
Abstract
Background
Disruption of the coracoclavicular ligaments may be associated with dislocation of the acromioclavicular joint, resulting in pain and functional disability. The Surgilig (Surgicraft Ltd, Redditch, UK) is a synthetic ligament used to reconstruct the ligaments, thereby stabilizing the joint.
Methods
Between 2004 and 2009, 50 patients with acromioclavicular joint dislocation were reconstructed using the Surgilig system. Five patients were lost to follow-up; hence, 45 patients underwent review. Patients were evaluated clinically and radiologically at an average of 26.9 months (range 6 months to 60 months) postoperatively using the Oxford, University of California, Los Angeles (UCLA) and Simple Shoulder scoring systems.
Results
The mean Oxford score was 45.31 (SD 4.52, range 35 to 48), the mean UCLA score was 31.38 (SD 5.07, range 11 to 35) and the mean Simple Shoulder score was 10.92 (SD 1.7, range 6 to 12). Ninety-one percent of patients were completely satisfied with the procedure and outcome. Few complications were encountered, with no recorded infections. However, one patient underwent early revision for persistent instability. Six patients had the screw removed at a later stage as a result of local skin irritation. Removal of the screw did not result in recurrent instability.
Discussion
The present study is the largest reported mid-term results using the Surgilig technique, and appears to be successful for treating both acute and chronic injuries, with high patient satisfaction and excellent functional results.
Introduction
Acromioclavicular joint (ACJ) injuries commonly result from a direct force, generally occurring from a fall onto the tip of the shoulder with the arm adducted. They comprise 3% to 5% of all shoulder injuries [1]. Disruption of the acromioclavicular ligaments alone after such trauma may result in inferior subluxation (i.e. the acromion is driven anteroinferiorly) of the ACJ. Larger forces can lead further to rupture of the coracoclavicular ligaments, resulting in the complete dislocation of the ACJ, with long-term pain and functional disability.
ACJ injuries were classified by Tossy et al. [2] and Allman [3] as incomplete (Grades I and II) and complete (Grade III). Neviaser [4] subdivided Grade III injuries into IIIA (reducible) or IIIB (irreducible) depending on the effect of upward force on the elbow, suggesting the latter type required operative treatment. Whereas, Rockwood [5] expanded the original classification by subclassifying Grade III injuries into four types, resulting in a total of six types (I to VI).
We use Rockwood's classification to describe injury patterns in our study [5].
The treatment for ACJ disruption varies according to the grade of injury. In general, there is a consensus that Types I and II are treated conservatively with analgesia, a short period of support in a broad arm sling, followed by early mobilization [1]. However, the evidence suggests that Types IV, V and VI comprise injuries that have a poorer outcome if conservatively managed and operative intervention is required [1], [6].
The ideal treatment of the Type III injury remains controversial and practice varies between centres and individuals. Most Type III injuries are currently treated conservatively [7]. A series of retrospective studies showed no outcome differences between operative and non-operative groups. Furthermore, the patients treated non-operatively returned to full activity sooner than surgically treated groups [8], [9]. Exceptions to this include those individuals who perform repetitive or heavy lifting, those who work with their arms overhead, and thin patients who have prominent ACJ. These patients may benefit from surgical repair [10], [11].
Surgical repair can be divided into six main types:
Acromioclavicular fixation: intra-articular repair with Kirshner wires [12], hook plates [13].
Coracoclavicular fixation: Bosworth screws [14], Cerclage
Distal clavicular excision [15].
Distal clavicular excision and coracoacromial ligament transfer: Weaver–Dunn [16].
Coracoclavicular ligament reconstruction using soft tissue: free tendon grafts, dynamic muscle transfer [17].
Coracoclavicular ligament reconstruction using prosthetic ligament: Surgilig [18], Tightrope.
We report our experience and medium-term results with the use of the Surgilig (Surgicraft Ltd, Redditch, UK) prosthetic ligament for ACJ reconstruction.
Materials and Methods
In this prospective cohort study, 50 patients with Type III to V ACJ injuries, who consented for surgical management, were treated using the Surgilig prosthetic ligament. The ligament utilizes a braided synthetic polyester ligament with loops on both ends to reconstruct the disrupted coracoclavicular ligaments by securing the distal clavicle to the coracoid, thus providing strong biocompatible fixation (Fig. 1).
