
Abstract
The incidence of deep wound infection following rotator cuff repair is rare, although it can cause significant problems with respect to diagnosis and treatment. Sub-optimal management may result in the loss of the chondral surfaces, the rotator cuff and the deltoid musculature, and also result in septic arthritis of the glenohumeral joint. This review presents data from 10,457 rotator cuff repairs with 92 confirmed deep wound infections. It discusses the rate and presentation of infections, as well as the bacteria involved and the treatment used. From this, a set of principles to guide best practice is proposed.
Introduction
The incidence of deep wound infection following rotator cuff repair is rare, although it can cause significant problems with respect to diagnosis and treatment. Sub-optimal management may result in the loss of the chondral surfaces, the rotator cuff and the deltoid musculature, and also result in septic arthritis of the glenohumeral joint. This review presents the data from the literature and proposes a protocol to manage infections post-rotator cuff repairs.
Materials and Methods
A systematic review of the literature was performed using the Medline (NCBI) and the Embase (Ovid) database using the keywords: ‘rotator cuff’ AND ‘pyogenic’ OR ‘Septic’ or ‘Sepsis’ OR ‘infected’ OR ‘infective’ OR ‘complications’. Abstracts were then reviewed to identify publications presenting data on the diagnosis and management of deep infections after rotator cuff repair. The definition of a deep infection for the present study is one that requires surgical intervention and has had deep wound samples sent for culture. The references of all relevant articles were cross-referenced to search for further relevant articles. A meta-analysis of the data was then performed.
Results
Seven papers were identified and reviewed in full [1]–[7]. In total, 92 cases of deep infections following rotator cuff repair were available for analysis.
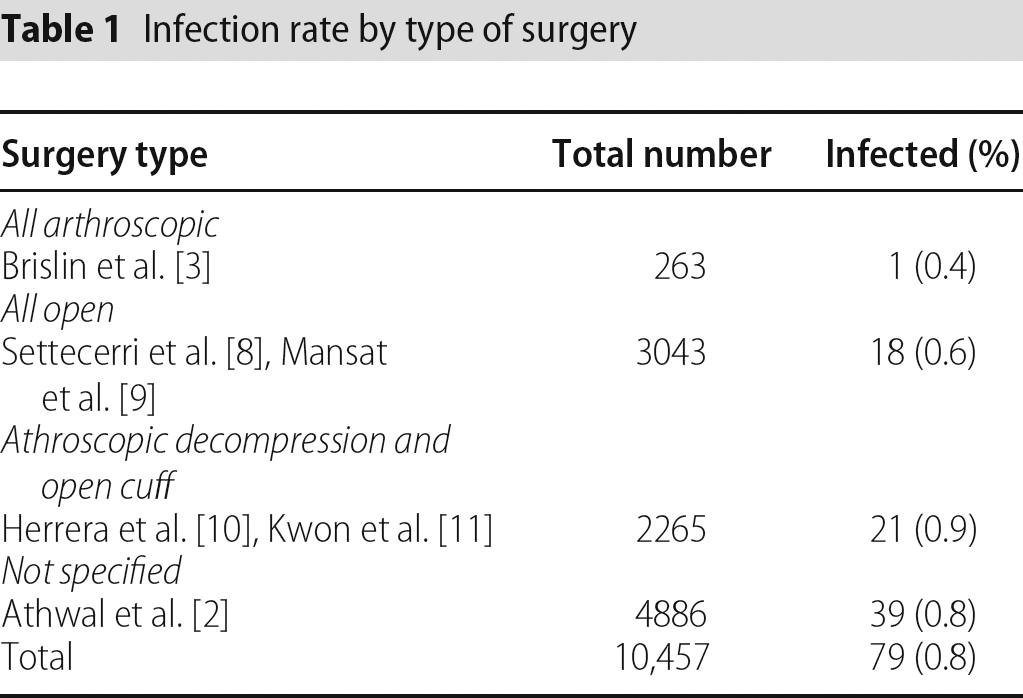
The infection rate for an all arthroscopic technique is compared with an all open technique and a combined technique of arthroscopic decompression with open rotator cuff repair (Table 1). One paper [6] did not identify what technique was used and is excluded from Table 1.
