
Abstract
Longitudinal instability of the forearm (the Essex-Lopresti injury, radioulnar dissociation) is uncommon and is often missed in the initial assessment of a patient with a radial head fracture. The present review outlines the anatomy and biomechanics of the forearm unit, as well as the current means of diagnosis and the range of treatment options avaailable for this challenging problem.
Keywords
Introduction
Longitudinal instability of the forearm occurs when normal axial loading at the wrist produces abnormal longitudinal motion between the radius and ulna and abnormal load transfer between the wrist and elbow, resulting in pain and functional loss. This chronic situation arises following an acute axial injury with supra-physiological loading. Essex-Lopresti described a clinical scenario in which axial loading at the wrist produced radial head fractures in two patients. The first underwent acute radial head excision and developed proximal migration of the radius postoperatively. The second patient underwent open reduction and fixation of the radial head when it was noted that the distal radioulnar joint was subluxated [1]. The combination of injuries to the radial head and/or neck, interosseous membrane (IOM) and distal radioulnar joint (DRUJ) has become known as the Essex-Lopresti injury. Subsequently, much attention has been directed to improved understanding of this uncommon and high-energy injury. The present review focuses on the anatomical and mechanical considerations of longitudinal instability of the forearm and its diagnosis, as well as its treatment principles.
Anatomy and Mechanics of the Forearm
Traditional conceptualization of the forearm considers the DRUJ, the IOM and the proximal radioulnar joint (PRUJ) to be separate and discrete structures. However, this isolating approach makes it difficult to appreciate the integrated function of these structures. Several studies have reconceived the forearm as a single ‘joint’ or working unit with three inter-related parts: the PRUJ, the IOM (or middle radioulnar joint, MRUJ) and the DRUJ [2], [3] (Fig. 1). This model emphasizes the integrated function of the forearm unit and reminds the surgeon that both injury and treatment of one part may affect the others. Another way to approach the forearm unit is to consider it similar to a knee joint: two compartments/condyles (the PRUJ and the DRUJ) with ligaments (the IOM) between [2]. One would not consider the lateral compartment of the knee joint in isolation; disorders of one part directly impact on the other parts. Furthermore, the healing capacity of the IOM may be similarly as poor as the cruciate ligaments of the knee.
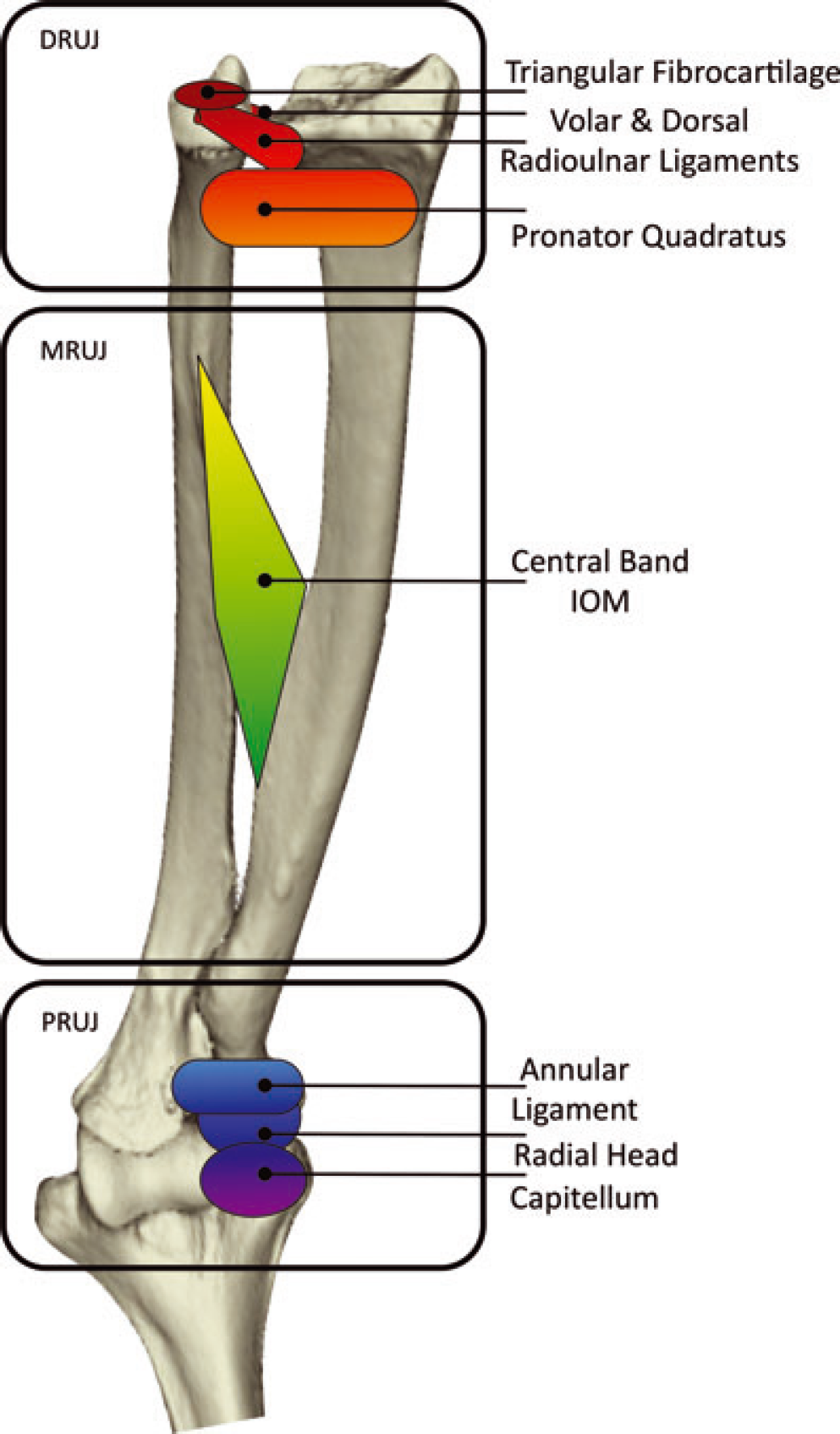
Schematic anatomy of the forearm joint, its components, and its stabilizers. The proximal radioulnar joint (PRUJ) is stabilized by the interaction between the radial head and capitellum and by the annular ligament. The middle radioulnar joint (MRUJ) is stabilized by the interosseous membrane (IOM). The distal radioulnar joint (DRUJ) is stabilized by triangular fibrocartilage complex, radioulnar ligaments, and pronator quadratus (among other structures).
