
Abstract
Background
Shoulder arthrodesis is a unique procedure, which has shifted from a well-established procedure for osteoarthritis to a salvage procedure. In the present retrospective study, functional outcome and morbidity in shoulder arthrodesis using combined plate/screw fixation versus screw fixation alone were evaluated.
Materials and Methods
Shoulder arthrodesis was performed on 28 shoulders: 16 cases with only cancellous screws and 12 cases with combined plate/screw fixation. At a mean follow-up of 6.8 years (range 1 years to 20.4 years), patients were invited for clinical follow-up, with evaluations of visual analogue scale for pain, function and satisfaction, Constant–Murley scores, and recorded complications.
Results
All patients had severe limitations in the use of their shoulder, although they had little pain and were satisfied. The overall Constant–Murley score increased significantly from 33.4 to 52.2. In eight cases with combined plate/screw arthrodesis and nine with screw arthrodesis, there was persistent pain, which resolved after removal of osteosynthesis material. Non-union was only found in five patients with screw arthrodesis.
Conclusions
Although the risk of a second operation for removal of osteosynthesis material in combined plate/screw arthrodesis is equal to screw fixation alone, for complete glenohumeral fusion, a combined plate/screw fixation appears to be superior to screw fixation alone.
Introduction
In the past, shoulder arthrodesis proved to be a successful procedure for glenohumeral joint destruction from tuberculosis [1] or paralysis from poliomyelitis [2]. With the effective treatment of these diseases, indications for an arthrodesis of the shoulder moved to osteoarthritis and post-traumatic conditions. Currently, shoulder (hemi-)arthroplasty comprises an effective alternative for these disorders, leading to a marked reduction in the number of shoulder arthrodesis performed. On the other hand, there still remain indications for shoulder arthrodesis as a salvage procedure, including paralysis of shoulder muscles and chronic infections.
Subsequent to the first reported successful shoulder arthrodesis in 1881 performed by Albert [3] various intra-articular and extraarticular techniques using autologous bone grafts have been applied. In the 1960s, screws or pins were used to achieve consolidation of the arthrodesis [1]. Nowadays, most surgeons prefer plate fixation and/or screw fixation for performing a shoulder arthrodesis. Unfortunately, despite new and improved techniques, complications after shoulder arthrodesis remain frequent and complication rates of approximately 25% to 35% [4]–[6] are still reported. As a result, a high rate of secondary operations can also be found in the literature.
Despite the high rate of complications, repeat surgery and a significant loss of movement after this salvage procedure, several studies [7]–[9] in the past few decades have reported on the excellent outcome in terms of pain and satisfaction after shoulder arthrodesis.
Because surgical techniques may have improved over the years, we considered that it would be useful to evaluate present subjective and objective functional results and morbidity in combined plate/screw arthrodesis of the glenohumeral joint versus screw fixation alone.
Materials and Methods
Patient selection
From January 1985 to June 2005, a total of 28 shoulder arthrodesis was performed in 27 patients (Fig. 1). The group consisted of 11 women and 16 men with a mean age of 45 years (range 18.5 years to 82.0 years) (Fig. 2) at the time of arthrodesis. Shoulder arthrodesis was performed in nine left shoulders and 19 right shoulders (one patient had undergone a shoulder arthrodesis in both shoulders).