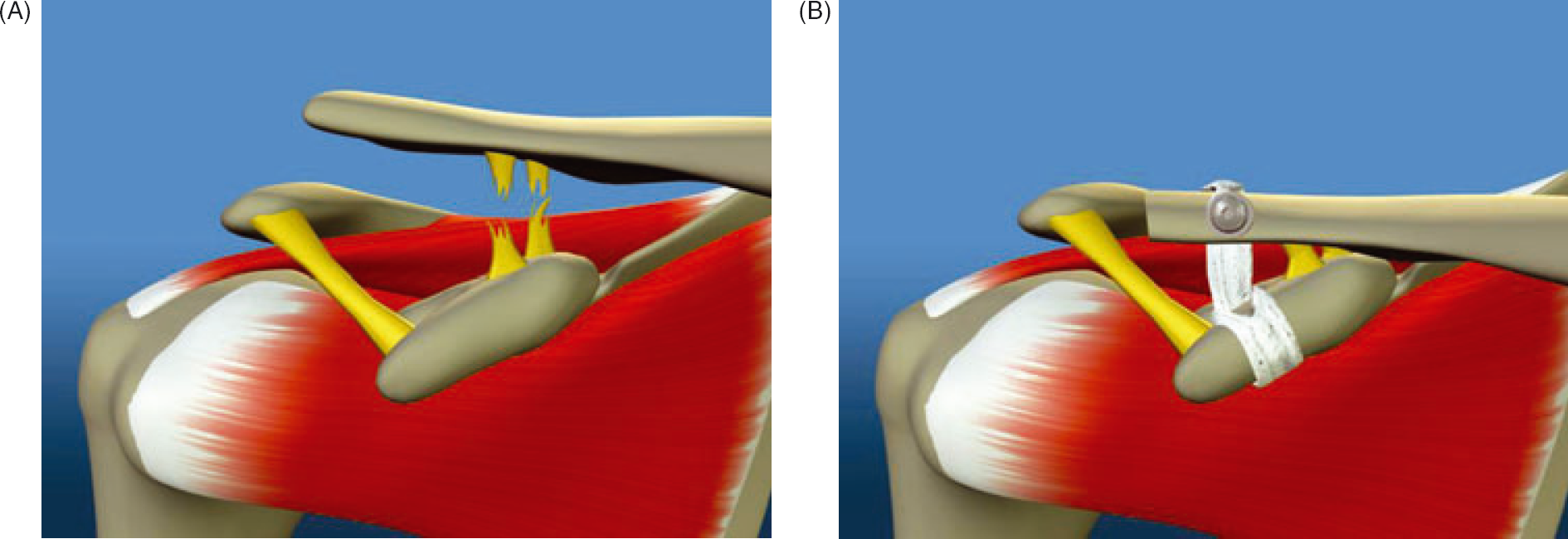
(A) Acromioclavicular joint (ACJ) dislocation and coracoclavicular (CC) ligament rupture. (B) Surgilig: ACJ stabilization (CC ligament reconstruction).
Operative technique
All operations were performed by the two senior authors, under general anaesthesia with the patient in the supine position, with head-up tilt. A vertical skin incision was made from above the clavicle just medial to the ACJ to the level of the coracoid process. The deltoid muscle was split in line with its fibres and the trapezius deltoid interval was incised to expose the lateral clavicle. The distal 5 mm to 10 mm of clavicle was excised. The base of the coracoid was identified and a curved guide instrument was carefully slid adjacent to and around the bone from medial to lateral to allow the Surgilig to be seated close to the coracoid. The instrument was then used to feed the Surgilig Length Gauge around the coracoid. This measuring tape was then looped around the coracoid in the same manner as the proposed ligament, and passed up and behind the lateral end of the clavicle. The clavicle was reduced to its normal alignment and the appropriate length was determined.
The Surgilig was then ‘daisy chained’ to the Surgilig Length Gauge and passed around the base of the coracoid. The hard loop on the ligament was threaded through the soft loop, so that the soft loop sat on the superior aspect of the coracoid. The Surgilig was tensioned to the coracoid using a Loop Tensioner and the free end (hard loop) passed inferiorly around the posterior aspect of the clavicle. This was then fixed to the anterosuperior surface of the clavicle with a 3.5-mm bi-cortical screw and accompanying washer. Postoperatively, the arm was supported in a sling for 4 weeks and then mobilized with supervised physiotherapy.