Infection rate by type of surgery
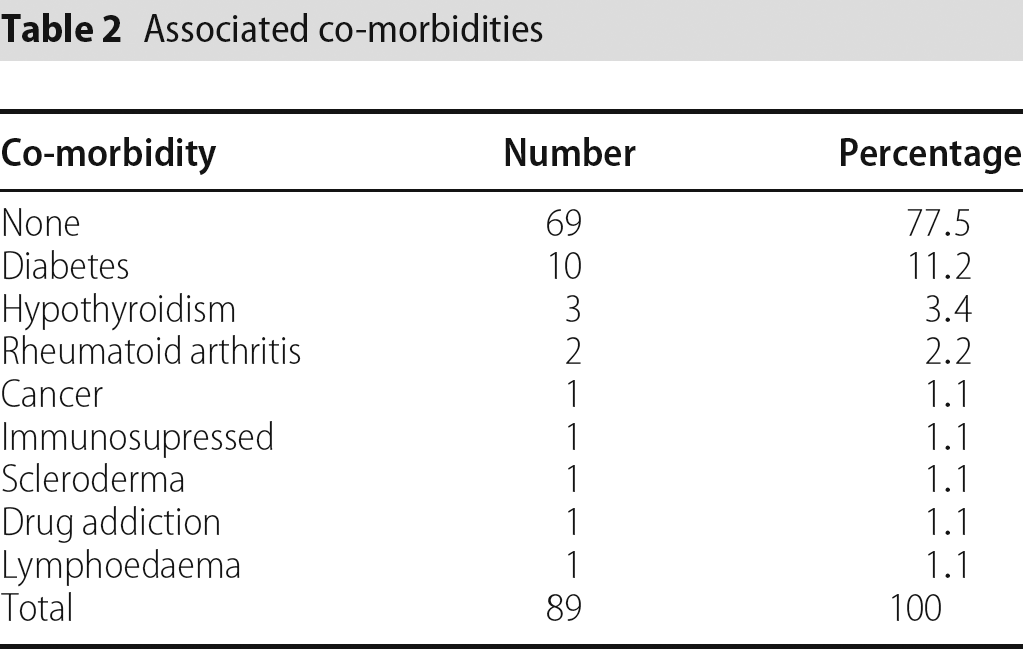
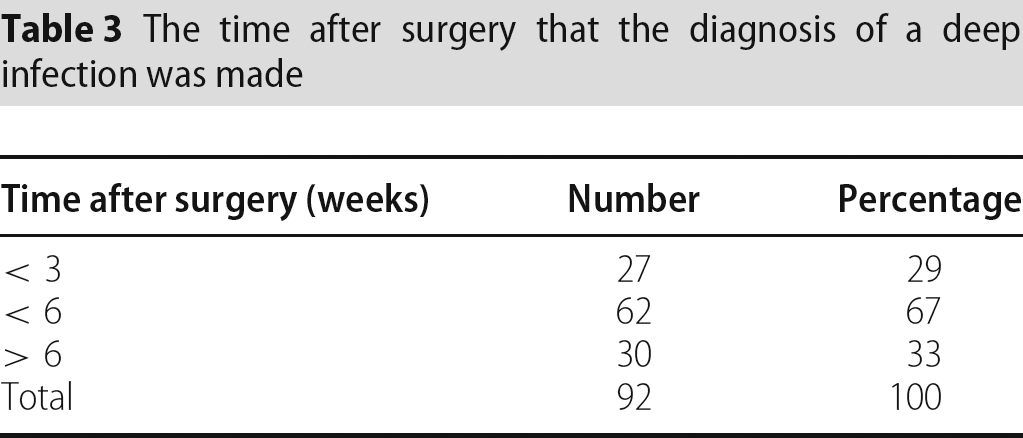
The associated co-morbidities (Table 2) and the time after surgery that the diagnosis of a deep infection was made (Table 3) are presented.
