
Abstract
Background
Shoulder pain is a common problem and disorders of the rotator cuff are considered to be the commonest cause of this pain. Despite this, there is a paucity of high-quality research upon which to base practice. There is a clear need to determine the range of current practice as a basis upon which to inform future research.
Objectives
To describe current physiotherapy practice in relation to the assessment and management of rotator cuff disorders and to gain an insight into the perceived research needs of physiotherapists in the UK.
Methods
An electronic survey was developed and responses were sought in relation to a case report considered to represent a patient with a typical rotator cuff disorder.
Results
A total of 110 surveys were completed. The respondents stated that they would undertake a range of diagnostic tests, offer a wide variety of interventions and offer a broad prediction of prognosis.
Conclusion
Current physiotherapy practice in relation to rotator cuff disorders is variable, which might reflect the lack of high-quality evidence available. There is a clear need for high-quality research to inform physiotherapy practice in this burdensome area.
Keywords
Introduction
Shoulder pain is one of the most common musculoskeletal symptoms with a prevalence estimated at between 16% and 26% in the general population [1], [2]. It is the third most common primary care musculoskeletal presentation [3] and the third most common reason for consultation with a physiotherapist [4]. Impaired shoulder function impacts significantly upon activities of daily living, including eating, dressing and working [5].
Disorders of the rotator cuff are considered to be the commonest cause of this pain [6]. Long-term outcome is frequently poor for a significant proportion of patients, which means that many might subsequently be exposed to more invasive and costly treatment options (e.g. injections, surgery) and/or long-term pain and disability [7].
Shoulder pain, incorporating rotator cuff disorders, is a significant burden to the National Health Service (NHS) and society. It has been identified that approximately 1% of adults in the UK consult their general practitioner with a new presentation of shoulder pain each year. This amounts to over 500,000 adults. Costs in the first 6 months after primary care contact have been estimated to be €690, which means that costs attributable to this problem are in the region of €345 million or £310 million per year (i.e. a significant economic burden). Almost 50% of this cost is attributable to sick leave from paid employment [8]. This is an important health and social care problem for patients, clinicians, commissioners and researchers to consider.
Despite the commonality and burden of rotator cuff disorders, there are a lack of high-quality studies upon which to base practice [9]. Numerous systematic reviews have been undertaken in relation to the various plausible interventions, including exercise, corticosteroid injections and surgery, although all identify the insufficiency of the evidence base when attempting to draw conclusions [10]–[15].
There are a wide variety of physiotherapy treatment approaches that might be applied during the management of rotator cuff disorders but, as far as the authors are aware, no previous studies have formally investigated physiotherapy practice for rotator cuff disorders. In light of the limited evidence in this area, there is a clear need to determine the range of current practice to inform future research. Hence, the present study aimed to describe current physiotherapy management of rotator cuff disorders and gain an insight into the perceived research needs of physiotherapists in the UK.
Materials and Methods
An online survey was developed by the authors (Appendix 1) with initial reference to previously published surveys of practice of shoulder disorders [16], [17]. This draft version of the survey was distributed via informal professional networks available to the authors. The participants, with a range of experience, were asked to complete the survey and then feedback in relation to the content, format and general suitability of the measure. Based upon the pilot phase responses to the survey and feedback, some minor modifications were made in relation to the range of possible interventions that a physiotherapist might offer, whether questions were open/closed, the space available to answer the question where text was requested, and the fact that one question was regarded as leading such that the wording was modified to prevent this.
As a basis upon which to answer the questions, a brief case report was presented at the outset of the survey. This vignette was based upon a previously published case report [18] which was developed with reference to current literature [19] as follows:
‘A 57-year-old gentleman presents with a 12-month history of pain affecting the left shoulder. The onset was insidious and the problem is unchanging over time. The symptoms are intermittent and consistently produced with lifting, elevating the arm, reaching behind the back or lying on the left side. Symptoms ease with rest. He is medically well. He continues to work as a printer which involves regular lifting above and below shoulder level.
Observation of the patient is unremarkable. There was no pain at rest. Cervical range of movement is full and testing does not provoke any shoulder pain. There is a full range of active and passive movement at the left shoulder but there is an arc of pain provoked between 80° and 120° during active abduction. Scapulo-humeral rhythm was defined as normal during active movement testing. Pain was also provoked during isometric abduction and lateral rotation with associated mild weakness. The Hawkins–Kennedy impingement test was positive.’
