
Abstract
Severely displaced glenoid fractures require open reduction and internal fixation to avoid chronic instability or degenerative changes. Arthroscopic techniques potentially facilitate accurate fracture reduction and fixation without the need for extensive surgical dissection. We report three male patients (mean age 26 years; range 17 years to 40 years) who underwent arthroscopically-assisted reduction and internal fixation for a displaced Ideberg type III (two cases) or IV glenoid (one case) fracture. Cannulated, partially-threaded screws were inserted percutaneously via a superior approach just anterior to the clavicle in all cases. Patients were assessed postoperatively with serial radiographs and clinically using the Constant–Murley shoulder score (0 points to 100 points) at 1 year. There were no recorded complications of surgery, and all fractures united within 3 months. At 6 months, all patients returned to their previous levels of activity and regained an excellent range of motion. The mean Constant–Murley shoulder score at 1 year was 95 points (range 94 to 96), and there was no radiological evidence of arthrosis. Arthroscopic fixation of transverse-orientated glenoid fractures can have excellent functional results, and percutaneous screw insertion via a superior approach appears to be a safe and reproducible technique.
Introduction
Intra-articular glenoid fractures are rare, comprising approximately 0.1% of all fractures [1], [2]. Most glenoid fractures are relatively nondisplaced and are treated non-operatively [3], [4]. However, severe displacement is associated with chronic instability and degenerative joint disease [5]–[8]. The criteria for operative intervention include displacement of the glenoid >10 mm, articular steps >5 mm and persistent subluxation of the humeral head [5], [8]–[13]. Open reduction and internal fixation is currently recommended for such injuries, although, recently, arthroscopy has facilitated percutaneous fixation. Potential advantages over open surgery include accurate fracture reduction without the need for major soft tissue dissection. We report the results and functional outcome of a series of three patients with transverse Ideberg type III or IV [5], [6] glenoid fossa fractures treated with arthroscopically-assisted reduction and percutaneous internal fixation.
Case Reports
Patient 1
A 22-year-old, right-hand-dominant office worker was an unrestrained rear seat passenger in a high-speed motor vehicle accident. The patient presented with a posterior dislocation of the right glenohumeral joint. Conventional radiographs showed a transverse, intra-articular Ideberg type III glenoid fracture. The shoulder was reduced under sedation but was grossly unstable. Computed tomography (CT) scan reconstructions were obtained to further define the fracture pattern and to plan surgery. The intra-articular glenoid fracture was severely displaced and comminuted, with clinical and radiographical evidence of instability. Arthroscopically-assisted percutaneous cannulated screw fixation (see below) was performed 10 days after surgery.
Patient 2
A 17-year-old, right-hand-dominant male mechanic presented with a left shoulder injury after falling off a motorized scooter travelling at approximately 48 km/hour. Conventional radiographs of the shoulder revealed an Ideberg type III, transverse intra-articular fracture of the left glenoid. CT images with three-dimensional reconstruction (Fig. 1A) showed displacement >5 mm. There was no radiographical evidence of glenohumeral instability. Six days after the injury, the fracture was stabilized via arthroscopically-assisted percutaneous cannulated screw fixation (see below) (Fig. 1B, C).