Associated co-morbidities
The time after surgery that the diagnosis of a deep infection was made
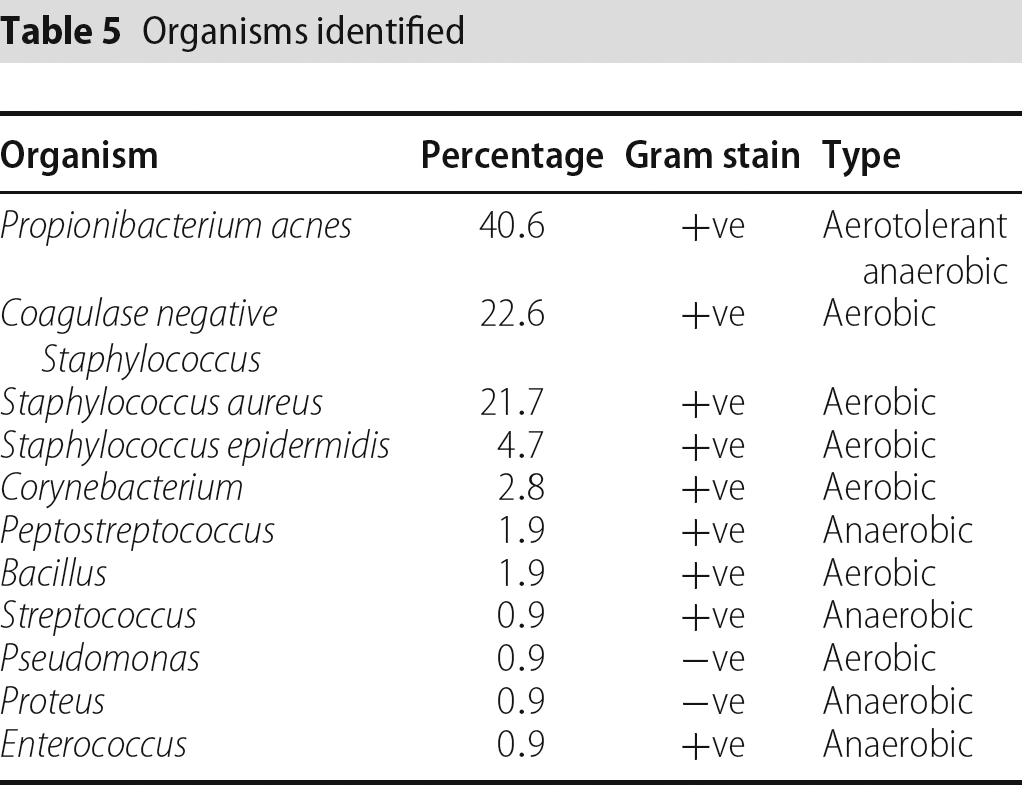
The clinical symptoms and inflammatory markers are shown in Table 4. The organisms identified are presented in Table 5. Some patients grew more than one organism; thus, in total, 106 organisms were identified.
Inflammatory markers and clinical presentation at diagnosis

Organisms identified
The management protocols used are presented in Table 6. One paper [6] that involved chronic infections (presenting greater than 6 weeks after operation) is not included.
Treatments prescribed
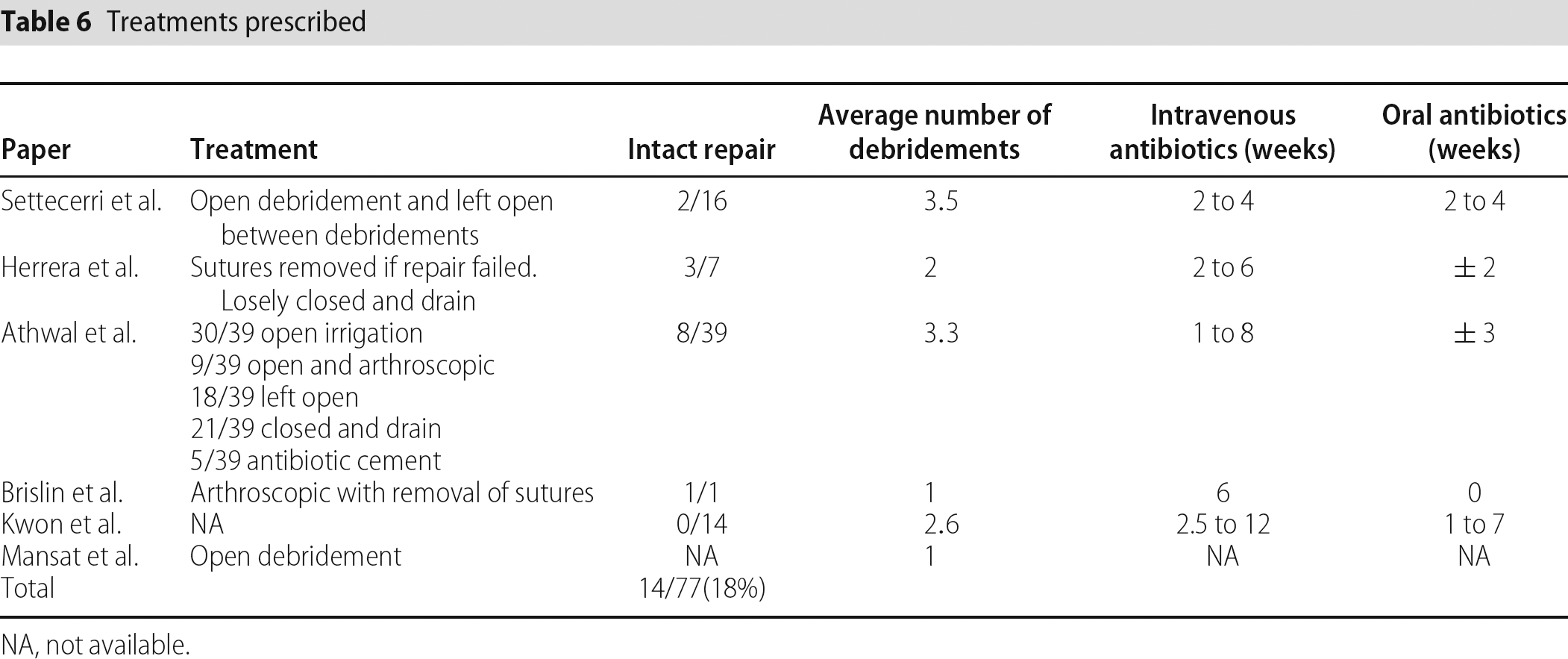
NA, not available.
The deltoid muscles was not repairable in 33 cases (62%) out of 53 cases where its condition at final debridement was recorded [1], [4].
Discussion
This review of the literature demonstrates that little is known about the management of deep infections after rotator cuff repairs. This is partly a result of the rarity of the condition and the likely under-reporting of complications following surgery. One study specifically examined patients with chronic infections [6]. This group of patients has a poor prognosis, with extensive salvage surgery being required to obtain any function. The aim of our review was to attempt to define the best management of deep infections and avoid the consequences of delayed and sub-optimal treatment.
The overall deep infection rate from the 10,457 rotator cuff repairs included in the study is 0.8% and compares favourably to an infection rate of 0.14% to 1.7% [10], [12]–[14] for anterior cruciate ligament reconstructions and a infection rate of 1.8% following primary shoulder arthroplasty [15]. There appears to be little difference in the infection rates for the different techniques used. However, one study [3] with the highest infection