All 50 patients were reviewed clinically and radiographically by the two senior surgeons.
Anteroposterior, lateral and axillary view radiographs were taken pre-operatively and post-operatively (Fig. 2).
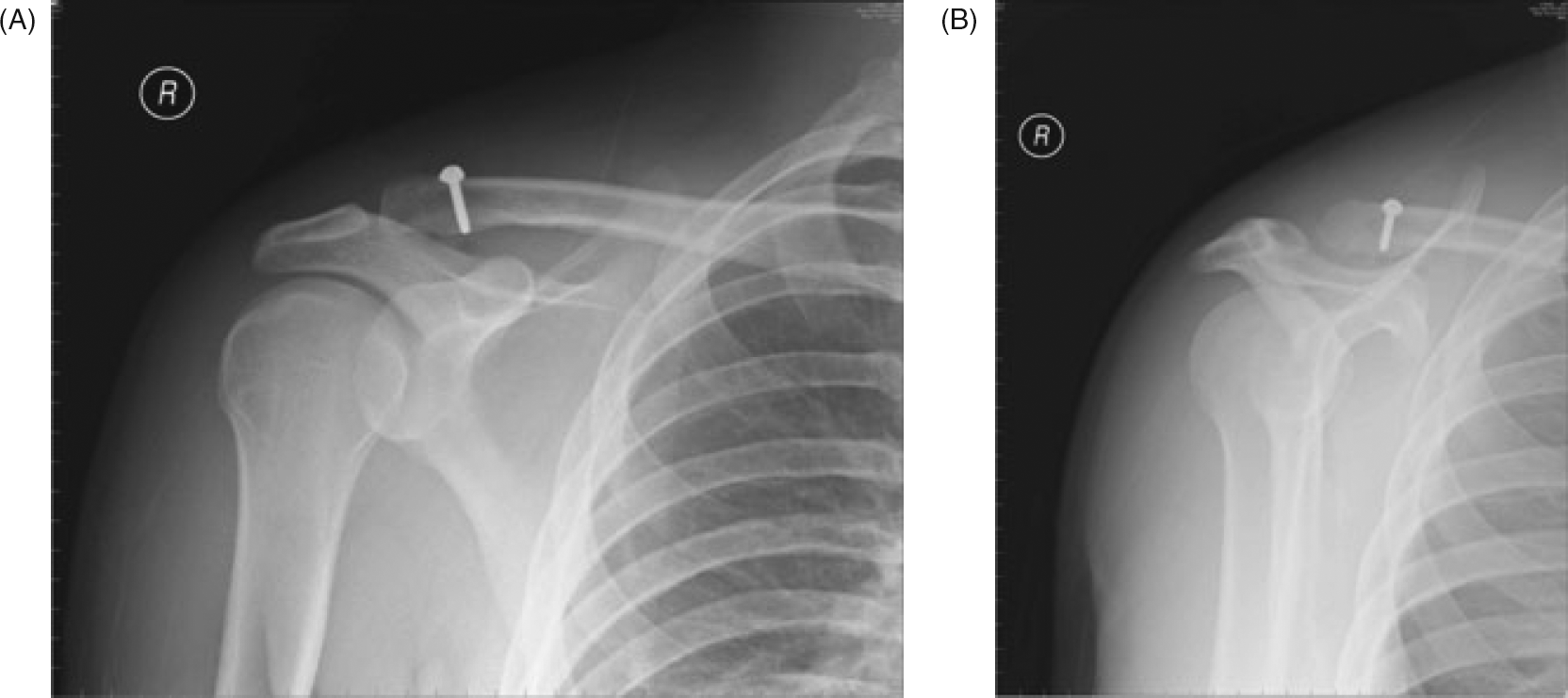
(A) Postoperative anteroposterior view radiograph showing a reduced and Surgilig stabilized acromioclavicular joint (ACJ) dislocation. (B) Postoperative lateral scapular view radiograph showing a reduced and Surgilig stabilized ACJ dislocation.
