
Abstract
Background
Radiofrequency (RF) devices are widely used in arthroscopic shoulder surgery for tissue ablation and other effects. They have heating effect during tissue application. It is known that chondrocyte death occurs with temperatures above 45 °C. The present study aimed to investigate the effect of various factors on the heating effect of RF probes in a controlled in vitro model.
Methods
A perspex model was used, in which volume, flow, outflow position, duration of RF probe use and inflow temperature could be closely controlled.
Results
Temperature rises in the bathing fluid sufficient to cause cell death were seen. The temperature rise was most noticeable when there was no fluid flow through the compartment, at smaller fluid volumes, if the fluid inflow temperature is elevated, and if the outflow is distant from the RF device. Of note, 30 seconds of use in a volume of 20 mL with no flow led to temperatures above 50 °C.
Discussion
Most of the factors affecting temperature rises using RF devices are directly under the surgeon's control. Further work is needed in this area to define the potential clinical effects of the use of these devices.
Introduction
Radiofrequency energy (RFE) devices are routinely used in orthopaedics, particularly during arthroscopic surgery. They may be either monopolar (mRFE) or bipolar (bRFE), and perform functions such as tissue cutting, shrinkage or ablation. In shoulder arthroscopic surgery, much work has previously focussed on the role of these devices in thermal capsulorraphy [1]–[3]. Tissue shrinkage from the effect of RF energy application and their potential use in joint instability were initially met with enthusiasm [4], [5]. This technique, however, requires tissue temperatures above 65 °C to cause significant tissue changes [6]. Of concern is the fact that chondrocyte death has been demonstrated at temperatures above 45 °C [7], [8] and direct application of RFE to articular cartilage has been shown to produce temperatures above 78 °C, even to depths of 2000 μ with bRFE [9]. Additionally, the RF device heats the fluid within the working space, and may therefore have an indirect effect on all tissues exposed to the fluid. Despite initial reports on the safety of thermal capsulorraphy [10], there are clinical reports of severe chondrolysis related to these devices in this setting [11], [12].
Although arthroscopic subacromial decompression (ASD) is now probably the most frequent indication for the use of these devices in shoulder surgery, there is little work on thermal injury to tissues other than articular cartilage. Tissues including the bursal surface of the rotator cuff, the acromion and distal clavicle, the acromio-clavicular joint and the deltoid muscle will all be in contact with the arthroscopic fluid in these procedures. Although acute termal injury to these tissues may not be generally seen, the potential effects on these tissues over the longer term is unknown. Given the possibility of thermal injury to intra-articular structures, recent work has also explored the effect of fluid temperature during arthroscopic use of these devices. In vitro cadaveric and custom-built models [1]–[3], [13] and in vivo patient studies [14] have recently been reported. Only two of these studies, however, have focussed on the subacromial space [13], [14]. The data from these studies has produced confusing results, with some suggesting no evidence of excessive fluid temperature generation [13], [14], and others finding fluid temperatures sufficient to potentially cause cell death [1]–[3]. Additionally, these studies have been inconsistent in both parameters measured and controlled for, and assumptions have been made about the uniformity of fluid flow within the studied space.
In the present study, we have produced a model of the subacromial space in which parameters that might influence temperature generation with the use of a RF device in a closed space could be tightly controlled. We have specifically investigated the effect of cavity volume, fluid flow rate, inflow temperature, and outflow cannula position, as well as the use of a variety of continuous and intermittent RF device modes on fluid temperature. Accordingly, we aimed to produce advice on the safe use of RF devices in an enclosed fluid space, such as during arthroscopic surgery of the subacromial space.
Materials and Methods
An acrylic model (perspex) with a cavity height of 10 mm and an adjustable volume from 10 mL to 60 mL was used to represent the subacromial space. Measurements of the volume of the subacromial space from bursography have been estimated at 10 mL [15], but without the bursal dissection that takes place in arthroscopic subacromial decompression. The soft tissue releases that are performed in this procedure result in an increase in the effective volume of the space. The effective volume of this space in vivo will also increase in the presence of full-thickness cuff tears, and it was for these reasons that we chose to vary the volume between 10 mL and 60 mL.
The model had inflow and outflow portals and allowed the introduction of a RF probe via a standard arthroscopic cannula. The cavity volume of the model was adjustable in 10-mL increments. The cavity was instrumented with thermocouples placed through unused ports and, hence, there were a number of measurement locations for each cavity volume (Fig. 1).