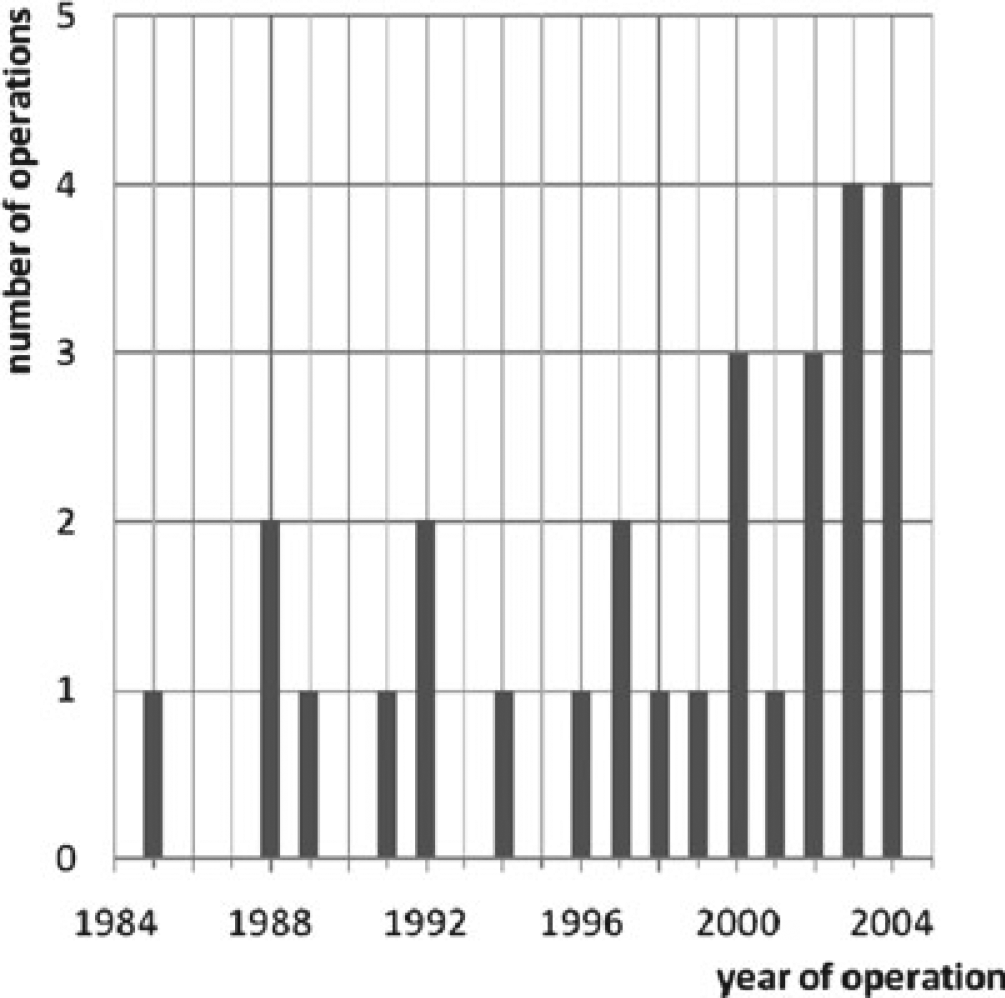
Number of operations carried out per year.
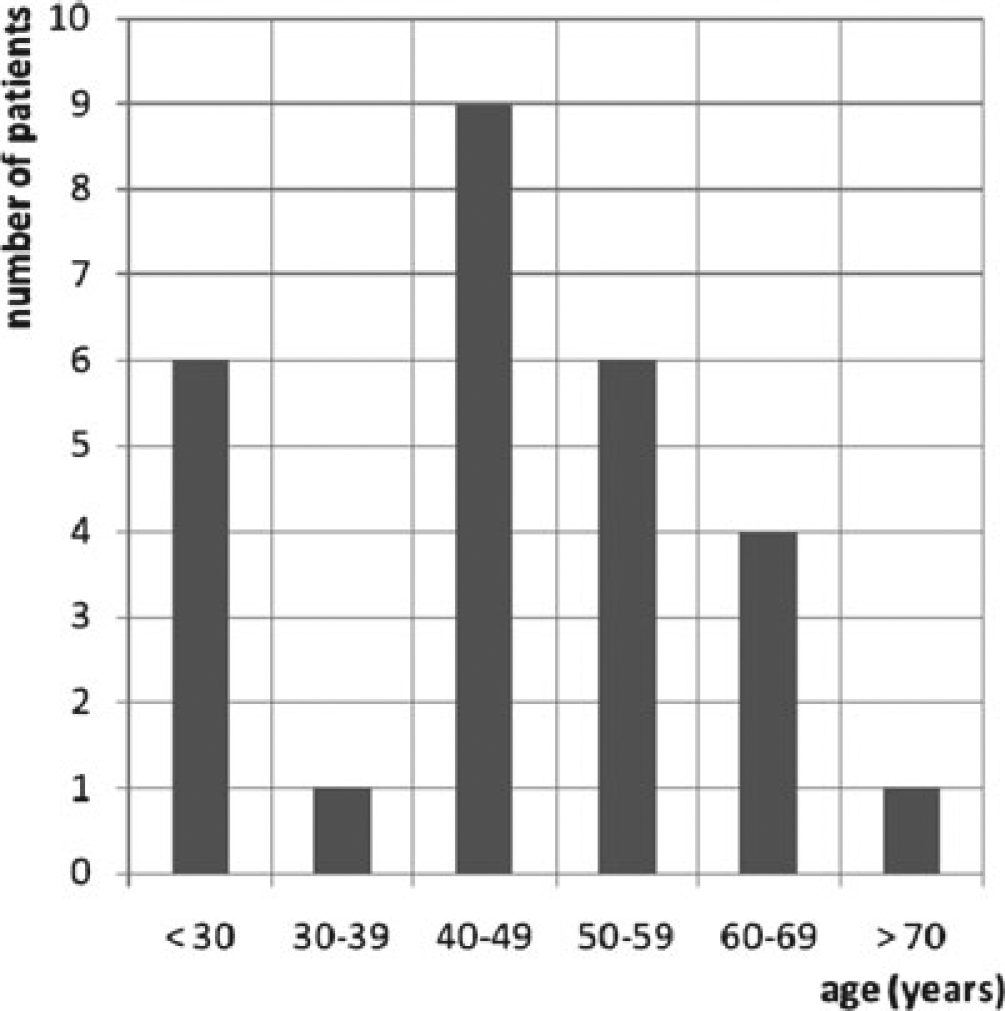
Age distribution.
Indications for shoulder arthrodesis were primary (n = 2) or secondary glenohumeral osteoarthritis (septic or post-traumatic, n = 6), salvage after failed arthroplasty (n = 5) and recurrent shoulder dislocations (n = 13), despite one or more previous operative procedures such as reversed Putti Platt, Bristow or capsulorrhaphy. In two patients, shoulder arthrodesis was performed for a traumatic brachial plexus lesion with paralysis of shoulder muscles.
Surgical technique
After positioning of the patient in a beach-chair position, the operation was performed using a lateral approach without sacrificing the axillary nerve to preserve the deltoid muscle. After exposure of the glenohumeral joint, the articular and acromial surfaces were decorticated. With the humerus in relation to the scapula, the glenohumeral positions selected were: 10° to 40° abduction (mean 23.6°); 15° to 30° forward flexion (mean 26.3°); and 20° to 45° internal rotation (mean 33.6°). For proper compression of the humeral head onto