rate (1.9%) used a combined surgical technique (arthroscopic subacromial decompression and open cuff repair) and suggested that the fluid extravasations during arthroscopy may decrease the efficacy of pre-operative skin preparation [3]. They advised repeat skin preparation and draping after arthroscopy and prior to the open incision. They reported no further cases of infection using this protocol in 200 cases. Increased infection rates after knee arthroscopy have been related to prolonged operating time, multiple procedures and previous steroid injections [11]. Co-morbidities will also affect infection rates and the rate of deep infection after open rotator cuff repair in insulin-dependent diabetics has been documented as 6.6% [16]. However, the vast majority of patients presented in this cohort did not have underlying medical conditions.
Of the patients presented, approximately one-third presented before 3 weeks, two-thirds before 6 weeks and the remaining third after 6 weeks. There was only one (1.6%) possible case of osteomyelitis reported for patients presenting before 6 weeks, although the exact time postoperatively that this patient presented is not documented [1]. This compares to 11 (84.6%) cases of osteomyelitis of the humeral head or clavicle for chronic infections (at least 12 weeks post-surgery) [6].
Clinical presentation cannot be relied on for diagnosis of deep shoulder infections and inflammatory markers cannot be relied on to rule out deep shoulder infections. In a review of 89 cases of large joint septic arthritis (knee, shoulder and ankle), C-reactive protein (CRP) was raised in 95% of patients when positive cultures were found and in only 65% of patients when cultures were negative [9]. In that study, the shoulder had the biggest delay between diagnoses after surgery compared to knee and ankle infections.
