
Abstract
Background
The present study aimed to describe the comorbidity burden of a rotator cuff disease cohort and to examine the effects of patient comorbidities on general health and shoulder-specific outcome measures.
Methods
A retrospective cohort of patients with rotator cuff disease was identified using the coding of the International Classification of Diseases, Ninth Revision, Clinical Modification. Demographic variables and numbers of systemic and musculoskeletal comorbid conditions were collected. General health and shoulder-specific tools were used to assess disability. Analyses using regression, correlation and analysis of variance were performed to assess the impact of comorbidity upon outcome measures.
Results
Three hundred and seventy-three patients with rotator cuff disease were identified. Two-thirds of the group reported at least one systemic comorbidity. Non-shoulder musculoskeletal comorbidities were reported by 80% of the cohort. Women reported a significantly greater number of comorbid conditions than men (p < 0.02). Baseline health-related quality of life and self-reported shoulder function were impacted significantly by comorbidity when controlling for patient demographic characteristics.
Discussion
Comorbidities are common in this population and significantly affect health-related quality of life and self-reported shoulder pain and disability in patients presenting with rotator cuff-related symptoms. Comorbidities should be considered when shoulder disability measures are utilized in clinical practice and when studying outcomes.
Introduction
Rotator cuff disease is common among disorders affecting the shoulder. The spectrum of disease related to the rotator cuff includes subacromial bursitis, rotator cuff tendonitis, and partial and full thickness rotator cuff tears. Over four million physician visits and 20,000 inpatient surgeries related to rotator cuff complaints were reported in 2006 in the USA [1], [2]. These complaints are costly both in terms of healthcare utilization and occupational disability.
Several outcome instruments have been developed to demonstrate the impact of shoulder disease on patient perceived disability, function and pain, both at baseline presentation and after treatment. These patient-reported outcomes measures are becoming a more frequently used tool in the clinical orthopaedic setting because such measures may demonstrate patient perceived baseline disability and may be utilized during the treatment process. In addition, the vast majority of current clinical outcomes research includes validated outcome measures to reflect treatment effect. Given that clinical outcomes research and journal publications frequently influence the clinical practice of care providers, it is important to recognize possible influences on outcomes measures.
Ideally, shoulder disability instruments reflect the impact of shoulder disease on patient function with minimal influence of non-shoulder problems. It has been recommended to additionally use general health outcome instruments in patients with shoulder disorders in addition to limb-specific measures [3]–[6]. There is increasing evidence that comorbid conditions may substantially affect subjective patient outcomes on both general health status and disease or limb-specific measures [7]–[15].
Previous studies have analyzed the effect of comorbidities on shoulder-specific and general health measures for patients with disease processes including adhesive capsulitis and glenohumeral arthritis [9], [15]. Previous investigations into the influence of comorbidity on patients with rotator cuff disease have focused only on those patients selected to undergo surgery [13], [14], [16], [17]. However, minimal information is available regarding the impact of patient comorbidities on outcome measures of patients with the spectrum of rotator cuff disease that includes rotator cuff tendonitis, impingement syndrome and subacromial bursitis at baseline, regardless of treatment chosen.
The present study aimed to describe the comorbidity burden of a rotator cuff disease cohort and to examine the effects of patient comorbidities on general outcome measures and shoulder-specific measures, controlling for demographic variables, in a nonselected patient cohort with rotator cuff-related shoulder symptoms. We hypothesized that comorbidity burden significantly influences health-related quality of life and patient-perceived pain and disability in rotator cuff patients.
Materials and Methods
Subjects
After Institutional Review Board approval, a retrospective cohort of patients diagnosed with rotator cuff tendonitis or bursitis was identified using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) coding from the initial visit. A single ICD-9-CM code 726.10 (Disorders of bursae and tendons in shoulder region, unspecified) was selected. Patients meeting these criteria were included from 1 July 2001 to 18 May 2007. One of several orthopaedic surgeons at a large university medical centre diagnosed rotator cuff disease based on clinical and radiographic findings and selected the ICD-9-CM code at the initial visit. This patient cohort included all new patients to the orthopaedic shoulder clinic and included patients from the local area and referrals from surrounding areas. At the time of the initial visit, patients completed computer-based questionnaires at kiosks designed and staffed specifically for this purpose. Study subjects completed questionnaires related to demographic information, musculoskeletal comorbidities, systemic comorbidities and general health. They also completed three shoulder-specific outcome measures. Patients were only included in the final cohort if complete questionnaire and demographic data were available. All data were available at the time that patient records were reviewed and no subsequent patient contact was made.
Demographic information
The demographic variables collected were age, gender, highest level of education attained and smoking status. Patients were classified into four age groups: < 40 years, 40–49 years, 50–59 years and ≥60 years. Educational level was condensed into three categories: ‘8th grade or less/some high school’, ‘high school graduate’ and ‘any college/college graduate/any postgraduate work’.
Comorbidity information
Patients were asked to report the presence of comorbidities from the following groups based on the Musculoskeletal Outcomes Data Evaluation and Management System questionnaire and Self-Administered Comorbidity Questionnaire [18], [19]: cancer, circulatory system disorders, depression, diabetes, heart disease, haematological disorders, intestinal problems, lung disease, migraines or frequent headaches. ‘Yes’ answers were summed to produce a total comorbidity count. If a particular comorbidity was present, then patients were asked if that comorbidity was limiting using the question ‘Does your (disease) limit your activities’. No definition of ‘limiting’ was provided leaving it to the patient's subjective interpretation. In addition, patients were queried on the presence, and limiting nature, of seven non-shoulder musculoskeletal comorbidities that interfered with their life. These included back, neck, elbow/forearm, hand/wrist, hip/pelvis/thigh, knee/leg and foot/ankle.