The anatomy of the IOM has been extensively studied [4]–[6]. Despite the variability in naming and numbering the component parts of the IOM, these stusies all agree on the universal and robust nature of the central band. Skahen et al. identified the origin of the central band on the radius beginning an average of 7.7 cm distal to the radial head, and inserting on the ulna beginning at 13.7 cm distal to the olecranon tip [5]. Noda et al. related the origin and insertion as percentages of the bone length [6]. The fibres of the central band are oriented at 21° to the long axis of the ulnar shaft [5]. A variable complement of other bands is proposed to help stabilize the forearm proximally or distally to the central band.
At the elbow, the radial head is prevented from further proximal migration by its interaction with the humeral capitellum. The radius and ulna are linked proximally through the annular ligament [7] and distally through the distal radioulnar joint and its soft-tissue stabilizers. These include the triangular fibrocartilage complex, dorsal and volar radioulnar ligaments, and the pronator quadratus [8] (Fig. 1).
The forearm unit has two major tasks: rotation of the radius around the ulna and load transfer between the wrist and the elbow. Because of these dual functions, the stabilizing structures have contributions to rotational and longitudinal stability within the forearm unit. Given its focus is on longitudinal instability, the present review emphasizes the longitudinal stabilizers and the normal load-transfer mechanics. However, this is a simplification of the forearm mechanics in vivo.
The first principle of forearm mechanics is that the ulna is a fixed structure. The radius rotates about the ulna and translates proximally and distally by a small amount during rotation. Any forearm stabilizer will act to maintain this physiological relationship between the radius and ulna. This is useful when undertaking a reconstruction because the fixed length and position of the ulna can act as a reference point. For example, the mean (SD) normal ulnar variance is 0.74 (1.46) mm [9]; a helpful guide when assessing the quality of reduction of the radius relative to the ulna.
The second principle is that longitudinal stability is not the responsibility of a single structure but rather has contributions from structures at all levels of the forearm. Proximally, the radius is prevented from further proximal translation by the capitellum [10], as well as through the action of the annular ligament. In the MRUJ, the central band of the IOM provides considerable resistance to proximal migration of the radius [10]. Distally, the triangular fibrocartilage complex and DRUJ stabilizers also prevent longitudinal migration of the radius [10]. Rabinowitz et al. have demonstrated that up to 7 mm of proximal radial migration can occur after excision of the radial head without disruption of the IOM [10].
The third principle is that the IOM is solely responsible for the redistribution of load as it travels within the forearm between the wrist and the elbow. Under physiological conditions, the radius bears 80% of the load as it crosses the wrist (subject to variation based on ulnar variance) [11], whereas it transfers only 40% to 60% of this load at the elbow [12]. Sectioning of the IOM, particularly the central band, prevents this load transfer in vitro [10], with clinical consequences even when the radial head is reconstructed [13].
Detecting Longitudinal Instability
Although injury to the radial head is a common occurrence, the Essex-Lopresti injury is not [14], with an estimated incidence of 1% of radial head fractures [15]. However, the latter can be quite difficult to distinguish from the former, and an index of suspicion must be maintained.
History and physical examination provide the first clues, although these may be nonspecific. Many injuries can result from a fall on an out-stretched arm, applying axial loads through the forearm. Many patients will not be able to give a detailed or clear account of the precise mechanism. Furthermore, the patient may focus on elbow pain and not note forearm or wrist pain. Distal arm pain can also be masked by the elbow pain or dismissed as referred pain. Examination of the elbow must always include an examination of the forearm and wrist [16]. Forearm or wrist swelling and asymmetry and significant DRUJ tenderness should raise concern of a more serious injury [14], although there is often mild wrist tenderness in association with radial head fractures [17].
Radiography is another important source of information. Fractures of the radial head associated with significant impaction or dislocation of the fragments may indicate a change in the length of the radius with respect to the ulna. Radiographs of the ispilateral and possibly contralateral wrist can demonstrate proximal migration of the radius with respect to the ulna on the injured side [16]. In more obvious cases, this may be sufficient to diagnose the longitudinal forearm instability, although it should be noted that up to 7 mm of proximal migration can occur without loss of the central band of the IOM [10] and not all injuries of this type will present with abnormal ulnar variance initially [18]. Dynamic radiographic examination can also be performed. Davidson et al. described an axial compression test in which the upper arm is stabilized when compressive and distractive loading is applied to the forearm distally to assess the amount of longitudinal motion of the radius at the level of the DRUJ. They set 5 mm of axial motion as being a positive test [14].