Although the lack of diagnostic accuracy with regard to rotator cuff disorders is well recognized [20], [21], the authors felt that the case report reflected current thinking with regard to symptoms and signs that might currently be regarded as attributable to rotator cuff pathology by physiotherapists [18], [19].
The final version of the survey was hosted by Survey Monkey (http://www.surveymonkey.com). An invitation to complete the survey and link/contact details of the lead author was posted on the interactive Chartered Society of Physiotherapy (iCSP) website and was available for a period of 4 weeks between June and July 2011. All chartered physiotherapists in the UK have access to iCSP. The only inclusion criteria were that respondents should have some experience of treating patients with rotator cuff disorders. The decision relating to eligibility was left to the discretion of the participants.
Statistical analysis
Descriptive statistics for all respondents, those with a self-determined special interest in rotator cuff disorders (SI) and those with no special interest (NSI) were generated by Survey Monkey and subsequently imported into Microsoft Excel (Microsoft Corp., Redmond, WA, USA) to facilitate development of the associated figures and tables. Where responses appeared to differ by level of interest, the difference in the proportion of respondents between groups was analyzed using chi-square tests, which was undertaken using SPSS, version 17 (SPSS Inc., Chicago, IL, USA).
Text responses were summarized by one author (CL) and subsequently independently verified by two authors (AL, JM).
Results
In total, 110 surveys were completed. Where appropriate, Table 1 displays the descriptive data (actual count) from the survey.
Descriptive survey data
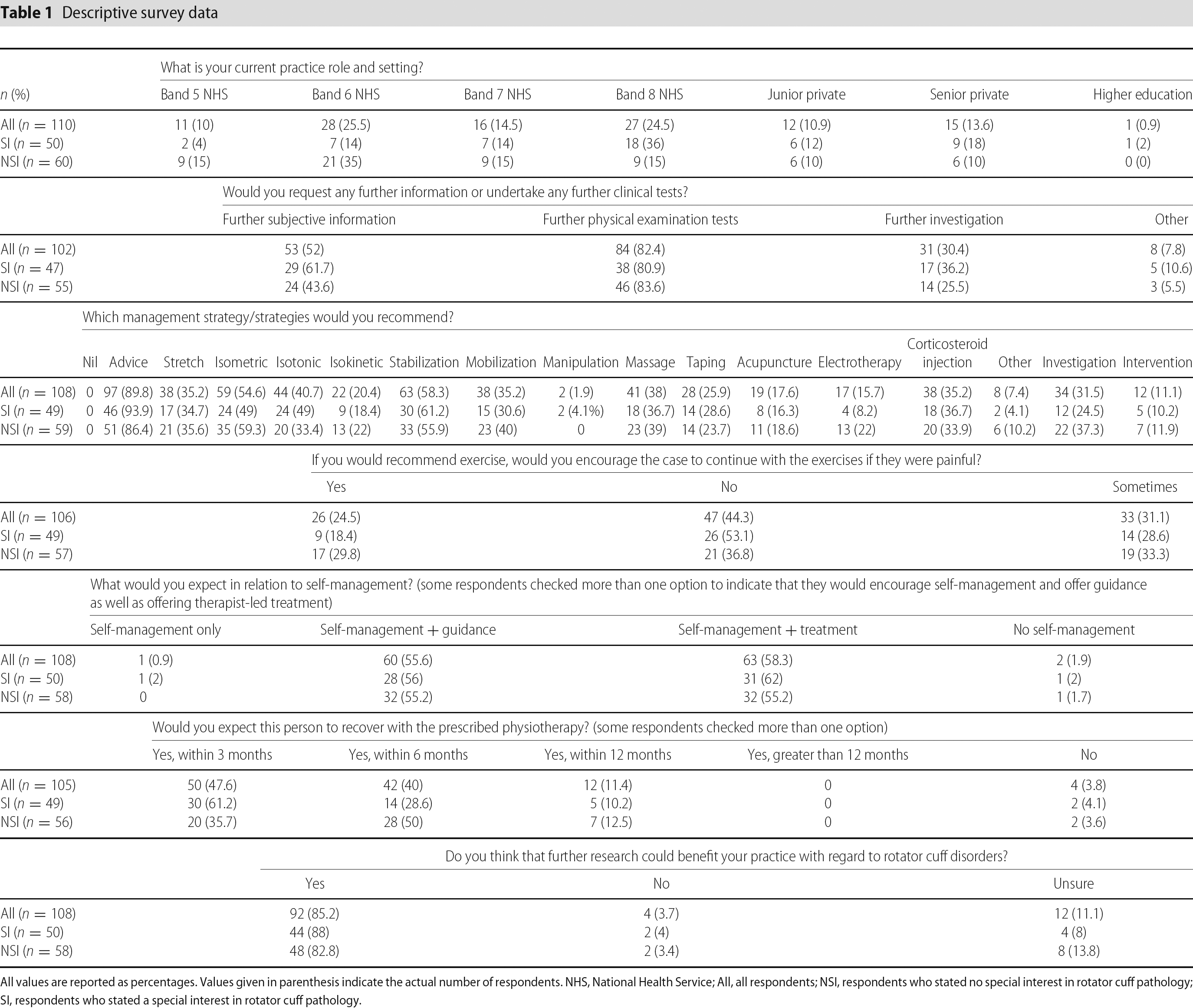
All values are reported as percentages. Values given in parenthesis indicate the actual number of respondents. NHS, National Health Service; All, all respondents; NSI, respondents who stated no special interest in rotator cuff pathology; SI, respondents who stated a special interest in rotator cuff pathology.
