
Abstract
Background
Glenohumeral internal rotation deficit (GIRD) and posterior shoulder stiffness have been associated with impingement symptoms in the overhead athlete. Stretching of the posterior shoulder is advised in injury prevention as well as rehabilitation programs. The purpose of the present study was to determine if stretching of the posterior shoulder improves ROM and reduces symptoms, and to compare angular with non-angular stretching techniques.
Methods
60 overhead athletes with GIRD (age 25 ± 7.2 years, height 176 ± 8 cm, weight 69.8 ± 10.2 kg) participated to the study. Thirty athletes had no shoulder pain, 30 had impingement symptoms on the dominant shoulder. The subjects were randomly assigned into an “angular” or a “non-angular” treatment group. They were treated for 3 weeks (9 sessions) and followed for another period of 3 weeks after completion of the treatment. Treatment outcome variables were glenohumeral internal rotation range of motion, and, in the patient group, pain (VAS) scores and functional performance (ROWE-score).
Results
Statistical analysis showed a significant increase in ROM (p < .05) in both treatment groups, in the patient as well as in the healthy control group. In addition, patients showed a significant improvement in pain assessment scores, and a significant increase in the Modified Rowe Score. There were no significant differences between both treatment techniques.
Discussion
Stretching, angular as well as non-angular techniques, increases internal rotation ROM in overhead athletes, and may decrease sport specific shoulder pain in overhead athletes with impingement symptoms.
Keywords
Introduction
Overhead athletes place their shoulder under tremendous stress during their throwing or smashing activities. Powerful acceleration and eccentric energy absorption are necessary components that result in an optimal throwing performance. Altered glenohumeral joint mobility and flexibility are reported in overhead athletes, and have been attributed to adaptive structural changes to the joint, resulting from the extreme demands of overhead activity [1]–[15]. These adaptive changes have been defined as glenohumeral internal rotation deficit (GIRD), very often combined with external rotation gain [1], [8], [16]. Pappas et al. were the first to suggest that posterior shoulder stiffness results from repetitive microtrauma leading to the development of fibrotic scar tissue of the posterior capsule [17]. Currently, the exact cause and underlying mechanism of posterior glenohumeral joint stiffness remains a matter of debate. Posterior capsule contracture, as well as posterior cuff muscle inflexibility and osseous adaptations, are described to clarify the decreased internal rotation range of motion (ROM) [1], [2], [7], [11], [12], [18][19][20][21][22]–[23].
Posterior shoulder stiffness has been suggested to be a causative or perpetuating factor in shoulder impingement and labral pathology [1], [5], [9], [16], [20], [24], [25]. Abnormal humeral head translations, caused by selective tightening of the posterior-inferior capsule, may decrease the width of the subacromial space, thus causing subacromial impingement [26]. Other studies [20] suggest a posterior and superior translation of the humeral head during cocking (i.e. the phase in throwing where the glenohumeral joint is placed into maximal external rotation and horizontal abduction) with a tight posterior capsule, possibly leading to an encroachment of the rotator cuff tendons against the postero-superior rim of the glenoid. As a result, posterior capsule stiffness possibly increases the risk for internal (postero-superior) as well as subacromial impingement in the overhead athlete [16], [20], [26].
Based on the findings of these sport-specific adaptations in the overhead athlete, and the possible association with the development of impingement symptoms and labral injury, stretching has been recommended in the prevention, as well as rehabilitation, of chronic shoulder pain [1], [5], [15], [16], [27]–[30]. In general, two unique intervention techniques are described in literature to increase glenohumeral internal rotation ROM [1], [15], [16], [24], [31]–[33].
In the angular stretching techniques, internal rotation (e.g. the ‘sleeper-stretch’) or horizontal adduction (e.g. the ‘cross-body-stretch’) movements are passively performed, by the therapist, or by the patient [1], [15], [16], [24], [32].
In addition to angular stretching techniques, translational mobilization techniques (using accessory movements [34]) have been described to increase internal rotation ROM [16], [35], [36]. High-grade (grade III and IV in the Maitland classification) [34] end-range dorsal glide mobilizations have been suggested to influence the posterior capsule of the glenohumeraal joint [36].
Little scientific evidence is available regarding the effectiveness of these techniques, nor the possible influence of these stretching protocols on impingement symptoms [15], [24]. Therefore, the present study aimed to compare angular and non-angular stretching techniques for improving passive internal rotation ROM of the glenohumeraal joint in asymptomatic and symptomatic subjects with GIRD, and also to examine the effects of the two intervention techniques on pain and function in the symptomatic group.
