
Abstract
Background
The coracoid cortical ring sign is a radiographical view that targets the coracoid base. We hypothesized that the use of this view to treat acromioclavicular separations would achieve desirable results with a rapid, percutaneous procedure.
Methods
Percutaneous coracoclavicular screws, guided by the cortical ring sign view, were used to treat acute, Rockwood grade III or greater acromioclavicular separations with instability to cross-body adduction. The anaesthesia database, clinical and radiographical outcomes were retrospectively reviewed for 41 cases (average age 35 years, range 18 years to 78 years). Average follow-up was 4.7 months (range 1 month to 23 months).
Results
There were six episodes of screw loosening (15%); three of six required an additional surgical procedure. The average residual joint subluxation at final follow-up was approximately 40%, which was significantly improved from the pre-operative displacement (p < 0.01) and not statistically different from the reduction achieved with the screw in place. All patients had full range of motion and, using the modified UCLA score, 98% (40/41) achieved ‘Good to Excellent’ results. The procedure was rapid (average surgical time: 35 minutes), minimally invasive (average blood loss: 15 mL), and the coracoid cortical ring sign view averaged less than 5 minutes to localize.
Conclusion
When using the coracoid cortical ring sign to target a coracoclavicular screw, the procedure is rapid, minimally invasive, and clinically predictable. There is, however, a high rate of screw loosening and subluxation.
Introduction
The coracoid cortical ring sign is an easily reproducible radio-graphical view that allows consistent targeting of the coracoid base. This image is obtained by directing the X-ray beam perpendicular to the medial border of the scapula in the parasagittal plane and approximately 45° off the axis of the scapular spine in the axial plane (Figs 1 and 2). In a previous radiographical and