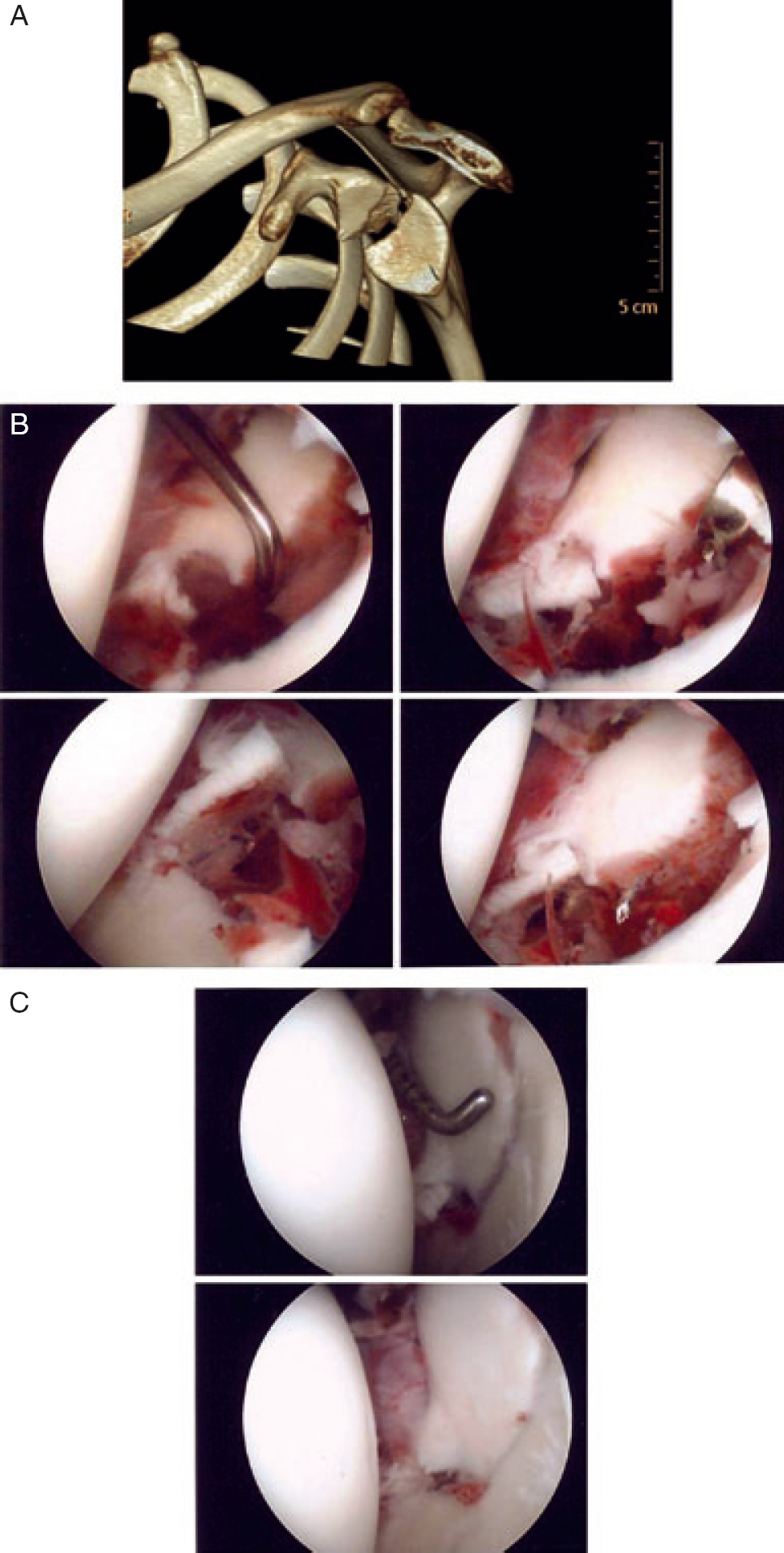
Patient 2. (A) Computed tomography with three-dimensional reconstruction showing an Ideberg type III glenoid fracture. Arthroscopic images showing the appearance of the glenoid before (B) and after (C) reduction and percutaneous fixation
Patient 3
A 40-year-old, right-hand-dominant business man fell off his bicycle and sustained an isolated right shoulder injury. Radiographs and a subsequent three-dimensional reconstructed CT image (Fig. 2A) confirmed an Ideberg type IV, T-shaped fracture of the right glenoid. The main fracture line was transverse, revealing the fracture gap to be approximately 5 mm. The vertical fracture extension was nondisplaced. The patient underwent arthroscopic fixation 21 days after sustaining the injury (Fig. 2B–D).