Materials and Methods
Subjects
Sixty athletes (29 males, 31 females) from various overhead sports (volleyball, tennis, squash and badminton) participated in the present study. Thirty of them were asymptomatic, and were recruited from local sports federations; the other athletes were recruited based on chronic shoulder pain (>3 months) and impingement symptoms. All subjects completed questionnaires about their training and athletic performance history, and their history of shoulder pain when applicable. The inclusion criteria for the symptomatic subjects were: (i) participation in overhead sports at competition level; (ii) shoulder pain during daily activity of 2/10, measured on a visual analogue scale (VAS) [11]; (iii) internal rotation ROM deficit of 20°, compared to the non-injured side, measured with a goniometer [1], [37]; and (iv) three positive provocation tests for impingement symptoms [38], [39]. For the asymptomatic subjects, only criterion (i) and (iii) were applicable and, for this population, the dominant/throwing shoulder was tested and treated. Subjects were excluded from both groups in the study if they had a history of dislocation of the shoulder, shoulder surgery, current symptoms related to the cervical spine, or documented structural injuries to the shoulder complex. All demographic and anthropometric data from both subject groups are summarized in Table 1. An independent t-test with alpha set at 0.05 between both groups revealed no significant differences with respect to age (p = 0.62), height (p = 0.78), weight (p = 0.83), and training frequency (p = 0.24). All subjects provided their written informed consent to participate in the study. The study was approved by the Ethical Committee of the Ghent University (registration number BE67020072856).
Demographic data of the subjects in the asymptomatic group (n = 30) and the patient group (n = 30)
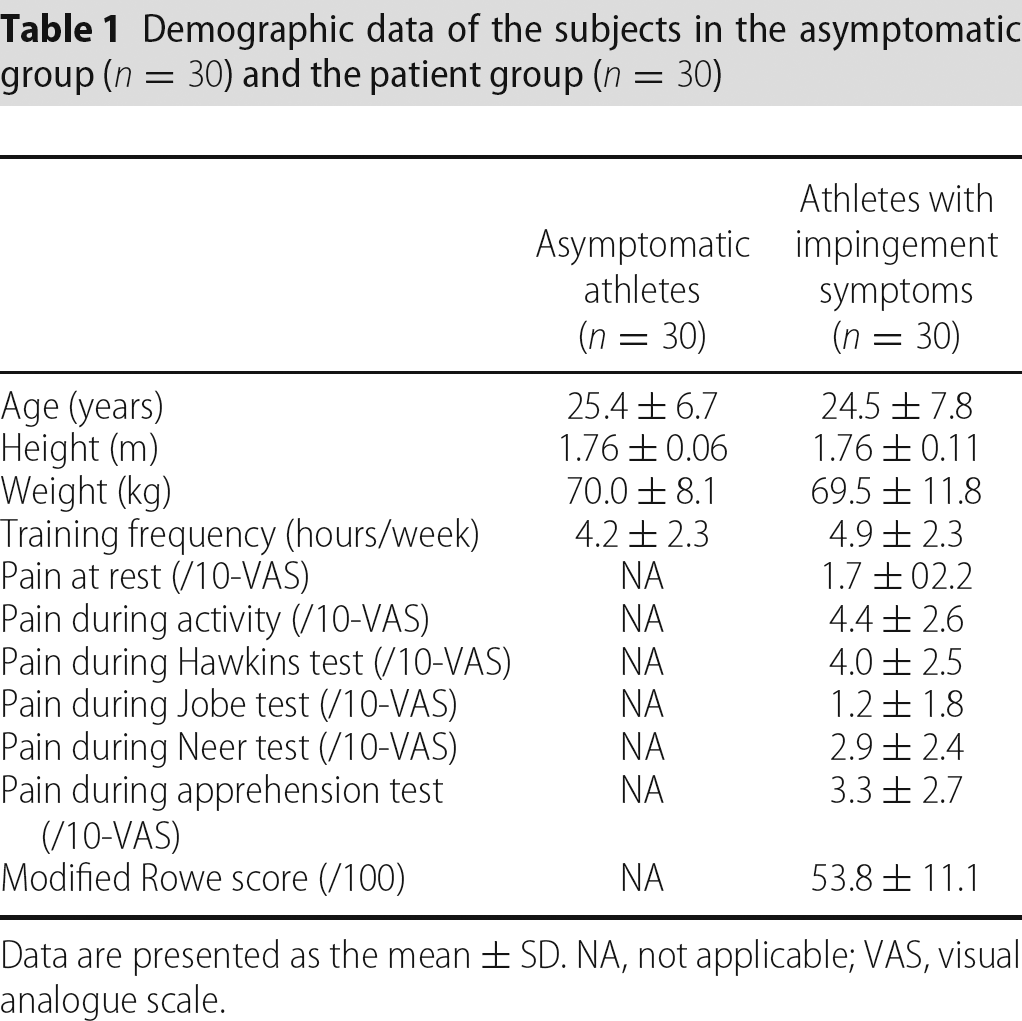
Data are presented as the mean ± SD. NA, not applicable; VAS, visual analogue scale.
Measurement protocol
Before participation, subjects were screened for impingement symptoms and underlying instability, using the tests of Jobe, Hawkins, Neer, and the Apprehension and Relocation tests [38]–[40]. Based on the results of these tests, subjects were allocated into the symptomatic subjects group (minimal three tests positive) or the control group (maximal one test positive).
The pain during the provocation tests was rated using a VAS, with 0 as no pain and 10 as extremely painful. Subjects had to indicate, on a blinded 10-cm line, the amount of pain.
