
Abstract
Background
Lateral epicondylitis has been studied mainly in work related and occupational groups, however little is known about the incidence or demographic associations in the general population. We have undertaken a large study using The Health Improvement Network (THIN) database to examine the epidemiology of lateral epicondylitis in the UK general population.
Methods
Diagnoses of lateral epicondylitis between 1987 and 2006 were used to calculate the incidence stratified by age, gender, deprivation score, UK health authority, and year. The age standardised rates for lateral epicondylitis in the UK were calculated with reference to the European Standard Population.
Results
The incidence rate of lateral epicondylitis was 2.45 per 1000 person-years. This was more common in males than females (males 2.63, females 2.55 per 1000 person-years, p < 0.001). After direct standardization, the age adjusted rates were 2.38 for males and 2.43 for females.
The highest incidence rate of 7.35 per 1000 person-years was found in the age group 45-50 years. Regional distribution of the incidence rates showed a fairly even spread across 13 UK Health Authorities with the exception of London where incidence rates were significantly lower (1.75 per 1000 person-years, p < 0.001). Social deprivation was assessed using the Townsend score. The least deprived areas of the population had the highest incidence rates (2.86 per 1000 person years).
Conclusions
Our study represents the largest general population study of lateral epicondylitis reported to date. The results obtained provide the clinician with a better understanding of the epidemiology of lateral epicondylitis in the community.
Introduction
Lateral Epicondylitis is a common musculoskeletal condition seen frequently by clinicians in both primary and secondary care. Despite this, data are scarce with respect to the incidence of lateral epicondylitis in the general population and how this varies with demographic factors, such as age, gender and socioeconomic status.
Lateral epicondylitis causes significant disability, especially in the working population, who are unable to carry out manual tasks. During 1995 alone, 3.8 million working days were lost in Britain as a result of upper limb disorders [1]. Work absence in turn has financial implications both for the individual patient and society at large.
Estimates of prevalence vary widely and studies often focus on specific occupational groups [2-8], limited population studies [9-11] or small general practice studies [12]. There are few large general population studies. Walker-Bone et al. screened 9696 working age adults by questionnaire to permit a focused physical examination and estimated the prevalence of lateral epicondylitis to be 1.3% in males and 1.1% in females [11]. Shiri et al. examined 4783 adults aged 30 years to 64 years in Finland and found the prevalence of definite lateral epicondylitis to be 1.2% in males and 1.4% in females [10]. Roquelaure et al. found the prevalence of lateral epicondylitis in 3710 French workers to be 2.5% in males and 2.7% in females, respectively [9].
We aimed to overcome the size limitations of previous studies by using The Health Improvement Network (THIN), a large-scale source of longitudinal data from general practice records. We examined the incidence rates by age, gender, regional distribution and socioeconomic status aiming to further clarify the epidemiology of lateral epicondylitis in the general UK population.
Materials and Methods
The THIN database was utilized for the present study. The data represent the computerized recordings of routine patient care from 479 general practices in the UK. The total number of patient records held is 9.15 million, with 3.36 million current active patients comprising approximately 5.7% of the UK population. Each general practice provides prospectively-acquired, fully-coded demographic, medical and prescription data to THIN; these data are not patient-identifiable. The THIN database is subject to regular audit and verification processes to provide quality assurance.
Patients
Data were extracted using Read codes; an National Health Service patient data coding system used in UK general practices. These map other coding systems including The International Classification of Diseases, ninth revision, and the Classification of Surgical Operations & Procedures, fourth revision.
Read codes specific for lateral epicondylitis were identified and used to extract the records of all patients in the database with a first recorded date of diagnosis between 1 January 1987 and 31 December 2006.
Patients who move their registration between general practices have their past medical histories coded at their new practice; this is standard practice. This leads to an acquisition bias in the THIN database; the incidence rate of a condition may be artificially inflated because the diagnosis of that condition may have been made many years previously, although the coded date of diagnosis may be the date of registration at that practice. To remove this effect, we excluded all diagnoses made within the first 6 months of a patient's registration period with their general practice. The ‘crude’ rates in the data are after this exclusion.
For each case of lateral epicondylitis, we extracted data on age, gender, deprivation score, UK health authority and year of first diagnosis. The deprivation score was based on the Townsend score [13]. This represents an index of socioeconomic deprivation in the range 1 to 5, with high scores relating to higher deprivation. Patients were grouped by age in intervals of 5 years for ease of analysis.
The age group incidence rates were adjusted with reference to the 1999 WHO European standard population [14] to obtain age-adjusted incidence rates.
Statistical analysis
The STATA software package, version 10 (StataCorp, College Station, TX, USA) was used for the statistical analysis. Incidence rates per 1000 person-years and 95% confidence intervals were calculated using Poisson regression analysis and compared using a chi-squared test for proportions. Age-adjusted incidence rates for lateral epicondylitis were calculated based on the European standard population using the direct standardization method.
The Poisson regression model was utilized to analyze the effect of age groups, gender, health authority and socioeconomic score on the incidence of lateral epicondylitis. The nested models were compared using the log-likelihood criterion. p < 0.05 was considered statistically significant.
