders (15%) showed more than 2 mm of glenoid erosion. In six of these, there was no associated pain. One shoulder, as mentioned above, had severe glenoid erosion and a coracoid osteotomy.
Discussion
In the present study, we report a significant improvement in pain, function, movement and power after a mean period of over 5 years following CRSA for rheumatoid arthritis of the shoulder. The mean improvement in the Constant score was 31 points. Fink et al. reported a similar improvement using the Durom cup in 45 rheumatoid shoulders with a 34-month follow-up [23]. One of the main objectives of operation is pain relief. In our series, 70% of shoulders had no or minimal pain and, overall, 85% of shoulders had less pain than preoperatively. Despite seven shoulders having a pain score that was the same (five shoulders) or worse (two shoulders) than pre-operatively, all of these seven shoulders were subjectively reported to be better than previously. Other reports of shoulder arthroplasty in the rheumatoid population show a similar proportion of patients obtaining relief from pain [19], [24]–[26].
There were four shoulders that were reported as being no better subjectively, despite having an improvement in all parameters of the Constant score. None of these shoulders had been re-operated or had had complications. This highlights the disparity between surgeons’ and patients’ assessment of outcome; the present study may have benefited from a more extensive assessment using quality-of-life scoring such as the SF-36 or a rheumatoid disease-specific assessment tool; the appropriateness of the Constant score in the rheumatoid population can be questioned [27].
There is still controversy over whether total or hemiarthroplasty provides the optimum treatment for RA of the shoulder. Proximal migration of the humeral component is frequently observed with both TSA and hemiarthroplasty, and was observed in 52% of cases in our series [24], [25], [28]–[30]. This occurs irrespective of the rotator cuff status at the time of surgery [25], [31]. Therefore, a concern with TSA is that, as the rheumatoid rotator cuff deteriorates with proximal migration of the humeral component, eccentric forces on the glenoid component will lead to its loosening and failure [32]. The prevalence of progressive radiolucent lines around the glenoid component in RA is reported to be extremely high, ranging from 50% to 90%; Sperling et al. reported frank loosening of the glenoid component in 51 of 152 TSA [14], [19], [25], [27]–[30], [33]. However, although the majority of revisions in TSA are performed for problems with the glenoid component, the rate of revision, reported at approximately 8%, is far lower than might be expected given the frequency of radiolucent lines and loosening [14], [25], [29].
The rate of glenoid erosion after hemiarthroplasty has been reported at up to 98%, although Alund et al. report that glenoid erosion had no correlation with the functional result or pain [26]. Therefore, with hemiarthroplasty, a concern is that progressive glenoid erosion may lead to pain requiring revision. Again, however, the rate of revision for erosion is much lower, at between 6% and 9% [24], [27], [29]. In the current series, 15% of shoulders had over 2 mm of glenoid erosion, of which one shoulder required reoperation.
Few series directly compare the functional results of TSA and hemiarthroplasty. Trail et al. report no difference in outcome between the two in a series of 40 TSA and 65 hemiarthroplasties with a mean follow-up of greater than 5 years [27]. In a series of of 25 TSA and 36 hemiarthroplasties at a relatively short mean follow-up of 30 months, the only difference was improved active elevation in the TSA group, although there was more severe disease pre-operatively in the hemiarthroplasty group [33]. In one of the largest series, Sperling et al. report on 195 TSA and 108 hemiarthroplasties performed for RA, of which 108 and 63 were available for assessment, respectively [29]. Overall, there was no statistically significant difference in outcome between the TSA and hemiarthroplasty groups, although a subgroup of patients with an intact rotator cuff (as opposed to a thin or torn cuff) at the time of surgery had better survivorship, abduction and pain scores if a TSA was performed.
