
Abstract
We present a case of extreme glenohumeral dysmorphism with pain and arthropathy which benefited from a Computer-Aided Design and Computer-Aided Manufacture (CADCAM) ‘Piggy-Back’ reverse total shoulder arthroplasty.
Introduction
Computer-Aided Design and Computer-Aided Manufacture (CADCAM) shoulder arthroplasty is used to fabricate a custom fit prosthesis where a lack of bone stock does not permit an ‘off-the shelf’ total shoulder replacement, including an ‘off-the-shelf’ reverse prosthesis. CADCAM shoulder arthroplasty has been used at our tertiary referral centre for over 10 years, facilitating complex primary reconstruction of the glenohumeral joint and revision arthroplasty [1]. We report a case of extreme glenohumeral dysmorphism with pain and arthropathy, which benefited from a CADCAM ‘Piggy-Back’ reverse total shoulder arthroplasty.
Case Report
Pre-operative clinical assessment and treatment proposal
A 17-year-old man with Type 1 neurofibromatosis (Von Recklinghausen's disease) with associated skeletal dysplasia presented with poor function and a painful right shoulder. He had been diagnosed with Type 1 neurofibromatosis at the age of 15 years. Examination revealed cutaneous signs of neurofibromatosis, cervicodorsal kyphoscoliosis and marked wasting of the muscles around the right shoulder and proximal arm. There was weakness of the deltoid, serratus anterior, trapezius and the rotator cuff, although he had normal sensation and power in all other limbs. Radiographs (Fig. 1) revealed a highly disorganized right shoulder with absent glenoid and humeral head, and a narrow humeral shaft. Scalloping of the lateral border of the scapula was also noted, suggesting the presence of a neurofibroma. Brain, spine and shoulder magnetic resonance imaging scanning and electromyography were carried out. A large plexiform neurofibroma was demonstrated, predominantly involving the entire right brachial plexus. A dystrophic spine with kyphoscoliosis and multiple neurofibromas (in particular, a very large suboccipital neurofibroma from the occiput to C6 and further lesions in the mid to lower cervical spine) were also demonstrated. His pain was initially well controlled with conservative treatment. He developed cervical instability and an occipito-cervico-thoracic fusion was performed at the age of 22 years. Shoulder pain and function subsequently deteriorated. Although some power and muscle bulk had returned after the occipitospinal stabilization, humero-scapula movement was absent. The residual acromion had enveloped the posterior and lateral humeral shaft and had dissociated by approximately 7 cm from the distal clavicle, leaving the residual humeral head trapped between the scapula and the clavicle (as if a ball held between tongs; Fig. 2a, b). Surgical options were limited. A shoulder fusion was unlikely to be successful as a result of the extensive bone loss and the poor scapulothoracic control, which opposed the patient's wish for active functional movement. An arthrodesis of the glenohumeral joint would have restricted him to either hand-to-face or hand-to-back activity, and not both. He wished to retain both fields of motion and so arthrodesis was not a function-preserving option for him.

Preoperative AP right shoulder showing the abnormal anatomy of the shoulder.
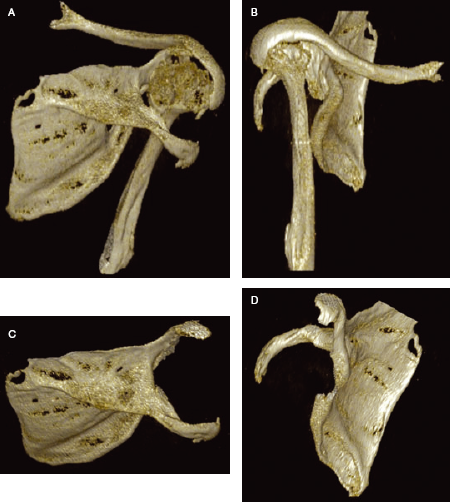
3D CT reconstruction of the right shoulder. (A-B) Bony anatomy of the scapulahumeral articulation. (C-D) Bony anatomy of the scapula after digital subtraction of the humerus.
CADCAM arthroplasty presented a reasonable option. The patient was 24 years old at the time of his shoulder surgery.