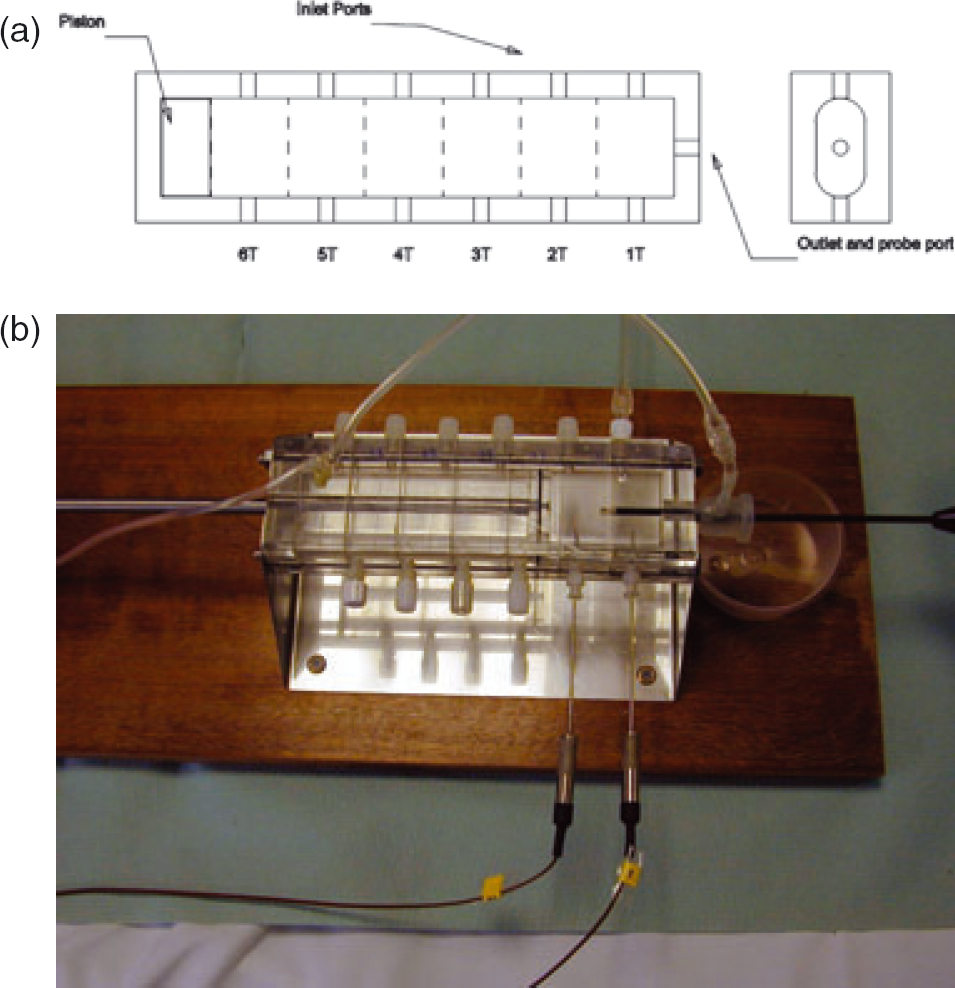
(a) Schematic of experimental model. (b) Photograph of experimental model.
All thermocouples were type copper/constantan and connected to a commercial amplifier/convertor with the temperature data transferred to a personal laptop computer. This was continuously recorded for each experiment. This circuit attenuated the RF and guaranteed a RF interference-induced measurement error of less than 1 °C. The system calibration was verified against an ice bath standard and found to be within 1 °C.
The fluid inflow was either with gravity of different flow rates (no flow, 52, 115, 225 mL/minute) via an arthroscopic fluid pump system (FMS DUO*, DePuy Mitek, Raynham, MA, USA). These flow rates were those in clinical use with this fluid system. The fluid inflow temperature was 22 °C (room temperature) or warmed to 35 °C. Although no suction was used in direct association with the RF probe, the position of the fluid outflow was altered with respect to the cavity volume.
The RF probe was either used continuously for 60 seconds or intermittently for three cycles each of 20 seconds. When the probe was used intermittently it was switched off between cycles for either 5 seconds or 20 seconds. For each investigation (continuous use, intermittent use with 5-second intervals and intermittent use with 20-second intervals), the temperature of the fluid space was recorded.
For comparison a monoploar (VAPR II RF-system: Mitek, Westwood, MA, USA; 120 w side-effect) and bipolar (Opes bipolar RF-system: Arthrex, Naples, FL, USA; 120 w side-effect) electrode were studied.
Well controlled volumes, flow rates and power from the RF probe were used for each set-up and it was found that the system produced very similar results when a test was repeated.
Results
In all aspects of the study, an overall effect was observed that is illustrated by one example in each case for simplicity.