Other diagnostic modalities have been evaluated to improve detection of significant IOM injuries. Ultrasound has been assessed in several studies performed in both cadaveric models and live participants. The IOM appears as a hyperechoic line bridging the radius and ulna, and disruption of this line over a 2-cm distance represents an IOM rupture [19]. A dynamic component to the assessment has been explored by Soubeyrand et al. in which muscle can be seen to herniate from the volar compartment into the dorsal through the disrupted IOM when pushing dorsally on the volar compartment muscles [20]. This may improve the diagnostic yield and reduce some of the operator-dependent concerns. Accuracy in cadaver models has been as high as 100% for identifying IOM injuries [20], and clinical studies thus far have found good correlation between abnormal ultrasound findings and injury noted intra-operatively [21], [22].
Magnetic resonance imaging (MRI) has also been investigated for use in detecting IOM injuries. Haemorrhage and oedema within the interosseous space appear to represent the findings that are most suggestive of injury [19]. Partial injury to the IOM can also be detected with this method [23]. The potential advantages of MRI over ultrasound include the ability to diagnose multiple injuries and also that the technique is less operator-dependent, whereas the disadvantages include the usual contraindications to MRI and also that it is more expensive [18]. A direct comparison of MRI and ultrasound has not demonstrated the superiority of one technique over the other. MRI had better accuracy, specificity and positive predictive value, whereas ultrasound had slightly lower accuracy, better sensitivity and negative predictive value, although these differences were not significant [24].
Although it is helpful to have investigations to assist in detection of significant IOM injuries, the above studies need to be interpreted carefully. Most of the validation studies have been performed in small numbers of cadaveric arms with sharp transection of the IOM. The IOM does not fail by this method in vivo but rather elongates until failure, making it possible for incompetent but continuous fibres to remain after injury. Few of these studies have attempted to characterize the appearance of the IOM after an acute axial loading injury aiming to differentiate what represents a mild injury and what represents true longitudinal forearm instability. In vivo, MRI is very sensitive for detecting tissue oedema, which could lead to the over-diagnosis of IOM disruption. For example, Hausmann et al. found a high incidence of partial IOM injury on acute MRI in their series of 14 patients with Mason 1 radial head fractures, although none were found to have a structurally important lesion (i.e. a true Essex-Lopresti) [23]. Furthermore, no work has been carried out to validate imaging in chronic longitudinal instability, and it is not clear how the radiographic appearance of the IOM after a period of healing and/or scarring correlates with its functional integrity. A soft tissue link between the radius and ulna may not equate with functional tissue. Therefore, the stated accuracy, sensitivity and specificity may represent the ideal condition and, in reality, results of these investigations need to be considered in context with other clinical data from these patients.
A final source of information on the status of the IOM may be the intra-operative findings when treating the radial head fracture. Soubeyrand et al. proposed use of a radius ‘joystick’ manoeuver intra-operatively consisting of placing the forearm in full pronation and applying a laterally directed traction force to the radial neck. A positive test is present when the radial neck displaces laterally (i.e. the amount of displacement is not defined). Although this test has been reported on in vitro, it was felt that it is sufficiently promising to move to in vivo validation [25].
On a delayed basis, the presentation of Essex-Lopresti can include features of ulnar impaction syndrome (wrist pain, especially with power grip) and abnormal forearm rotation [26]. The ulnar head may appear asymmetrically prominent compared to the contralateral normal extremity. Radiographs may show a positive ulnar variance that is also different than the contralateral normal extremity [26]. There may also be restriction of movement or pain at the elbow [27]. These features may also vary depending on the previous treatment undertaken.
A recent study has challenged the incidence of longitudinal instability related to radial head fracture. Duckworth et al. examined 60 patients presenting with a closed radial head fracture and ipsilateral wrist pain. They performed bilateral wrist radiographs and declared radial migration of ≥ 2 mm compared to the contralateral side to be suggestive of an Essex-Lopresti injury. The maximum migration observed was 4 mm. Of the 22 patients with ≥ 2 mm migration, only one underwent surgery (radial head replacement). Unfortunately, no intra-operative observations about forearm stability in that patient were noted in their study. Follow-up was less than 1 year for some of the patients, and there was no radiographic follow-up. Nineteen of 22 patients had very favourable results. It was suggested that upwards of 30% of all persons with closed radial head fractures display evidence of an Essex-Lopresti injury [17]. Their study highlights the need for clear definition of what constitutes a clinically important IOM injury because many individuals may have mild or partial injuries that go on to heal with minimal consequence [17], [23]. A shortening of up to 4 mm being representative of longitudinal instability is inconsistent with a previous study on the amount of proximal migration permitted by simply excising the radial head [10]. Labelling these patients as having an Essex-Lopresti ‘spectrum’ injury will serve to add confusion to the literature with respect to treatment outcomes and prognosis.