In case subjects were allocated in the symptomatic subjects group, the Modified Rowe score was used to determine the functional capacities [38], [41]. The Rowe score can range from 0 to 100, with lower scores indicating worse function.
Measurements of bilateral passive shoulder internal rotation at 90° of abduction were assessed by one investigator, using a standard goniometer with a bubble lever to control the vertical position of the arm [37]. The order of extremity was randomized before data collection. The same two examiners were involved in the measurement collection: one to position the extremity and one to align and read the goniometer. Subjects were positioned in the supine position. The examiner passively moved the shoulder to the end of ROM, controlling scapular movement by palpation of the coracoid process with the thumb and the spine of the scapula with the fingers [42]. The axis of the goniometer was aligned with the olecranon. The angle between the vertical line and the goniometer arm, aligned along the ulna towards the styloid process, was measured. ROM was determined by calculating the complimentary angle of the measurement. Each measurement was performed twice, and averaged for further analysis. Intraclass correlation coefficients (III3,1) between both trials was 0.83, indicating good intra-rater reliability of our procedure, with a SEM of 3.4°. This procedure, using a standard goniometer to measure ROM of the shoulder, is reported to be reliable, with a rotational measurement error of ± 3° and an ability to detect differences in ROM of 6° [37], [42]–[44].
Study design and procedure
In both groups, subjects were randomly allocated into two intervention groups: (i) an angular stretching group and (ii) a non-angular translation mobilization group.
After initial testing (measurement 1), subjects from both groups were treated for nine sessions over 3 weeks (three times/week) by two trained physiotherapists, who were familiar with the procedures, and instructed by the first author (A.C.). All measurements were repeated after the 3-week treatment period (measurement 2). During the study, all subjects were asked to resume their normal athletic activity if possible, with no additional stretching intervention. In a third testing session (measurement 3), 3 weeks after measurement 2, ROM and, if applicable, VAS scores regarding pain and Rowe scores were repeated. A flow chart of our procedures is presented in Fig. 1.
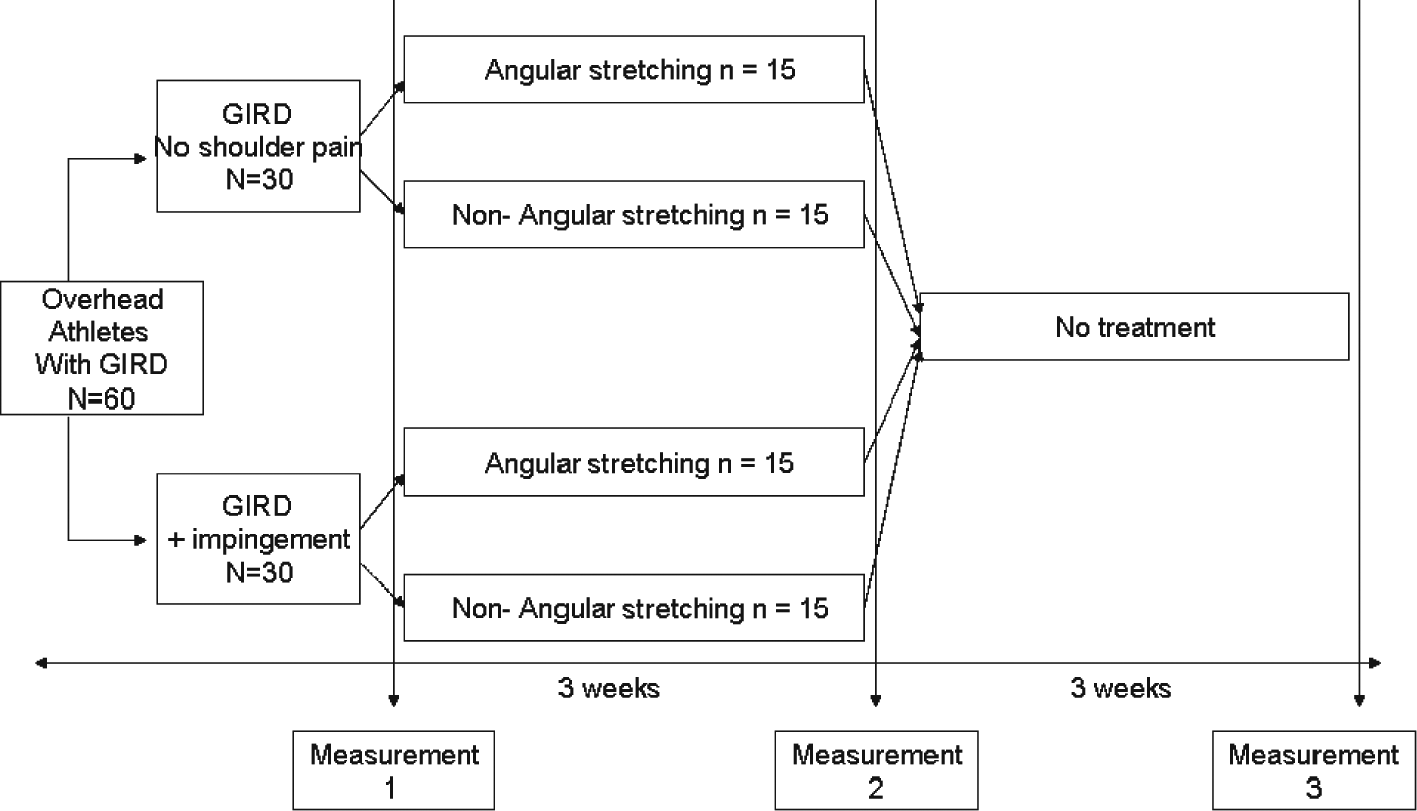
Flowchart of intervention procedures and measurement times. GIRD, glenohumeral internal rotation deficit
Stretching intervention methods
All stretching techniques were performed, in accordance with the description by Cools et al. [16] In the angular stretching group, the ‘sleeper-stretch’ (Fig. 2) and the ‘cross-body-stretch’ (Fig. 3) were performed by the therapist. In the sleeper-stretch, the subject is lying on his injured side with the shoulder in 90° forward flexion and the elbow flexed. When the scapula is manually fixed into retraction, and scapular movement is controlled, glenohumeral internal rotation is performed passively, thus stretching the posterior structures of the shoulder. In the cross-body-stretch, the subject is supine, and the arm is passively moved into horizontal adduction, when the therapist fixes the scapula into retraction. Each stretching technique was sustained for 30 seconds, and was repeated until the subject was treated for 15 minutes.