None of the cases in this cohort used frozen section in the diagnosis of infection. Frozen section has been used in infected failed rotator cuff repairs, at the time of surgery to decide whether to proceed to a one-stage reverse arthroplasty or a two-stage arthroplasty [17]. It has been shown to have a good ability to rule-in an infection, although a poor ability to rule-out an infection following hip and knee arthroplasty [18]. This would suggest it could be a useful tool in chronic low grade infection, rather than an acute postoperative infection.
The most common organism isolated is Propionibacterium acnes, although almost half of the cases are related to Staphylococcus infection. Staphylococcus infection in primary shoulder sepsis (with no previous surgical intervention or needle insertion) and secondary to all causes is similar, but only 0% to 5% of cases are related to P. acnes [8], [19]. This difference in prevalence of P. acnes demonstrated between postoperative patients and native shoulder sepsis could be a result of poor detection because it can take up to 15 days to grow in enriched broth [20]. It has also been argued that it is a contaminant [20] or it could be a true pathogen introduced from surgical intervention.
P. acnes is a non spore-forming anaerobic commensal bacillus of the sebum rich hair follicles of the skin. It has low virulence and can be difficult to diagnose in patients with no fever, normal blood tests and no local inflammation. A study of 50 patients with P. acnes infected prosthetic joint replacements (hip, knee shoulder) demonstrated that only 38% had signs of fever and only 16% had local inflammation [20]. The erythrocyte sedimentation rate in patients with P. acnes infected prosthetic joint replacements was raised above 30 mm in only 34% to 36% of cases and C-reactive protein was raised above 10 mg/L in 32% to 64% of cases [20], [21].
P. acnes has been found to be more prevalent over the shoulder than the knee or hip and men have a significantly greater prevalence over the shoulder than women. However, the bacterial burden of P. acnes was not significantly different to Staphlococcus over the shoulder [22].
It is known to be resistant to metronidazole and sensitive to penicillin and clindamycin [21].
The treatments used for confirmed deep infections vary considerably with the open, arthroscopic and combined debridements presented. There does not appear to be a consensus for the duration of intravenous and oral antibiotics. Outcomes following these regimes are difficult to assess. Only 18% of repairs were intact following infection and all of the studies attempted re-repair if possible at the last debridement.
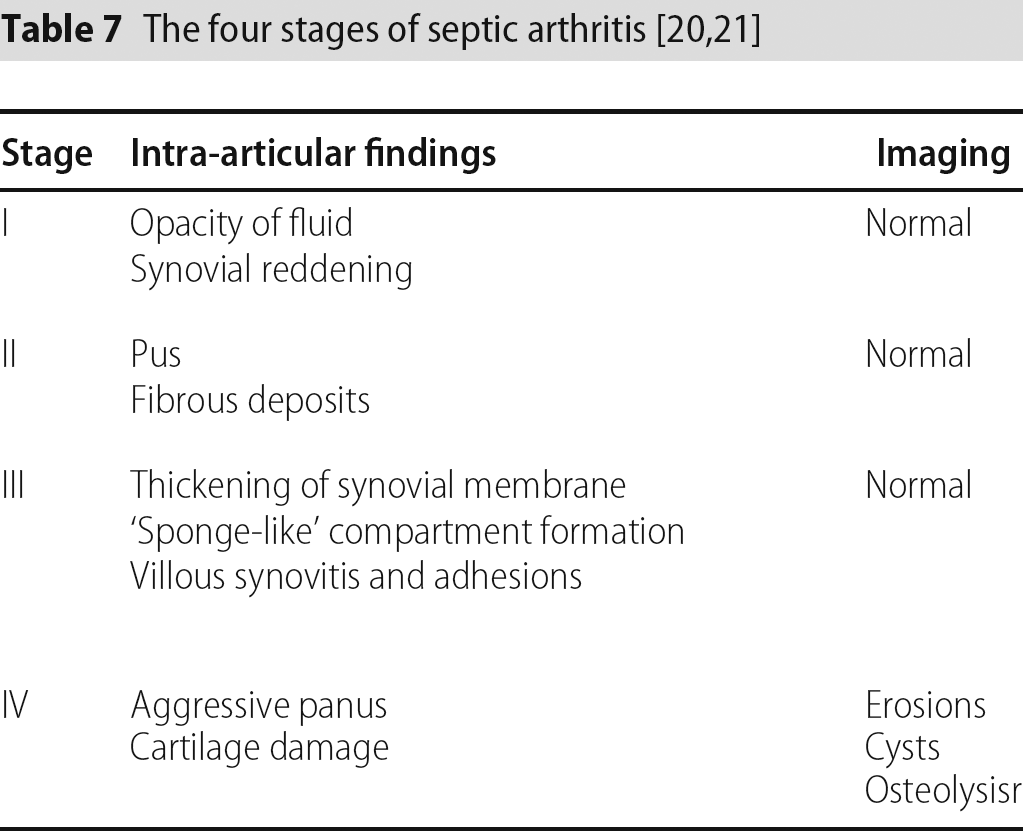
Septic arthritis of large joints has been staged into four stages [9], [23] and is summarized in Table 7. Some studies have suggested that cases of stage III septic arthritis or greater present only after 3 weeks of symptoms [9]. Arthroscopic debridement in large joint septic arthritis has shown a successful rate of 91% (95% stage I and II, 67% stage III) and only one patient out of 10 required removal of metalwork [23]. The authors performed open washout of stage IV cases and stated that arthroscopic debridement is not successful in stage IV. Retention of suture material after rotator cuff repairs in one study did not appear to affect outcome [4] and it has been suggestion that sutures may be left in situ if the organism grown is P. acnes [3].
