
Abstract
A 41-year-old man was referred for an ultrasound scan to investigate a soft tissue mass in his axilla, considered to be the cause of an axillary vein thrombosis. The scan showed the mass to be a cystic lesion, with a deep extension towards the humeral head. Magnetic resonance imaging showed a large paralabral cyst arising from the inferior labrum and extending into the axilla, compressing the axillary vein, and this was considered as the likely cause of the thrombosis. There was associated tearing of the inferior labrum, which was detached from the underlying glenoid. The patient is heterozygous for the factor 2 gene mutation, which predisposes him slightly to thrombosis. In this patient's case, his moderate increased risk of clotting coupled with extrinsic compression of the axillary vein was sufficient to lead to thrombosis. He subsequently underwent arthroscopic drainage of the cyst.
Introduction
Paralabral cysts can be responsible for a multitude of symptoms around the shoulder. We present an unusual case of a man presenting with a painful, swollen arm which turned out to be an axillary vein thombosis secondary to an inferior paralabral cyst.
Case Report
A 41-year-old man was under the care of the haematologists for an axillary vein thrombosis, which had presented as an acutely swollen, painful arm. He was anticoagulated with warfarin but referred to the upper limb clinic with a residual, ill-defined soft tissue mass in his axilla with no shoulder joint symptoms. An ultrasound scan was requested, which showed the mass to be a cystic lesion, with a deep extension towards the humeral head. However, it was not possible to define the full extent of the lesion with ultrasound (Fig. 1), and so magnetic resonance imaging (MRI) was undertaken. This showed a large paralabral cyst arising from the inferior labrum and extending inferiorly into the axilla, compressing the axillary vein, and this was considered as the likely cause of the thrombosis (Fig. 2). There was associated tearing of the inferior labrum, which was detached from the underlying glenoid. There was no evidence of atrophy to the rotator cuff muscles. He subsequently underwent arthroscopic drainage of the cyst by increasing the size of the inferior glenoid flap-valve to enable the fluid to drain into the shoulder joint (Fig. 3). This has led to complete resolution of his axillary mass. He has subsequently been discharged from orthopaedic care and, because the cause of the thrombosis has been removed, he has ceased anticoagulation therapy.
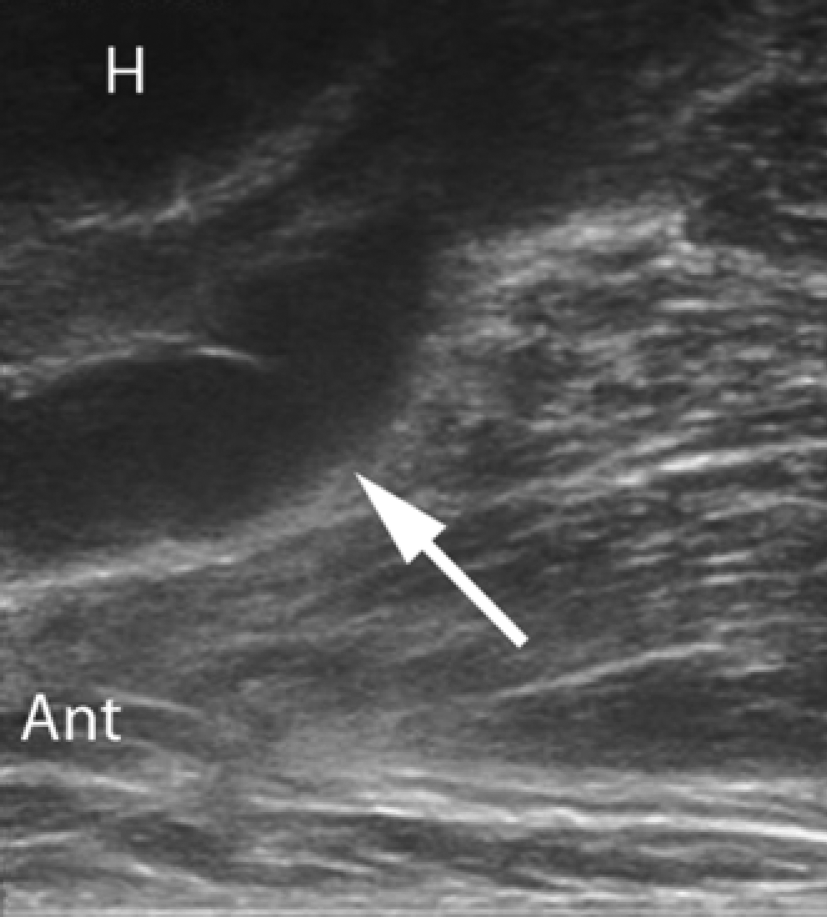
Sagittal ultrasound image. The image has been inverted to show the features as they would be seen in the anatomical position. The skin surface of the axilla is at the bottom of the image. The elongated cystic structure (arrow) is seen passing inferior to the humeral head (H). Ant, anterior.