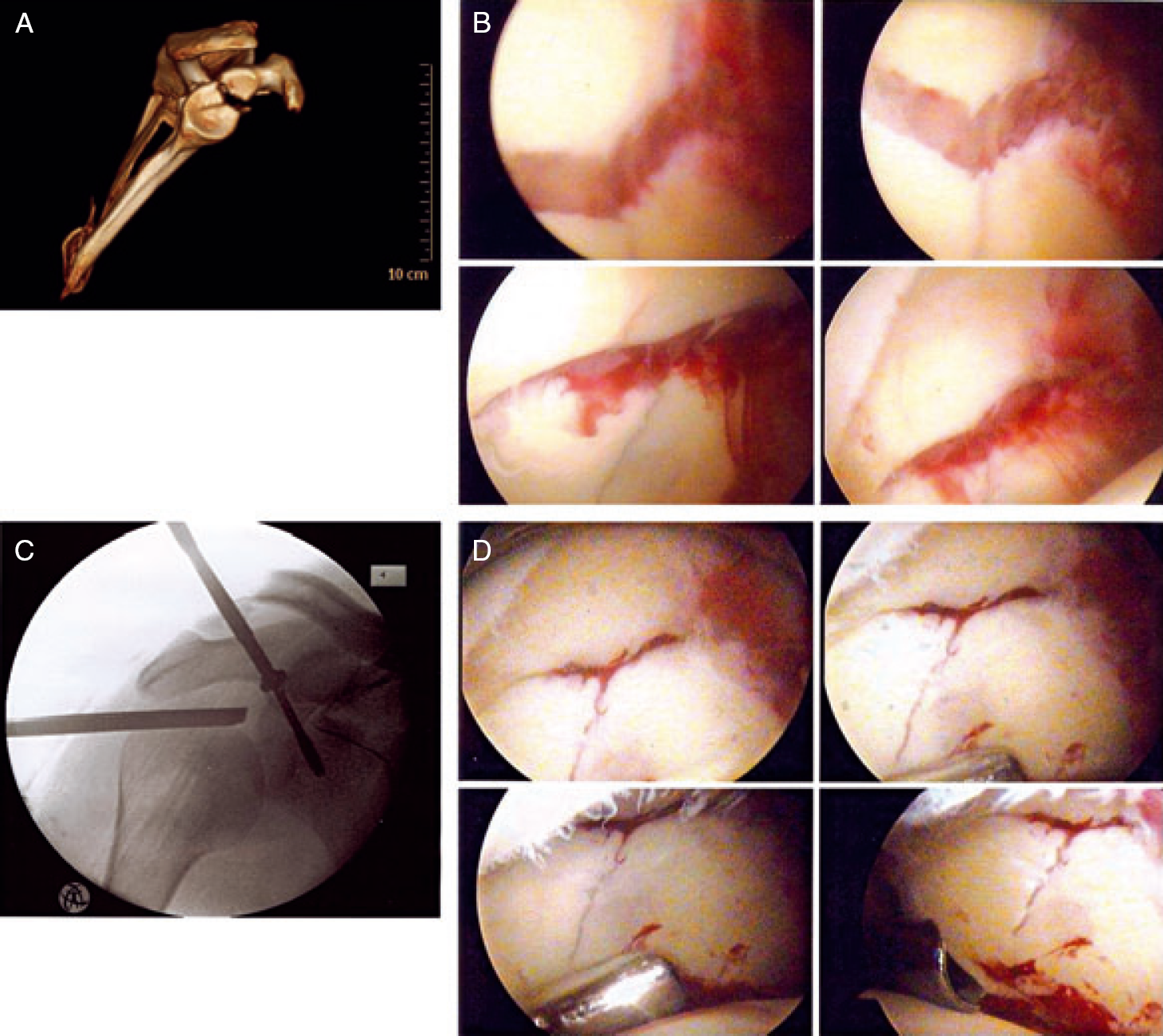
Patient 3. (A) Computed tomography with three-dimensional reconstruction showing an Ideberg type IV glenoid fracture; the vertical fracture line is nondisplaced. (B) Pre-operative arthroscopic images of the glenoid. (C) An intra-operative fluoroscopic image taken during screw insertion. (D) Arthroscopic images after reduction and percutaneous fixation
Surgical technique
For the arthroscopically-assisted percutaneous internal fixation, patients were placed in a beach-chair position using a 30° arthroscope (Karl Storz Endoskope, Tuttlingen, Germany). Two standard arthroscopy portals (posterior and anterosuperior) were used. An arthroscopy pump was used, with the pump pressure set initially at 50 mmHg. Conservative use of short bursts of higher pressures maintain optimal visualization at the same time as limiting extravasation of fluid. The use of cannulae with outflow also limits fluid extravasation into soft tissues. After washout and debridement of the haemarthrosis, the glenoid fracture was clearly visualized (Figs 1B and 2B). Loose flaps of damaged articular cartilage were removed. In patient 1, a small posterior rim fracture was noted.
For each fracture, the optimal direction for screw placement had been established with the CT scan reconstructions (Fig. 1A, B). Images can be manipulated to allow the viewer to look directly down on the glenoid from above and determine the perpendicular angle of screw insertion. This also allows assessment of possible bony obstructions, such as the clavicle, coracoid and acromion. For all patients, CT confirmed that the screws could be inserted perpendicular to the main fracture line by approaching the glenoid from a superior direction, entering the skin just anterior to the clavicle. Pre-operatively, the senior author also used a dry bone skeleton to help determine the orientation of screws and approximate screw lengths required.