the glenoid and acromion in 12 cases (43%), an AO-plate was used in combination with cancellous screws (range two to four screws) (Fig. 3a) and, in 16 cases (57%), only cancellous screws (range two to six screws) were used (Fig. 3b). After operation, the shoulder was immobilized in a humeral abduction cast for 3 months.
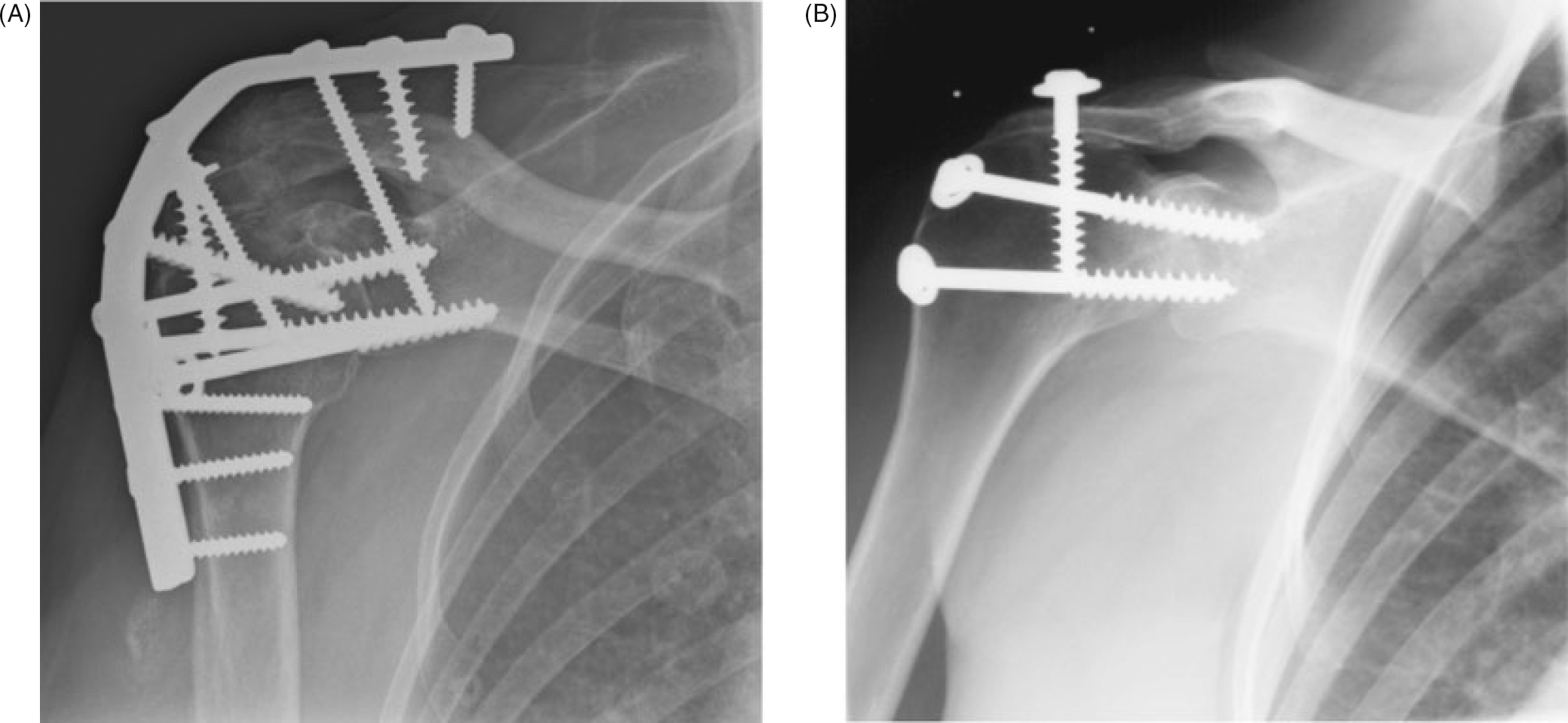
(A) Shoulder arthrodesis performed through combined plate/screw fixation. (B) Shoulder arthrodesis performed through screw fixation alone.
Follow-up and clinical evaluation
The mean time to follow-up examination was 6.8 years (range 1 years to 20.4 years) (Fig. 4). Unfortunately, four patients died as a result of cardiorespiratory pathology or metastasized lung cancer. Three patients could not be contacted and were lost to follow-up. Therefore, 20 patients with 21 shoulder arthrodesis (combined plate/screw arthrodesis in 11 cases, screw arthrodesis in 10 cases) were available for clinical evaluation. First, patients were asked to rank postoperative function and strength on a visual analogue scale (VAS) from 0 to 10 (0 = normal function and strength; 10 = no function and strength). They