
Abstract
A 51-year-old female underwent an uncomplicated resection of a sigmoid adenocarcinoma. Postoperatively, 12 cycles of the FOLFOX chemotherapy regime were completed, consisting of a combination of folinic acid, 5-fluorouracil and oxaliplatin over a 24 week period. Following chemotherapy, the patient developed simultaneous adhesive capsulitis in both shoulder joints, as radiologically confirmed by magnetic resonance imaging. Bilateral adhesive capsulitis is rare and usually associated with a systemic cause. This case highlights a possible previously unreported association between the widely used FOLFOX chemotherapy regime and bilateral adhesive capsulitis. Oncologists and orthopaedic surgeons should be aware of such presentations in FOLFOX patients to facilitate prompt investigation and management.
Introduction
Adhesive capsulitis of the shoulder (or ‘frozen shoulder’) manifests as chronic pain and gradual deterioration in both passive and active glenohumeral movement as a result of extensive fibrosis and eventual contracture of the glenohumeral joint capsule [1]. It is a relatively common condition, with a reported prevalence of 2% to 5%, typically affecting women aged between 40 years and 60 years [2]. The progression of the disease manifests in three widely recognized stages. In the first stage (freezing stage), early inflammatory changes and reactive synovitis lead to severe shoulder pain and restricted range of motion. The second stage (frozen stage) presents with marked stiffness of the shoulder with significant restriction in everyday activities as a result of pathological capsular thickening. The final stage (thawing stage) is the slow return of normal range of movement and strength.
Bilateral adhesive capsulitis can occur in up to 20% of patients; however, simultaneous bilateral pathology is very uncommon, with the majority of cases being associated with an underlying systemic cause [3]. A previous study by Hutchinson et al. demonstrated a strong association between adhesive capsulitis and a synthetic matrix metalloproteinase (MMP) inhibitor called Marimastat (British Biotech, Oxford, UK), which is used for inoperable gastric carcinoma [4]. To date, no other chemotherapy regimes have been linked with adhesive capsulitis pathology. A significant relationship has also been shown between unilateral adhesive capsulitis and human immunodeficiency virus patients on highly-active antiretroviral therapy, particularly protease inhibitors [5,6].
The FOLFOX chemotherapy regime is widely recognized for the management of advanced colorectal carcinoma. In particular, it is used for adjuvant treatment following curative resection of a tumour invading beyond the muscularis propria [7]. It utilizes the cytotoxic synergy of oxaliplatin and 5-fluorouracil (5-FU). The main recognized side effects of these drugs include oxaliplatin-induced neurotoxicity, gastrointestinal upset and mild haematological toxicity [8]. However, to our knowledge, there are no previous cases or studies reporting an association with adhesive capsulitis.
Case Report
A 51-year-old female university lecturer presented with 1-year history of progressive bilateral shoulder pain and restriction of range of movement with no history of trauma. The left shoulder was symptomatically much worse than the right. Two years previously, she had undergone an anterior resection procedure for a Duke's C sigmoid colon adenocarcinoma. This was followed with 12 adjuvant cycles of the FOLFOX chemotherapy regime over 24 weeks, with the omission of oxaliplatin in the final two cycles as a result of associated neuropathy. Bilateral shoulder pain initially manifested 2 months following the final cycle of chemotherapy, and this gradually worsened with associated stiffness, particularly on the left. There was no other relevant past medical or surgical history, and, specifically, no history of previous shoulder conditions. Medications included paracetamol and ibuprofen as required, which had little effect on her symptoms.
Physical examination revealed bilateral rotator cuff muscle wasting and tenderness of the left acromioclavicular joint (ACJ). There was a gross range of movement restriction in both shoulders with combined elevation of 70° on the left and 120° on the right. External rotation was 20° on the left and 40° on the right. As a result of painful restricted active and passive range of movements in both shoulders, special tests could not be performed. There were no abnormal findings on examination of the cervical spine or neurological system. Clinically, the patient's symptoms and signs were highly suggestive of first-stage adhesive capsulitis.
Plain radiographs of the shoulders revealed mild left ACJ degenerative changes. Magnetic resonance imaging of the left shoulder demonstrated evidence of capsular thickening, focal thickening of the coracoacromial ligament and mild bursal surface irregularity of the supraspinatus rotator cuff suggestive of superior impingement. The right shoulder demonstrated increased soft tissue around the rotator cuff interval with a thickened axillary recess. The combined findings confirmed bilateral shoulder adhesive capsulitis, which was particularly evident on the left shoulder (Fig. 1), with predisposing features of probable left subacromial impingement. There was no evidence of rotator cuff tear, metastatic lesions or avascular necrosis.
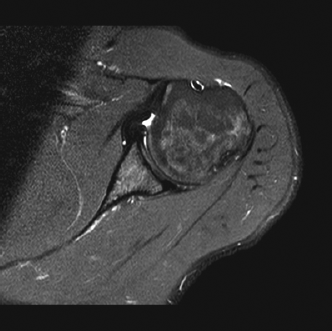
Magnetic resonace image of the shoulder showing evidence of adhesive capsulitis.
