
Abstract
Background
Operative stabilisation of long segment periarticular, periprosthetic and pathological fractures in humerus is a challenging problem.
Methods
A total of 18 patients were treated by open reduction and internal fixation using the long proximal humeral internal locking system (PHILOS) plate. The types of fractures treated were long segment periarticular fractures extending into the diaphysis (11 of 18), periprosthetic fractures around humeral resurfacing (five of 18) and pathological fractures (two of 18). This study is a retrospective case series review of these cases with a final follow-up observation. The mean follow-up was for 13 months (range 4 months to 48 months). There were 11 women and seven men with a mean age of 52 years (range 19 years to 86 years). Outcomes were assessed using the Constant and Visual Analogue Score.
Results
There was no incidence of loss of fixation, malunion or a vascular necrosis. The mean time to radiological union was 15 weeks (range 9 weeks to 22 weeks). The mean Constant score for posttraumatic fractures at final review was 76/100 (range 64 to 100). The mean Visual Analogue Score was 0.8 (range 0 to 3). The patients with pathological fractures survived for a mean 5 months (4 to 6 months).
Conclusion
The long PHILOS plate fixation provides reliable secure fixation for the treatment of complex humeral fractures, especially long segment periarticular fractures, segmental fractures involving proximal humerus and shaft, periprosthetic fractures around well-fixed humeral resurfacing prosthesis and pathological fractures.
Introduction
Operative fixation of proximal humeral fractures has significantly improved as a result of advances in implant design. However, fractures with extension into the humeral diaphysis, as well as fractures around a well-fixed prosthesis or in pathological bone, remain a therapeutic challenge. Intra-medullary nailing has been preferred as the choice of fixation for comminuted diaphyseal fractures of the humerus. However, proximal humeral periarticular fractures pose a unique challenge because adequate fixation may not be possible in the small and/or osteoporotic proximal fragments. Similarly, decreased bone stock may not provide adequate purchase for internal fixation, which has been advocated for the management of periprosthetic fractures in well fixed humeral prosthesis [1]. Fractures in pathological bone need fixation over a long segment to avoid a stress riser. Closed intramedullary nailing has been the standard treatment of pathological fractures of the humeral diaphysis [2], [3]. However, the soft pathological bone may not provide secure hold to interlocking screws, especially in the very proximal or distal fractures.
Extensive soft tissue dissection needed for the application of long plates and the uneven contour of the bony surfaces has deterred surgeons from using long plates in the humerus. However, pre-contoured locking plates with its angular stability and non-intimate biological fixation have circumvented these limitations of conventional plating [4], [5]. The proximal humeral internal locking system (PHILOS) plate (Synthes, Stratec Medical Ltd, Mezzovico, Switzerland) has been developed to improve screw fixation in osteoporotic bone and to minimize soft-tissue dissection. The plate is pre-contoured for the proximal humerus and allows multiple proximal locking screws in different directions. In addition, the smaller holes allow passage of sutures for reattachment of tuberosities with their corresponding rotator cuff. This increases the security of proximal fixation. The screw holes in the shaft can take either standard or locking screws. Because compression of the plate to the bone is not required, this preserves the periosteal blood supply to the bone. Locking the screws into the plate ensures angular as well as axial stability and reduces the risk of loss of reduction.
Even though the PHILOS plate has been extensively used and studied in proximal humeral fractures, there have not been any studies reported in the English literature regarding the use of the long PHILOS plate. A recent paper in the Chinese literature reports good results in 35 cases of the proximal humerus and humeral shaft post-traumatic fractures [6].
Patients and Methods
The present study is a retrospective case series review with a final follow-up observation. A total of 18 patients were treated by open reduction and internal fixation using the long proximal humeral internal locking system (PHILOS) plate in our institution between 2004 and 2008. The surgery was performed by the two senior authors (D.M. and R.C.) who had extensively used the conventional PHILOS plate for proximal humeral fractures. All case notes were reviewed and the patients were brought to a special follow-up clinic where they were reviewed by an independent observer (M.P.).