also ranked work, sport activities, pain and satisfaction in the same manner (0 = normal work, sport activities, no pain and very satisfied; 10 = inability to work, no sport activities, severe pain and very dissatisfied).
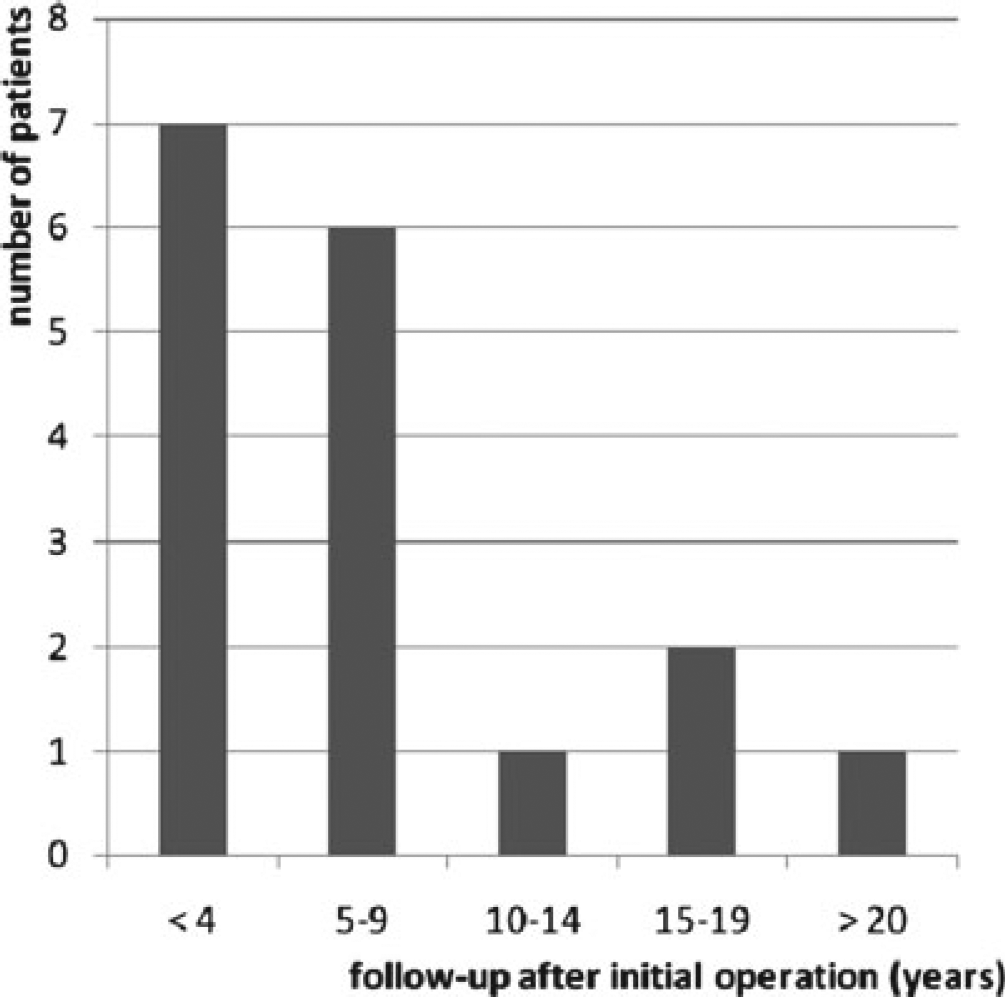
Follow-up examination in years after the intial operation. The mean time to follow-up examination was 6.8 years.
Second, postoperative function and outcome were evaluated using the Constant–Murley score, which is based on both subjective and objective parameters [10], [11]. This postoperative assessment was compared with the pre-operative scores that were registered before operation and recorded in the patient records.
Finally, secondary operations and complications both early (during the first 30 days postoperatively) and late (after the first postoperative month) were recorded by retrospectively analyzing patient records or taken from patients history.
Statistical analysis was performed using SPSS, version 16.0 (SPSS Inc., Chicago, IL, USA). Because the variables did not have a normal distribution, the results are presented as the median and minimum, as well as maximum. Wilcoxon's signed ranks test was used to detect statistically significant differences in the Constant–Murley score between pre-operative and postoperative scores for both plate/screw and screw alone groups. In all analyses, p < 0.05 (two-sided) was considered statistically significant.
Results
All patients had severe limitations in the use of their shoulder, with mean VAS scores for daily function, work and sport activity of 5.4 (range 0 to 9), 4.7 (range 0 to 9) and 6.7 (range 0 to 9), respectively. Most patients were unable to comb their hair, although they were able to reach their mouth and their back pocket. Seven patients were highly dependent on their environment, because they were unable to perform toilet hygiene or reach above xyphoid level. They also experienced severe problems with work and sport activities (VAS 7 to 9). Despite these severe limitations, there was little pain (mean VAS 2.5, range 0 to 9) and these patients were satisfied (mean VAS 2.8, range 0 to 9). Three patients did not experience any improvement as a result of persistent complaints from non-union, scapular winging or severe impairment from bilateral shoulder arthrodesis.