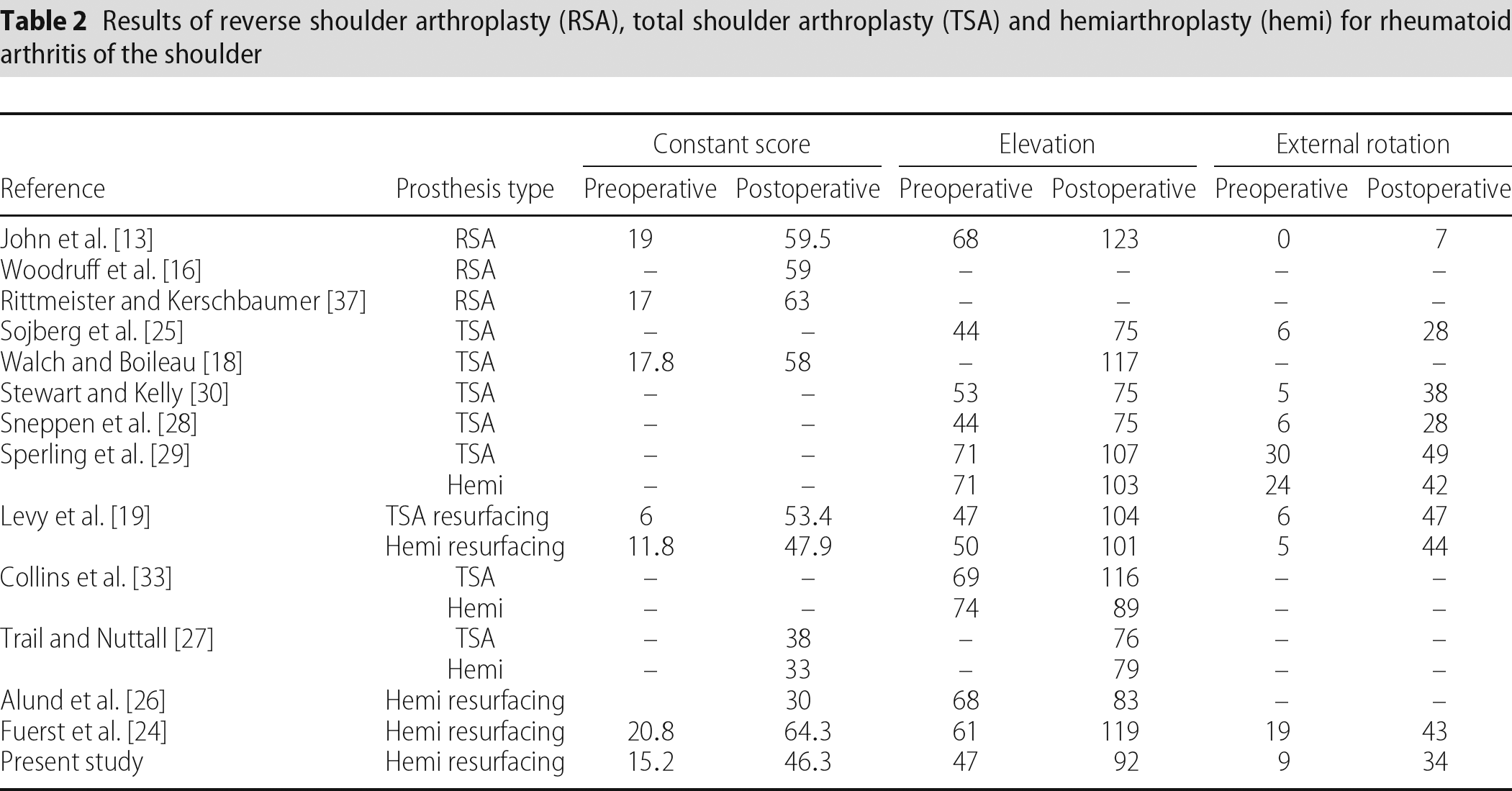
The status of the rotator cuff at the time of surgery in RA is variable; Kelly et al. reported that the cuff was normal in only 13% of arthroplasty cases compared to the 32% to 55% reported in other studies [19], [24], [30], [34]. The distinction between a normal and thin cuff may be difficult to make, and the frequency of proximal humeral migration implies that, in any case, the cuff deteriorates with time. Rozing et al. suggested that the rotator cuff should be repaired at the time of arthroplasty, although this was only possible in nine of 21 cases with a cuff tear [35]. Smith et al. report no gain from repair of the rotator cuff in rheumatoid patients, and other studies reported no influence of the cuff status at the time of arthroplasty surgery on the clinical results [33], [36]. In the present study, no patients had a cuff repair at the time of surgery, although the actual status of the cuff (i.e. normal, thin or torn) was not uniformly documented. Reverse shoulder arthroplasty has so far been used in only a small number of patients with RA and severe cuff deficiency (Table 2) and has yet to be reported to be of superior benefit compared to other options; further studies are required to clarify its role in this patient group [16], [37], [38].