Sleeper-stretch, performed by the therapist

Cross-body-stretch, performed by the therapist
In the non-angular stretching group, manual translational mobilizations were performed by the therapist. These consisted of high-grade end-range dorsal glides (Fig. 4) and mid-range caudal glides (Fig. 5). The subject's shoulder was positioned into maximal internal rotation, and dorsal glide mobilizations were performed. In the second mobilization technique, high-grade caudal translation mobilizations were performed with the subject's shoulder in 90° of abduction. The latter technique was chosen because there is some evidence that caudal glide techniques might also influence the posterior capsule similar to dorsal glide techniques [45], [46]. Each technique was sustained for 30 seconds and repeated until the subjects were treated for 15 minutes, with a resting time 30 seconds in between techniques.

End-range dorsal glide mobilizations

Mid-range caudal glide mobilizations
Statistical analysis
Descriptive statistics were calculated for all variables, and all dependent variables were controlled for normal distribution and homogeneity of variance using the one-sample Kolmogorov–Smirnov test. Because all ROM data were normally distributed with equal variances, parametric statistics were performed. Differences in internal rotation ROM were analyzed with a general linear model analysis of variance (ANOVA) for repeated measures, in which the within subject factors were side (two levels) and measurement time (three levels). The between subject factors were stretching intervention (two levels) and group (two levels). Alpha for the ANOVA was set at 0.05. Four-way interactions (side × stretching intervention × measurement time × group) were of interest. In case of the absence of significant four-way interactions, three-way interactions and two-way interactions among the variables of interest were explored. Post-hoc analyses were performed using a Bonferroni procedure (α = 0.017) when a significant difference was found with
The data from de VAS and the Modified Rowe score in the symptomatic subjects group were analyzed using nonparametric statistical tests. Initially, a Friedman test was performed, with α set at 0.05. In case of significant differences between the three measurement times, pairwise comparisons were executed using Wilcoxon tests, corrected for multiple comparisons (α = 0.017). Group differences based on stretching intervention were analyzed by a Mann-Whitney U-test. Based on previous literature [15], [24], power analysis was performed on an effect size of 10°. Based on those data, it was estimated that a 10° difference in ROM after stretching could be detected with 80% power at p < 0.05 in a total sample of 56 subjects. All statistical analyses were performed using SPSS, version 16.0 (SPSS Inc., Chicago, IL, USA).