In all cases, ‘Switch’ indicates the time period with the probe on, and Temp 1 to 6 indicates the temperature probe readings within the cavity.
Cavity volume
Without any fluid flow in the system, the peak temperature was directly related to the cavity volume. For example, 60 seconds of continuous use of the RF probe resulted in the fluid temperature of a 20-mL volume rising from 22 °C (room temperature) to 76 °C. Fora 40-mL volume, the temperature rose to 52 °C and, for a 60-mL volume, to 46 °C (Fig. 2).
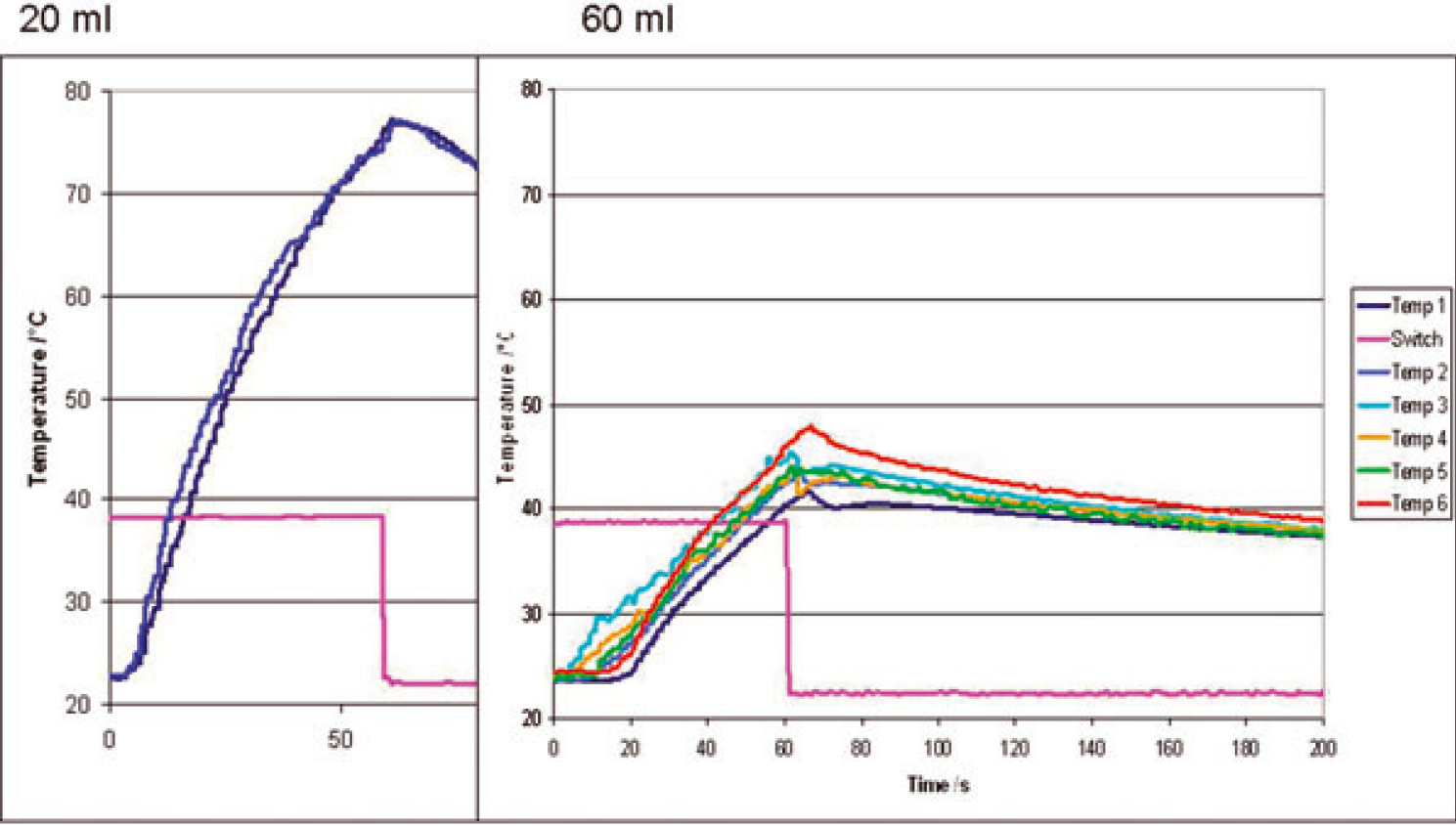
Effect of system volume on temperature rise with no flow and 60 seconds of continuous radiofrequency use.