General health and shoulder-specific measures
Study subjects also completed computer-based versions of the the Medical Outcomes Study Short-Form 36 (SF-36) [20], [21] and three validated shoulder-specific outcomes tools: Disability of the Arm, Shoulder and Hand (DASH) [22], Simple Shoulder Test (SST) [23] and the Shoulder Pain and Disability Index (SPADI) [5], [24]. For analysis, all shoulder outcome measure scores were adjusted so that 0 represented the poorest outcome and 100 the best.
The standard DASH measure utilizes 30 Likert-scaled questions to assess function, disability and symptoms related to the arm shoulder and hand. Each question is assigned 1–5 points based on the severity of the pain, disability or limitation. An additional optional module was created to address issues related to work. This optional module has four additional questions that specifically address work. The DASH module for sports/performing arts was not used in the present study population. The DASH has been validated and used across populations [4], [25].
The SPADI measure consists of 13 items with five devoted to a pain subscale and eight devoted to a disability subscale [24]. The SPADI was originally described using a 10-cm visual analogue scale but has also been found to be valid using a numeric response [26]. The SPADI has recently been validated across languages and cultures for pain and disability of the shoulder [27], [28]. The SPADI was administered using a numerical response in the present study.
The SST consists of 12 ‘yes/no’ questions [23]. The questions include patients' subjective perception of their shoulder and questions that ask about specific functions and tasks for the shoulder. The reliability, responsiveness and validity of the SST have been studied [3], [29]. The SST has performed well in the age group typical of rotator cuff disease [29].
The SF-36 is a generic measure of health status comprising 36 items and eight subscales. The subscales are scored on a 100-point scale. Subscales are used to generate two summary scores, the physical component score (PCS) and a mental component score (MCS). Summary scores are normalized to the US population with a mean score of 50 and a standard deviation of 10. Scores lower than 50 imply poorer health status. Results from specific groups of patients may then be compared with published norms [30].
Statistical analysis