Visualizing the glenoid via the posterior portal, a temporary 1.25-mm Kirschner wire (K-wire) was inserted through the anterosuperior portal, entering through the rotator interval. The wire was viewed arthroscopically entering the fracture site through the superior fragment. This wire was used to ‘joystick’ the fracture into a reduced position and then advanced into the inferior portion of the glenoid. A K-wire was inserted into the glenohumeral joint and positioned parallel to the glenoid articular surface to determine the orientation of the glenoid and to aid subsequent guidewire insertion. Via a percutaneous approach just anterior to the clavicle and medial to the acromioclavicular joint, two 1.25-mm guide wires were inserted, perpendicular to the fracture. These wires entered the superior glenoid just anterior to the long head of biceps insertion. Stripping of soft tissues was not required. An image intensifier was used during the procedure to confirm the position of the guidewire. The fluoroscopy C arm was positioned on the same side of the patient as the operated arm, which facilitated an ‘over-the-top’ anteroposterior view, a modified axial view and an axillary lateral view. If there was any doubt regarding screw or wire position, various oblique images were taken. Subsequently, a cannulated drill was used, and two 50-mm long, 3.5-mm partially threaded cannulated screws (Synthes, Inc., Bettlach, Switzerland) were inserted, compressing the fracture.
In patient 1, the fracture gap could be closed only to 3 mm after screw insertion, although there was no visible articular step. The small posterior rim fracture was not stabilized because there was no evidence of posterior instability after fixation of the primary transverse fracture. In patient 2, complete fracture reduction was achieved (Fig. 1C). In patient 3, a single screw was inserted, which resulted in stable fixation in a good position; therefore, a second screw was not inserted (Fig. 2D).
Postoperative management
A Polysling (Seton Healthcare Ltd, Oldham, UK) was applied with restriction of active movements for 6 weeks. All patients were discharged the day after surgery and were seen in the fracture clinic after 2 weeks. For patients 2 and 3, gentle rotation was commenced at 4 weeks. However, patient 1 was placed into a DonJoy external rotation brace (DJO UK Ltd, Guildford, UK) for 6 weeks because of the presence of posterior instability pre-operatively and the small posterior rim fracture. All three patients commenced supervised physiotherapy at 6 weeks with unrestricted rehabilitation.