RF mode
With no flow, the same peak temperature was reached when the RF probe was used intermittently (20 seconds on 5 seconds off, or 20 seconds on 20 seconds off) providing that the probe was used for a total period of 60 seconds. For example, with a fixed cavity volume of 40 mL and no fluid flow, the temperature of the fluid rose from 22 °C to 52 °C when the RF probe was used continuously for 60 seconds (Fig. 3). The time taken, however, to reach this peak temperature increased with intermittent use.
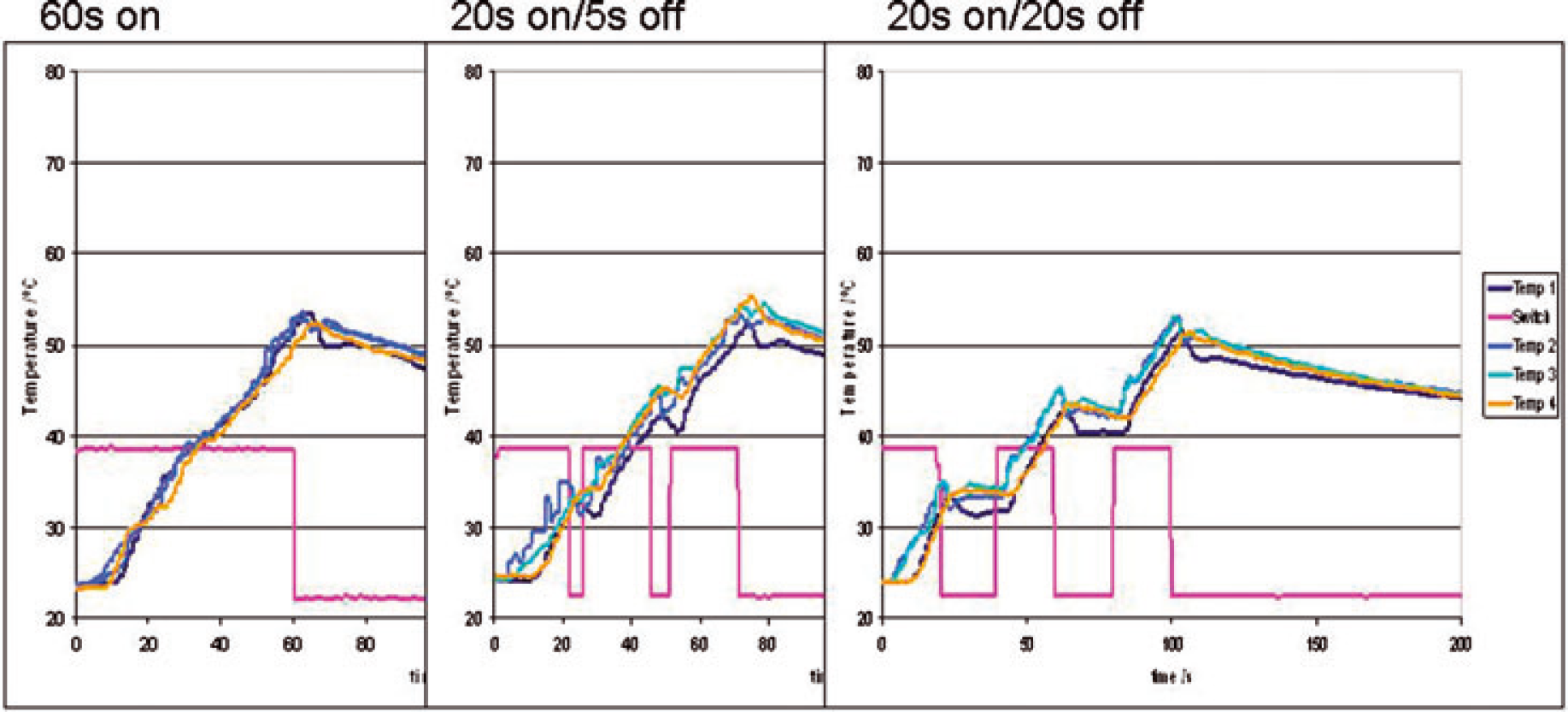
The effect of varying radiofrequency mode on temperature with no flow and room temperature inflow.
Inflow fluid temperature
The temperature of the inflow fluid was noted to affect the final temperature reached following use of the RF probe for 60 seconds. For example, with an inflow temperature of 22 °C, a cavity volume of 20 mL, intermittent RF of 20 seconds on/5 seconds off, and a fluid pump flow of 133 mL/minute, the fluid temperature rose to 41 °C. When the inflow fluid temperature was 35 °C and the other variables remained constant, the fluid temperature increased to 56 °C (Fig. 4).