1. Do you have a special interest in rotator cuff disorders?
Fifty-one respondents indicated that they had a special interest in rotator cuff disorders (SI) and 60 indicated that they did not have a special interest in rotator cuff disorders (NSI). For reasons that are unclear, one participant checked both options. For pragmatic reasons, this dataset was maintained but, as a result of the uncertainty associated with such a response, this participant was regarded as NSI for the purpose of further analysis (n = 110).
2. Please briefly describe your current role(s) and practice setting(s).
One hundred and 10 (50 SI; 60 NSI) respondents completed this question. The respondents undertook a wide range of predominant current roles within a variety of practice settings. There were a greater proportion of NHS band 5 (15% versus 4%) and 6 (35% versus 14%) physiotherapists in the NSI group, whereas NHS band 8 was more prevalent in the SI group (36% versus 15%). This difference in the proportion of grades between the groups classified as SI and NSI groups was statistically significant (χ2 = 15.52 p = 0.017).
3. Before you suggest a management strategy, with reference to the above case, would you request any further information or undertake any further clinical tests?
One hundred and two (47 SI: 55 NSI) respondents completed this question. Figure 1 indicates the percentage of respondents who would request further information or undertake/request further clinical tests. The difference in the proportion of respondents with a SI who would gather further subjective information was significantly different from those regarded as NSI (χ2 = 4.23 p = 0.04). Otherwise, the responses between the SI and NSI groups were not significantly different (p < 0.05).
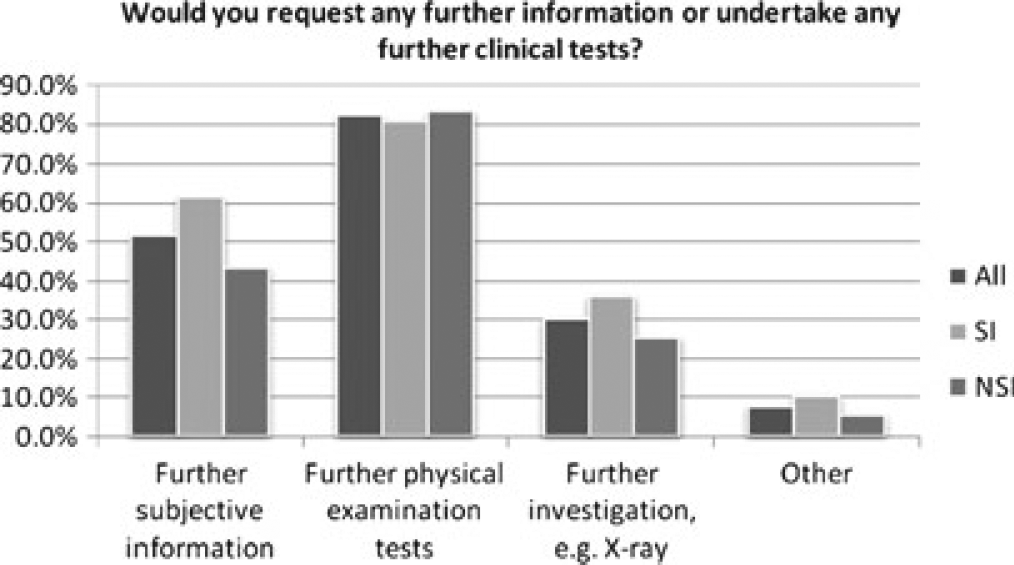
Would you request any further information or undertake any further clinical tests? All, all respondents; NSI, respondents who stated no special interest in rotator cuff pathology. SI, respondents who stated a special interest in rotator cuff pathology
Ninety-four out of 102 respondents qualified their responses. Requests for further information largely related to closer questioning around symptom response (e.g. is sleep affected) and any previous therapy. Further physical examination testing included reference to palpation, assessment of the thoracic spine, neurological tests, assessment of shoulder stability and further special tests (e.g. alternative impingement tests, empty/full-can test). Of those suggesting the need for further investigation, some participants would request imaging to aid diagnosis, whereas others would only consider this option if the patient was not responding to therapy. Reference to diagnostic ultrasound, X-ray and magnetic resonance imaging was made. The respondents indicating ‘other’ all related to further information gathering, tests or investigations.