Treating Longitudinal Forearm Instability
General principles
The ultimate goal of any course of treatment is to restore and maintain motion through the forearm unit, as well as to restore and maintain normal load bearing and load sharing. This may mean addressing some or all of the component injuries: the radial head, the IOM and the DRUJ. The options for management depend on the stage in which the instability is recognized, as well as on what treatment has already been applied. Treatment can be classified in terms of repair or reconstructive techniques and salvage techniques. Interpreting the literature on the treatment of longitudinal instability is particularly difficult because of the small number of patients, delays in diagnosis, heterogeneity of previous treatment, heterogeneity of reported treatment, lack of standardized pre and postoperative scoring, and incorporation of the longitudinal instability patient group into larger groups with assorted complex upper extremity conditions.
The radial head
This is generally the first injury recognized, and carries a range of severity. Essex-Lopresti recognized early that excising the radial head was a misstep [1]. The options for management of the radial head fracture are either open reduction and internal fixation or prosthetic replacement. Attempts at reconstruction using osteochondral radial head grafts have met with mixed results and high rates of nonunion, such that this approach has largely been abandoned [28], [29]. Prosthetic options have advanced considerably in the past few decades to include a range of metallic and pyrocarbon designs. Although silastic components have been used, they are not an effective prosthetic choice because they lack the material properties to resist axial forces, and the components can wear and fracture leading to destructive synovitis [15], [30]. Consequently, metallic or pyrocarbon components are preferred.
Restoration of the anatomy with a prosthesis can be challenging because there may not be a radial head available from which to template as a result of comminution or prior radial head excision. ‘Overstuffing’ is a constant concern that can lead to pain and stiffness of the elbow and capitellar erosion [31]–[33]. One reference point is the ulnar variance, and contralateral wrist radiographs can assist with restoration of the patient's ‘normal’ variance. Another is the relationship of the radial dish to the sigmoid notch and the ulnohumeral articular space [34], [35]. This should be assessed with the forearm placed in full pronation because it is taught that the radius ‘pistons proximally in pronation.’ However, because the usual soft tissue constraints on longitudinal displacement of the radius have been lost by definition, these references may be less reliable.
Results of radial head replacement for chronic longitudinal instability are challenging to interpret. These patients may be mixed in with other patients with a variety of elbow pathology [36] or may have been treated with techniques and implants no longer in widespread use [15]. However, a recent case series has looked at the results of chronic longitudinal instability treated with metallic radial head replacement in eight patients [37]. Two patients required capitellar replacement as a result of the development of symptomatic radiocapitellar arthritis. Five of eight patients required revision of their radial head replacements from unipolar to cemented bipolar implants after aseptic loosening. At last follow-up, six patients were considered to have successful outcomes, whereas the remainder were considered failures, although only three were successful after the first radial head replacement in this series. The study did not report on final outcomes for the five patients who underwent revision and no patient received an excellent result on either the Mayo Wrist or Elbow Score [37]. A second series by Jungbluth et al. reported on 12 patients, 10 of who received metallic radial head prostheses as part of the treatment for chronic longitudinal instability. In four, this proved to be adequate treatment over the duration of follow-up (12 months to 69 months). No pre-operative scoring was performed, and the average postoperative result was ‘fair’ in the Mayo Elbow Performance Score. Forearm rotation continued to be limited. Ten of the 12 patients in the series were satisfied with their result [27].
There are two problems with radial head replacement after previous radial head excision. The first relates to loss of the space that was previously occupied by the radial head. This is less of a concern acutely but, with chronic instability, it may not be possible to create a space within the tissue to accommodate the desired height of prosthesis, or any prosthesis at all in more severe situations. Trying to recreate this ‘lost compartment’ is difficult and fraught with risk. The result of being unable to fully restore the radial head and neck anatomy can be residual ulnar positive variance at the wrist.
The second relates to precipitous capitellar wear. This has been described previously [13], [33], [37] and may be the result of abnormal load transfer and material property mismatch in the radiocapitellar joint. This has been addressed with radiocapitellar arthroplasty in selected instances [13], [38]. Capitellar osteopaenia has been observed after radial head excision, which could contribute to the precipitous wear in selected chronic reconstructions [36]. Heijink et al. noted that the osteopaenia resolved in some of their patients over time. However, they recommended capitellar replacement in patients that showed capitellar arthritis at time of radial head replacement. They also recommended that cemented components be used and a bipolar prosthesis be employed if there was concern about maltracking on the capitellum [37]. There is limited clinical follow-up even in the short term for radiocapitellar arthroplasty for any indication, and simply resurfacing both sides of the joint does not address the issue of the abnormal loads seen at the radiocapitellar joint with a deficient IOM. Wear of the components continues to be a serious concern, and the risk of overstuffing the articulation is magnified when both sides are resurfaced when used for this indication.
Ulnar shortening osteotomy
An ulnar shortening osteotomy in the context of longitudinal instability is performed to relieve the ulnar impaction symptoms after proximal migration of the radius. Duckworth et al. described two cases of established longitudinal instability treated with ulnar shortening. At 3-year and 7-year follow-up, the results were satisfactory (Mayo Elbow Performance Scores of 85 and 100; Disabilities of the Arm, Shoulder and Hand scores of 0 and 2.5). No wrist-specific assessment was performed for these patients [39], which is important given that ulnar shortening is generally performed to address wrist symptoms, not elbow symptoms. A second case report from Jungbluth et al. described a sequence of interventions beginning with acute radial head excision. When the patient presented with 11 mm of positive ulnar variance, a shortening was undertaken. Fifteen months later, the patient represented with ongoing wrist pain and a further 8 mm of positive ulnar variance. Further surgical management ensued [13]. Although ulnar shortening is a well-known procedure, it does not address the pathoanatomy and pathomechanics of this injury. If the radial head is left deficient, proximal migration may occur again, leading to recurrence of the ulnar impaction. However, a role for ulnar shortening as part of the overall reconstructive strategy may be important because, even with radial head replacement and IOM reconstruction, there may be some residual positive ulnar variance [40], [41].