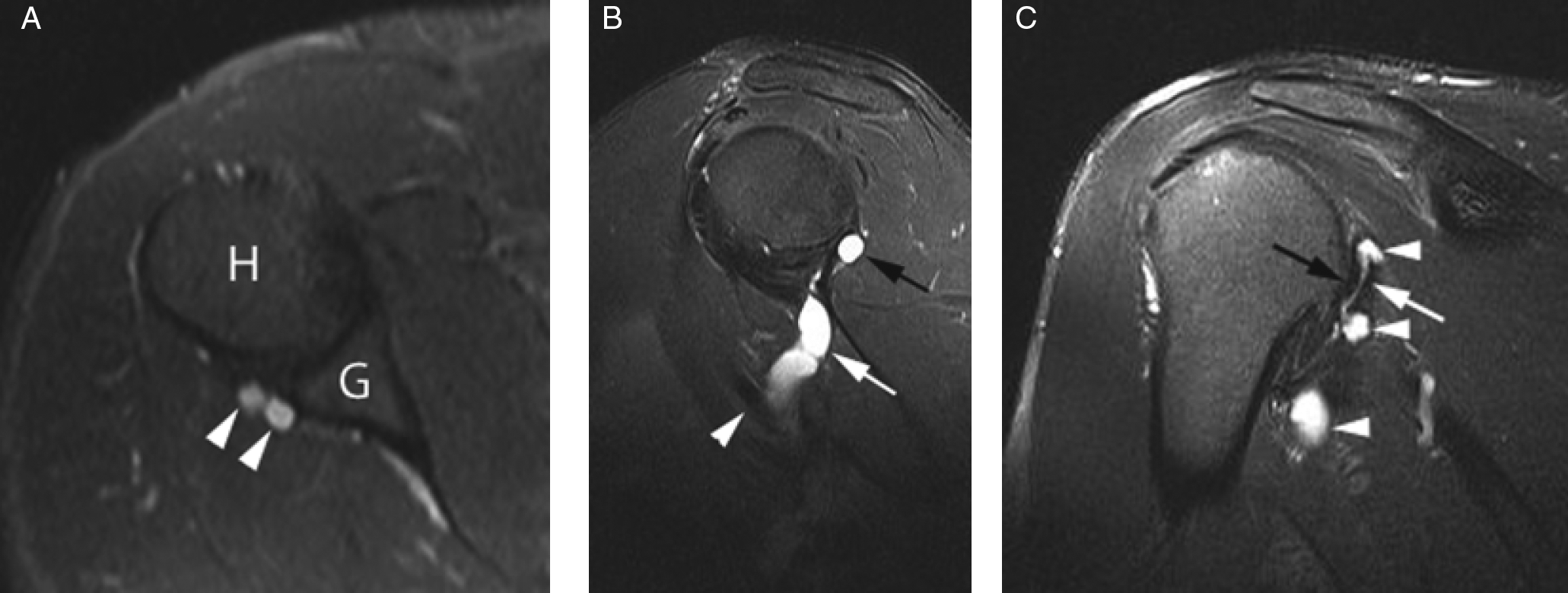
(A) Axial T2 fat suppressed image through the inferior glenohumeral joint. Two locules of the cyst are seen in association with the posterior labrum (arrowheads). H, humerus; G, glenoid. (B) Sagittal oblique proton density fat suppressed image through the glenohumeral joint. The cyst is seen extending inferior to the joint (white arrow), where it is seen to encroach on the axillary vein (arrowhead). A small locule of the cyst is also seen more superiorly (black arrow). (C) Coronal oblique T2 fat suppressed image through the posterior glenohumeral joint. Several parts of the cyst are shown (arrowheads), emphasizing their close relationship with the posterio-inferior labrum (black arrow), which is seen to be detached from the glenoid (white arrow).