4. Which management strategy/strategies would you recommend?
One hundred and eight (49 SI; 59 NSI) respondents completed this question. The UK physiotherapists in this study would offer a wide range of interventions (Fig. 2).
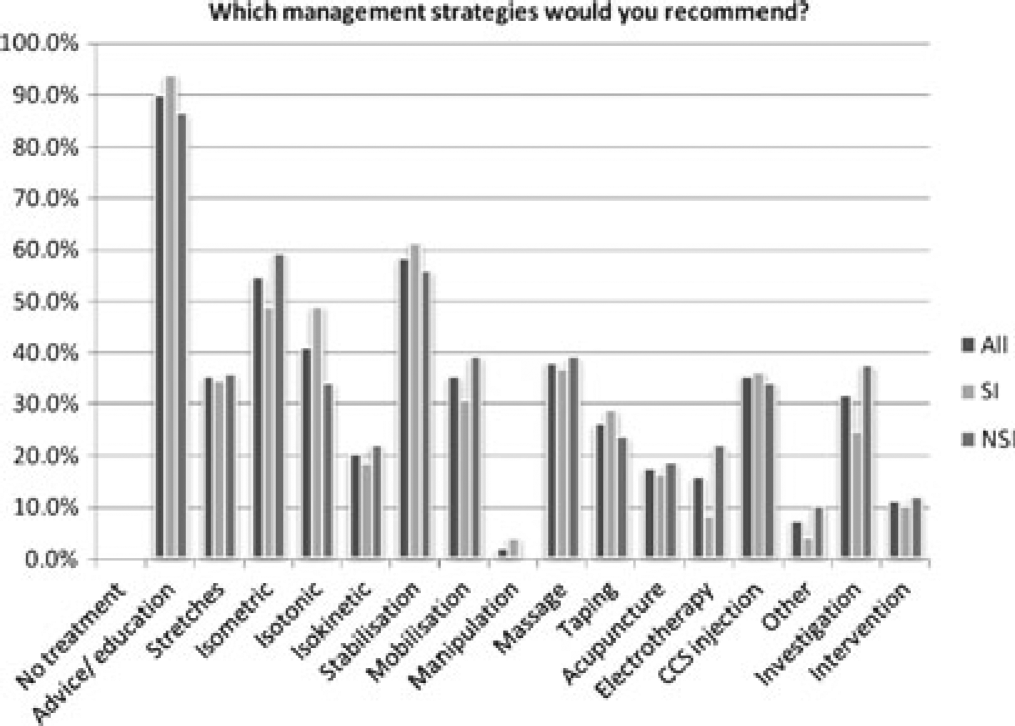
Which management strategies would you recommend? All, all respondents; NSI, respondents who stated no special interest in rotator cuff pathology. SI, respondents who stated a special interest in rotator cuff pathology; CCS, corticosteroid injection
5. If you would recommend exercise, would you encourage the case to continue with the exercises if they were painful?
One hundred and six (49 SI: 57 NSI) respondents completed this question. A greater proportion of SI respondents (53.1% versus 36.8%) would not prescribe painful exercises (Fig. 3). This difference in the responses between the SI and NSI groups was not statistically significant (χ2 = 3.165 p = 0.205).