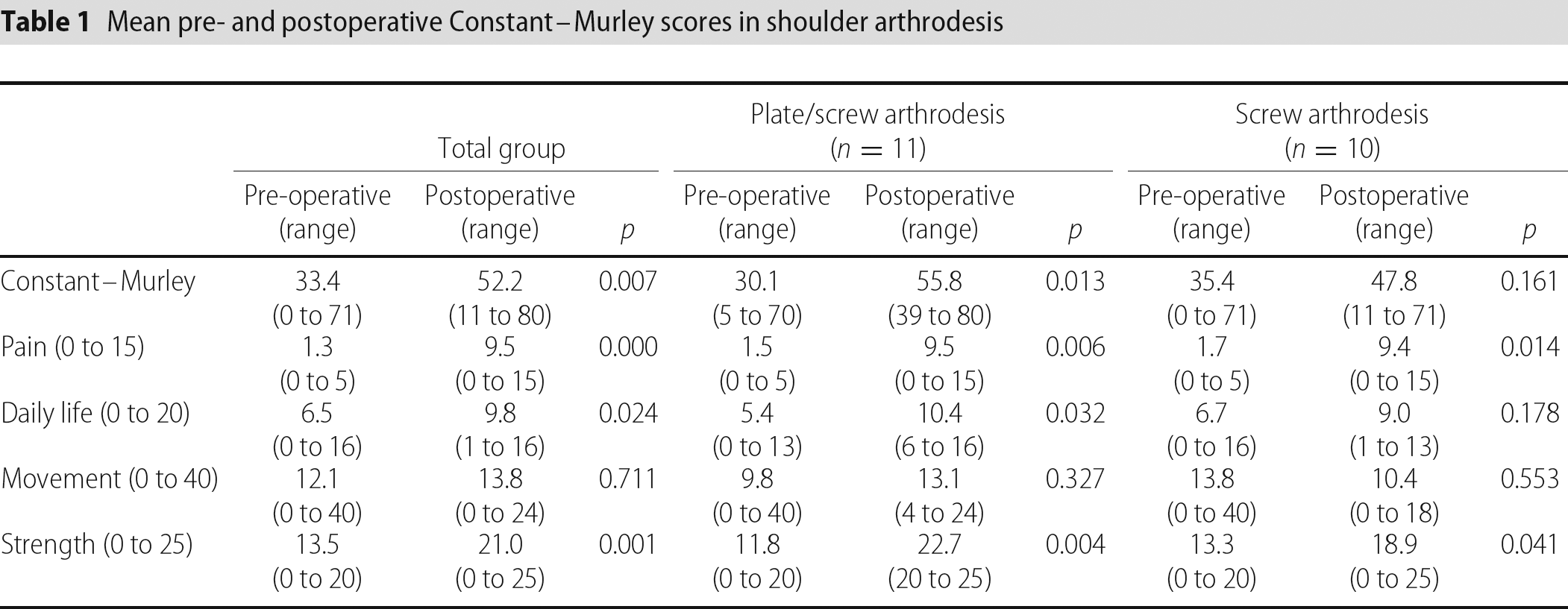
The overall Constant–Murley score (Table 1) increased significantly from 33.4 points pre-operatively to 52.2 points postoperatively, which is mainly the result of a significant decrease in pain and secondary improvements in strength and daily life. In four patients (two patients had also high VAS scores), a decrease in the postoperative Constant–Murley score was recorded. In these cases, this was the result of decreased range of motion.
Mean pre- and postoperative Constant–Murley scores in shoulder arthrodesis
With regard to complications, some patients had more than one complication. Three patients had an early surgical complication: wound infection, haematoma and pneumothorax, which occurred twice in one patient (Table 2). One patient without respiratory or cardiovascular history died 2 days after operation as a result of respiratory problems, and a deep venous thrombosis in the lower extremity was found in a 68-year-old patient after prolonged immobilization.