Results
The results of the internal rotation ROM for both groups on both sides and for the three measurement times are summarized in Table 2 and Figs 6 and 7. The
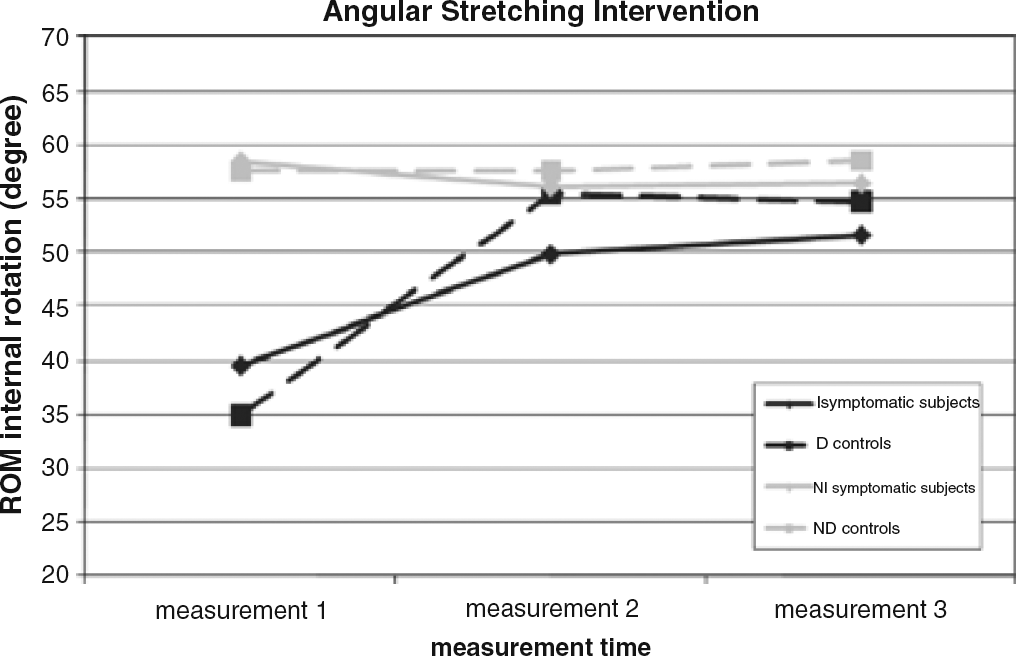
Results of the angular stretching intervention on glenohumeral internal rotation range of motion. I, injured side symptomatic subjects; D, dominant (throwing) side controls; NI, non-injured side symptomatic subjects; ND, nondominant side symptomatic subjects; ROM, range of motion
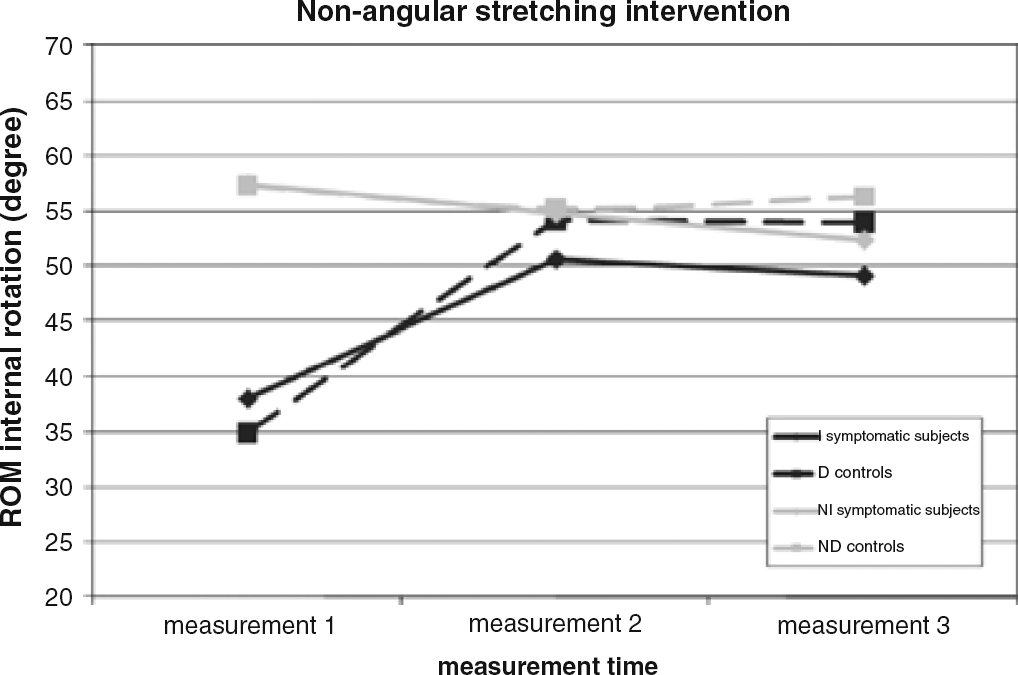
Results of the non-angular stretching intervention on gleno-humeral internal rotation range of motion. I, injured side symptomatic subjects; D, dominant (throwing) side controls; NI, non-injured side symptomatic subjects; ND, nondominant side symptomatic subjects; ROM, range of motion
Mean ± SD shoulder internal rotation range of motion (ROM) (in degrees) for the nondominant (ND)/non-injured (NI) side and the dominant (D)/injured (I) side for the athletes with impingement symptoms (n = 30) and the asymptomatic athletes (n = 30) before treatment (measurement 1), immediately after the treatment regimen of 3 weeks of stretching (measurement 2), and 3 weeks post-treatment (measurement 3)
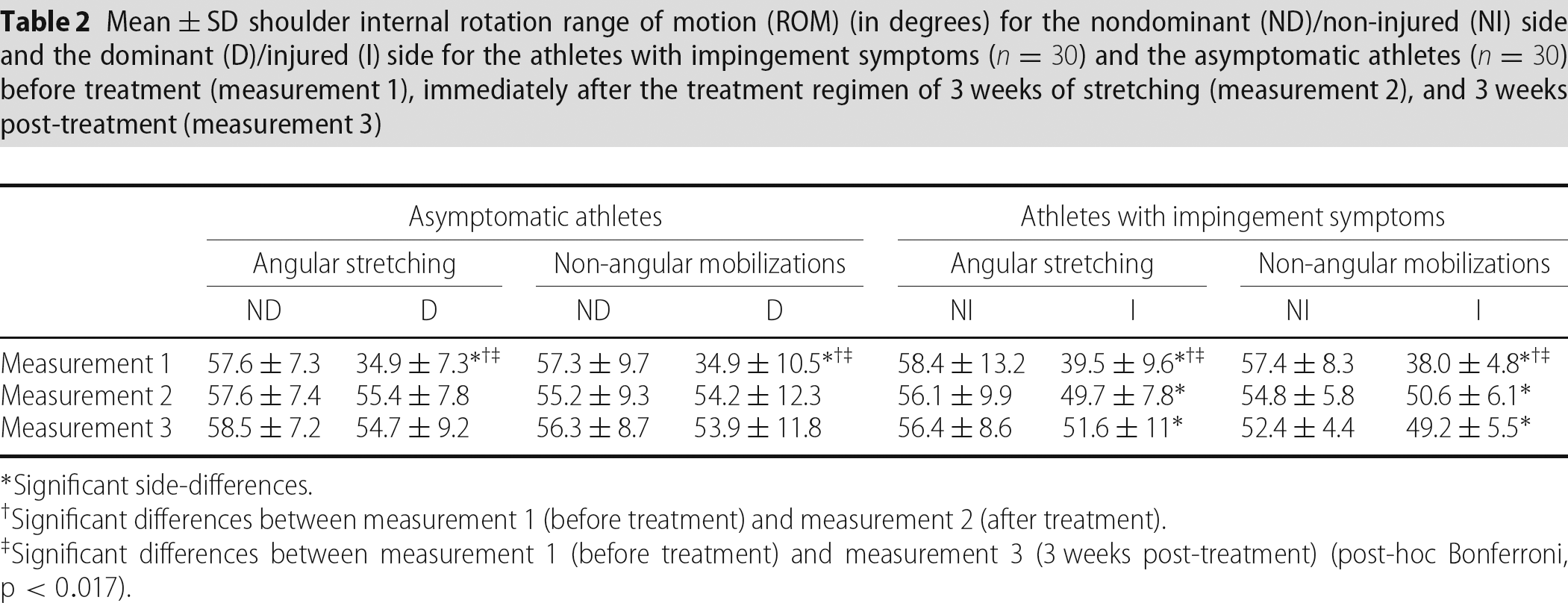
Significant side-differences.
Significant differences between measurement 1 (before treatment) and measurement 2 (after treatment).
Significant differences between measurement 1 (before treatment) and measurement 3 (3 weeks post-treatment) (post-hoc Bonferroni, p < 0.017).
Results based on time (pre-post treatment)
On the injured side of the symptomatic subjects and the dominant side of the controls, a significant increase in internal rotation ROM was found after 3 weeks of stretching (p < 0.017). This gain in ROM remained for 3 weeks without stretching because no significant differences in ROM were found between measurement times 2 and 3.
In the control group, significant side differences were found at initial measurement. However, after 3 weeks of stretching, and at the final measurement time, these differences did not reach statistical significance anymore.
In the symptomatic subjects group, ROM was also significantly different between sides at the first measurement time. Although in both treatment groups, ROM significantly increased, side differences remained statistically significant after the treatment, indicating that ROM was not normalized compared to the non-injured side (p < 0.017).
Results based on stretching intervention method
Post-hoc tests did not reveal any significant stretching intervention differences on the dominant/injured side on any of the three measurement times.
Results regarding pain and functional scores in the symptomatic subjects group
In the symptomatic subjects group, all VAS significantly decreased, with the exception of VAS in rest at measurement time 2, and, during the Jobe test, at measurement times 2 and 3 (Table 3). The Modified Rowe score significantly increased after 3 weeks of stretching, and this increase was confirmed again at measurement time 3. No significant differences were found for the VAS scores or the Modified Rowe score between measurements 2 and 3.