Univariate analysis was performed for demographic information. Musculoskeletal and systemic comorbidity was analyzed as a categorical variable with five groups of 0, 1, 2, 3 and 4 or more comorbidities based on the distribution of numbers of comorbidities reported. General linear model regression analysis was employed to examine the impact of demographics and comorbidity upon outcome scores. Mean outcome measure scores were compared between categories of patients with different numbers of comorbidities using an unbalanced analysis of variance. Lastly, a linear regression was performed to assess the impact of comorbidity upon outcome measures with comorbidity treated as a continuous variable. SAS, version 9.1 (SAS Institute Inc., Cary, NC, USA) was used for data analysis. p < 0.05 was considered statistically significant.
Results
Five hundred and thirty-one patients were identified with an ICD-9-CM code of 726. 10 were identified at their initial visit, of which 373 (70%) had complete demographic, comorbidity and questionnaire data during the study period. One hundred and twenty-two (23%) patients had no demographic data recorded and were excluded. An additional 36 patients were excluded as a result of missing data on one or more questionnaires.
Table 1 describes the demographic characteristics and comorbidity burden of the cohort by age group. Almost one-third of patients were aged ≥ 60 years. Fifty-seven percent of the patients were male. Three-quarters were nonsmokers and over half the cohort had at least some college education. Over 60% the group reported at least one systemic comorbidity. Non-shoulder musculoskeletal comorbidities were reported by 80% of the cohort. Women reported a significantly greater proportion of both systemic comorbid conditions (χ2 = 15.784, d.f. = 4, p = 0.003) and musculosketal conditions (χ2 = 12.070, d.f. = 4, p = 0.017) than men (Table 2). Hypertension, depression, heart disease and headaches were the most common systemic comorbidities. The most common comorbid musculoskeletal conditions were those affecting the back, neck, knee or leg and hand or wrist (Table 3).
Patient characteristics by age group
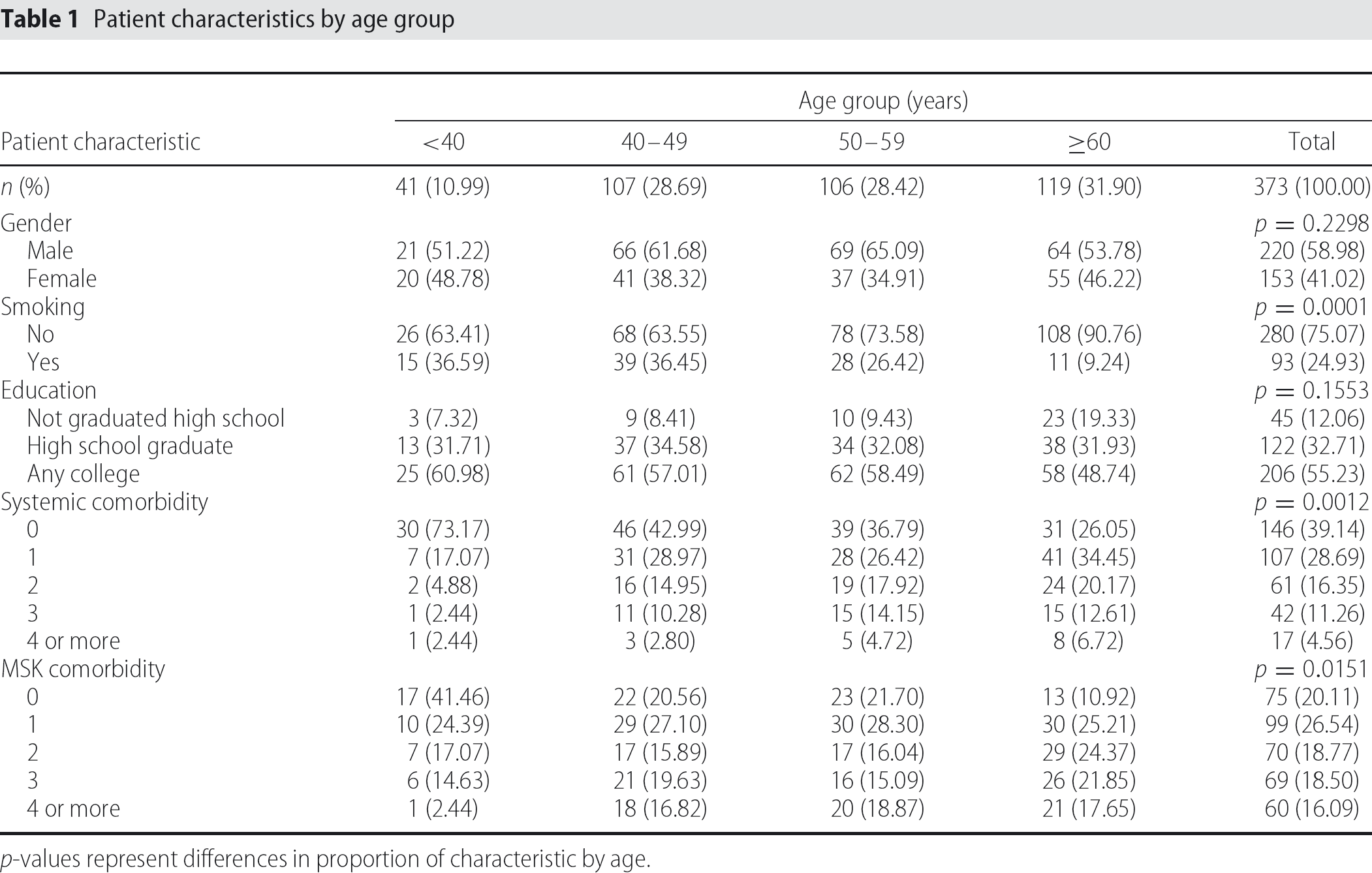
p-values represent differences in proportion of characteristic by age.
Numbers of comorbidities reported by gender
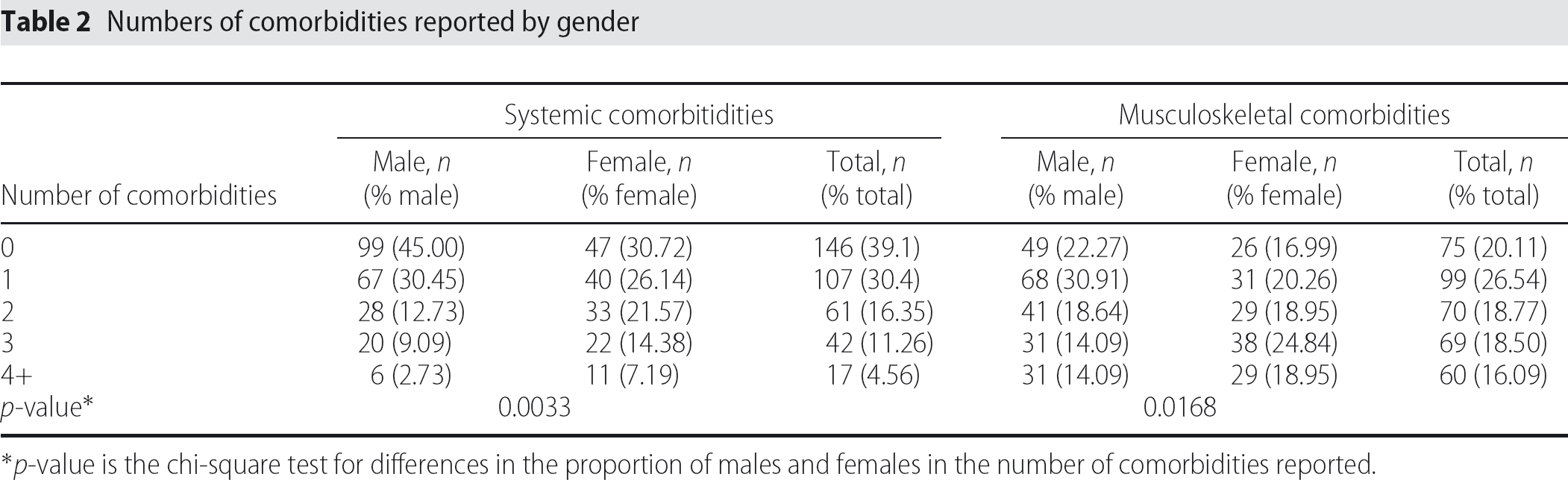
p-value is the chi-square test for differences in the proportion of males and females in the number of comorbidities reported.