cadaveric study, we analyzed this technique and showed it to be a reliable and safe way to target fixation from the clavicle to the coracoid base (Figs 1 and 2) [1]. We also briefly discussed acromioclavicular separation; a review that is summarized below. As a companion to that study, we present our clinical experience, using the coracoid cortical ring sign to target coracoclavicular screw placement.
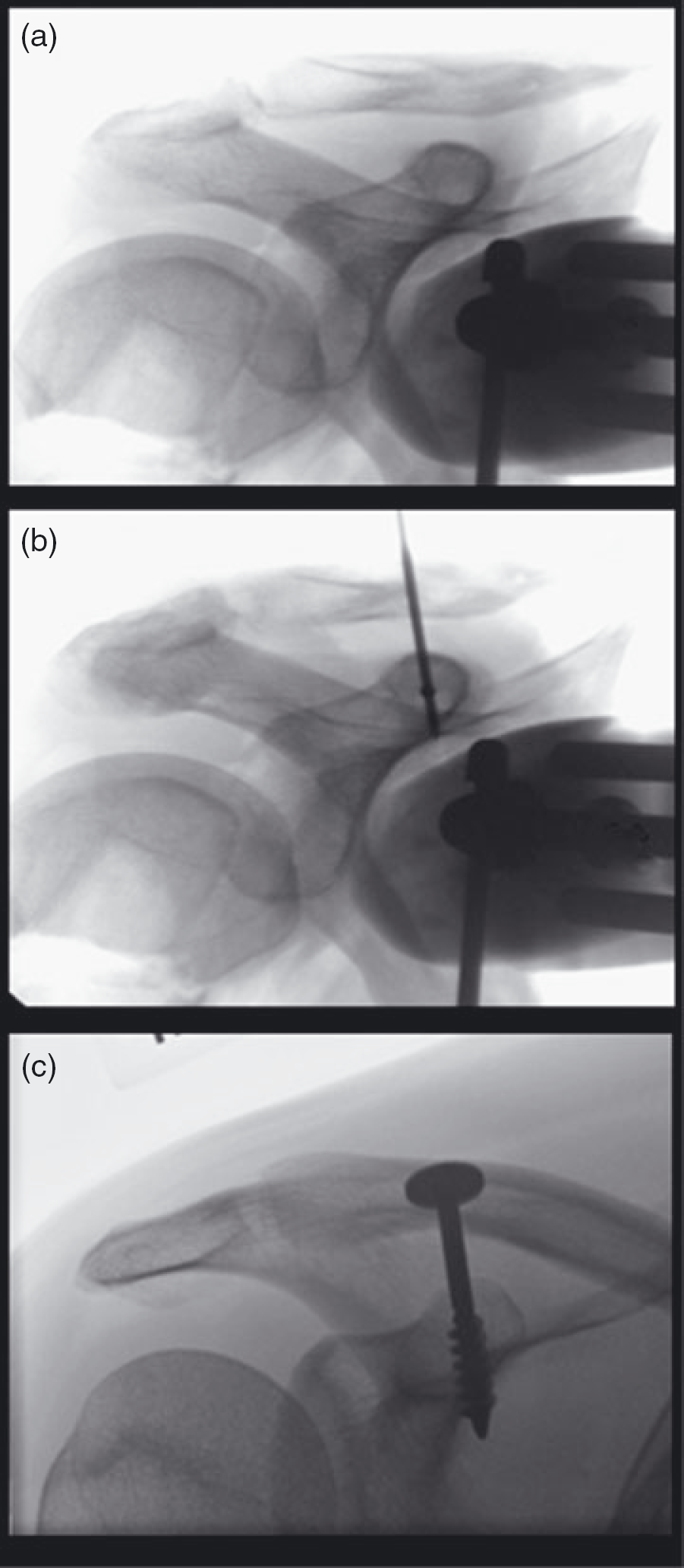
(a) An example of the coracoid cortical ring sign in a cadaveric shoulder found by directing the X-ray beam perpendicular to the medial border of the scapula in the parasagittal plane and approximately 45° off the axis of the scapular spine in the axial plane. (b) Proper coracoclavicular (CC) fixation trajectory through the centre of the ring will result in fixation in the centre of the coracoid base. (c) An anteroposterior radiograph of a clinical case showing a CC screw placed with this method.
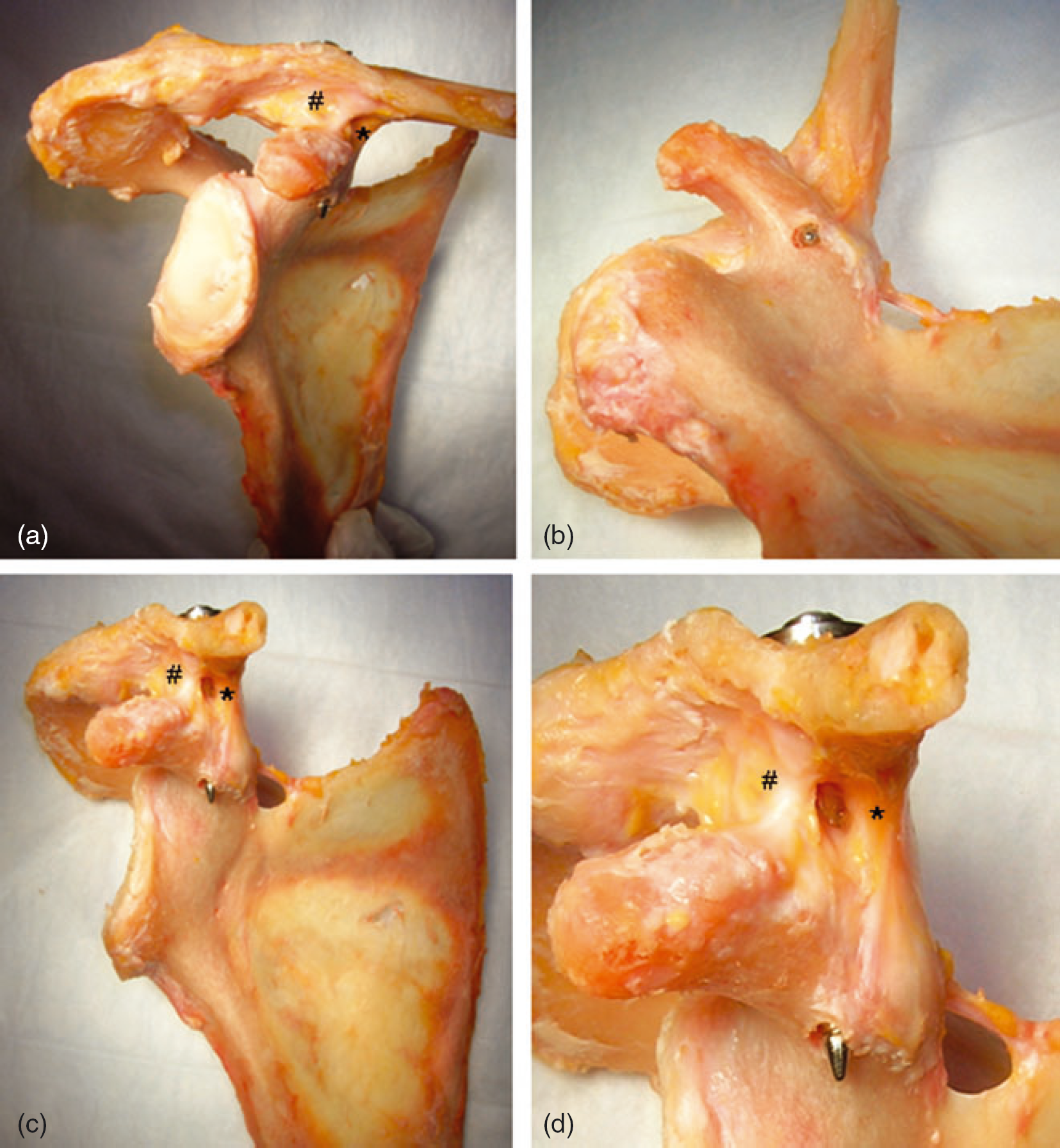
A cadaveric dissection after percutaneous screw placement using the cortical ring sign. (a) The approximate orientation of the cortical ring sign view. (b) Note the screw placement in the centre of the mass of the coracoid base, (c, d) between the coracoclavicular ligaments, conoid (*) and trapezoid (#).
The acromioclavicular (AC) articulation is a small, superficially located joint that plays an important role in the suspension and function of the upper limb, although it is susceptible to frequent traumatic events [2]–[4]. The joint is held in place by the AC capsular ligaments and the stout coracoclavicular (CC) ligaments: the conoid and trapezoid [5].
Acromioclavicular separations are commonly graded according to the classification system of Allman and Tossy, as modified by Rockwood and Young [6]–[9]. Type I and type II injuries are generally considered as stable patterns, and are treated well without surgical intervention. Types IV through type VI separations are characterized by complete