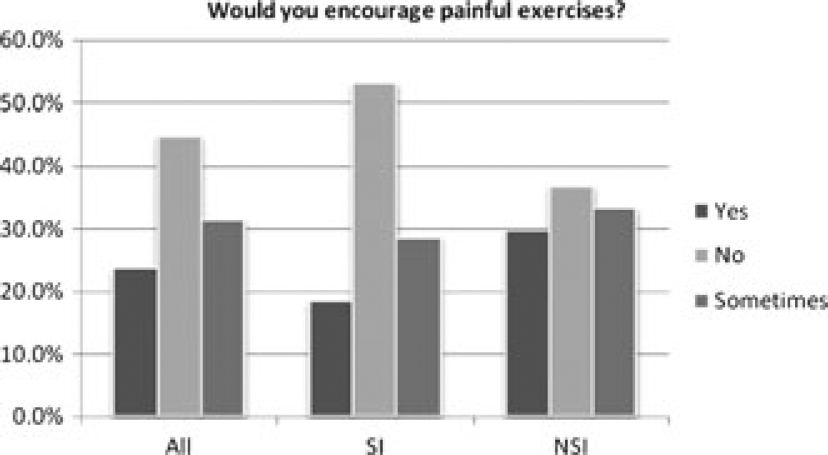
Would you encourage painful exercises? All, all respondents; NSI, respondents who stated no special interest in rotator cuff pathology. SI, respondents who stated a special interest in rotator cuff pathology
6. What would you expect in relation to self-management?
One hundred and eight (50 SI; 58 NSI) respondents completed this questionnaire. A minority of participants would suggest self-management only or entirely therapist-led intervention only. Most participants would suggest self-management with return to the clinic for guidance or self-management with return to the clinic for therapist led treatment or a combination of these approaches (Fig. 4).
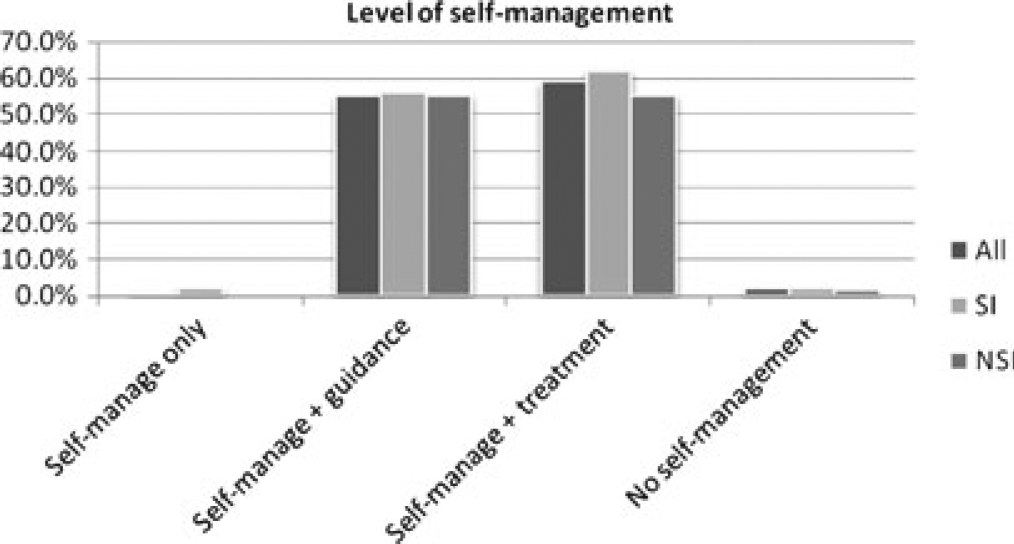
Level of self-management. All, all respondents; NSI, respondents who stated no special interest in rotator cuff pathology. SI, respondents who stated a special interest in rotator cuff pathology
7. Would you expect this person to recover with the prescribed physiotherapy?
One hundred and five (49 SI; 56 NSI) respondents completed this question. The vast majority of respondents would expect their patients to recover within 12 months (Fig. 5). A greater proportion of respondents with a SI would expect recovery within 3 months, although the difference in the responses between the SI and NSI groups was not statistically significant (χ2 = 6.687 p = 0.083).