The four most frequently reported systemic and musculoskeletal comorbidities by age group
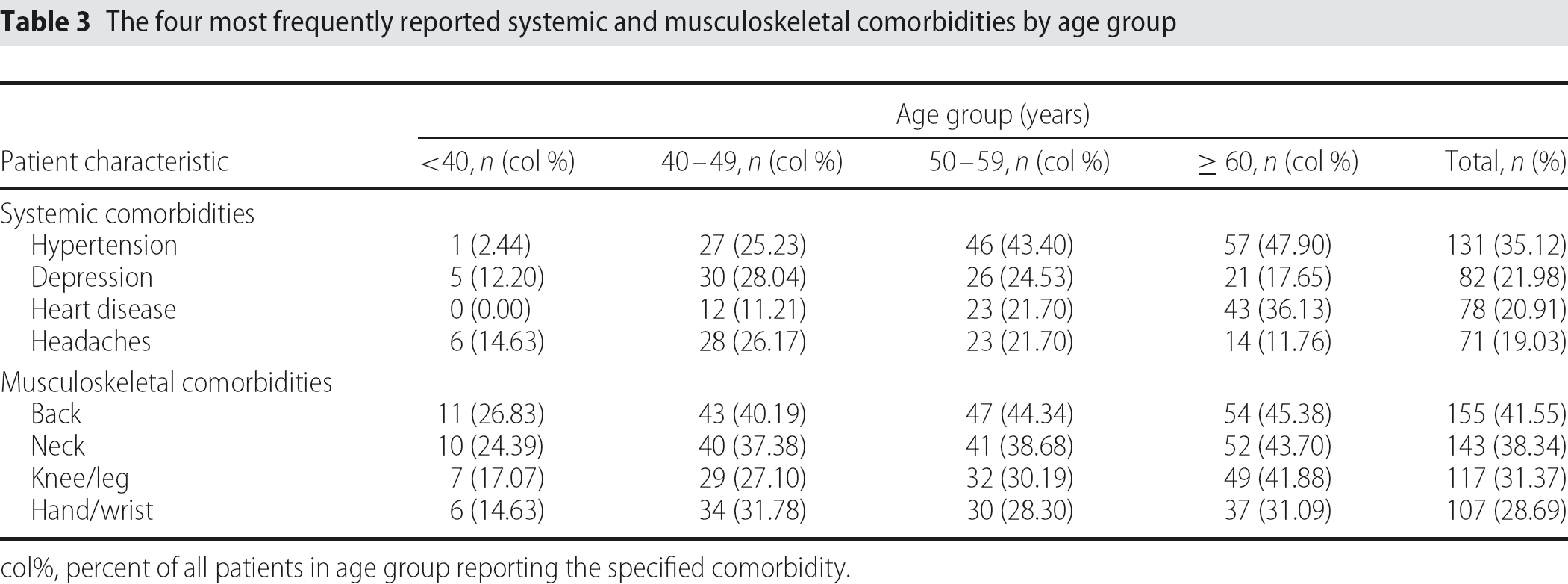
col%, percent of all patients in age group reporting the specified comorbidity.
Tables 4 and 5 summarize the mean scores for outcome measures by age group and number of comorbidities. For all outcome measures with the exception of the DASH Work score, a significant negative linear association was observed between the overall mean score and increasing number of comorbidities (p < 0.005), although the significance of the difference in mean score between number of comorbidities varied (Figs 1 and 2. The DASH Work score exhibited a significant negative linear trend only with the number of musculoskeletal comorbidities reported (systemic: F = 2.09, d.f. = 4,p = 0.082; musculoskeletal: F = 11.11, d.f. = 4, p = 0.000).
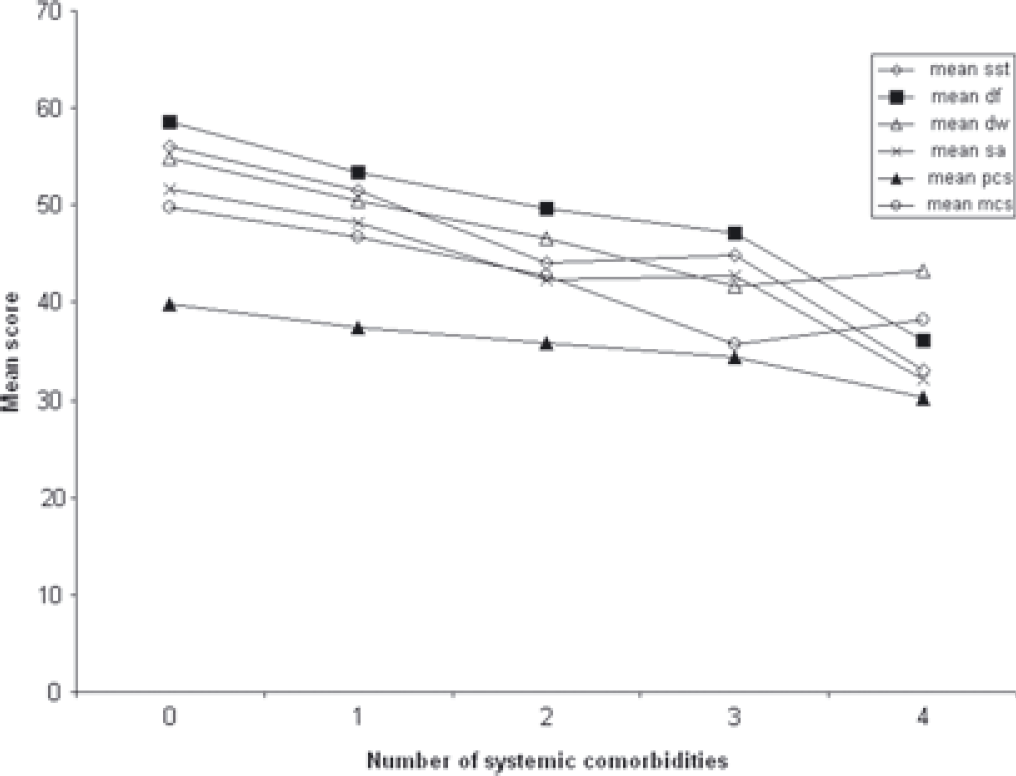
The impact of increasing numbers of systemic comorbidities on outcome measures is demonstrated [sst, Simple Shoulder Test; df, Disability of the Arm, Shoulder and Hand (DASH) score; dw, DASH work module score; sa, Shoulder Pain and Disability Index (SPADI); pcs, Medical Outcomes Study Short-Form 36 (SF-36) Physical Component Score; mcs, SF-36 Mental Component Score].