dislocation of the AC joint with disruption of the AC and CC ligaments and injury to the deltotrapezial fascia. Type III separations similarly disrupt the AC and CC ligaments, although they do not violate the deltotrapezial fascia. There continues to be debate regarding surgical versus nonsurgical treatment of type III injuries [4], [10]–[13]. However, for type IV injuries and above, the advantage of surgical treatment over non-operative care has been clearly demonstrated [4], [14]–[16].
Numerous operative strategies for severe (types IV to VI) AC injury have been described in the literature. Disruption of the coracoclavicular ligaments is the critical part of the pathogenesis and, consequently, most techniques focus on the repair, reconstruction or reapproximation of the conoid and trapezoid ligaments [4], [7], [17]–[19].
Although the coracoid cortical ring sign view can be used to target the coracoid base with any fixation, in the present study we analyze the clinical results with CC screw fixation. CC screw placement, originally described by Bosworth, is one such method designed to hold the distal clavicle in position with respect to the acromion and the coracoid until the damaged ligaments or graft can maintain the reduction [2]. CC screw placement is amenable to a percutaneous technique; however, difficulties visualizing and interpreting the complicated three-dimensional anatomy of the coracoid have led to a large number of technical failures (32%) using a percutaneous technique [20]. The present study aimed to describe the clinical outcomes of patients with acute AC separations treated with percutaneous CC screw fixation using the fluoroscopic guidance of the cortical ring sign. Although CC screws are certainly not without complications (screw backout, screw breakage, clavicle fracture, and the need for hardware removal) [10], we hypothesize that using the coracoid cortical ring sign will yield more satisfactory results, even with a percutaneous technique.