Interosseous membrane reconstruction
Most of the clinical attention in treatment of the Essex-Lopresti injury has been directed either at management of the radial head and ulnar impaction, or at salvage of a missed injury with its chronic sequelae. However, there has been increasing interest in the past 15 years in reconstructing the IOM itself given the mediocre results of current treatment. There is now clinical evidence that even with restoration of radial length acutely, the IOM may not heal adequately to resume its load-transference and stabilizing roles [42], [43].
Various procedures have been described to reconstruct the biomechanical function of the central band of the IOM. In principle, this should stop excessive proximal migration of the radius and rebalance the load passing through the forearm. Historically, these procedures have had an unpredictable outcome, although technology has evolved and more options and techniques are available. Most of these techniques have been described and assessed in cadaveric populations, and an understanding of the functionality of the IOM reconstruction has been gained. Table 1 summarizes the existing body of work. Essentially, IOM reconstruction needs to be combined with radial head reconstruction for optimal results in vitro. The proximal condyle of the forearm joint is a critical component. Load transfer can be brought to near-normal and proximal migration of the radius considerably reduced. However, in a clinical setting, full reduction of the radius may be challenging as a result of the ‘lost compartment’, and an ulnar shortening osteotomy may be required. Choice of graft can be bone–patellar–tendon–bone, doubled flexor carpi radialis, or synthetic for best mechanical result. Only a handful of patients have been reported on and these biomechanical studies need to be interpreted with caution until more in vivo work is performed.
Summary of interosseous membrane (IOM) reconstruction techniques and their biomechanical effectiveness
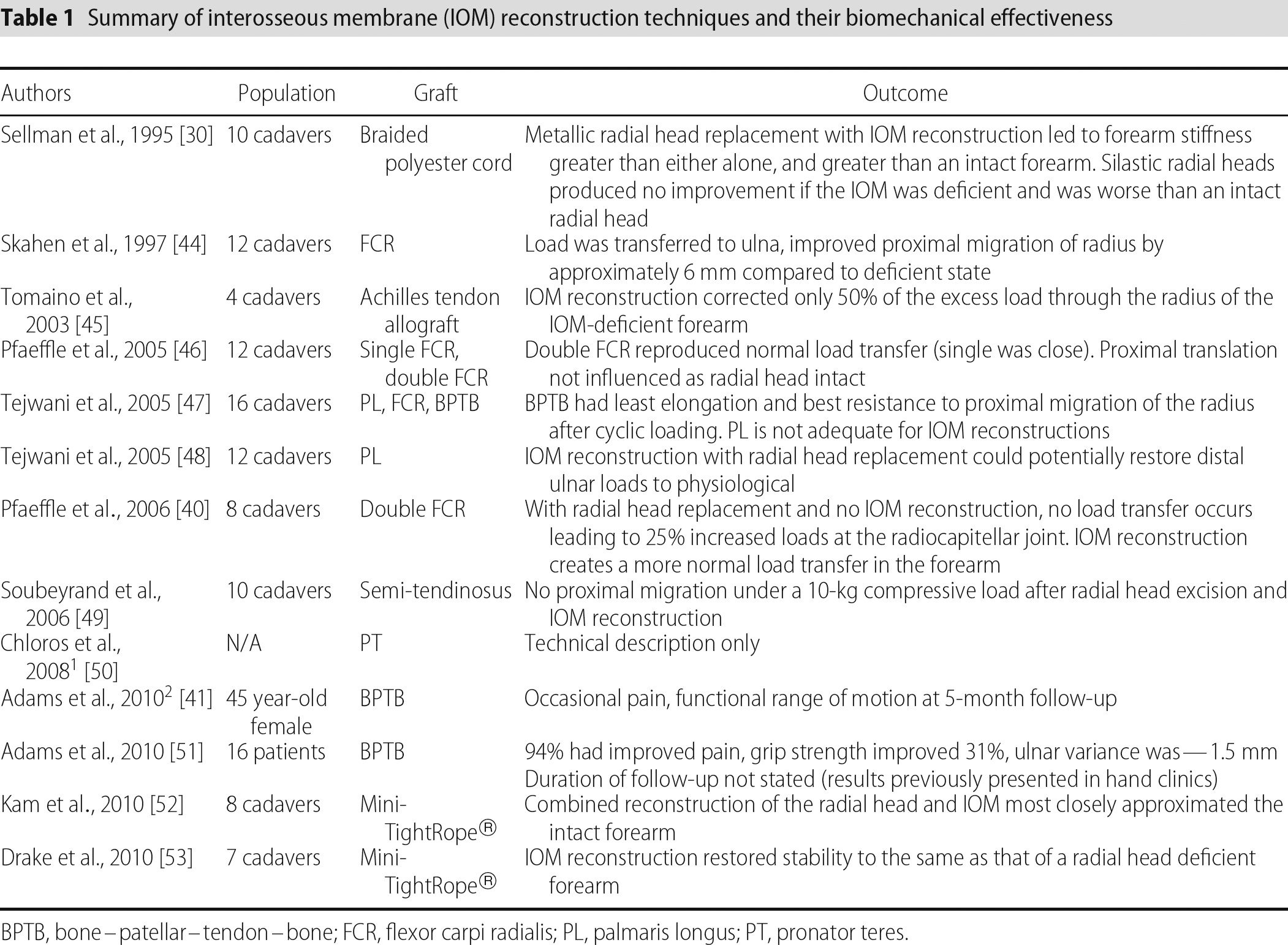
BPTB, bone–patellar–tendon–bone; FCR, flexor carpi radialis; PL, palmaris longus; PT, pronator teres.