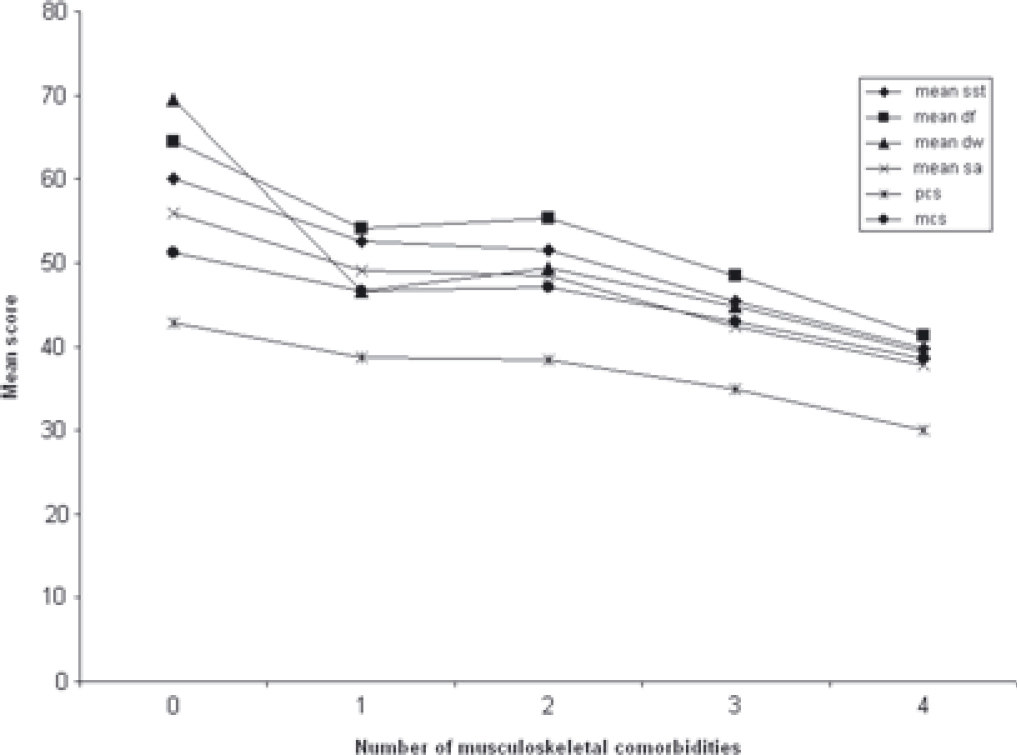
The impact of increasing numbers of muskuloskeletal comorbidities on outcome measures is demonstrated [sst, Simple Shoulder Test; df, Disability of the Arm, Shoulder and Hand (DASH) score; dw, DASH work module score; sa, Shoulder Pain and Disability Index (SPADI); pcs, Medical Outcomes Study Short-Form 36 (SF-36) Physical Component Score; mcs, SF-36 Mental Component Score].
Mean ± SD outcomes scores for patients with an initial diagnosis of shoulder bursitis or tendonitis based on age and number of systemic comorbidities
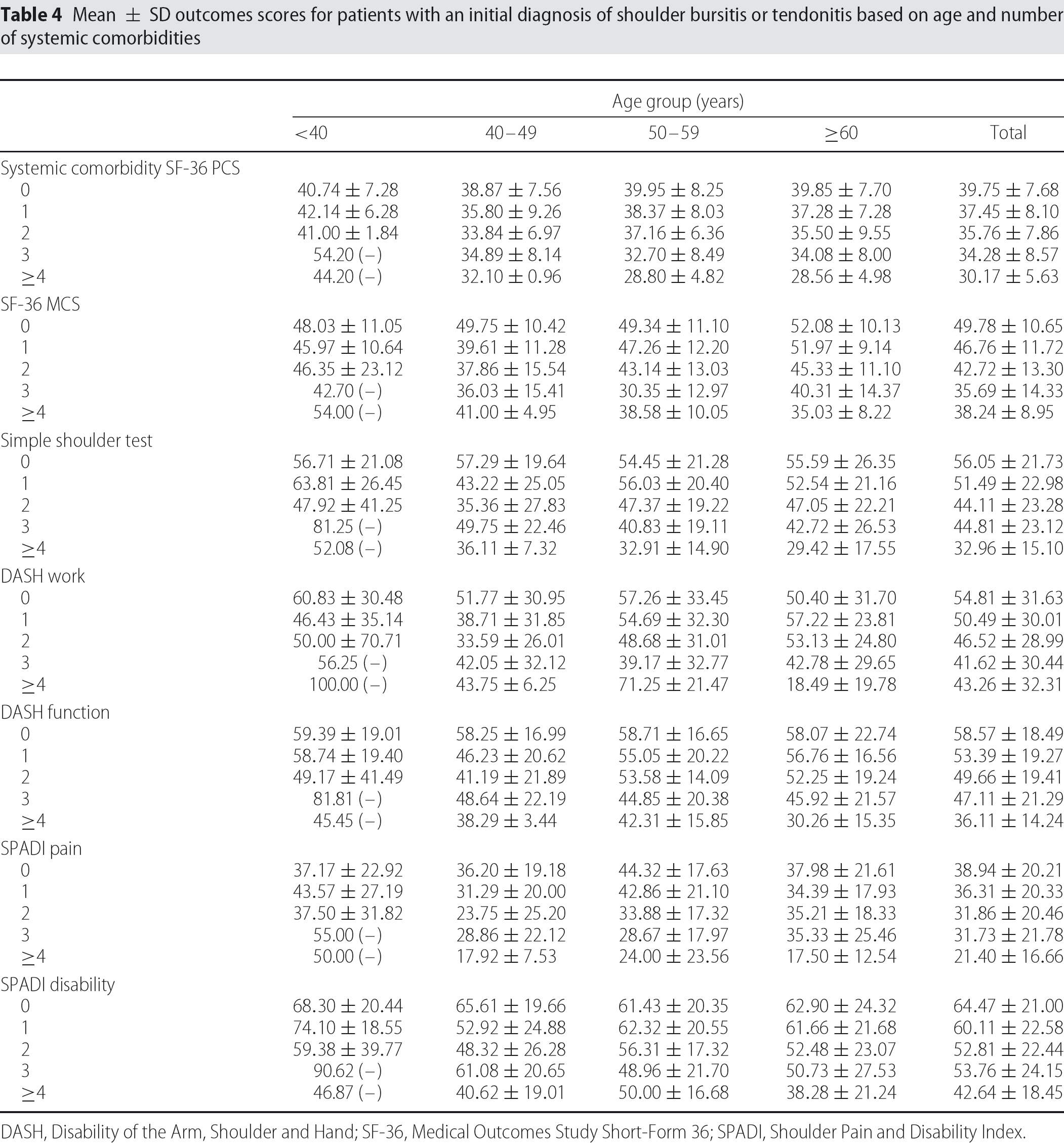
DASH, Disability of the Arm, Shoulder and Hand; SF-36, Medical Outcomes Study Short-Form 36; SPADI, Shoulder Pain and Disability Index.