Materials and Methods
Institutional review board approval was obtained before initiating this study. A retrospective review of all CC screws (Rockwood Screw, DePuy, Warsaw, IN, USA) placed between 1 January 1998 and 1 May 2008 was undertaken using a Current Procedural Terminology code database. Ninety-eight patients were identified in this search. Only the 41 patients with CC screws placed for acute AC separations with minimum 3-month follow-up were carried forward, whereas CC screws placed for other indications (e.g. distal clavicle fracture, chronic AC separation as part of a modified Weaver–Dunn reconstruction) or AC separations treated with other techniques were excluded.
In addition to grade IV and V injuries, only grade III injuries with a cross-over on the adduction view, indicating a significant degree of mediolateral instability, were included (Fig. 3e, f) [21], [22]. We have found that patients with an instability that allows the acromion to scissor under the clavicle tend to remain symptomatic, resistant to non-operative treatment. Grades I and II injuries, in addition to grade III injuries with a stable cross-body adduction view were all treated non-operatively and are not included here.
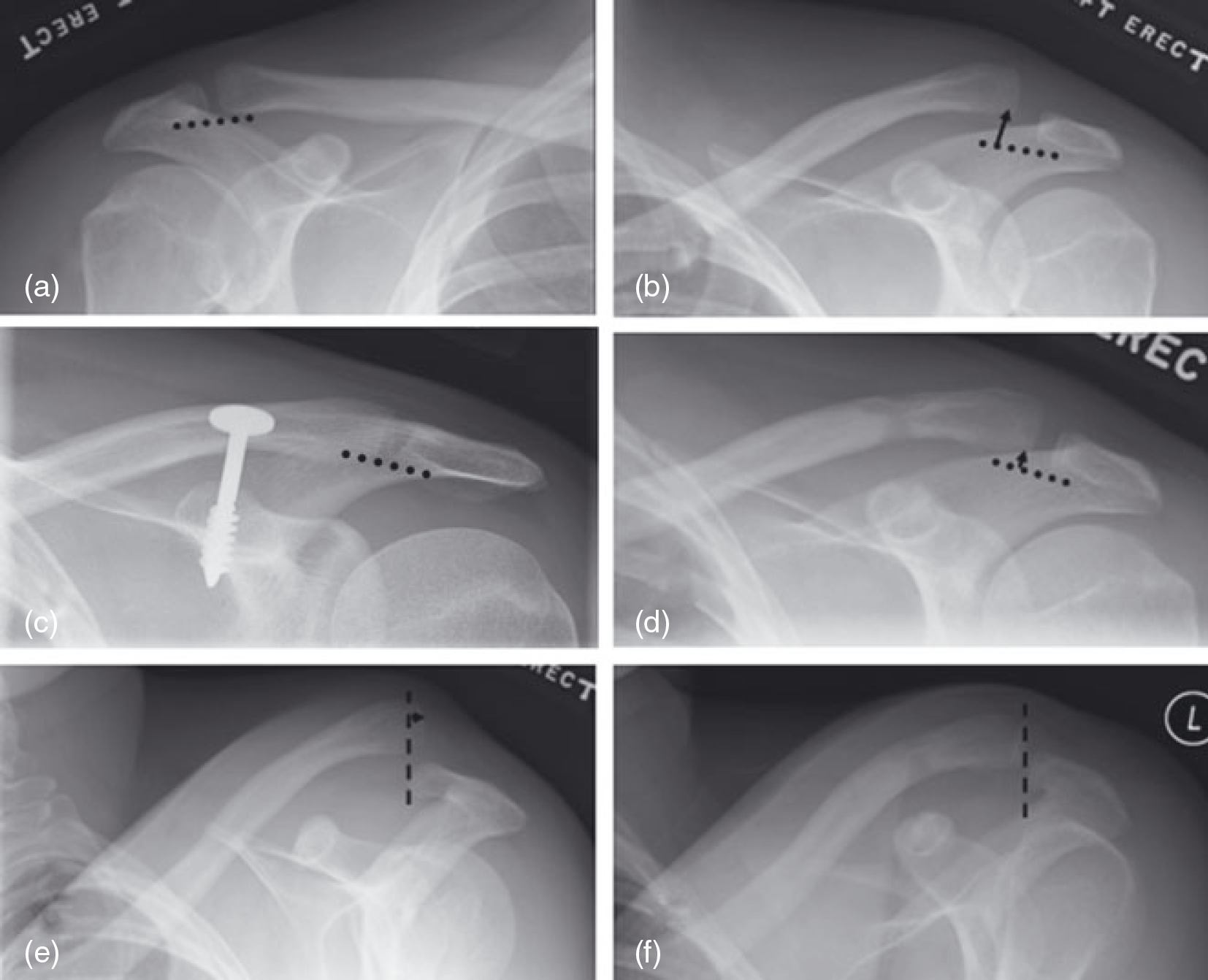
An illustrative example. (a) Anteroposterior radiograph of uninjured shoulder for comparison showing no acromioclavicular (AC) displacement. (b) AP radiograph of injured shoulder showing approximately 80% displacement on unstressed view, type III AC separation. (c) AP view showing reduced, or even slightly over-reduced, AC joint with coracoclavicular screw in place, symmetric with uninjured side. (d) Mild loss of reduction after screw removal. (e) Overlap of the lateral clavicle with cross-body adduction indicates instability pre-operatively. (f) AC joint stable on cross-body adduction view after screw removal.
Medical records were reviewed to collect demographic and injury-related data, including age at injury, injury side, handedness, gender, mechanism of injury, pre-operative symptoms, duration of screw fixation, length of follow-up, range of motion, pain, and any complications. These data were used to rate each patient outcome according to the Acomioclavicular Rating Scale, which is a modification of the UCLA rating scale [17]. Records from the anaesthesia database were analyzed to calculate the time for positioning and obtaining the cortical ring sign (patient in room to start of procedure time), surgical time, and estimated blood loss. Serial radiographs were reviewed by three blinded examiners to measure AC instability (overlap) on cross-body adduction views and percentage AC displacement pre-operatively, with screw in place, and at each visit after screw removal.