The types of fractures treated were long segment periarticular fractures extending into the diaphysis (11 of 18), periprosthetic fractures around humeral resurfacing (five of 18) (see Fig. 1) and pathological fractures (two of 18) (see Fig.2). The 11 patients in the first group include one case in which a long PHILOS plate was used to stabilize a long segment after a failed internal fixation (Fig. 3). Of the five periprosthetic fractures, four were around a well-fixed Copeland resurfacing and one was around a well-fixed Neer prosthesis. One of the periprosthetic fractures around Copeland prosthesis was initially fixed in a different hospital with an AO-T plate, which failed in 4 weeks. The pathological fractures were distal humeral fractures as a result of metastasis from primary carcinoma of the prostate and breast. Both patients also had a proximal metaphyseal metastatic lesion.
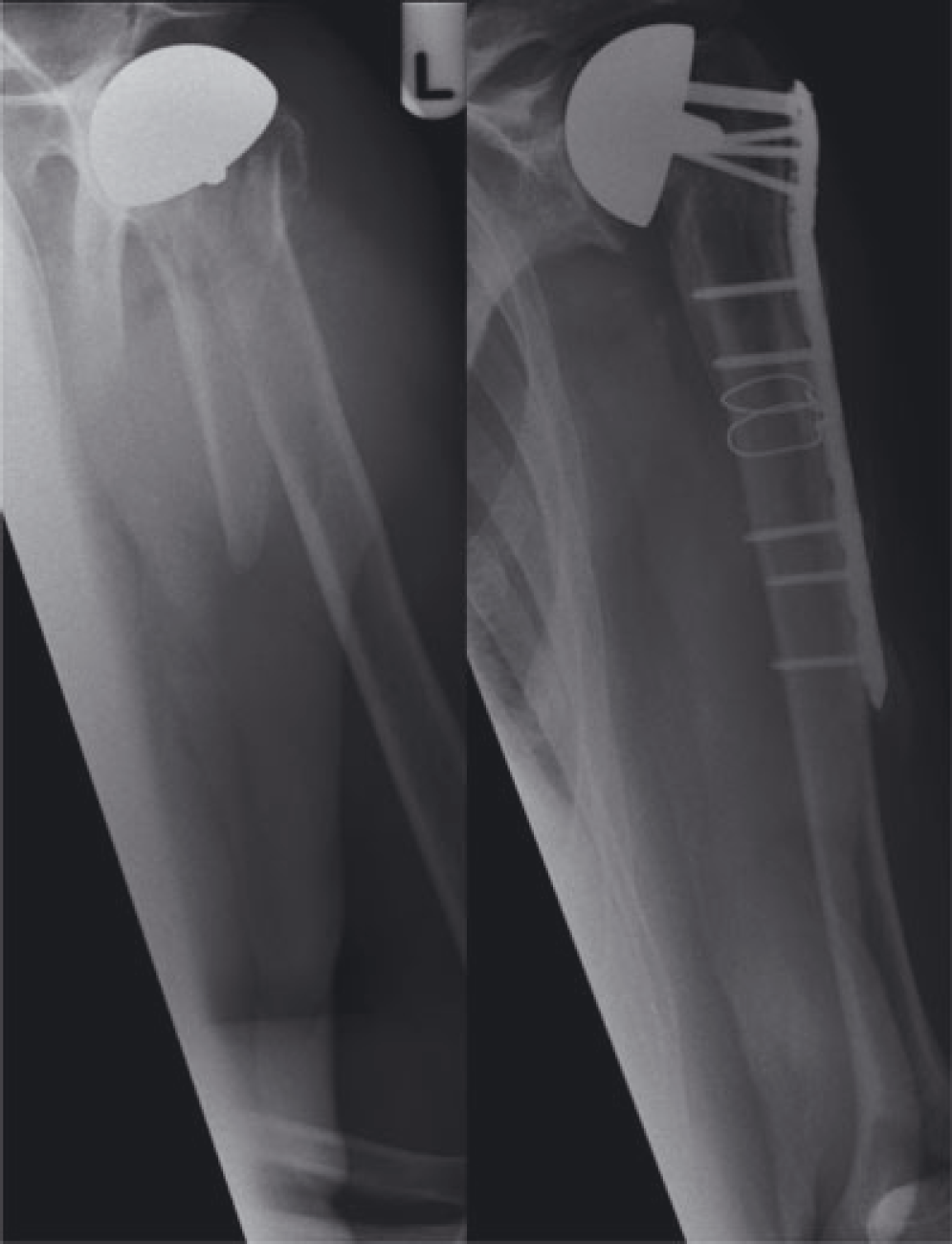
Periprosthetic fracture around a well fixed resurfacing managed with a long PHILOS plate.