Mean ± SD for the visual analogue scale scores (/10) during rest, activity and during clinical examination, and Modified Rowe score (/100) in the overhead athletes with impingement symptoms (n = 30) before treatment (measurement 1), immediately after the treatment regimen of 3 weeks of stretching (measurement 2) and 3 weeks post-treatment (measurement 3) for both treatment groups (angular stretching + non-angular mobilization)
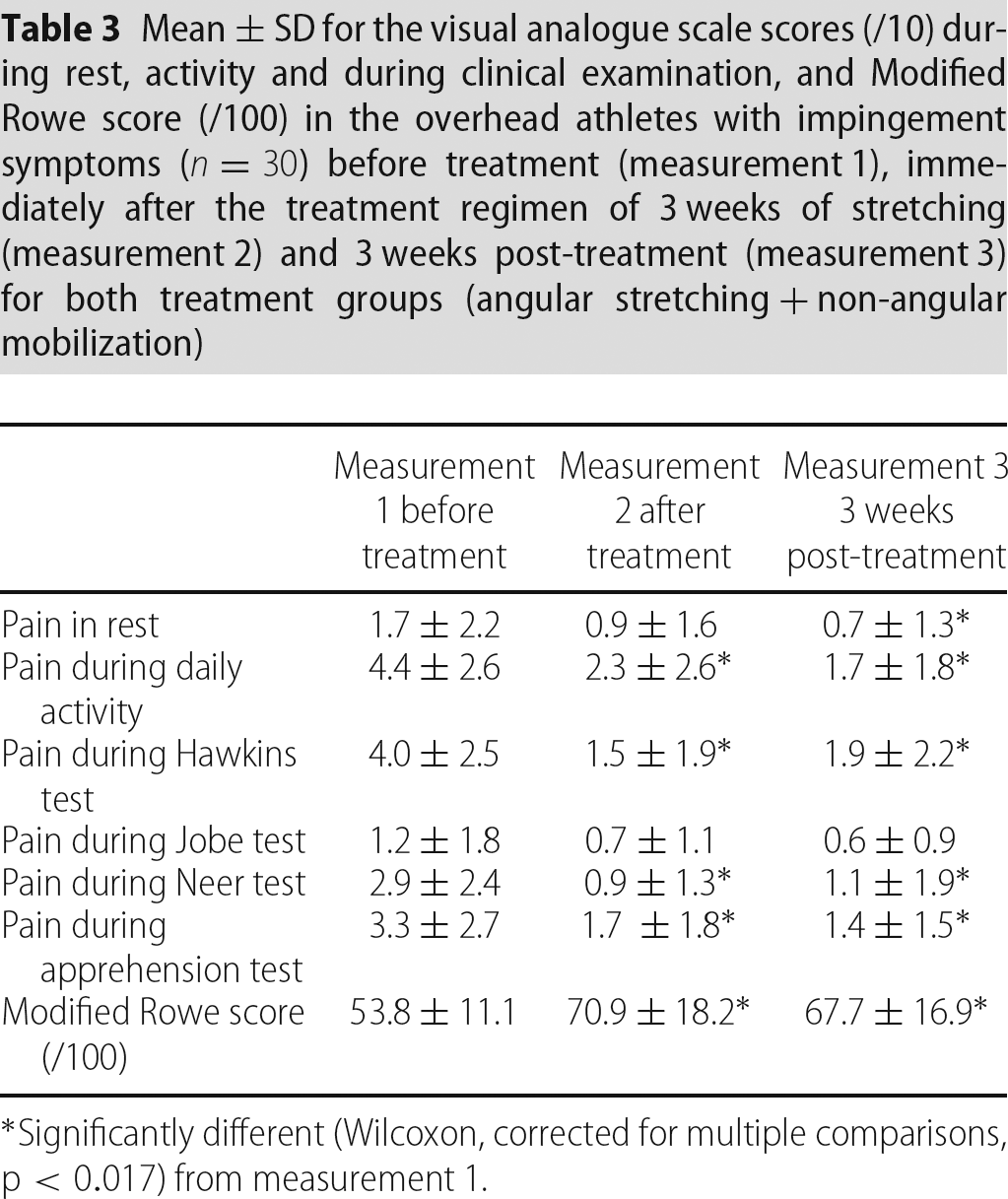
Significantly different (Wilcoxon, corrected for multiple comparisons, p < 0.017) from measurement 1.
Discussion
Despite the importance of maintaining shoulder flexibility in the overhead athlete, little evidence exists regarding the effectiveness of specific stretches that clinicians and athletes use in the prevention and rehabilitation of shoulder injuries.
The present study aimed to compare angular stretching and non-angular joint mobilization techniques in the treatment of GIRD and to apply these stretching techniques on healthy overhead athletes, as well as on overhead athletes with chronic shoulder pain.
Results based on time (pre-post treatment)
A first result that can be derived from the present study is the fact that glenohumeral internal rotation ROM is improved after a 3-week period of stretching, both in the symptomatic subjects as well as in the healthy overhead athletes with GIRD, and also in the angular treatment group as well as in the translation mobilization group. Our results support the previously reported results of stretching regimens in overhead athletes, and are of clinical relevance, in view of the intraclass correlation and SEM found in the pilot study regarding the ROM measurements [15], [22], [24], [33]. Moreover, the effects of stretching appear to remain over a period of 3 weeks after the stretching intervention. Laudner et al. demonstrated that the sleeper-stretch resulted in significant acute increase in glenohumeral ROM and posterior shoulder motion [33]. However, the clinical relevance of their results was questioned. Indeed, only an increase of 3.1° was found immediately after two repetitions of 30 seconds of stretching, performed by the therapist. Recently, Tyler et al. found an association between correction of posterior shoulder stiffness with symptom relief in patients with impingement[15]. Lintner et al. showed, in their retrospective study, that professional pitchers who underwent an internal rotation stretching programme for more than 3 years had significant more internal rotation ROM (+20°) compared to pitchers enrolled in a stretching programme for less than 3 years [22]. In the present study, the increase in ROM varies from 11.2 to 12.1 in the symptomatic subjects group to 19 to 19.8 in the control group. McClure et al. compared both stretching techniques in asymptomatic subjects, and found an increase of 20° after 4 weeks performing the cross-body-stretch, and 12.4° after performing the sleeper-stretch [24]. The results of the present study are partially in agreement with the results of McClure et al.[24]; however, differences in subjects recruitment, treatment procedure and stretching interventions make any comparisons between both studies difficult. It must be noted that, despite the fact that differences were not statistically different, the healthy athletes gained more ROM than the symptomatic subjects, regardless of the stretching intervention. Possibly symptomatic subjects were less responsive to the treatment, or the dose of treatment provided. Based on the results of the present study, however, it is impossible to define the possible cause of these differences.