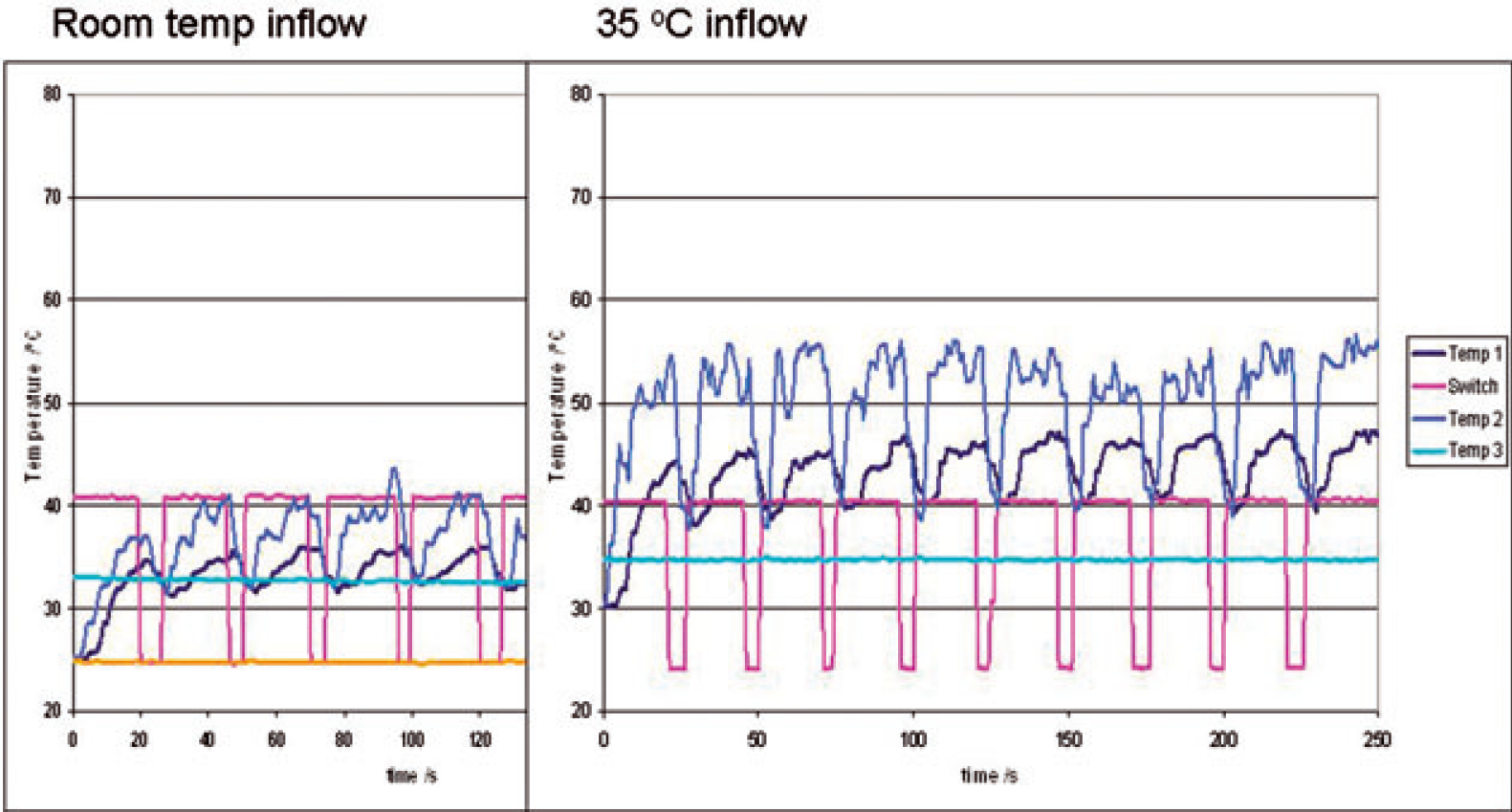
The effect of inflow temperature in a 20-mL system volume, flow 133 mL/minute, 20 seconds on and 5 seconds off.
Fluid flow
The ambient fluid temperature was found to be inversely dependent on the rate of flow of the lavage fluid. For example, in a 40-mL cavity volume with no fluid flow and 60 seconds of continuous RF application, the peak ambient temperature within the cavity rose to 54 °C. By increasing the fluid flow, there was a progressive reduction in the peak temperature reached within the fluid cavity: flow 52 mL/minute peak temperature 45 °C, flow 115 mL/minute peak temperature 40 °C, flow 225 mL/minute peak temperature 32 °C (Fig. 5).