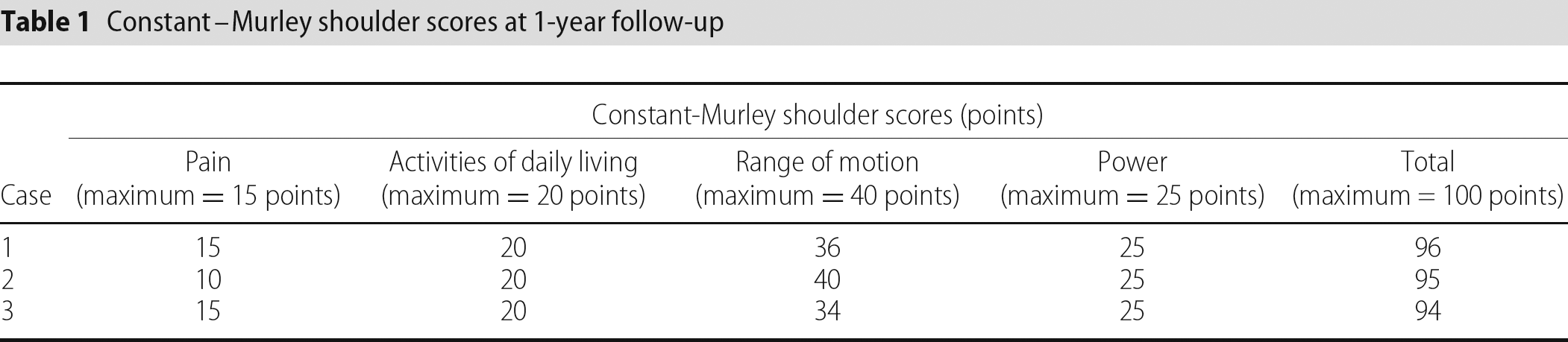
Anteroposterior and lateral radiographs were taken at 2, 6 and 12 weeks and 1 year after surgery. Patients were assessed clinically at regular intervals in the fracture clinic, and at 1 year with the validated Constant–Murley shoulder score (Table 1) [14], [15].
Constant–Murley shoulder scores at 1-year follow-up
Outcomes
Follow-up radiographs revealed that adequate fracture reduction was maintained at 6 weeks in all patients (Fig. 3). At 12 weeks, all three patients had complete radiographical union and were able to achieve 130° of forward flexion and 90° of abduction without major discomfort. At 6 months, all patients had returned to work and stated that they were able to undertake all their previous activities without disability or major discomfort. The Constant–Murley shoulder scores obtained at 1 year (Table 1) showed excellent scores for all patients. There was no clinical evidence of glenohumeral instability and, at 1 year, all patients had regained virtually full motion (Fig. 4) and excellent function. Final radiographs at 1 year did not show any evidence of secondary arthrosis.

Sample postoperative radiograph (patient 2) showing screw position and maintenance of fracture reduction at 6 weeks

Clinical photographs showing range of motion at 1 year for patients 2 (A) and 3 (B)
Discussion
Glenoid fractures with considerable displacement lead to a risk of chronic instability and degenerative joint disease [5]–[8]. The aims of surgery are to achieve anatomical reduction of the glenoid articular surface and to regain glenohumeral stability. Arthroscopic fracture treatment of the shoulder was first described by Gartsman and Taverna [16] and, subsequently, procedures such as arthroscopic repair of glenoid rim fractures have become well established [17]–[20]. To our knowledge, the present study represents the first series of transverse glenoid fractures to be treated successfully with arthroscopically-assisted percutaneous fixation.