Anteroposterior radiographs were taken with a 10° cephalic tilt view of the ACJ. Radiographic analysis of postoperative clavicle migration on the AP radiographs was measured in millimetres using the measuring tool from the Picture Archive Communication System (PACS) software (Centricity, GE Medical Systems).
Functional outcome was assessed using the University of California, Los Angeles (UCLA), Oxford and Simple shoulder scoring systems. The subjective result of surgery was assessed in terms of patients’ satisfaction, with patients being asked whether they would undergo the same procedure again for a similar problem.
Results
We have evaluated the medium-term clinical outcomes in a cohort of 50 patients treated with a Surgilig reconstruction of acromioclavicular injuries. Five patients were lost to follow-up, leaving 45 for review. This group had a mean age 37.6 years (range 19 years to 67 years), and consisted of 32 males and 13 females. Sixteen of the injuries were classified as Rockwood Type III, four as Type IV and 25 as Type V.
Seventeen of the cases were treated within 2 weeks of the original insult, whereas 28 were treated at a longer time interval. The average interval from injury to operation was 7.2 months (range 0.5 months to 120 months).
The mean follow-up period was 26.9 months (range 6 months to 60 months). The mean UCLA score for the whole group was 31.38 (SD 5.07, range 11 to 35). The mean Oxford Score was 45.31 (SD 4.52, range 35 to 48). The mean Simple score was 10.92 (SD 1.7, range 6 to 12).
Forty one of the patients stated that they were satisfied with the procedure, and would undergo the same operation again if a similar problem occurred. Four patients were not satisfied. Two had residual pain (one of these patients had an outstanding compensation claim), one patient was unhappy with the cosmetic appearance, and one patient was unhappy with both the cosmetic appearance and ongoing pain.
The majority of patients (n = 32) showed no migration of the clavicle, when comparing immediate postoperative radiographs with those taken at latest follow-up. Migration was defined as the difference in coracoclavicular distance when comparing postoperative radiographs. Migration was noted in 13 cases. In this minority group, the mean migration was 6.3 mm (range 3 mm to 9 mm).
Seven patients required further surgery. One patient required an early revision because the Surgilig displaced within the first week. Six patients ultimately required removal of the screw because of skin irritation. This was usually performed at approximately 9 months postoperatively and did not result in recurrent instability.
Discussion
ACJ dislocation is a common injury and, given the number of different surgical procedures that have been described for its treatment, no single technique has been demonstrated to be ideally suited. Although there appears to be consensus that Type IV to VI injuries should be surgically managed, the management of Type III injuries still causes debate, with some centres advocating immediate surgery, whereas others suggest a conservative approach and intervention at a later date should the patient remain symptomatic.
In the present study, our preferred protocol involved initial non-operative treatment of Type III injuries, with analgesia and physiotherapy, and consideration of the surgical option if the shoulder remains painful and there is functional loss beyond 6 months after the injury. We treated all Type IV and V injuries operatively. A proportion of Type V injuries in our series were not immediately surgically treated. These cases had been initially managed elsewhere or had alternative initial advice in Accident and Emergency departments and hence had considerable delay in their presentation to our unit.
Over 60 different surgical procedures have been suggested for treating ACJ dislocations [2].
Amongst those described, the Mumford and Gurd technique involves simple distal clavicular excision and is mainly indicated for symptomatic Type II subluxations [15], [19].
In the Modified Phemister technique, the ACJ is reduced and internally fixed with unthreaded Kirschner wires through the acromion, joint and lateral clavicle [12]. There is a risk of wire loosening and migration until they are removed at 8 weeks postoperatively and reduction can be lost soon after wire removal.
In the Modified Bosworth technique, the ACJ is reduced, and fixation achieved by drilling a Bosworth screw from the clavicle into base of coracoid, followed by coracoclavicular ligament repair with sutures [14]. Again there is risk of migration, loosening with erosion of bone, which sometimes leads to fracture of the weakened clavicle.
The Hook Plate technique has the disadvantage of a larger incision, a reduced range of movement postoperatively as a result of impingement symptoms from the subacromially placed ‘hook’ and the necessity of a second procedure to remove the implant [13].