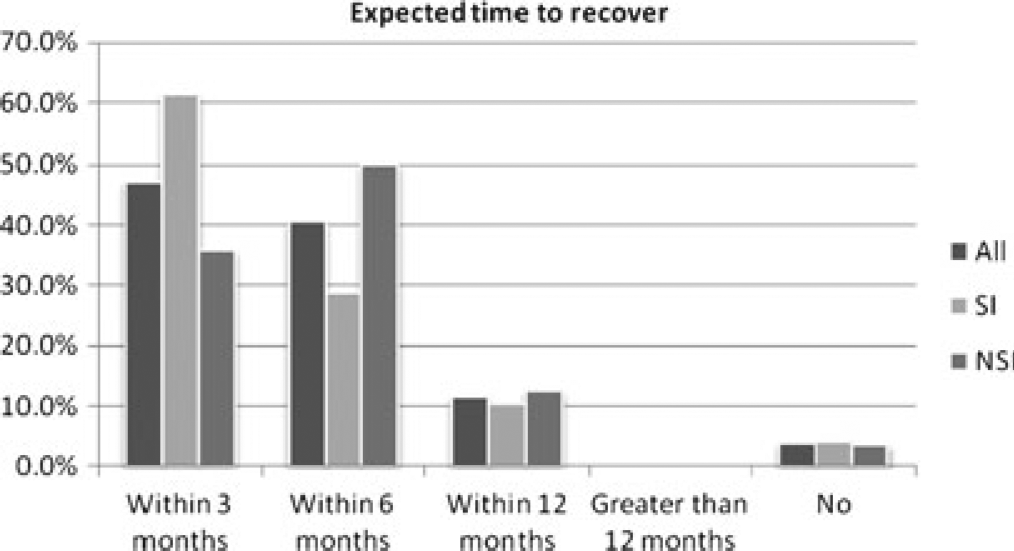
Expected time to recover. All, all respondents; NSI, respondents who stated no special interest in rotator cuff pathology. SI, respondents who stated a special interest in rotator cuff pathology
8. Do you think that further research could benefit your practice with regard to rotator cuff disorders?
A total of 108 respondents completed this question with 92 (85.2%) indicating that further research could benefit their practice, four (3.7%) indicating that they did not think that further research could benefit their practice and 12 (11.1%) respondents being unsure.
Of the 92 respondents indicating that they considered that further research could benefit their practice, 69 qualified their responses suggesting that further research should incorporate investigations into aetiology, assessment/diagnosis, the range of interventions offered by physiotherapists (including exercise and the need to develop prescription) and prognosis (including the identification of sub-groups who might respond more favourably to specific physiotherapy interventions).
Discussion
A survey of current practice was conducted to help better understand current physiotherapy practice in relation to rotator cuff disorders. A total of 110 responses were gained from a wide range of UK physiotherapists with varying experience working in a range of practice settings. Band 5 and 6 NHS physiotherapists more commonly regarded themselves as NSI with respect to rotator cuff disorders, whereas Band 8 NHS physiotherapists more commonly regarded themselves as having a SI. The physiotherapists who responded to this survey currently offer a wide variety of interventions and recognize the need for further research to help inform their practice.
The paucity of high-quality research that has been conducted in relation to the management of rotator cuff disorders is well recognized. This degree of variability in how physiotherapists treat patients presenting with disorders of the rotator cuff might reflect the lack of high-quality evidence available upon which physiotherapists can base their practice. The lack of an established evidence base means that a comparison of the findings of this survey with themes from current research is not warranted, although there are aspects of the responses to this survey that warrant further consideration in light of what is known.
In terms of establishing a diagnosis, a majority of respondents to this survey would undertake further physical examination tests (e.g. palpation, additional impingement tests) despite the lack of diagnostic accuracy of these procedures [20], [21]. It has been suggested that using these tests to make their associated diagnosis is invalid and clinical reasoning processes based upon these tests should be re-evaluated [20], [21]. Other classification systems have evolved that do not rely on specific tests to arrive at a structure specific diagnosis, such as Mechanical Diagnosis and Therapy [22] and the Shoulder Symptom Modification Procedure [20], although these other systems have not yet been widely integrated into practice and were rarely mentioned by the respondents.
To complement clinical diagnosis, a significant proportion of respondents would request further investigation (e.g. diagnostic ultrasound, magnetic resonance imaging or X-ray). As in other areas of the body, the value of these diagnostic tests has been challenged as a result of the presence of abnormal morphology in the absence of pain and/or functional deficit [23]. In the absence of clear signs for further investigation, such as severe trauma and possible red flag pathology [22], the value of these tests in relation to this clinical scenario appear unclear.