Surgical technique: acute AC separation
All surgeries were performed by two fellowship trained shoulder surgeons at two tertiary care centres using the same technique. Patients were placed in the beach chair position with the c-arm fluoroscopy arched over the operative shoulder. The coracoid cortical ring sign was identified by first directing the X-ray beam perpendicular to the medial border of the scapula in the parasagittal plane and 45° off the axis of the scapular spine in the axial plane, then fine-tuning until the coracoid cortical ring was evident (Fig. 1) [1]. The limb was then prepped and draped, with the C-arm draped into the field.
A 2 cm to 3 cm incision is generally made 2 cm to 3 cm medial to the lateral end of the clavicle. A sharp dissection is taken through the skin on the superior aspect of the distal clavicle, through the trapezius fascia in line with its fibres, and onto the distal clavicle. In some cases, the full thickness skin flap was undermined 2 cm laterally to the AC joint so that the exact anatomic reduction could be verified. The skin over this portion of the shoulder is quite mobile and, by undermining skin flaps, we were able to identify and later close defects in the deltotrapezial fascia in the case of grade IV separations. The decision regarding open versus closed reduction was made intra-operatively. In most cases, the AC joint reduced with gentle manipulation. In the rare cases where the AC joint was irreducible, a small (2 cm) incision was made over the acromioclavicular joint to facilitate reduction. The AC joint was reduced with a combination of downward and anterior pressure on the clavicle during which an assistant translated the arm and scapula superiorly.
At this time, a CC lag screw (Rockwood Screw) was placed in the standard fashion, with guidance provided by targeting the drill into the centre of the coracoid cortical ring and thus the centre of the coracoid base (Figs 1 and 2). The AC joint was reduced to the point of reduction, or slight over-reduction. A layered closure was performed with care given to closure of the deltotrapezial fascia, using braided, resorbable, interrupted suture. Postoperatively, the patient was placed into a sling for a period of 3 weeks, to allow early healing of the coracoclavicular and acromioclavicular ligaments. At 3 weeks postoperatively, the patient is allowed unrestricted shoulder motion but is limited to lifting 5 lbs (2.27 kg) with the operative extremity. It has been our experience that a full range of motion is obtained once the screw is removed.