More recently, the modified Weaver–Dunn technique has been very popular for treating symptomatic ACJ dislocations [16]. This involves excising the distal clavicle. Next, the coracoacromial ligament, along with a sliver of acromion at its attachment, is freed and sutured to the remaining distal clavicle through the intramedullary canal, to achieve reduction. Although good results have been reported, the coracoacromial ligament is not always present, and this procedure unavoidably disrupts the coracoacromial arch. Recent biomechanical studies have stressed the importance of preserving, where possible, the subacromial arch and specifically the coracoacromial ligament for shoulder stability [20]. Release of the coracoacromial ligament can lead to increased glenohumeral joint translation andlaxity [21]. Additionally, transection of this ligament removes the buffer between the acromion and the rotator cuff, which may lead to subacromial symptoms and cuff pathology [22]. Although it is accepted that the original Weaver–Dunn technique has had various modifications, especially in higher-grade injuries, which require combined coracoclavicular ligament reconstruction or fixation, the use of a corocaoacromial ligament sparing artificial ligament may therefore confer an anatomical advantage.
Augmentation cerclage techniques for the reconstruction of the coracoclavicular ligament include PDS [23], Merselene [24] and carbon fibre [25] and these have been associated with the risk of the device cutting through the bone and failure of reduction. In our series, we did not see any evidence of coracoid erosion or fracture, although we accept that this has been described in earlier smaller series with shorter follow-up [18].
Recently, all-arthroscopic or arthroscopic-assisted techniques have been described to achieve reconstruction; however, the results so far have limited numbers with only short-term follow-up [26]–[28]. Some studies include cases with intact acromioclavicular ligaments, allowing arthroscopic excision of symptomatic ACJ without any underlying or resulting instability. All these studies cite high patient satisfaction with cosmetic appearance. Interestingly, however, only two of our series (4%) were concerned regarding their cosmesis after surgery.
The overall success rate in ACJ reconstruction surgery is approximately 90%, as reported in various studies [1], [6], [16], [29]. In the case of late reconstruction, the success rate has been reported at approximately 78% [6], [29]. In the present study, the use of the Surgilig in ACJ disruptions has yielded comparable, if not better, overall results compared to the other techniques of early and/or late reconstructions reported in the literature, with comparatively less adverse effects [18], [30].
A single patient had recurrent instability warranting early revision surgery in our series. This was considered to be a failure of technique because the Surgilig slipped from behind the clavicle as a result of inadequate positioning and tensioning. By performing an oblique cut to the distal clavicle, thereby preserving more posterior bone, and with increased experience of using the implant, no subsequent failures were observed.
Six patients elected to have the screw removed at least 9 months after surgery as a result of irritation or prominence beneath the skin. However, we found that the prosthetic ligament appeared to allow tissue in growth because, whenever the screw in the distal clavicle was removed, the new ligament remained in situ, securely attached to the periosteum of the clavicle. This finding is also reported in previous studies [30]. Additionally, no recurrent displacement or instability of the clavicle occurred. Despite requesting removal of these screws, most of these patients remained satisfied with their surgery.
A minority of 13 patients showed migration of the clavicle postoperatively. None had an appearance greater than a Type II injury position on postoperative radiographs and only two patients had concerns with cosmesis. We found no correlation between migration and pain, grade or chronicity of injury. We accept that it was not possible to completely standardize the radiographic views and there is a potential observer bias in the radiographic analysis.
There were no cases of postoperative infection or re-operations as a result of impingement of the lateral end of the clavicle on the acromion, as previously described in other series [18]. Also, unlike previous studies, none of our patients reported any untoward reactions to the synthetic materials used for reconstruction [31].
Despite a good sample size, the limitations of the present study include the lack of pre-operative functional scores, thereby making it difficult to assess and compare the definitive improvement after the procedure. We accept that the heterogeneity of our cases, in terms of grades and chronicity, makes it difficult to make clear conclusions on a specific classification subgroup.
Conclusions
The present study provides the largest reported medium-term results using the Surgilig technique. We have been successful in treating both acute and chronic injuries, with high patient satisfaction and excellent functional results. So far, there has been sparse evidence on the use and longer-term outcomes of this implant for treatment of ACJ injuries [18], [30]. We have not had any significant complications or adverse reactions outlined in previous studies. The implant appears inherently strong and allows preservation of the coracoacromial ligament. We conclude that this technique is a safe, simple and reproducible method of reducing and stabilizing the acromioclavicular joint.