Results based on stretching intervention method
No significant differences were found between both stretching techniques, neither in the symptomatic subjects group, nor in the healthy overhead athletes. It appears that angular stretching as well as non-angular translation mobilizations are effective for the reduction of a glenohumeral internal rotation deficit. Based on the specific action of both treatment techniques, the literature suggests that angular techniques possibly influence the posterior muscle–tendon units [5], whereas non-angular mobilization techniques, specifically the dorsal glide technique, possibly stretch the posterior capsule [34]. Izumi et al. [47] showed that a position of 30° of extension and internal rotation increases the strain on the upper and lower parts of the posterior capsule, possibly explaining our results, whereas a position of flexion, horizontal adduction and internal rotation results in a more global stretch of the posterior capsule according to a study by Borstad and Dashotter [48]. However, in view of the results obtained in the present study, it is not possible to derive conclusions regarding possible tissue-specific effects of stretching, and, based on our results, clinicians should use both stretching techniques in the treatment of GIRD. In addition, the value of proprioceptive neuromuscular facilitation techniques was not explored in the present study. Previous studies showed a significant increase in shoulder ROM after a 6-week proprioceptive neuromuscular facilitation stretching programme in overhead athletes [49].
The present study aimed specifically to evaluate the effect of passive stretching and mobilization techniques on shoulder ROM. However, the clinician should keep in mind that, besides normalization of ROM by stretching the tight and shortened structures, strengthening of the surrounding musculature, in particular scapular retractors and glenohumeral external rotators [16], might increase the endurance of these muscles that are eccentrically loaded during throwing, hence decreasing the deceleration load on the shoulder capsule.
Results regarding pain and functional scores in the symptomatic subjects group
In the symptomatic subjects group, besides changes in flexibility, pain and functional outcome scores were also assessed. The Modified Rowe score, which is widely used in the assessment of functional outcome in overhead athletes [41], significantly increased after 3 weeks of stretching. However, it should be noted that no full return to sport (Modified Rowe score of 70.9/100) was achieved after 3 weeks of stretching. Possibly, patients should be instructed to stretch a longer period because, after 3 weeks of rest after the stretching intervention, there is no spontaneous increase in the functional score.
All VAS results, with the exception of the pain assessment score during the Jobe test, significantly decreased after 3 weeks of stretching, demonstrating an overall pain reduction. Farrar et al. showed that a reduction of approximately two points or a reduction of approximately 30% represents a clinically important difference [50]. However, because we did not include a nontreatment placebo control group, we cannot conclude that reducing flexibility deficits may be responsible for symptom reduction in overhead athletes with impingement symptoms.
Limitations
One limitation of the present study was the use of a treatment intervention in asymptomatic athletes, in which a therapist performed the stretching techniques. In view of the fact that athletes are often encouraged to perform self-stretches in their injury prevention programme, treatment strategies in which the manual intervention of a therapist is obligatory are less clinically relevant in this population. Moreover, our treatment regimen consisted of a 15-minute stretching protocol; possibly, a healthy overhead athlete will not comply with this long period of stretching before or after a training session. In addition, the short- and long-term value of stretching should be explored not only in overhead athletes with a moderate participation in overhead activity, as in the present study, but also in professional athletes, having much higher exposure to throwing or smashing activities. A second limitation is the relatively short period of follow-up after the stretching intervention, as well as the fact that we did not include a control group in the present study (i.e. comprising individuals not undergoing any treatment). Although the results obtained in the present study are promising regarding the middle-term effects of stretching, the extrapolation of the results to a longer-term follow-up should be performed with caution. Moreover, future studies should also investigate the effect of stretching on the incidence and prevention of shoulder injuries in the athletic population.
Conclusions
The results obtained in the present study indicate that both angular and non-angular stretching techniques should be used in the treatment of GIRD, and that this treatment regimen results in an improvement of ROM, impingement-related pain scores, and functional status in the overhead athlete with impingement symptoms.
The authors would like to thank Katrien De Meulenaere, Sarah Fissers, Leen Verhaeghe, Kristien Depluverez and Yara Delagrange for their assistance in the acquisition of the data and data-analysis.