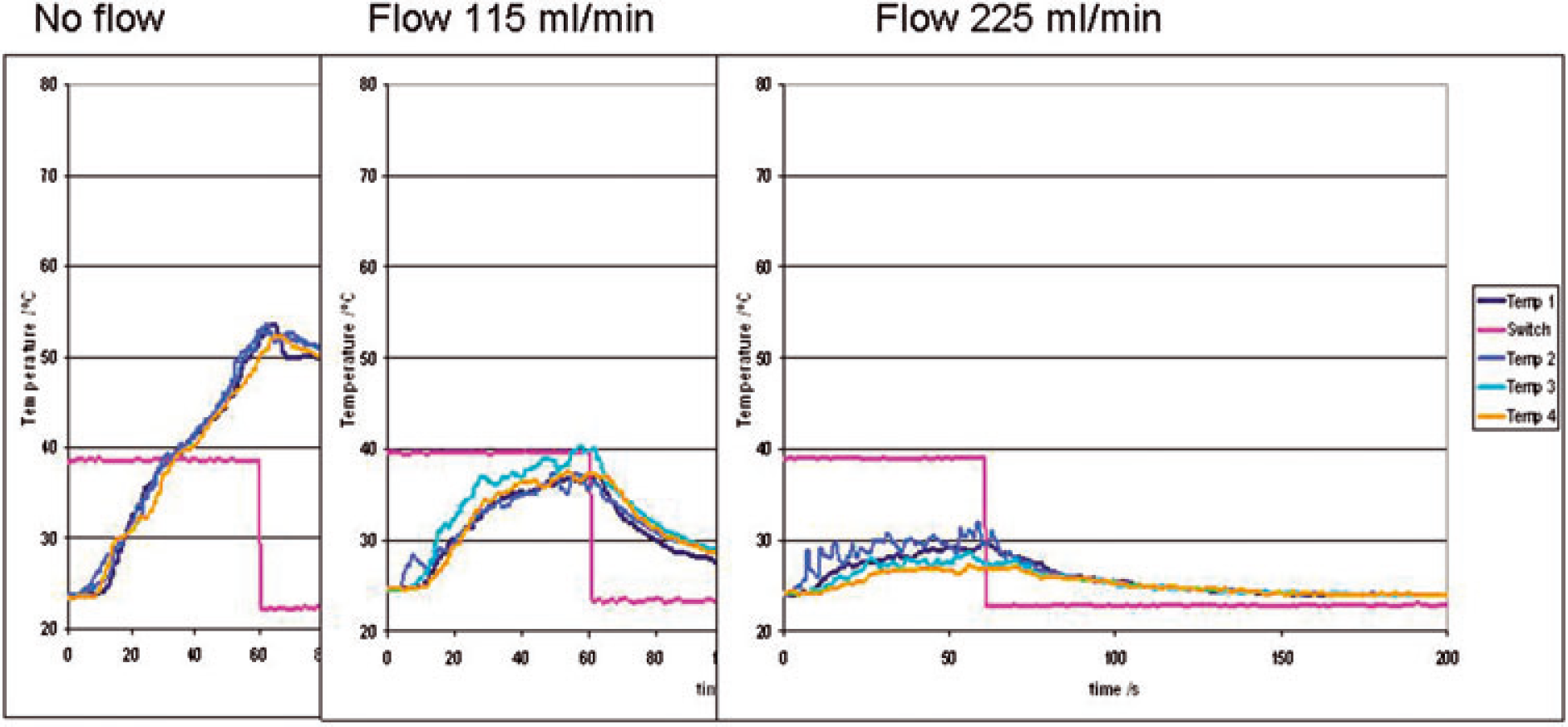
The effect of varying fluid flow on cavity fluid temperature for a 40-mL system volume, room temperature inflow, 60 seconds continuous radiofrequency use.
Outflow
The position of the outflow cannula in relation to the tip of the RF probe also affected the peak cavity temperature. When the outflow cannula was at maximum distance from the RF probe, higher cavity temperatures were recorded than when the outflow cannula was adjacent to the probe (Fig. 6).