Pre-operative planning
CT (Philips Brilliance, 64 slice, slice thickness-2 mm, dose DLP 571.05 mgy/cm; Philips Heathcare, Best, The Netherlands) was undertaken to assess the deformity, as well as to plan, design and manufacture the CADCAM implant. Figure 3 shows an axial cut at the level of the humeral head and Fig. 2(A, B) provides a three-dimensional reconstruction of the abnormal bony anatomy around the shoulder. Figure 2(C, D) illustrates the morphology of the scapula and the complete lack of glenoid. Clinical and magnetic resonance imaging assessment suggested that the supraspinatus and subscapularis were completely deficient and a reverse-polarity prosthesis was indicated. Poor deltoid anatomy and function required a fixed-fulcrum design. Conventional or augmented glenoid fixation was impossible as a result of the extensive lateral scapular deficiency and so a device that relied on fixation to the posterior surface of the scapula was designed. The design of the prosthesis had to ensure the maximum possible number of points of fixation possible in a situation where simple fixation into the glenoid was impossible. This allowed it to load-share over a larger area. The proximal humerus was of small calibre with an almost absent medullary canal precluding the use of a conventional medullary stem. A triplate fixation mechanism was designed to fit on the outer surface of the humerus (Fig. 4; reproduced with permission from Stanmore Implants, Middlesex, UK). We refer to this fixation as ‘piggy back’, implying exoskeletal fixation as opposed to conventional intra-osseous fixation. Both prostheses were coated with hydroxy-apatite to encourage bone on-growth.
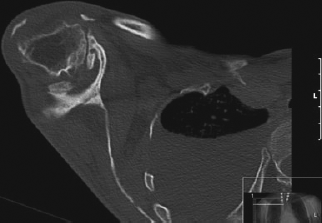
Axial CT right shoulder showing the extensive bone loss from the scapula with no true glenoid and associated arthritic changes in the glenohumeral joint.
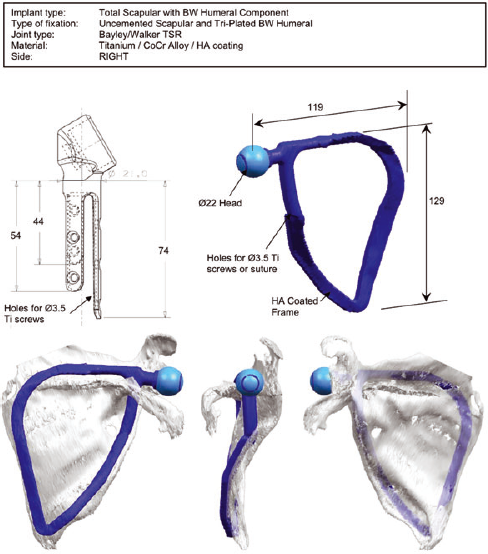
Computer generated schematic diagrams of the CADCAM design.
Operation and postoperative care
The operation was carried out under general anaesthetic in the lateral decubitus position. The incision was an inverted horseshoe: a combination of Ollier (sub-deltoid), Judet (sub-infraspinatus) and deltopectoral approaches to the shoulder were used.
The operative findings confirmed the complex deformities and deficiencies noted on the pre-operative imaging. There was no glenoid, and no acromioclavicular joint. The trapezius and infraspinatus muscles were of good quality. There was a plexiform neuroma of the infraspinatus branch of the suprascapular nerve, although this was preserved to protect the good function of the infraspinatus. The infraspinatus was elevated using the Judet approach and dissection was carried out laterally to the back of the humeral head. The deltoid was elevated subperiosteally from the humerus and reflected from the spine of scapula, folding it laterally, noting the entry of the axillary neurovascular bundle. The trapezius was elevated from the spine of scapula, which was then excised to expose the supraspinatus fossa. The infraspinatus tendon was identified and the humeral head exposed by reflecting residual cuff and bursal tissue. A provisional humeral shaft osteotomy and excision of the proximal humerus was performed. The scapular prosthesis was positioned and fixed with screws. Calcium trisilicate putty (Actifuse, Apatech, Hertfordshire, UK) was placed around the plate/bone junction. The humerus was exposed anteriorly through the deltopectoral approach and a pectoralis major tenotomy was performed. The humeral shaft was delivered anteriorly to protect the axillary neurovascular bundle and the definitive humeral osteotomy performed. The humeral prosthesis was secured to the shaft with five transosseous screws with excellent fit and hold. Actifuse putty was again used and packed around the plate to encourage incorporation. The prostheses were then mated. The infraspinatus was repaired to the plate and the deep thoracoscapular fascia. The deltoid was repaired: because it was a shortened muscle, the posterior fibres were vertical. The trapezius fascia was sutured to the infraspinatus fascia. There was no impingement between the prosthesis and the residual clavicle. The construct was protected in a sling with body band for 6 weeks to permit bone on-growth. Hand, wrist and elbow ranging were allowed. Active-assisted sagittal flexion and functional rotation at waist level was commenced under the supervision of a physiotherapist at 6 weeks. The 2-year follow-up clinical and radiological results are shown in Fig. 5. The pre-operative status and the outcome at 1 and 2 years postoperatively were assessed by the Oxford Shoulder Score [2], the Stanmore Percentage of Normal Shoulder Assessment [3] and a Numeric Rating Score for pain at rest and during movement. Active and passive range of movement was also recorded. There was virtually no scapulothoracic or glenohumeral joint movement in any direction pre-operatively as a result of pain and the aberrant anatomy.