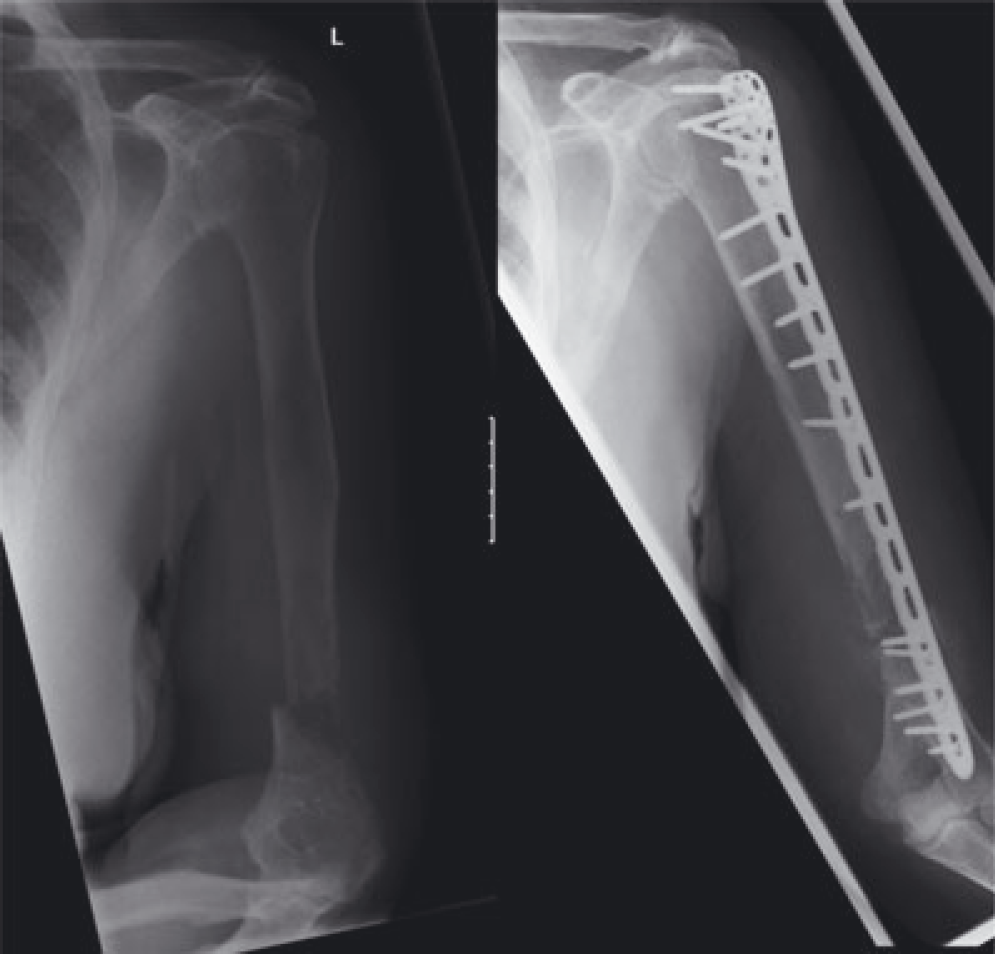
Pathological fracture with associated proximal lesion.