Mean outcomes scores for patients with an initial diagnosis of shoulder bursitis or tendonitis based on age and number of musculoskeletal comorbidities
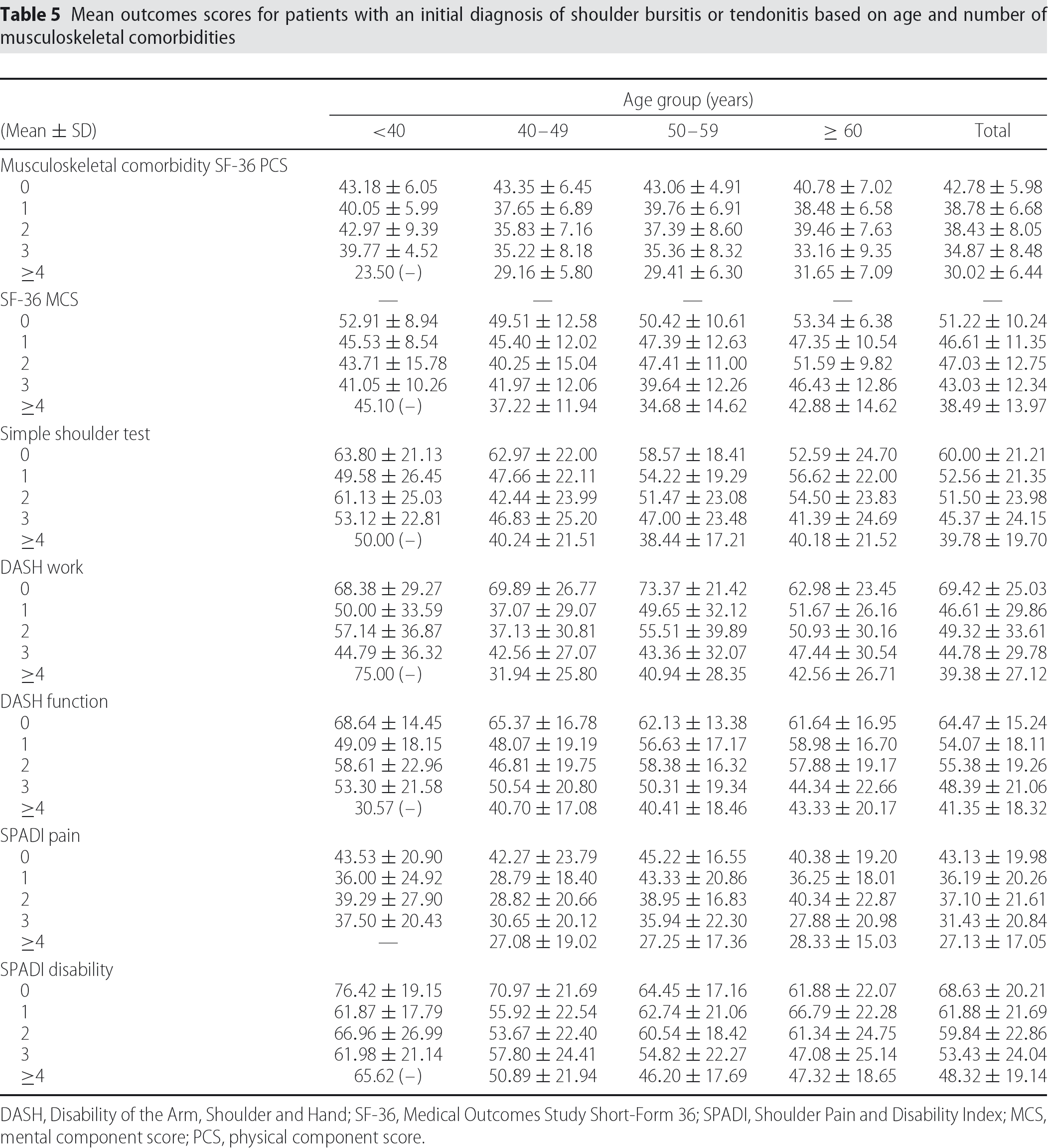
DASH, Disability of the Arm, Shoulder and Hand; SF-36, Medical Outcomes Study Short-Form 36; SPADI, Shoulder Pain and Disability Index; MCS, mental component score; PCS, physical component score.