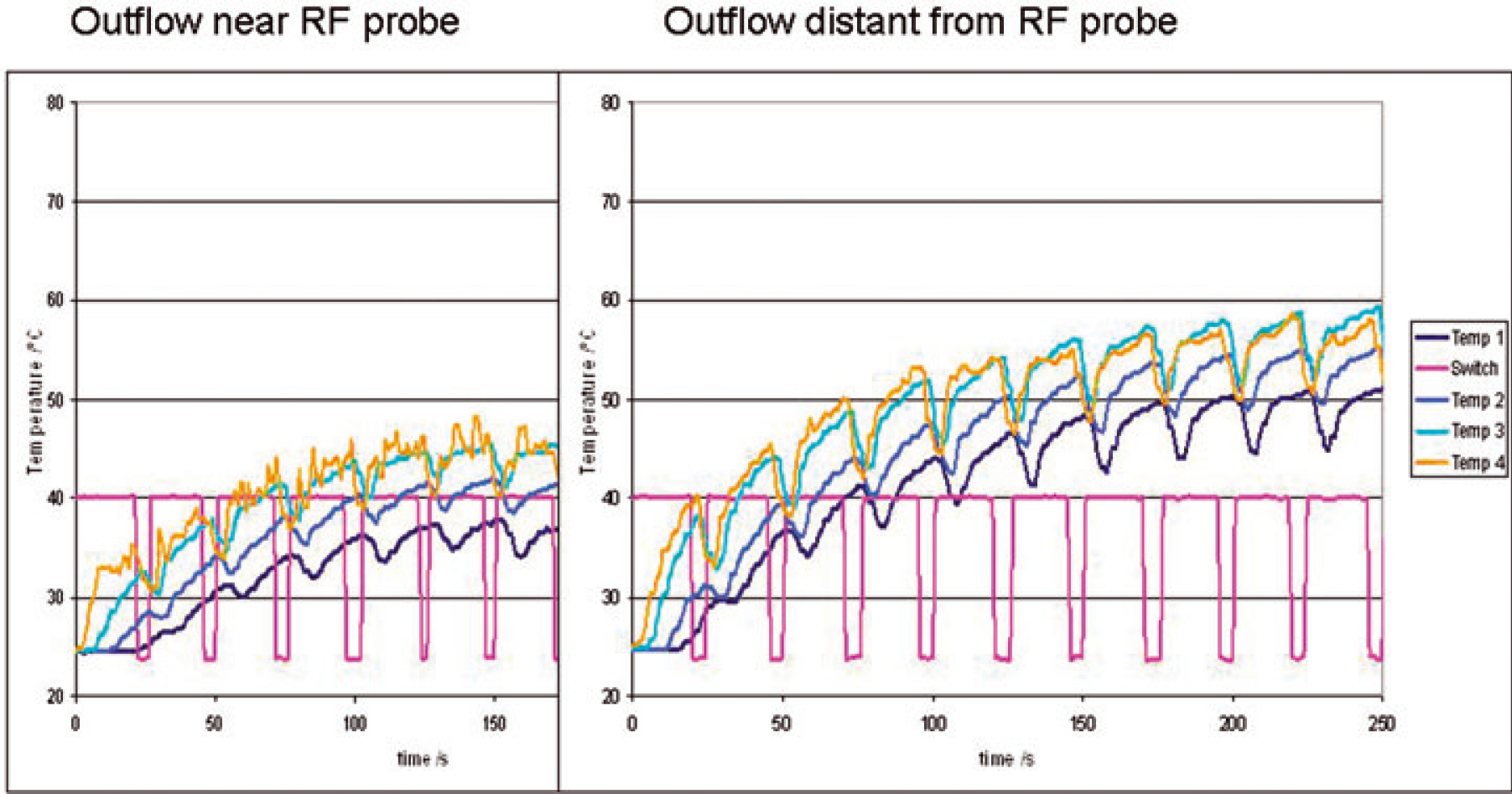
The effect of outflow cannula position on temperature with flow 52 mL/minute, radiofrequency use of 20 seconds on and 5 seconds off, 40-mL cavity volume.
Comparison of monopolar and bipolar electrode configurations
There was no difference in the peak cavity fluid temperatures when a monopolar electrode (Opes, Arthrex; 120 w side-effect) was compared to a bipolar electrode (VAPR II RF-system, Mitek; 120 w side-effect).
Discussion
Our in vitro model suggests that RF probes of all types may cause a temperature rise in the bathing fluid sufficient to cause cell death. In particular, the rise in temperature is most marked when there is no fluid flow through the compartment (regardless of whether the RF probe is used continuously or intermittently), at smaller fluid volumes, if the fluid inflow temperature is elevated, and if the outflow is distant from the RF device. We have demonstrated that higher temperatures can be generated if an outflow cannula is placed distant from the RF probe. Many devices now have a suction catheter built into the RF device, a feature that our evidence supports.
The effects of RF probes on articular cartilage have been well studied following the introduction of thermal capsulorraphy. Chondrocyte death has been noted at temperatures above 45 °C [8], [16], with a time-dependent effect noted in other studies [17]. The application of RF energy directly to a bovine articular cartilage model has demonstrated temperatures of 78 °C as deep as 2000 μ from the surface for bipolar RF probes, with a less severe effect from monopolar devices [9]. In a similar study, bRFE was noted to cause heating 90% deeper into cartilage than mRFE [18], [19]. The present study failed to demonstrate a differential direct fluid heating effect between bipolar and monopolar devices.