Our preferred technique (Fig. 2) uses a braided polyethylene graft (LARS ligament, Corin Group, Cirencester, UK). The ulnar fixation point is planned 6 cm proximal to the ulnar styloid, whereas the proximal radial fixation point is templated for a graft angle of 21° to the ulnar shaft. The IOM is accessed through a midline volar incision on the supinated forearm centred over the radial fixation point. A 3.5-mm unicortical hole is drilled, followed by a 2.5-mm hole in the far cortex, aimed slightly oblique. A suture passer is used to pass the graft through the docking hole with the tails of the graft threaded through an endobutton and tied on the radial cortex. A separate distal incision is used to create the ulnar tunnel in similar fashion. A clamp is used to retrieve the graft under the muscle. The graft is cut to a length that will leave it within the ulnar tunnel and two No. 2 Orthocord® (Johnson & Johnson, New Brunswick, NJ, USA) are whip-stitched into the end. The sutures are passed through the ulnar tunnel and threaded through a second endobutton. An assistant applies longitudinal traction to the forearm at the same time as a second assistant applies traction to one set of sutures. The surgeon then ties the sutures sequentially. Other reconstructive procedures such as radial head replacement or ulnar shortening osteotomy can be combined with this (Fig. 3). The patient is placed in a Muenster-style splint in neutral forearm rotation postoperatively. Early results are encouraging, although more time is needed to assess the longer-term results of this technique in vivo.
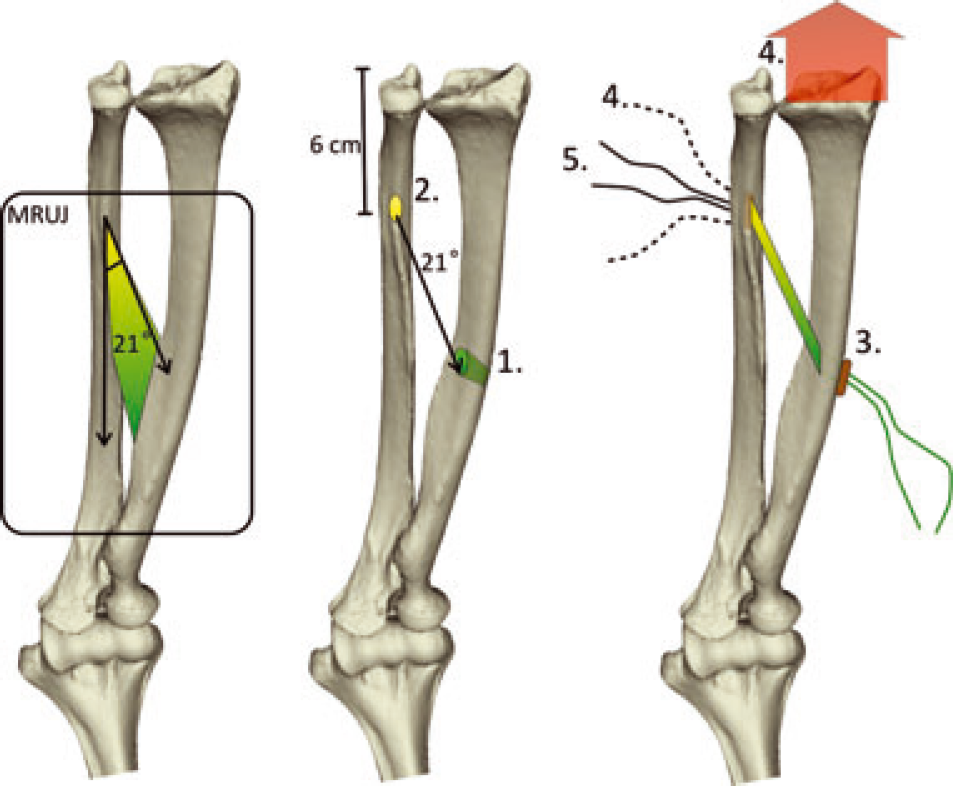
Interosseous membrane reconstruction. The central band forms an angle of 21° with the axis of the ulna (left). The ulnar tunnel is templated to be 6 cm from the tip of the ulna, and the radial tunnel is planned to have the graft at 21° to the ulnar shaft (middle). The radial tunnel [1] is drilled first, then the ulnar tunnel [2]. The radial end of the graft is passed through the tunnel and tied over an endobutton [3]. The graft is passed to the ulna and sutured. The assistants apply longitudinal traction on both the forearm and one set of sutures [4]. The surgeon ties both sets of sutures sequentially over an endobutton [5]. MRUJ, middle radioulnar joint.