After 8 weeks to 12 weeks, the screw is removed using the same incision and unrestricted motion is encouraged. Aggressive strengthening was not allowed for another 6 weeks to 8 weeks. Return to athletics was predicated on full return of range of motion and strength (usually 4 months from the initial screw insertion).
Results
The overall study population had a mean age of 35 years (range 18 years to 78 years) and all of the patients were male. The dominant arm was injured approximately two-thirds of the time. Motor vehicle, motorcycle and bicycle accidents were the most common mechanism of injury, followed by contact sports. The distribution of injuries was 14 grade III, 10 grade IV and 17 grade V. All patients were unstable on cross-body adduction views, showing the clavicle over-riding the acromion (intra- and interobserver agreement, 100%) (Fig. 3). Screws were left in place for an average of 2.8 months (range 2 months to 5 months) and patients were followed up for an average of an additional 4.7 months (range 3 months to 2 years).
There were six episodes of screw loosening (15%), with three of six requiring an additional surgical procedure to re-tighten the screw. Two patients had been noncompliant and started heavy lifting (suit-cases and weight-training) in the first week postoperatively, one screw dislodged during a seizure, and one screw was displaced when a patient was tackled by the police. Two screws backed out for unknown reasons in patients that were apparently compliant with the postoperative protocol.
All patients had full range of motion at final follow-up. No patients required chronic narcotic pain medications; however, five of 41 had continued occasional mild discomfort during activity and two of 41 had continued, noticeable pain requiring occasional nonsteroidal anti-inflammatory analgesics. One patient had skin sensitivity, likely a result of irritation of a supraclavicular nerve that was relieved with temporary use of lidoderm patches (Lidocaine patch 5%; Endo Pharmaceuticals, Chadd Ford, PA, USA). Employing the modified UCLA rating scale/acromioclavicular rating scale of Guy et al. [17], 98% (41/41) of the cases were judged to be ‘Good’ or ‘Excellent’ results.
Set-up time including positioning, prepping, draping and the time to position the C-arm took an average of 17 minutes (range 9 minutes to 26 minutes) for screw insertion cases and 12 minutes (range 6 minutes to 20 minutes) for screw removal. This difference of only 5 minutes suggests that only a few minutes were needed to position the fluoroscopy unit, find the coracoid cortical ring sign, and drape it into the field. Operative time took an average of 35 minutes (range 28 minutes to 40 minutes). The screw removal procedure took approximately 24 minutes (range 18 minutes to 30 minutes). Blood loss was estimated at 15 mL (range 5 mL to 100 mL) for the insertion procedure and 7 mL (range 5 mL to 25 mL) for the removal.
Injury films showed an average displacement of 121%, which dropped to 24% after the first postoperative visit with the screw in place (Fig. 4). The average change in the percent AC displacement was statistically significant when injury films were compared with postoperative films with the screw in place (p < 1 × 10−6) and when the injury films were compared to the final films (p < 0.01). Displacement was recorded at each visit after screw removal, increasing to 52% and then to 64%, but dropping to 43% at the final follow-up at least 3 months later. Once the screw was removed, none of the changes in the reduction of the AC joint between screw removal and final follow-up were statistically significant (p = 0.08). Intraclass correlations were computed to assess intra- and inter-rater agreement, which were both excellent (0.98; 95% confidence interval, 0.97 to 0.99). No patients had residual instability on cross-body adduction.