Complications in shoulder arthrodesis
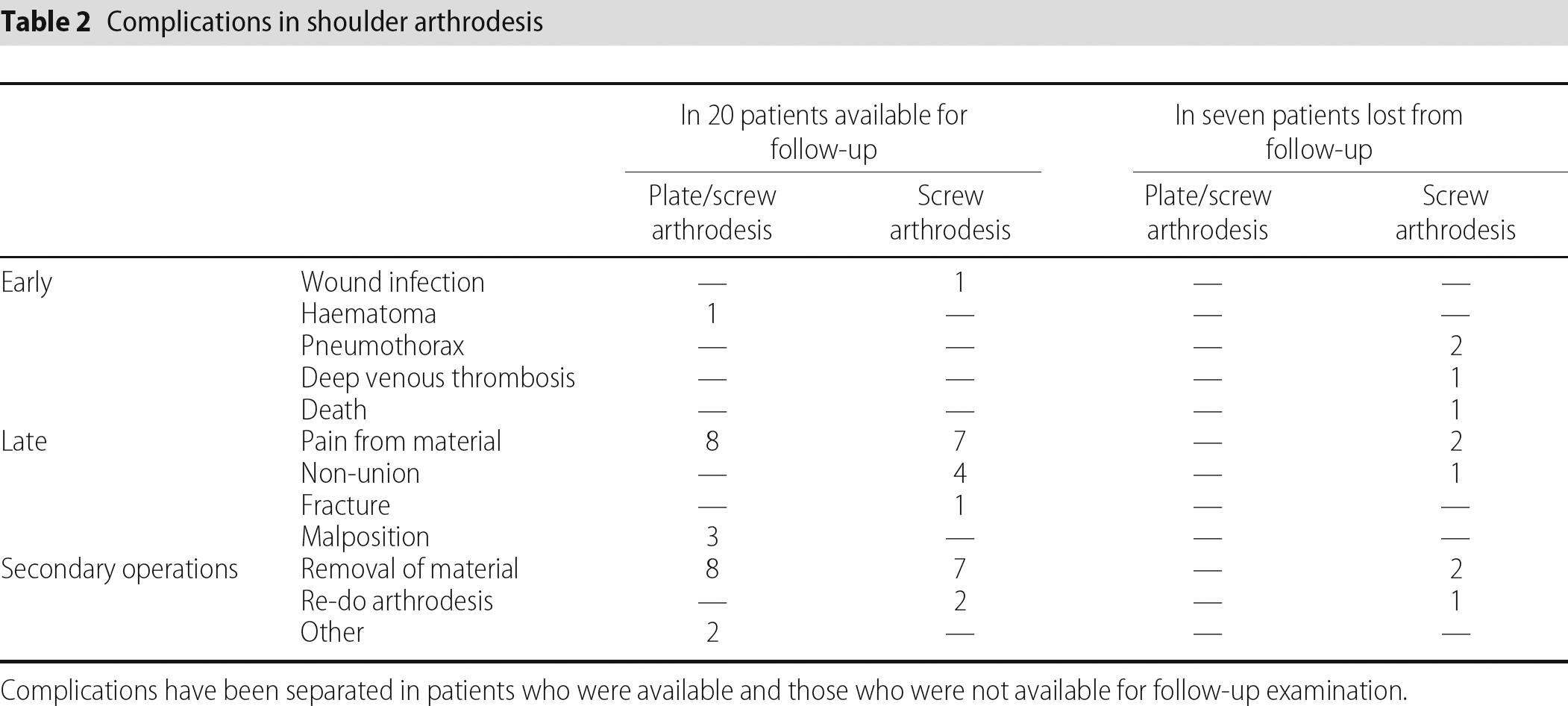
Complications have been separated in patients who were available and those who were not available for follow-up examination.
When considering the total group including the patients lost to follow-up, late complications were seen in 21 patients (75%). In eight cases with combined plate/screw arthrodesis and nine with screw arthrodesis, there was persistent pain, which resolved after removal of osteosynthesis material. In five patients with screw arthrodesis, non-union was found; three patients had a successful re-operation, one patient was successfully treated with an electromagnetic pulse system to stimulate bone growth and, in one patient with a poor pre-operative general condition (American Society of Anesthesiology IV), non-union was accepted after failure of the electromagnetic pulse system. Non-union was not found in combined plate/screw arthrodesis.
One patient was treated 3 months with a humeral abduction cast for late postoperative upper arm fracture and two patients had other procedures: one acromioclavicular resection was performed for persistent pain from acromioclavicular osteoarthritis and a biceps tenodesis was performed for severe degenerative tendinopathy. Finally, three patients complained of a persistent, dull and aching pain in the shoulder and scapulothoracic area as a result of overload from scapular winging after malposition of the shoulder arthrodesis (flexion >30°). All three had a combined plate/screw arthrodesis.
Discussion
In the present study, we found three patients out of the 20 available patients (15%) who were still experiencing severe pain postoperatively. These patients were very dissatisfied because of complications; one non-union and one scapulothoracic overload as a result of winging of the scapula in a malpositioned (specifically in flexion) shoulder arthrodesis. One patient is severely impaired as a result of bilateral shoulder arthrodesis. Despite the disappointing results for these three patients, the remaining patients had a subjective improvement in pain and satisfaction, although pre-operative VAS scores were lacking. Even scores for strength, ability to work, participation in sport activities and function improved subjectively according to the patients. This is in accordance with significant improvements in pain (p = 0.000), daily life (p = 0.024) and strength (p = 0.001) when considering the pre-and postoperative recorded Constant–Murley scores.