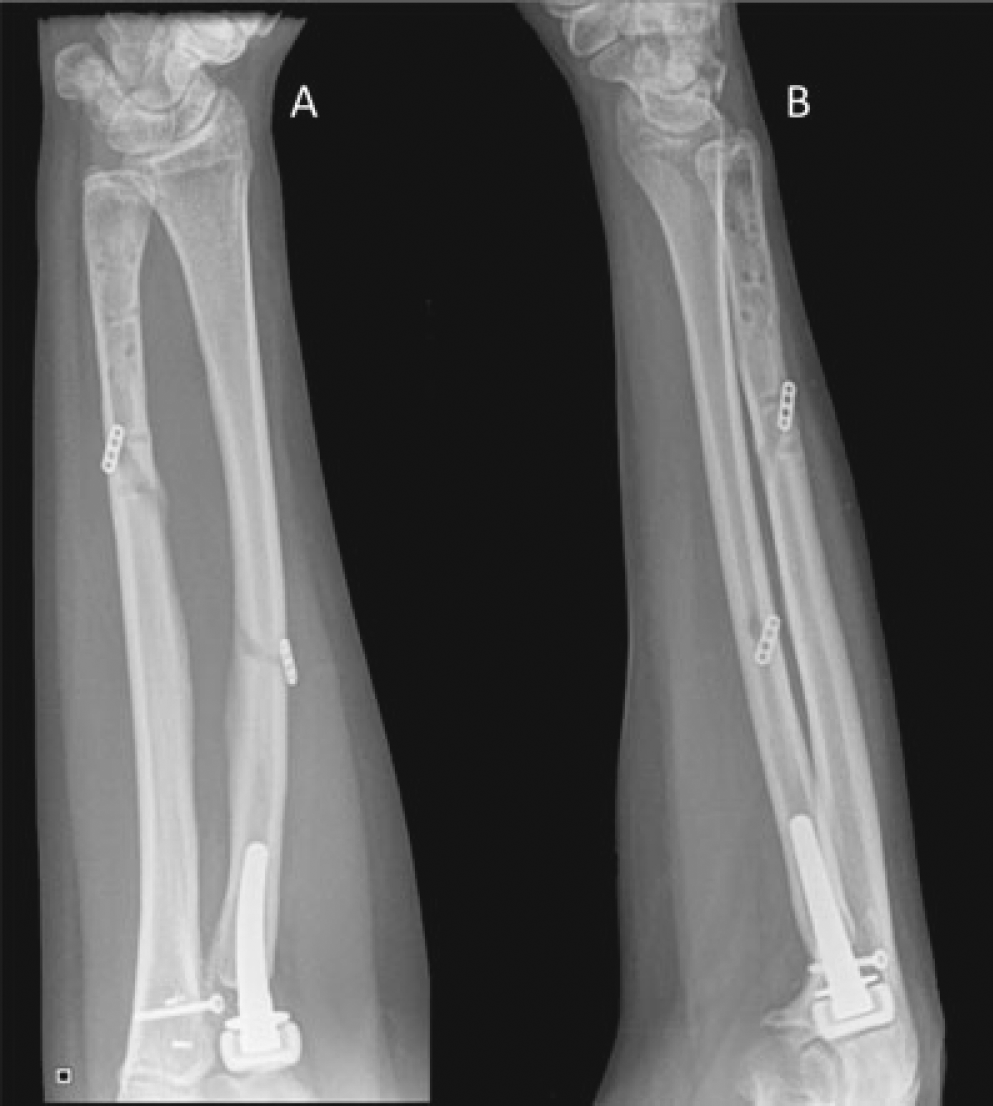
Postoperative radiographs after interosseous membrane reconstruction combined with radial head replacement. (A) Anterior–posterior view. (B) Lateral view. The radial and ulnar tunnels are clearly visible with the endobuttons at each. A prior ulnar shortening had been performed. Note the restoration of the relationship of the radius and ulna at the distal radioulnar joint. The proximal ulnar screw is retained hardware from a previous surgical approach.
Salvage procedures
If other procedures have failed to address the symptoms associated with chronic longitudinal instability, treatment focus shifts from reconstruction to salvage. Procedures described for this include the Sauvé-Kapandji procedure and creation of a one-bone forearm.
The use of the Sauvé-Kapandji procedure (i.e. fusion of the distal radioulnar joint with ulnar pseudarthrosis proximally) has been advocated by some surgeons as a means of addressing the DRUJ-related symptoms of the chronic Essex-Lopresti injury [27]. Jungbluth et al. treated three women with chronic forearm instability and considered it to be a success. No problems associated with the ulnar stump were reported at follow-up, ranging from 22 months to 50 months. However, the results in these patients were pooled with nine other patients who were treated with other procedures for the same clinical problem, making it difficult to draw conclusions about the specific outcomes of this procedure for this indication. This procedure may address ulnar impingement, although it completely destroys load-transfer in the forearm unless the radial head has been replaced because there is then no direct bony link between the wrist and the forearm. This technique should be viewed with caution.
Because of the rarity of performing a procedure to induce radioulnar synostosis, there is limited literature on surgical outcomes, and what does exist only represents small series with multiple techniques for multiple indications. In the largest series to date, Petersen et al. reported on a series of 19 patients who had treatment during an 18-year time frame had various post-traumatic and post-neoplastic disorders. Of the 11 patients who underwent synostosis for post-traumatic concerns, none had an identified Essex-Lopresti injury, and many had protracted clinical courses complicated by nerve injury and/or infection before their salvage procedure. Multiple surgical techniques were used and a range of synostosis positions was employed. Outcomes were assessed using a bespoke scoring system. There were no excellent results in the post-traumatic group, althoguh nine were considered good. In their scoring system, one generally had to have only mild to moderate pain, and at least be able to manage activities of daily living to achieve a ‘good’ result. Complications were higher in the post-traumatic group [54].