Results
Our dataset included over 3.7 million patient records of which there were an average of 1.8 million active patient records per year throughout the study period. Over a 20-year period from 1987 to 2006 inclusive, 90,472 first diagnoses of lateral epicondylitis were recorded.
Overall incidence
The overall crude incidence rate of lateral epicondylitis in our cohort between 1987 and 2006 was 2.45 per 1000 person-years [95% confidence interval (CI) = 2.43 to 2.46]. The incidence rate in males during this period was 2.63 (95% CI = 2.60 to 2.65) and was significantly higher than in females whose incidence rate was 2.55 (95% CI = 2.53 to 2.58) per 1000 person-years; p < 0.001).
The crude age incidence rates were adjusted with reference to the 1999 WHO European standard population [14] to obtain age-adjusted incidence rates. The adjusted incidence rate for males was 2.38 (95% CI = 2.36 to 2.40), although the incidence rate for females was significantly higher (incidence rate = 2.42; 95% CI = 2.40 to 2.45 per 1000 person-years; p < 0.001).
Age- and gender-based analysis
The incidence rate of lateral epicondylitis was related to age (Fig. 1) and higher rates were found in the age group aged 40 years to 54 years. The peak incidence rate was highest in the 45-year to 49-year-olds (incidence rate = 7.35; 95% CI = 7.23 to 7.45)
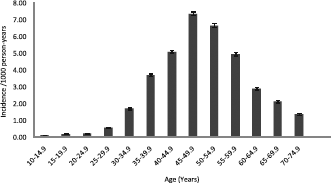
Lateral epicondylitis incidence by age group.
We further stratified the incidence rate according to age group and gender. Females in the age group 40 years to 54 years had a significantly higher incidence rate than males in the same age category; however, throughout all higher and lower age groups, the male population showed a higher incidence rate than females (Fig. 2).
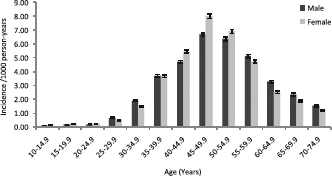
Lateral epicondylitis incidence by age group subdivided by gender.
Incidence by deprivation
We used the Townsend deprivation index [13] to further analyse the incidence rate of lateral epicondylitis. The least deprived group (Townsend score: quintile 1) had the highest incidence rate of 2.86 (95% CI = 2.82 to 2.89). The incidence rate decreased such that the most deprived group (Townsend score: quintile 5) had an incidence rate of 2.00 (95% CI = 1.95 to 2.04).
Adjusted incidence rates were then calculated by deprivation score (Fig. 3), with a similar trend of decreasing incidence rate between Townsend quintile one (incidence rate = 2.54, 95% CI = 2.51 to 2.58) and Townsend quintile five (incidence rate = 2.26, 95% CI = 2.22 to 2.31).
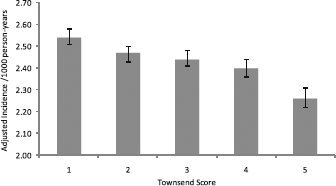
Lateral epicondylitis adjusted incidence rate by deprivation quintile.
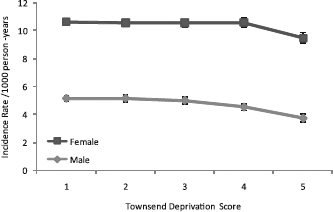
The deprivation score quintiles were further stratified according to gender (Fig. 4). Within the Townsend quintile one population, the incidence rate was higher in males (incidence rate = 2.97; 95% CI = 2.92 to 3.01) than females (incidence rate = 2.76; 95% CI = 2.71 to 2.81; p < 0.001). This relationship was reversed in Townsend quintile five, where the female incidence rate (incidence rate = 2.11; 95% CI = 2.06 to 2.18) exceeded the male incidence rate (incidence rate = 1.88; 95% CI = 1.83 to 1.94; p < 0.001).
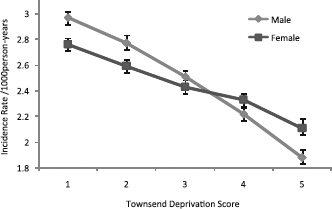
Lateral epicondylitis incidence rate by deprivation quintile subdivided by gender.
The deprivation score was further examined in the age group 40 years to 49 years, where the incidence rate of lateral epicondylitis is the highest (Fig. 5). Within these age groups, the incidence rate of lateral epicondylitis in females is not significantly different between Townsend quintiles one and five. However, the male incidence rate in quintile 5 is significantly less than quintile 1.
Lateral epicondylitis incidence rate by deprivation quintile subdivided by gender-specific age groups.
Incidence rates by geographical area
We compared the incidence rate of lateral epicondylitis in 13 health authorities across the UK for which data were available (Fig. 6). Incidence rates were comparable for all regions (range 2.05 to 2.68), except London where the incidence rate was 1.75. Adjusted incidence rates also confirm London as an outlier.