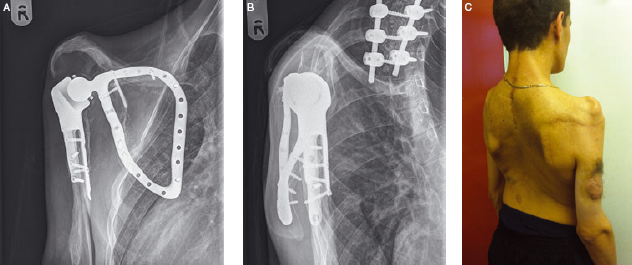
(A-B) Post op Radiographs and (C) Post operative patient photograph.
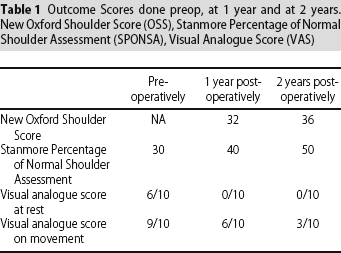
Table 1 summarizes the scores and shows an improvement in all, particularly the Numeric Rating Score. At the most recent review at 2 years, active forward elevation was 45° (passive elevation to 100°). Active external rotation at neutral elevation was 20° (40° passively). Active composite internal rotation was to the L3. Although the patient was unable to reach the top of his head, he was able to reach his mouth and behind his back, as well as to the opposite axilla for personal hygiene.
Outcome Scores done preop, at 1 year and at 2 years. New Oxford Shoulder Score (OSS), Stanmore Percentage of Normal Shoulder Assessment (SPONSA), Visual Analogue Score (VAS)
Discussion
The purpose of surgery in this patient with advanced deformity was primarily to achieve relief of pain. Shoulder fusion was not considered to be a viable option because of the amount of bone loss and poor scapular control.
Pain relief from an excision arthroplasty is unpredictable. If this arthroplasty does fail, then the option of excision arthroplasty remains, although this was not chosen as the primary method of treatment because the unsupported weight of the arm would have been detrimental to the function of the elbow and hand as a result of traction of the massive plexiform neuroma of the brachial plexus behind the clavicle, whereas the control of motion would have been non-existent.
Arthroplasty in dysplastic shoulders is relatively uncommon [4,5]. The risks of arthroplasty include infection, although this has been avoided for 2 years. The risk of periprosthetic fracture is present, although this is no different to risk of occurrence and subsequent outcomes of a fracture around a fusion. The hydroxylapatite-coating permitted surface bone on-growth, thus stabilizing the prosthesis on the scapula; otherwise, the screws would have failed by now: the nonfailure of the screw fixation on the scapula or humerus indirectly means that the implant is stable, and there is no reason to assume that this will now change, unlike a cemented prosthesis.
Good results have been described using bone grafting of the glenoid, although this was not technically feasible in our patient as a result of the extent of lateral scapular bone loss. We regularly use a CADCAM glenoid shell design with divergent screw fixation in the scapula for glenoid deficient shoulders [1] but the very abnormal morphology in this case mandated a novel CADCAM design with a scapular ‘exoskeleton’. The humeral shaft was incorporated using a triplate fixation on the exterior of the humerus because the medullary canal size precluded the use of a conventional stemmed implant. The reverse-polarity but fixed-fulcrum (Bayley-Walker, Stanmore Implants, Middlesex, UK) shoulder replacement provided stability by compensating for rotator cuff deficiency. At 2 years, the patient had improved outcome scores: he was pain free and could undertake the majority of his normal daily activities independently.
Footnotes
None declared