Towards a unified approach
It is understandably difficult to create an algorithmic approach to an injury that is difficult to identify and quite uncommon. However, given that our understanding of the pathoanatomy and pathomechanics has been expanding rapidly in the past few years, this may now be feasible. The wider orthopaedic community has been receiving the message of the importance of not excising the radial head acutely without some form of prosthesis, although this may not be sufficient. Despite very limited clinical information on the effectiveness of IOM reconstruction in vivo, Marcotte and Osterman have proposed a treatment algorithm for acute and chronic Essex-Lopresti injuries [41], [55]. In the acute scenario, they recommend either fixation or replacement of the radial head, reduction and immobilization of the DRUJ, and consideration of acute repair/reconstruction of the IOM. In established longitudinal instability, they recommend replacement or excision of the radial head, ulnar shortening osteotomy, and reconstruction of the IOM (Fig. 4). Further work is needed to determine the efficacy of an organized approach such as this, and also to determine the efficacy of IOM reconstruction in vivo.
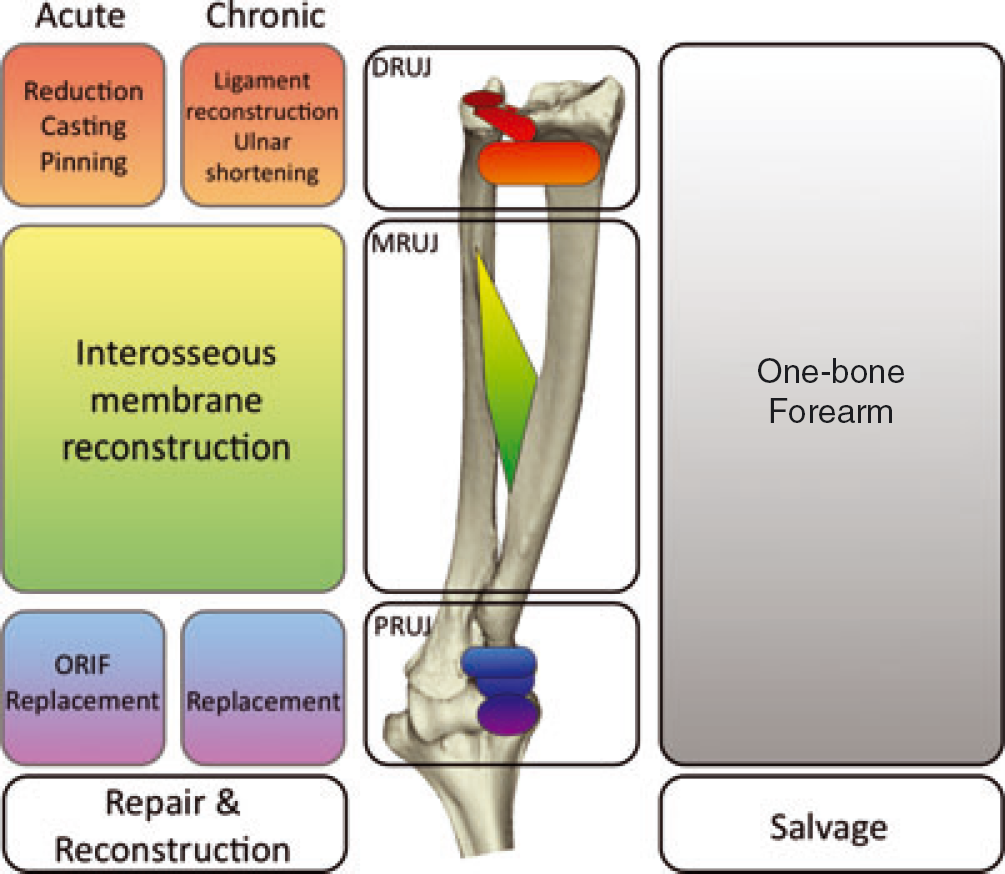
Summary of treatment algorithm for longitudinal forearm instability. Acute injuries have been defined as less than 4 weeks between injury and treatment. Each part of the forearm unit is addressed in this scheme. DRUJ, distal radioulnar joint; MRUJ, middle radioulnar joint; ORIF, open reduction internal fixation; PRUJ, proximal radioulnar joint.
Conclusions
The Essex-Lopresti injury may be uncommon, although recognition is critical to selecting the appropriate treatment of the patient and avoiding the difficult longer-term consequences. Acute excision of the radial head after trauma is a treatment decision that carries the potential for disaster and should be avoided. Many procedures for management of established longitudinal instability have been described, although small patient numbers and poor methodology of clinical studies make it very difficult to draw guidance from the literature. Comparing these procedures is difficult given a lack of pre-operative clinical data and validated scoring systems. Furthermore, variability in prior treatment and associated injuries makes a standardized treatment approach difficult. The next steps in trying to improve the outcome of this difficult injury must be improved recognition and the use of reconstructive techniques for the affected components of the forearm unit rather than procedures purely for short-term symptom management. More rigorous clinical evaluation of the outcomes will also be important.