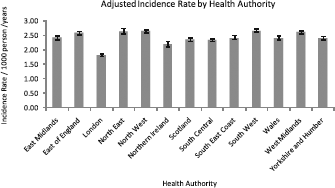
Lateral epicondylitis incidence rate by UK health authority.
Incidence rates over time
Over a period of 20 years, the crude and adjusted incidence rate has fluctuated between 1.5 and 3 (Fig. 7). The incidence rate was lower in the first 4 years (1987 to 1990) and there was a further dip during the years 1995 to 1999.
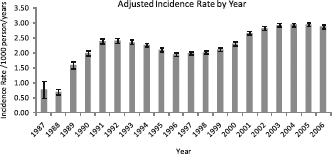
Lateral epicondylitis incidence rate per year.
Discussion
Main findings
We have analyzed the incidence of lateral epicondylitis in the UK general population and further examined the effect of age, gender and social deprivation on these rates. The overall incidence rate of lateral epicondylitis was 2.45 per 1000 person-years. This was more common in males than females. After direct standardization, the age adjusted rates were 2.38 for males and 2.43 for females.
Highest crude incidence rates were found in the group aged 45 years to 55 years. Between the ages of 40 years to 54 years, females had the highest incidence rates. The least deprived areas of the population had the highest incidence rates (2.86 per 1000 person-years). Regional distribution of the incidence rates showed a fairly even spread across 13 UK Health Authorities, with the exception of London where incidence rates were significantly lower.
Strengths and limitations
The data employed in the present study are acquired from computerized general practice records used for routine clinical care. This has the advantage of reflecting real-life experience rather than the research setting, and being a prospective continuous data collection that avoids recall bias. One disadvantage, however, is that the general practitioner is likely to have made the diagnosis of lateral epicondylitis on varying strengths of clinical suspicion and without referral to a musculoskeletal specialist. However Herrett et al. found that estimates of the validity of data within the General Practice Research Database (GPRD) were high [15]. The GPRD is the formative name for THIN database.
Other studies using general practice computerized records to examine musculoskeletal conditions such as carpal tunnel syndrome [16] and Dupuytren's disease [17] found the data to be valid when examining the database for cases that had undergone surgical intervention. This type of analysis was not appropriate for lateral epicondylitis, which is mainly managed in the community, and is surgically treated in a minority of cases.
The presenting features of lateral epicondylitis are quite specific but studies use varying diagnostic criteria. Consensus on diagnostic criteria for upper limb disorders in a work setting was reached in 1998 [18]. Davis suggested that the specific criteria to be used in epidemiological studies of lateral epicondylitis should include; lateral epicondylar pain and epicondylar tenderness and pain on resisted extension of the wrist [19]. It is quite likely, however, that general practitioners have a heterogenous set of diagnostic criteria for an entry of lateral epicondylitis into the patient record. Indeed, it is impossible to confirm on what basis the recorded diagnoses were made in the THIN database. However, data from practices are routinely validated by internal checks and there are specific audits of the data supplied by individual practices. Only data meeting the minimum standards are added to the research database. It is probable, however, that a diagnosis of lateral epicondylitis has a good specificity but low sensitivity.
Comparison with the existing literature
Most previous studies either examined a cohort of patients or screened a population using surveys and questionnaires to identify a specific subsection of the population for further examination. The reliance of such studies on physical examination obviously limits the number of participants that can be included and therefore reduces the power of subsequent analysis. Only one other study that we identified used a population database, although these data were restricted to members of the US military [5].
Walker-Bone et al. used a two-staged cross-sectional study employing a screening questionnaire and physical examination in symptomatic individuals [5]. It is likely that this design permits improvements in sensitivity and specificity, although the total number of subjects (n = 9969) is still very small compared to the present study. They estimated the prevalence of lateral epicondylitis to be 1.3% in males and 1.1% in females. This value is lower than the incidence reported in the present study, although it is important to note that the point prevalence may be lower than the annual incidence because the condition is likely to be relapsing and remitting.
It is interesting to observe that males have a higher crude incidence rate than females, whereas females have a significantly higher adjusted incidence rate.
Social deprivation was assessed using the Townsend score. The findings of the present study are interesting because they suggest that lateral epicondylitis is mainly a disease of the higher socioeconomic groups. This is in conflict with previously held assumptions suggesting that lateral epicondylitis is a disease of manual workers. Unfortunately, a population study of this size was unable to examine occupation, sporting and social activities. Further well designed large-scale population studies are required to assess the impact of these factors.
The reason for the fluctuation in incidence rates over the period of the study data is uncertain. It is possible that progressive computerization means that, as practices join THIN, their data are coded retrospectively. This may result in an over-reporting of incidence in later years.
Conclusions
The present study represents the largest general population study of lateral epicondylitis reported to date. The results obtained provide the clinician with a better understanding of the epidemiology of lateral epicondylitis in the community.
Although none of the authors has received or will receive benefits for personal or professional use from a commercial party related directly or indirectly to the subject of this article, benefits have been or will be received but will be directed solely to a research fund, foundation, educational institution or other nonprofit organization with which one or more of the authors are associated. Richard Hubbard is a Wellcome Trust Advanced Fellow.
Footnotes
None declared