Regression analysis revealed that health-related quality of life and self-reported shoulder function were impacted significantly by comorbidity when controlling for patient demographic characteristics as demonstrated in Table 6. The number of systemic comorbidities had the greatest effect on the SF-36 MCS after adjusting for the other variables. For each additional systemic comorbidity, the SF-36 MCS score decreased by 6.27 points when all other variables were held constant. The number of musculoskeletal comorbidities reported had the greatest affect on the SF-36 PCS after adjusting for the other variables. For each additional musculoskeletal comorbidity, the SF-36 PCS score decreased by 8.17 points when all other variables were held constant. Age was a significant predictor only in models for the SF-36 MCS and SPADI Disability. Gender was significant in all models except the DASH Work after adjusting for the other variables. Generally, female gender predicted a lower score. In one case, however, the SF-36 MCS, female gender predicted an increase in score of 3.11 points when all other variables in the model were held constant. Being a current smoker consistently predicted a statistically significant lower score, with the largest effect noted for the DASH Work measure.
Factors associated with self-reported assessment of shoulder function for patients with an initial diagnosis of shoulder bursitis or tendonitis
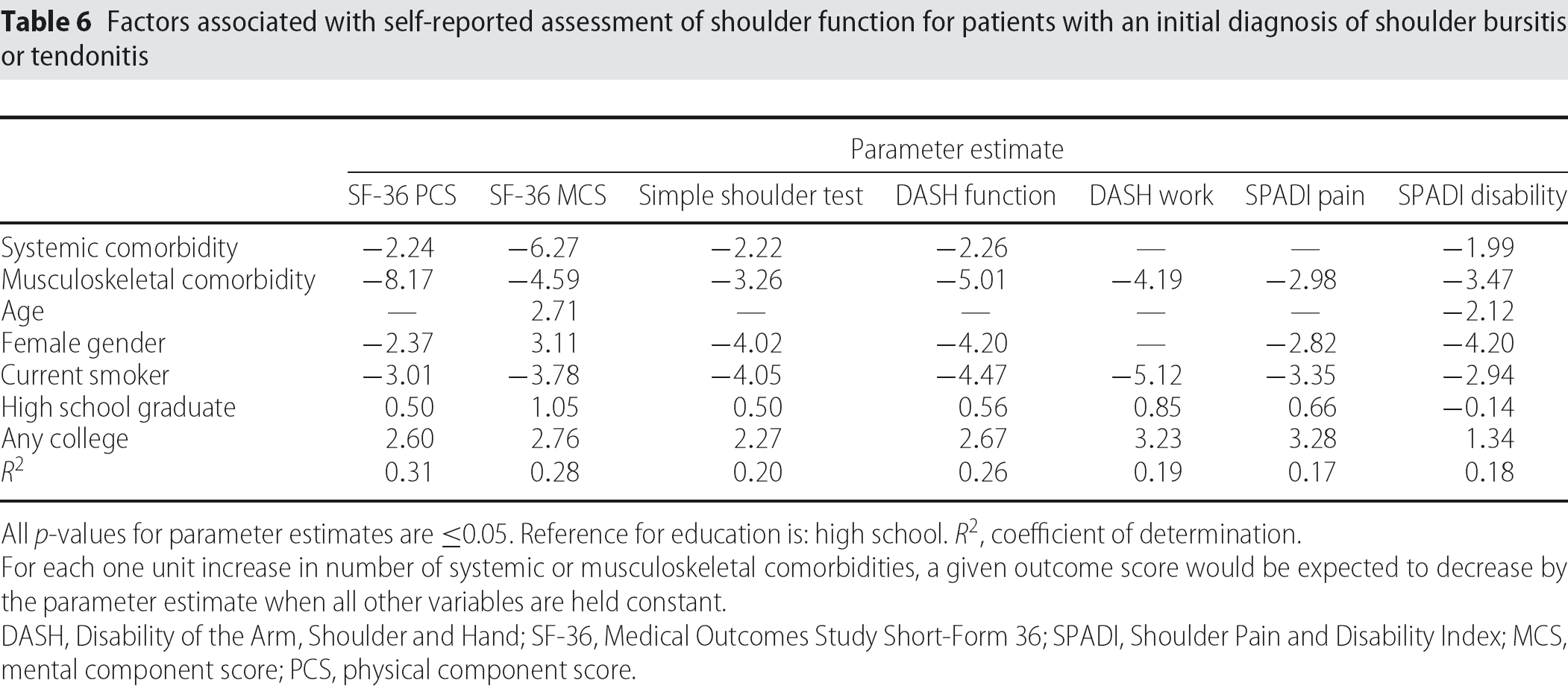
All p-values for parameter estimates are ≥0.05. Reference for education is: high school. R2, coefficient of determination.
For each one unit increase in number of systemic or musculoskeletal comorbidities, a given outcome score would be expected to decrease by the parameter estimate when all other variables are held constant.
DASH, Disability of the Arm, Shoulder and Hand; SF-36, Medical Outcomes Study Short-Form 36; SPADI, Shoulder Pain and Disability Index; MCS, mental component score; PCS, physical component score.
These models accounted for 17% to 31% of the variation in scores, depending on the outcome measured. In other words, up to 31% of the outcome scores could be attributed to the demographic and comorbidity variables in these models. Substituting the number of limiting systemic and musculoskeletal comorbidities for any reported systemic and musculoskeletal comorbidities did not alter the pattern of effect, although the magnitude of effect was greater.
Discussion
The comorbidity burden of patients presenting with rotator cuff tendonitis or bursitis-related symptoms is extensive and complex. Not unexpectedly, the comorbidity burden increases with age. For patients aged 50–59 years, approximately 37% had at least two systemic comorbidities and 49% reported at least two musculoskeletal comorbidities. In patients aged ≥ 60 years, 40% had at least two systemic comorbidities and 64% reported at least two musculoskeletal comorbidities. Almost 90% of patients aged ≥ 60 years in our cohort reported at least one non-shoulder musculoskeletal comorbidity. Although our numbers were higher than those reported by Taylor [31] for musculoskeletal pain observed in a population-based sample in New Zealand, our cohort was specifically seeking treatment for a musculoskeletal disorder. Those seeking treatment may differ in perception of pain and disability from the general population. The numbers from these studies are also not directly comparable as a result of cultural differences between populations and access to medical care.