The patient initially underwent ultrasound-guided hydrodilatation for capsular stretching of the left shoulder with concurrent intra-articular steroid injection by a radiologist. Hydrodilatation involves the injection of saline under pressure into the glenohumeral joint to stretch the capsule and release adhesions. The combined approach has been shown to significantly improve adhesive capsulitis pain and shoulder range of movement compared to steroid injection alone [9]. Unfortunately, the procedure had to be abandoned in this patient because of excessive pain despite the use of local anaesthesia.
Given the disabling condition of the shoulder and the failure of hydrodilatation therapy, this patient underwent operative management as a day case procedure. Because the left shoulder was more severely affected, it was examined arthroscopically, revealing signs of florid adhesive capsulitis (Fig. 2) with evidence of synovitis within the rotator cuff interval. As a result, arthroscopic capsular release including distension to 120 mmHg for 3 minutes was performed. Bursoscopy of the left shoulder also revealed co-existing signs of impingement and, inview of her radiological findings, it was elected to perform subacromial decompression and ACJ excision at the same sitting. The right shoulder was subsequently manipulated to achieve a full passive range of movement. Postoperatively, the patient recovered well and received intensive physiotherapy. At 6 weeks follow-up, the right shoulder was asymptomatic and the left shoulder demonstrated slower signs of progress. Clinical examination revealed a combined elevation of 90° on the left and 180° on the right, and abduction was 70° on the left and 180° on the right. At 1-year follow-up, there were no reports of pain, stiffness or limitation in activities of daily living. Clinical examination revealed a full range of movement and no signs of impingement or ACJ stress bilaterally.
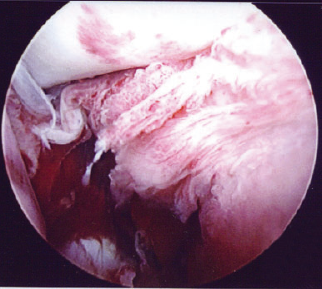
Florid adhesive capsulitis.
Discussion
The present case highlights the strong possibility of a correlation between adhesive capsulitis of the shoulder and the FOLFOX chemotherapy regime, which is used for treating colorectal carcinoma. Many side effects of the drugs used in FOLFOX have been reported by the pharmaceutical industry or in the available literature, including neurotoxicity and gastrointestinal upset, although no associated adhesive capsulitis has been reported. It is important to recognize this potential association because early preventative intervention is often successful in this disabling condition.
Bilateral simultaneous adhesive capsulitis of the shoulder is rare. The condition is associated with various conditions, including Dupytren's contracture, diabetes mellitus, thyroid disease, upper limb trauma, stroke, Parkinson's disease and adrenocorticotrophin deficiency [3,10]. A strong association with MMP inhibitor chemotherapy agents has also been reported. Hutchinson et al. found that 50% of patients on Marimastat (synthetic MMP inhibitor) for inoperable gastric carcinoma developed bilateral adhesive capsulitis, which improved once treatment was temporarily halted [4]. It was hypothesized that this correlation was the result of a decrease in MMP levels.
Matrix metalloproteinase are enzymes that degrade extracellular matrix and they are naturally inhibited by tissue inhibitors of metalloproteinases (TIMPs). Both work together to regulate remodelling of connective tissue under the influence of numerous growth factors and cytokines [11]. Previous studies have shown that there is an imbalance of this relationship in adhesive capsulitis, with greater levels of TIMPs than MMPs [12]. The resultant increased inhibition of MMP activity results in a failure of collagen remodelling and, ultimately, fibrosis of the shoulder capsule and potentially adhesive capsulitis [4].
The FOLFOX chemotherapy regime consists of folinic acid, 5-FU and oxaliplatin agents. Exposure to 5-FU, which is an antimetabolite, has also been shown to decrease MMP production in rabbit flexor tendon fibroblasts [13], as well as in conjunctival squamous cell carcinoma [14]. Oxaliplatin, which is a platinum compound, has also demonstrated inhibition of MMP production [15,16]. These laboratory studies highlight that FOLFOX chemotherapy regime agents may inhibit MMP production and potentially explain the bilateral adhesive capsulitis seen in this patient.
Although unproven, adhesive capsulitis could therefore be an unrecognized complication following the FOLFOX chemotherapy regime. The time lag to symptom onset may be explained by the subclinical shoulder pathology during this time and the prolonged effects of chemotherapy. In addition, the rare, bilateral and simultaneous nature of the condition strongly suggests an external, systemic cause in the absence of well known associations. Hence, we consider that this potential association requires further investigation with close monitoring of patients currently undergoing (or recently undergone) FOLFOX chemotherapy for shoulder pain and stiffness. Oncologists and orthopaedic surgeons should be aware of this possible correlation to enable prompt diagnosis with early radiological imaging. This can facilitate early stage management using physiotherapy, intra-articular steroid injection and hydrodilatation to halt disease progression. Following such intervention, adhesive capsulitis pathology should resolve spontaneously 2 years to 3 years after symptom onset [17].
Our case report suggests that adhesive capsulitis of the shoulder maybe a newly discovered adverse event of the FOLFOX chemotherapy regime. Further observations and future laboratory analysis will be necessary to confirm this, which will inevitably occur as the awareness of a possible association increases.
Footnotes
Acknowledgements
We wish to thank Professor Cunningham, Consultant Oncologist at the Royal Marsden Hospital, London, for his input into this case report.
None declared