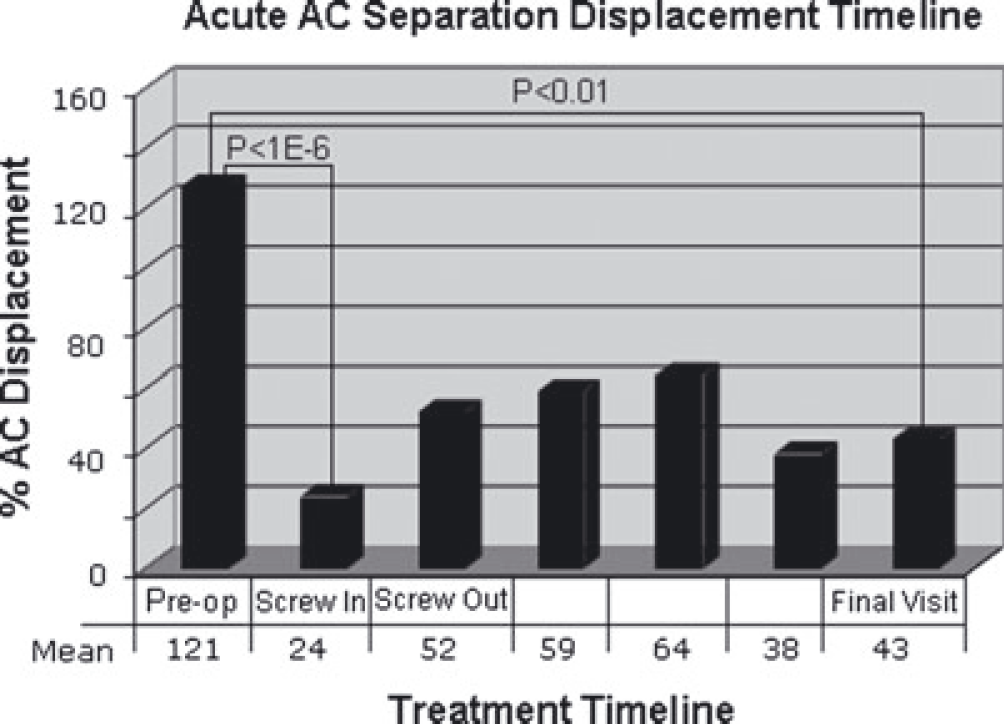
Average percent displacement (normalized to the joint height) of the acromioclavicular (AC) joint over time. Note the statistically significant reduction with screw in place, the nonstatistically significant loss of reduction after screw removal, and the position at final follow-up.
Discussion
The CC screw, described initially by Bosworth, allows for fixation of the clavicle in relation to the scapula. Based on the principles of rigid fixation and ligament healing, the CC screw has been used in isolation as a fixation device for acute separations [2], [20], as an augmentation for stability after suture reconstruction or chronic repair of the CC ligaments, and as an augmentation after ligament reconstruction [17], [18], [23].
Bosworth demonstrated that placement of a CC screw could be performed through a limited open or percutaneous technique. However, difficulties visualizing and interpreting the complicated three-dimensional anatomy of the coracoid led to a large number of technical failures (32%) using a percutaneous approach [20]. Subsequent reports have utilized the screw through an open approach [17], [18]. A recent cadaveric and radiographical study suggested that a particular fluoroscopic view, the coracoid cortical ring sign, can be used to target fixation into the coracoid base [1]. Using this technique clinically to guide percutaneous CC lag screw fixation, we have ultimately achieved satisfactory results in all patients with no hardware malposition, but with a 15% loosening rate and a 7% hardware revision rate to re-tighten unacceptably loose screws.
In 1941, Bosworth's original technique description involved blind, percutaneous screw placement through a 3/4 inch incision. The borders of the coracoid were palpated through the clavicular drill hole with a long needle or the drill tip to help guide the screw into the coracoid base [2]. The enthusiasm for the blind procedure was dampened by the uncertainty of screw fixation [20]. In 1989, Tsou published a series of 53 patients with acute AC separation treated with his method of fluoroscopically-guided CC screw placement using a cannulated screw. Although his report included a number of technical advancements, there were a large number of type III separations (40/53) and a technical failure rate of 32%. Although Tsou attributed this to the learning curve of his technique, seven out of 11 technical failures were a result of screw pull-out and two of 11 needed to be converted to open screw placement [20]. Screw placement guided into the coracoid base using the cortical ring sign in the present study resulted in six out of 41 episodes of partial screw pull-out and no conversions to open placements in a series with higher grade displacements.