Failed fixation managed with a long PHILOS plate.
Patients were assessed both clinically and radiologically. Their residual pain was assessed using a visual analogue scale. Functional outcome was assessed by Constant Shoulder Scoring system. This includes assessment of pain, activities of daily living (sleep, work, recreation and arm positioning), range of movements and power. Power was assessed by using Nottingham Mecmesin Myometer (Atlantech Medical Device Ltd, Harrogate, UK) and expressed as the average of three measurements expressed in pounds. The Constant score was expressed as the original score with no attempt to standardize for age or sex. Any complications and secondary procedures like removal of metal work were recorded.
Technique
Surgery was performed with the patient in the beach-chair position. Anterior extended deltopectoral approach was used. The radial nerve was identified and protected throughout the surgery. The anterior one third of deltoid insertion was subperiostelly elevated from the insertion to prepare bed for the long PHILOS plate. The fracture was reduced with indirect reduction techniques and the plate was applied in a bridging mode. The elevated insertion of anterior one third of deltoid insertion was reattached to the PHILOS plate using Number 5 Ticron non-absorbable sutures.
In cases of periprosthetic fractures, care was taken to ensure that the prosthesis was stable before plate application. The proximal locking screws were applied on either side of the prosthesis. In the shaft, both bicortical and unicortical locking screws were used.
Postoperatively, a sling was given for 4 weeks, allowing pendulum movements of the shoulder. Check radiographs were performed at 4 weeks postoperatively and the patients were then referred to physiotherapy services for full active, assisted and passive mobilization followed by muscle strengthening programme. All pathological fractures had postoperative external beam radiotherapy after the wound had healed.
Patients were followed up in the clinic at 4 weeks, 3 months and 6 months or until full radiological healing of the fracture. Assessment of shoulder function was carried out by employing the Constant score. Trabecular continuity and an absence of pain at fracture site was considered as union of the fracture.
Results
Of the 18 patients, 15 were available for follow-up. The three patients lost to follow-up included two patients with pathological fractures who had died approximately 4 months and 6 months after surgery. One patient in the post-traumatic fracture group attended just one postoperative follow-up at 4 weeks. The radiograph at this stage showed that the reduction was maintained.
The mean follow-up was for 13 months (range 4 months to 48 months). There were 11 women and seven men with a mean age of 52 years (range 19 years to 86 years). Two patients with segmental fractures had preoperative radial nerve palsy which recovered fully at 4 months and 6 months post-surgery.
The mean time to radiological union was 15 weeks (range 9 weeks to 22 weeks). There was no incidence of loss of fixation or malunion. There was no instance of screw penetration in to humeral head. Avascular necrosis was not radiologically or clinically suspected at our latest follow-up.
The mean Constant score for posttraumatic fractures at final review was 76/100 (range 64 to 100). The mean abduction was 142° (range 90° to 170°) and the mean flexion was 148° (range 100° to 180°). The mean external rotation was 19° (range 10° to 50°).
Two patients complained of mild pain; however, no patient had limitation in daily living or occupation. The mean Visual Analogue Score was 0.8 (range 0 to 3). The average power was 15 on the myometer with a wide variation from 8 to 25 (4 kg to 13 kg). However, the maximum difference was five points (2.5 kg) on comparison with the opposite side. Only one patient complained of weakness in the shoulder. She had a prolonged rehabilitation as a result of her preoperative radial nerve palsy.
We had two patients with pathological fractures. An 81–year-old gentleman undergoing treatment for prostatic carcinoma had a pathological fracture of his proximal humerus, with pathological involvement of the proximal half of the shaft of humerus. He underwent open reduction and plating with a long PHILOS plate followed by radiotherapy. He survived for 6 months and did not complain of any pain in his arm. An 86-year-old lady presented with a painful pathological fracture of the distal humerus, with skip lesions in the proximal shaft. Investigations revealed wide spread metastasis in the skeleton secondary to breast carcinoma. After consultation with the oncology and palliative teams, a decision was taken to operate for relieving pain. She had the fracture stabilized with a long PHILOS plate and underwent postoperative radiotherapy. She survived for 4 months with an asymptomatic arm. Although these patients were not available for follow-up, their next to kin were interviewed on the phone. In both cases, the fractures were described as ‘healed and painless’ by their next to kin.