As might be expected, advice/education and exercise appear to be at the core of what most physiotherapists would offer in this situation, although the actual prescription is variable (e.g. isometric, isotonic, isokinetic, stabilization exercise). It perhaps reflects the current direction of the physiotherapy profession to observe that approximately 35% of respondents would consider a corticosteroid injection as a component of their management programme. This is despite no apparent indications of an inflammatory component to the clinical presentation [6] and a consistent theme in the literature suggesting that no additional benefit is gained from these injections in the mid or long term over other conservative treatment options offered by physiotherapists [24].
Of the physiotherapists who would prescribe exercise, approximately 44% would not prescribe exercise that is painful. This proportion is higher in the group who reported having a SI (53%). This opinion appears to predominate as a result of historical reasons where previous studies labelled most disorders of the rotator cuff and related structures as inflammatory in nature [25]. However, in relation to current thinking, there does not appear to be a scientific basis for this opinion [26]. This aspect is important because positive results have been gained with painful loaded exercise in tendon disorders in other areas of the body [27] and these findings have been replicated in a small pilot study with a group of patients awaiting surgery in relation to chronic painful impingement syndrome of the shoulder [26]. This aspect of exercise prescription clearly warrants further consideration in relation to the rotator cuff.
A range of opinion exists amongst the respondents as to the likely prognosis. It has been suggested that a majority of patients will improve within a few months after consultation in primary care [2], although these data are based upon return for further consultation, which is not an adequate measure of recovery, and it is also unclear whether more resistant presentations require physiotherapy, which means that such an optimistic forecast might not be applicable. Thus, the uncertainty with regard to the prediction of prognosis also appears to reflect current available literature.
Finally, the majority of respondents recognized the limited evidence base upon which to base their practice and advocated high-quality research to address the deficits in a range of areas, including the assessment process and management, as well as the identification of prognostic factors that might influence treatment outcome with physiotherapy.
Limitations
A total of 110 responses to the survey were obtained. Although the exact number of physiotherapists in the UK with experience of treating rotator cuff disorders is unknown, the number of respondents is likely to be a small proportion of this number, which might limit the generalizability of these findings. However, it is reassuring to note that the respondents were from a range of clinical settings and had a range of experience, as determined by their current predominant post.
The recruitment window for this survey was limited to 4 weeks, which reflects surveys of physiotherapy practice undertaken by others [17]. Nevertheless, a longer window might have resulted in a greater number of respondents. However, our experience in the month subsequent to closure of the survey verified the 4-week period. The vast majority of respondents completed the survey in the first 2 weeks after the initial posting. After a period of 10 days with no activity, two respondents completed on the final day but, after this, and although the instructions regarding the survey remained active and visible on iCSP, there were no further contacts requesting the link to the survey.
Conclusions
A total of 110 physiotherapists responded to this survey. These respondents stated that they would undertake a range of diagnostic tests, offer a wide variety of interventions and offer a broad prediction of prognosis, which indicates that current UK physiotherapy practice is variable. This degree of variability might reflect the lack of high-quality evidence available upon which physiotherapists can base their practice. There is a clear need for high-quality research to inform physiotherapy practice in this burdensome area.
Footnotes
Thank you for your interest in this survey. It should take less than 5 minutes to complete. Your responses will help us understand current physiotherapy practice in relation to rotator cuff disorders, which will subsequently enable us to develop meaningful programmes of research. We anticipate that the results of this survey will be published.
Please be aware that your responses are anonymized and your details will not be accessible to anyone.
Thank you for your time.
Please read the case report below before completing the survey questions:
A 57-year-old gentleman presents with a 12-month history of pain affecting the left shoulder. The onset was insidious and the problem is unchanging over time. The symptoms are intermittent and consistently produced with lifting, elevating the arm, reaching behind the back or lying on the left side. Symptoms ease with rest. He is medically well. He continues to work as a printer which involves regular lifting above and below shoulder level.
Observation of the patient is unremarkable. There was no pain at rest. Cervical range of movement is full and testing does not provoke any shoulder pain. There is a full range of active and passive movement at the left shoulder but there is an arc of pain provoked between 80° and 120° during active abduction. Scapulo-humeral rhythm was defined as normal during active movement testing. Pain was also provoked during isometric abduction and lateral rotation with associated mild weakness. The Hawkins-Kennedy impingement test was positive. Now please complete the questions below.