Results of reverse shoulder arthroplasty (RSA), total shoulder arthroplasty (TSA) and hemiarthroplasty (hemi) for rheumatoid arthritis of the shoulder
Early reports of surface replacement arthroplasty for RA described a high rate of loosening (25%) after 4 years and its use was abandoned [26], [39]. However, the implant used was cemented, and did not have a central peg. The prevalence of radiolucent lines observed around the humeral component from previous generations of the Copeland implant has been reported at 30% [40]. In the present study, we used the uncemented mark-3 Copeland prosthesis, which is coated with hydroxyapatite, and did not observe any loosening, similar to Copeland's more recent experience [41].
In terms of stemmed humeral components, the majority of complications (i.e. intra-operative fractures or component loosening or subsidence) appear to be associated with the use of uncemented rather than cemented stems [29], [30], [34]. However, rheumatoid patients may require ipsilateral elbow arthroplasty. The use of a stemmed humeral implant leads to the creation of a ‘vacant segment’ stress riser, which predisposes to periprosthetic fracture, and this effect is avoided when using a resurfacing arthroplasty [42], [43]. We had one case of humeral fracture after a fall that healed with non-operative treatment. If a stemmed prosthesis had been in situ, this may have presented a more complex management problem requiring revision or internal fixation [44]–[46].
The present study contains potential bias in its methodology. The operating surgeon performed pre-operative scoring. Patients were not randomized for treatment and there was no control group for comparison. Five patients died or were lost to follow-up; their outcome results were not available for analysis. The strengths of the present study comprise the use of a single surgeon series, following a consistent surgical protocol with prospective collection of data, the use of a validated scoring system, and independent reviewers for postoperative assessments.
All the patients in the present study underwent hemiarthroplasty rather than total shoulder replacement surgery. The potential advantages of hemiarthroplasty include a reduced operating time, easier surgical exposure (and therefore less chance of intraoperative fracture), and lower cost. It is difficult to compare the clinical results of different series directly as a result of the in homogenous patient populations and varying outcome measures. Nevertheless, Table 2 provides a comparison of several different studies and it can be seen that there is little to distinguish between the results obtained with TSA and hemiarthroplasty. There is a trend towards higher functional results with TSA, but this may be the result of bias (e.g. patients with better bone quality or less bone destruction pre-operatively were more likely to receive a TSA). On the available evidence, TSA could be recommended over hemiarthroplasty for RA patients with a bone stock that is adequate to support a glenoid component and an intact rotator cuff. The revision rates for glenoid loosening (in TSA) and glenoid erosion (in hemiarthroplasty) are also comparable; further work is required to investigate whether the functional results after revision are different in the two groups.
We have used the CRSA implant, which has potential advantages over stemmed implants. These include minimal bone resection, avoidance of the ‘vacant segment’ stress riser effect and easier revision surgery [47]. However, this implant cannot be used with severe humeral head destruction (>40%) or poor subchondral bone stock [41]. This may only be confirmed at the time of the surgical procedure and therefore a stemmed implant should always be available as an alternative.
In summary, CRSA provides satisfactory results for the treatment of rheumatoid arthritis of the shoulder. Further work is required to ascertain precise indications for total versus hemiarthroplasty in this challenging patient group.