Arthroscopic management of native septic arthritis (non-operative cases) of the glenohumeral joint showed eradication of infection with one debridements in 14 out of 19 patients [24]. The remaining five patients requiring more than one debridement had bone and cartilage erosion on a magnetic resonance imaging (MRI) scan, which would be staged as stage IV. They performed debridement of both the subacromial space and glenohumeral joint with a shaver and lavage of at least 5 L of saline. It is argued that a synovectomy during debridement should be avoided if possible to preserve a barrier against migration of the microorganism [23].
This suggests that arthroscopic debridement has a good chance of irradiating infection if treated early and this would avoid the concern of an irreparable deltoid after repetitive open debridement. This occurred in almost two-thirds of the cases presented in our review. The loss of deltoid and the rotator cuff will result in significant functional impairment and limits future treatment options.
Although the literature is limited, we propose some recommendations that may aid to reduce the risk of postoperative infection:
Prophylactic antibiotic use that covers Staphylococcus and P. acnes.
Repeat skin preparation and draping after arthroscopic intervention and before open procedures.
Avoidance of prolonged operating time.
Avoidance of excessive steroid injections prior to surgery.
To diagnose an infection postoperatively, a high index of suspicion is required. Clinical signs and raised inflammatory markers are highly indicative, if present, but cannot be relied upon to rule out infection. Normal inflammatory markers may indicate P. acnes infection. Aspiration should be performed early in a theatre setting with the provision to proceed to an arthroscopic washout if the aspirate is suggestive of infection.
Arthroscopic washout should enter both the subacromial space and glenohumeral joint. Three deep tissue samples should be taken from both spaces and sent for microbiology with a specific request for P. acnes culture. Debridement with the shaver should be performed in both spaces with at least 5 L of saline. Debridement should include redundant suture material, although sutures may be left in situ if still forming part of a viable repair in early infection (grades I to III). After debridement, antibiotics should be commenced to cover Staphylococcus and P. acnes until definitive microbiology results are available. An MRI scan should be requested to exclude bony changes.
Reasonable indications for open debridement would be:
Cartilage damage seen on initial arthroscopic debridement (grade IV).
Bony changes seen on MRI scan (grade IV).
Failure to resolve the infection after two arthroscopic debridements.
Open debridement in these situations should include removal of all suture material and suture anchors.
It would also appear appropriate to continue with antibiotics until the inflammatory markers have returned to normal in those cases that initially had raised markers.
In summary, this present review has highlighted what can be gained from the literature with respect to the detection and management of deep wound infections after rotator cuff surgery. Based on this evidence, a set of principles to guide best practice have been proposed.