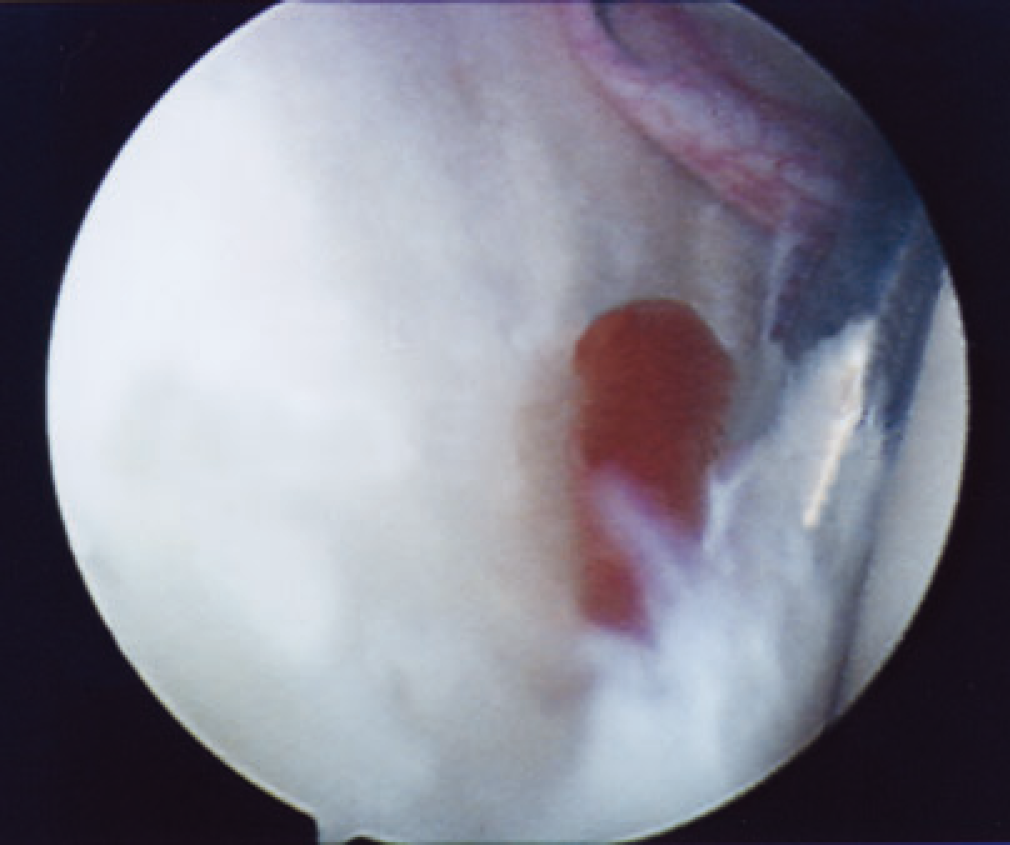
Drainage of cyst at arthroscopy by increasing the size of the flap-valve.
The patient is heterozygous for the factor 2 gene mutation, which is common in 1% of the general population, although the vast majority of individuals carrying this gene do not develop thrombosis. In this patient's case, his moderate increased risk of clotting coupled with extrinsic compression of the axillary vein was sufficient to lead to thrombosis.
Discussion
Paralabral cysts are a well recognized finding on shoulder MRI examinations and are associated with the presence of labral tears, which are often also shown on MRI [1]. It is considered that these cysts are formed following trauma to the capsulolabral complex, leading to extravasation of synovial fluid, which accumulates as either a unilocular or multilocular cystic structure. Similar mechanisms are considered to account for the association between paralabral cysts and hip labral tears, as well as parameniscal cysts and meniscal tears.
Paralabral cysts are a recognized cause of nerve entrapment. Posterosuperiorly, the cyst may extend into the spinoglenoid notch where the suprascapular nerve may be compressed, resulting in infraspinatus atrophy [2]–[4]. Less commonly, the cyst may compress the suprascapular nerve more proximally in the suprascapular notch, causing atrophy of supraspinatus with or without infraspinatus atrophy [3]. Occasionally, larger cysts may give rise to a quadrilateral space syndrome, impinging on the axillary nerve, with resultant teres minor denervation atrophy [2], [5]. Patients with paralabral cysts usually present with chronic, diffuse and deep posterolateral shoulder pain. They may also have symptoms and signs of instability as a consequence of the capsulolabral damage. Every other paralabral cyst drained by the senior author has been posterior with a definite tear posteroinferiorly, although the present case was particularly unusual because the cyst extended directly inferiorly.
Plain film radiography will not demonstrate paralabral cysts or associated capsulolabral injuries. Ultrasound may demonstrate paralabral cysts and muscle atrophy if there is associated nerve entrapment; however, the labral damage is rarely visualized. MRI imaging findings include a thin-walled, rounded, sometimes multiloculated hyperintense structure on T2-weighted imaging that is hypointense on T1-weighted imaging [6]. A track extending to the labrum will normally be identified and should always prompt a search for the associated labral tear. MRI arthrography improves the accuracy of labral tear detection. Contrast may not always be seen within the cyst itself [7].
The treatment of paralabral cysts has traditionally been performed by open surgery but, more recently, there has been success with arthroscopic cyst drainage [8]. To our knowledge, a paralabral cyst causing axillary vein compression followed by thrombosis has not previously been reported. The present report highlights that identification of these cysts may come to light when they cause extrinsic compression of structures, be they neurological, vascular or mass effect.