In Rockwood grade I and II AC separations, the intact CC ligaments are felt to hold the joint in a stable position, allowing healing and preventing instability. These injuries have consistently good results with non-operative treatment. Historically, nonoperative management of higher grade injuries with more displacement included the Kenny–Howard brace and other similar devices designed to depress the distal clavicle and elevate the acromion [2], [16]. These braces are generally painful and required continuous wear, leading to frequent problems with skin irritation and loss of reduction [16]. Currently, the trend in non-operative treatment is to accept the deformity and treat the patient initially in a sling followed by supervised physical therapy to regain function.
Operative management includes a variety of surgical options. For acute AC separations, the healing potential of the torn CC ligaments is felt to be adequate if they are held in anatomic approximation for sufficient time. Fixation of the acromioclavicular joint using pins or bioabsorable materials has also been advocated. This technique suffers from a steep learning curve, loss of fixation, pin breakage, pin migration, and further insult to the AC joint articular surfaces and AC joint meniscus [16]. A hook plate, designed to hold the CC ligaments in approximation with a plate placed on the superior surface of the distal clavicle that hooks over the end of the clavicle and under the medial acromion, has been reported with satisfactory outcomes, although it runs the risk of rotator cuff irritation and subacromial impingement, as well as potential damage to the AC joint surfaces [3].
Multiple biomechanical studies have shown properly placed CC screws to be stiffer and stronger than other constructs, including a CC sling, hook plate, CA ligament transfer or suture anchors [3], [24]–[26], although good clinical results have been achieved with a variety of constructs. Similar to other AC separation fixation techniques, the CC screw is not without drawbacks. A second procedure for removal is required, although we have found the entire screw extraction takes less than 25 minutes, can be done with local anaesthetic and light sedation, and only loses 7 mL of blood. Screw malposition, injury to neurovascular structures, and fracture of the coracoid tip were not seen in the present study, perhaps because screw placement in the centre of the coracoid base, as targeted by the cortical ring sign, guards against these complications. Targeting the centre of the base with bicortical coracoid screw purchase has been shown to be far superior than unicortical screw placement [25], [27].
However, screw loosening, seen in six of 41 cases, appears to be a risk even with proper screw position. Although four of these patients had a postoperative event that may have put undo strain on the screw, two patients had screw loosening after apparent compliance with the postoperative restrictions. In cases of screw loosening, the residual displacement was evaluated to determine whether the displacement was minimal enough that the CC ligaments might still be in approximation (grade I or II); otherwise, surgery was offered to tighten the screw. The weight of the entire forequarter acts against the inclined plane of the screw threads and, clearly, the friction of the screw bite is not always sufficient for secure fixation for the entire 3 months. Interestingly, screw back-out, as seen in the present study, has been noted as the primary mode of failure in both biomechanical studies [24], [27], [28] and clinical studies [22], [29]. We did not encounter screw breakage, a problem with earlier constructs using weaker screws such as 3.5-mm cannulated screws [17] compared with the more modern 6.3-mm Bosworth Screw (Stryker Howmedica Osteonics, Allendale, NJ, USA) [28], the 6.4-mm Rockwood Screw (DePuy) [26] or a custom made 7.0-mm cannulated CC screw [20]. On average, the shape of the radiographical displacement curve showed considerable displacement initially, a reduced state with the screw in place, then an increase in displacement after screw removal that did not reach statistical significance.
The main limitation of the present study is the short follow-up (approximately 3 months with the screw in place, then an additional 5 months after screw removal). The leveling of the radiographical results over time suggest that the outcome is not likely to deteriorate with longer follow-up and, for this reason, we do not routinely follow patients for more than 3–6 months after screw removal. The patients with longer follow-up corroborate the findings, with durable results at 2 years. However, although the clinical and radiographical follow-up would indicate most patients are on the road to success, we recognize that caution must be exercised in interpreting studies with short-term data.
Conclusions
The coracoid cortical ring sign can be used to target percutaneous coracoclavicular fixation reliably and safely in the coracoid base. We have used this view to target coracoclavicular screw fixation for the treatment of acute acromioclavicular separations with satisfactory clinical results. As seen in other series and with biomechanical testing, screw loosening was the most common complication. At final follow-up, the average patient's AC joint was left with 43% subluxation, no instability to cross-body adduction, minimal symptoms and a satisfactory outcome.
Footnotes
Conflicts of Interest
None declared