The present study demonstrates the importance of the cumulative number of systemic and musculoskeletal comorbidities on baseline general health and shoulder disability measures in patients presenting with rotator cuff tendonitis or bursitis-related symptoms. We found a significant negative linear association of additional systemic and musculoskeletal comorbidities on outcome instruments. Similar linear decreases were seen in both general health measures and in the shoulder-specific measures with additional comorbidities. A few previous comorbidity studies have included the musculoskeletal comorbidities of low back pain and degenerative joint disease [14]–[16]. However, the data obtained in the present study suggest that a more extensive exploration of patients' musculoskeletal comorbid conditions may be even more valuable than that for systemic comorbidities when using outcome measures. Approximately 80% of our entire cohort had at least one additional musculoskeletal comorbidity and 27% had at least three additional musculoskeletal comorbidities. Musculoskeletal comorbidities had a large impact on the SF-36 and all of the shoulder disability measures as demonstrated by the negative parameter estimates in Table 6. The relatively small sample of patients with four or greater systemic comorbidities (< 5.0% overall) increased the potential for unstable estimates and thus possibly reduced the significance of the effect.
Despite influence on baseline patient-perceived disability, comorbidities do not appear to negatively affect potential treatment effect in rotator cuff disease based on previous studies. Tashjian et al. reported no correlation of comorbidities with shoulder pain and function 1 year after rotator cuff repair surgery for a chronic rotator cuff tear in a prospective cohort analysis of 125 patients utilizing the DASH and SST measures [14]. Indeed, patients with greater comorbidity burden demonstrated greater improvement compared to pre-operative status. However, a greater number of comorbidities was associated with a poorer postoperative general health status as measured by the SF-36. Also, the present study only evaluated arthritis and low back pain amongst musculoskeletal comorbidities. This was an excellent study methodologically. However, it represents a group selected to undergo surgery and may not include those patients treated with other modalities or high-risk patients who were not offered surgery. Similarly, Boissonnault et al. demonstrated in a multicentre prospective study of 18 patients that undergoing rehabilitation following rotator cuff surgery had similar improvements on DASH and SF-36 scores regardless of comorbidity burden [32]. Despite this improvement, patients with higher comorbidity burden still had significantly lower SF-36 scores after rehabilitation concluded, although DASH scores were not significantly different. More information is needed on the influence of musculoskeletal comorbidities and treatment effect. Although the present study does not analyze treatment, the results obtained demonstrate the significant influence on baseline patient perceived disability as evaluated using common outcomes measures.
The self-perceived disability in rotator cuff patients in the current study is consistent with previous studies that investigated patients undergoing surgery for cuff related disorders [6], [13], [14], [33]. The mean scores in our cohort are similar for selected patients undergoing surgery. This level of disability may be relatively consistent with rotator cuff disease, and the degree of dysfunction as shown in commonly used general assessment tools may not correlate with what physicians perceive as increasing degrees of disease relative to the rotator cuff. Baseline DASH measures in previous studies were very similar for patients undergoing arthroscopic acromioplasty surgery for impingement syndrome compared to patients undergoing surgery for full thickness rotator cuff repairs [13], [34]. Deficits on the SST for partial thickness tears are slightly less than those seen with full thickness tears (6.0 versus 6.9) [35]. Similar physical function limitations were also seen for full thickness tears and impingement patients undergoing surgery as reported by Gartsman using the SF-36 [6]. However, previous studies have shown the shoulder instruments to be more sensitive to shoulder conditions than general health measures [5], [35].
The findings of the present study are limited in that our study group represents patients who have presented to a tertiary care centre for treatment and completed all questionnaires. Missing data from patients who did not complete the questionnaires limited our ability to assess the comparability of those who did not complete the questionnaires and those who were included in our analysis. The results obtained may not be generalizable to less symptomatic patients or patients in other medical care settings. The study cohort was determined by a baseline clinical evaluation by one of several attending orthopaedic surgeons and the diagnosis that was entered using ICD-9-CM codes. It is possible that patients may have been misclassified, either excluding those with rotator cuff disease or including those without disease. All patients were evaluated by an orthopaedic surgeon and ICD-9 codes reflect the diagnosis rendered at the initial evaluation. However, advanced imaging data were not included in the analysis of this cohort.
Another possible limitation is the equal weighting of all comorbidity. It is possible that some comorbid conditions are more significant than others, although this remains unknown. The number of comorbidities may be under-or over-reported by the patients during the initial survey. It is also possible that patients whose rotator cuff disease status was misclassified also differed with respect to number of comorbidities, thus biasing the results. The direction of this possible bias is unknown. Lastly, our models were limited to demographic and comorbidity information collected prospectively at the initial visit as part of our standard clinical practice, but reviewed retrospectively. Other influential demographic and comorbidity variables undoubtedly exist, although were unavailable to us.
A strength of the present study is the large size of the cohort that allows better elucidation of the impact of comorbidity after controlling for other confounders in this population. The present study highlights the need for complete and detailed assessment of the rotator cuff disease patient. The data obtained demonstrate the potential significant magnification of perceived shoulder dysfunction by concomitant patient comorbid conditions, including musculoskeletal comorbidities. These factors should be routinely scrutinized when evaluating patients with rotator cuff disease, when care providers and researchers utilize disability measures in their clinic practice, and when designing or interpreting clinical outcomes research and publications.
Footnotes
Conflicts of Interest
None declared
Acknowledgements
Dr B. R. Wolf's work was supported by a grant from the National Institutes of Health Mentored Clinical Research Scholar Program at Iowa (5K12RR017700-04) and was completed when he was an Iowa Scholars in Clinical Investigation Program trainee (9K30RR022268-06).