Implant removal was not routinely recommended. Two patients required implant removal. One was removed as a result of prominent metal work around the shoulder in a thin elderly patient. The other was removed on patient's request. Although, removal was peformed in both cases, it was observed that the deltoid had a very good soft tissue attachment to the bone covering the plate.
Discussion
The present study suggests that the long PHILOS plate provides stable fixation over a long segment in complex fractures involving proximal humerus and shaft, which are not amenable to other forms of fixation. We consider that the proximal fracture fragment is the weakest link in the fixation. The long PHILOS plate provides secure fixation of the proximal fragment with both locking screws, as well as suture holes for the fixation of tuberosities/rotator cuff insertion. The distal fixation is achieved by a combination of locking or nonlocking screws. The locking plate does not depend on the friction between the bone implant interfaces and therefore can be applied on uneven bony contours with minimal soft tissue dissection. Because the pull-out resistance of unicortical locking screws is almost identical to that of similar-diameter bicortical conventional screws, these can be used in the presence of a stemmed prosthesis.
The concern with long lateral humeral plate fixation has been the violation of the anterior half of deltoid insertion. Linear orientation of the screws may also increase the risk of fractures through these holes. To circumvent these problems, helical plate fixation has been described for fixation of long segment proximal humeral fractures. These studies have been mainly cadaveric or biomechanical [7], [8]. Yang reported his experience of helical plate fixation in 10 patients [9]. However, these plates are not commercially available. Contouring a straight plate has been suggested. Screw hole deformation takes place during contouring which damages the locking mechanism in locking plates. In addition, the stresses developed during contouring may affect the fatigue properties of the plate. Cadaveric dissections have shown that musculocutaneous nerve is at risk during the placement of the anterior segment of the helical plate. Anatomical studies have shown that the deltoid insertion is continuous with the lateral intermuscular septum posteriorly and the brachialis and the brachialis fascia anteriorly [10]. Elevation of the deltoid insertion, therefore, may not result in a great loss of deltoid function if these connections are intact.
Among the long bones, the humerus is second only to the femur in frequency of metastatic disease involvement (9.6%) [3]. The most frequent primary tumours are the same as those seen in the other long bones of the body. Closed intramedullary nailing is standard treatment of pathological fractures of the humeral diaphysis. In a retrospective study of 38 fractures caused by metastatic lesions of the humerus shaft, no significant difference in survival rate, pain relief, restoration of function and complications were associated with either nailing or plating [2]. Despite the poor life expectancy, the authors recommended stabilizing these fractures to restore arm function and improve quality of life. We have had limited experience with the long PHILOS plate fixation in pathological fractures. Closed nailing is our method of choice for diaphyseal pathological fractures. However, proximal and distal lesions are not amenable to nailing because there is insufficient purchase in the short fragments. We feel that long PHILOS is certainly a less morbid procedure than large endoprosthetic replacements, which is the only other option in these fractures.
Management of periprosthetic fractures around stemmed humeral component has been described [1]. However, there is scarcity of literature on management of humeral fractures in the presence of shoulder resurfacing. We were able to salvage the humeral resurfacings in our series without compromising the function. Revision to a stemmed implant is an option but is a more extensive surgery with variable outcome.
In our experience, long PHILOS plate fixation provides reliable secure fixation for the treatment of complex humeral fractures, especially long segment periarticular fractures, segmental fractures involving proximal humerus and shaft, periprosthetic fractures around well-fixed humeral resurfacing prosthesis and pathological fractures. We suggest that familiarity with the technique and instrumentation should be achieved before using this implant for these complex fractures.
Footnotes
Conflicts of Interest
None declared