The importance of an articular step on long-term glenohumeral function remains relatively unclear because of a lack of long-term follow-up studies [7], [10]. However, one study has shown that glenoid fractures with an articular step of >2 mm are associated with advanced arthrosis [10], and most studies consider the risk of joint degeneration to be high for intra-articular fractures with a step ≥5 mm [5], [8], [10]–[12], [21]. Residual joint congruity <2 mm appears to have good to excellent outcomes in the majority of patients [8], [12], [21]. All three of our patients had clear indications for surgical intervention: all had >5 mm of displacement (creating a large gap at the fracture site), two had considerable articular step-offs and one had posterior glenohumeral instability. In patients 2 and 3, complete fracture reduction was achieved. For patient 1, the articular step-off was corrected, although a 3-mm gap remained at the fracture site after fixation. This patient regained full function with no radiographical evidence of arthrosis at 1 year. The excellent clinical results of the patients in this small series are comparable with the reported results of patients treated with open reduction and internal fixation, with the advantage of low operative morbidity compared to that of open surgery [1], [3], [5], [22].
The results of arthroscopic treatment of transverse-orientated glenoid fractures have been limited to two case reports [23], [24]. One report indicated a good outcome after percutaneous external fixation of a Y-shaped glenoid fracture using Kirschner wires [23]. Yallapragada et al. attempted arthroscopically-assisted external fixation of a comminuted transverse glenoid fracture with a 7-mm articular step using wires [24]. The fixation failed early, requiring percutaneous fixation using a single 3.5-mm cannulated screw inserted from anterosuperior to posteroinferior via the anterosuperior portal. Yallapragada et al. reported difficulty in achieving perpendicular orientation of the guidewire for the fracture and stated that this difficulty was the reason for not attempting internal fixation at the initial surgery [24].
Our clinical series shows that a superior approach just anterior to the clavicle provides adequate access for the transverse glenoid fracture. Another option for superior screw insertion is to enter the glenoid via the portal described by Neviaser [25], entering the soft spot bounded by the clavicle anteriorly, the spine of the scapula posteriorly and the acromion laterally. A recent cadaveric study attempted to define the safe zones of percutaneous wire insertion [26], showing that the glenoid is accessible between the clock times of 07:40 (posteriorly) and 02:50 (anteriorly), via posterior, Neviaser's, anterosuperior and anterior approaches. Such a study aids pre-operative planning. In combination with conventional radiographs, 3D reconstructive CT scanning proved to be invaluable for assessing the configuration of the glenoid fractures when aiming to determine the most effective surgical approach. Bony obstructions such as the coracoid [26], [27] and acromion [26] may prevent perpendicular screw placement for obliquely-orientated fracture patterns. Severe comminution may be technically challenging, although it is not an absolute contraindication [17], [28]. Chronic lesions are generally best treated with open surgery [18], and we would usually not consider arthroscopic fixation for fractures older than 4 weeks.
Risks of percutaneous wire or screw insertion include neurovascular injury. The most relevant structures for screw insertion from a superior direction are the suprascapular artery or nerve, although percutaneous wire insertion via Neviaser's portal and an anterosuperior approach appears to be relatively safe with regard to these structures [26]. It has been suggested that a delay of 5 days to 7 days reduces the risk of other surgical complications such as extravasation of fluid and compartment syndrome [22]. In our series, the mean time to surgery was 12 days (range 6 days to 21 days), representing the time required to perform pre-operative investigations for the glenoid fracture and for associated injuries to reduce anaesthetic risk. We would agree that a short delay to surgery is sensible.
Conclusions
The potential advantages of arthroscopic treatment of glenoid fractures are clear, and there is growing evidence in the literature to support arthroscopic fixation for a range of glenoid fracture configurations. All patients in our series regained excellent function at 1 year after fixation of displaced transverse glenoid fractures. Additional research is required to determine the safety of percutaneous screw insertion and also the feasibility of percutaneous fracture fixation via other anatomical approaches for large oblique and vertical fracture orientations.