Although early clinical deleterious effects from heat injury appear to be rare, the potential of the RF probe to heat the fluid system remains a concern. We know little of the potential effects of increased fluid temperature on these tissues in the short term (postoperative pain and rehabilitation) or long term. To our knowledge, there are two studies focussing on heating effects of RF probes being used in subacromial decompression. This is despite the fact that the subacromial space is the most common site for the use of these devices. As surgery progresses and the bursa is excised, the effective volume of the space increases, and the fluid will contact tissues surrounding the bursa, and enter the glenohumeral joint in the presence of cuff tear. The present study, however, suggests that, at the beginning of the procedure, when the fluid volume is at its lowest, the risk of potentially dangerously high temperatures is at its greatest.
Although the pathological effect of temperature on articular cartilage at least is well understood, there is little clinical evidence of deleterious effects other than case reports [11], [12]. Other factors such as indwelling local anaesthetic catheters have also been implicated in post-arthroscopic chondrolysis [20]. We suggest that there is a need for controlled, in vivo pathological and clinical studies in this area, along with correlation between the use of these devices and outcomes, including postoperative pain and long-term outcome.
Other recent studies have evaluated the effects of RF devices on fluid temperature in shoulder arthroscopy. In similar experiments to ours, Lu et al. used a fixed volume 25 mL model and a fixed flow of 200 mL/minute [2]. As in the present study, they noted a temperature rise proportional to time of continuous probe use with no flow. However, no device tested produced a temperature above 40 °C with intermittent or continuous use and flow. All devices in the present study produced high temperatures.
Three cadaveric models have also been used [1], [3], [13]. Good et al. demonstrated fluid temperatures above 45 °C with the use of a Mitek VAPR device in both continuous and intermittent modes, and irrespective of whether or not flow was applied [1]. Temperature rises were greater if there was no flow. McKeon performed both capsulorraphy and ASD in 15 cadaveric shoulders, with three devices and varying flow [13]. No mean temperatures above 40 °C were recorded in ASD, with no significant differences between devices, although peak temperatures were not reported.
In a third study, Zoric et al. measured the temperature intermittently when using an ArthoCare device (ArthoCare Corp., Austin, TX, USA) in three flow environments [3]. Although temperatures increased in no flow, little increase was noted if low or high flow were present. There was found to be a 32% probability of the temperature exceeding 50 °C when no flow was present, but only 1% in any fluid flow.
In the only published in vivo study, Davies et al. recorded the temperature in the subacromial space during ASD, and found a mean temperature of 27.8 °C with a maximum of 41.8 °C [14]. They recorded no evidence of chondrolysis at 2-year follow up.
By using an in vivo perspex model, we clearly are creating a rather different situation than in vivo.
The heat sink effect of living tissue, whereby blood flow will conduct heat energy away from the heat source, is ignored. Additionally, the perspex material used has low thermal conductivity, and acts as a thermal insulator. These factors may lead to over-estimation of temperature rises seen in our model compared to intra-operatively. However, the magnitude of any heat sink effect of the body is difficult to quantify, and the body may well in itself insulate or heat the irrigation fluid and lead to greater temperature rises than observed in the present study.
We feel that the use of our model offers advantages. In most in vivo situations (and cadaveric models), there is an interaction of innumerable variables upon the studied effects that cannot be controlled. The volume changes during the procedure, the fluid flow within this space is complex; there may be areas of high and low temperature that cannot be adequately measured. In our model, the volume and flow can be very closely regulated, and we can make some assumptions about the uniformity of fluid flow within the space. Our model allows the control of volume, an important variable that cannot be achieved in vivo or with a cadveric model.
In a controlled system, we have demonstrated that many factors possibly leading to high temperatures are within the surgeons control. High temperatures were seen particularly at low volumes, with low flow, and with higher inflow temperatures and an outflow distant from the device. We recommend prudence in the use of these devices, particularly in low volume spaces such as at the beginning of ASD. An outflow should be used close to the device (many of which have inbuilt suction catheters), and care should be taken to ensure adequate flow through the system. We have demonstrated high irrigation fluid temperatures using warmed fluid. Irrigation fluid is often warmed to prevent patient hypothermia in prolonged procedures. Caution is therefore advised to balance these potential risks; perhaps the use of unwarmed fluid for shorter procedures using RF devices, and warmed fluid when these devices are not used, or at stages of surgery when their use has ended.
Finally, further in vivo clinical and pathological studies are needed to define whether the potential dangers of these devices translate into a cause for greater concern, both in terms of tissue injury and potential increases in postoperative pain.