Postoperative function after shoulder arthrodesis primarily depends on scapulothoracic mobility and the chosen position of the arthrodesis. The optimal position has been discussed exhaustively in the literature, although consensus on this matter has not yet been reached. Various studies [12], [13] found that abduction and flexion over 40° forced the scapula to rotate and wing excessively producing pain, especially when the shoulder was at rest with the arm at the side. Richards et al. recommended a position of 30° abduction, forward flexion and internal rotation, enabling patients to reach their mouth and perform toilet hygiene [14]. Nagy et al. tried to find an optimal position for performing a shoulder arthrodesis [15]. They found no single optimal position using clinical examination and computed tomography scans. They suggested an abduction in the range 35° to 45°, forward flexion in the range 15° to 30° and internal rotation in the range 30° to 40°, a position that also has been recommended in other studies [16], [17]. In our hospitals, we aimed for the same positions, which resulted in approximately 25° abduction (range 10° to 40°), 25° forward flexion (range 15° to 30°) and 35° internal rotation (range 20° to 45°).
When shoulder arthrodesis is performed in the recommended position, different studies [9], [18] report good to excellent results. In their small groups (n = 24 to 43 cases) with mixed indications, it was found that approximately 80% to 90% of their patients were satisfied and experienced pain relief. This is supported by the findings of the present study.
Although patients were satisfied subjectively, a high rate of late complications was still found, which is in contrast to the complication rates reported in the literature. However, only a few studies [8], [14], [19], [20] consider the removal of osteosynthetic material as a postoperative complication and it usually is classified under secondary operations. In the present study, this means that, if we were to consider the removal of osteosynthetic material as a secondary procedure rather than a complication, the late complication rate drops to 30%, which corresponds to the reported rates in literature.
The aim of shoulder arthrodesis is a decrease in pain, with the achievement of complete fusion of the humerus-glenoid and humerus-acromion. This can be achieved by varying techniques, of which screw arthrodesis and combined plate/screw arthrodesis are the most popular. Frequently, the shoulder arthrodesis is supported postoperatively by a rigid immobilization technique such as a humeral abduction cast for 6 to 12 weeks. Despite immobilization, non-union has been reported frequently, varying from 0% [7] to 40% [21] for screw arthrodesis and from 0% [19], [22] to 18% [23] for combined plate/screw arthrodesis. A systemic review of the literature by Ruhmann et al. also showed that nonunion is reported more frequently in screw arthrodesis (14 of 111 cases in the literature = 13%), although a difference with combined plate/screw arthrodesis (16 of 210 cases in the literature = 8%) appears to be absent [5].
When tested in vitro, screw arthrodesis in fresh cadaveric specimens with three humerus-glenoid screws was significantly more stable in anteversion and retroversion stress than was a 16-hole plate arthrodesis (the difference between the two techniques in abduction and adduction stress was insignificant). Therefore, screw arthrodesis with three humerus-glenoid screws is considered superior to combined plate/screw arthrodesis and may reduce non-union [24].
However, this is contested by Miller et al. who found a combined plate/screw arthrodesis in fresh human cadaveric specimens to be the most rigid fixation technique with the greatest bending and humeral torsional stiffness, whereas screw arthrodesis was found to be the least rigid technique [25]. This suggests that screw arthrodesis is inferior to combined plate/screw arthrodesis and non-union would occur more often in screw arthrodesis than combined plate/screw arthrodesis. This is supported by the findings of the present study, where non-union occurred in five patients, who had all undergone a shoulder arthrodesis with only cancellous screws. Non-union did not occur in the combined plate/screw fixation.
Conclusions
Although shoulder arthrodesis has a large impact on a patient's daily life and movements are severely limited, patient satisfaction after arthrodesis is high. Shoulder arthrodesis is a technically demanding procedure, where the operative technique and position of the arthrodesis appear to be essential. Because the indications for this procedure have been narrowed and procedures are limited in number, it should be done in only a few specialized centres.
Because a long revalidation period is necessary for complete glenohumeral fusion and a relatively high risk of late complications (non-union) and secondary operations (removal of material) is noted, shoulder arthrodesis should not be taken lightly and should be considered as a salvage procedure. A combined screw/plate fixation offers the best option for avoiding non-union of the arthrodesis.