
Abstract
We report two cases of shoulder resurfacing arthroplasty being used as a definitive treatment for acute locked posterior shoulder dislocation. Both patients presented after seizures secondary to brain neoplasms. Both patients were functionally stable postoperatively and remained pain-free, with no subsequent episodes of dislocation. Given the terminal diagnosis, prompt mobilization and discharge was of paramount importance. This case series documents our experience of treating this complex surgical problem and demonstrates the versatility of humeral head resurfacing in this unusual clinical situation.
Introduction
Locked posterior dislocation of the shoulder is uncommon and frequently difficult to treat [1]. It may result from a fall on an outstretched hand, direct impact to the shoulder or violent muscle contraction caused by an electric shock or seizure [2]. In patients with uncontrolled seizure activity, the recurrence of posterior dislocation is common and may result in persistent instability. Posterior shoulder dislocation can often lead to permanent glenohumeral joint incongruity. Reverse Hill–Sachs lesions complicate up to 80% of posterior dislocations. Glenohumeral stability is compromised when > 20% of joint surface is involved [3].
Cases of locked posterior shoulder dislocation associated with seizure activity pose a unique challenge, because the patients are unable to comply with postoperative restrictions during rehabilitation. Conventional approaches requiring restrictions on mobilization are likely to be unsuccessful.
We report on two cases where locked posterior shoulder dislocations were associated with recurrent seizures. In both cases, the precipitating factor for seizure activity was a terminal brain tumour. Early stabilization and return to pain-free activities of daily living was the key factor influencing the surgical treatment options in both cases. Both cases were successfully treated with a Copeland resurfacing prosthesis. Good postoperative function was obtained and further dislocation was obviated.
Case Report
Case 1
A 43-year-old male sustained a posterior dislocation of the right shoulder during a new onset grand-mal seizure. He had a background history of salivary gland carcinoma with temporal lobe metastases precipitating the seizure. Plain radiographs and computed tomography (CT) demonstrated a reverse Hill–Sachs lesion in addition to a locked posterior dislocation of the right shoulder. Open reduction was required. A reverse Hill–Sachs involving 50% of the humeral head was present that rendered the glenohumeral joint very unstable after reduction. The problem was addressed by resurfacing the humeral head with a Copeland implant (Fig. 1). Immediate glenohumeral stability was obtained. Postoperatively, the patient was discharged the next day and wore a simple sling for 2 weeks. He was allowed to perform activities of daily living but was instructed to avoid external rotation greater than 20° to protect the subscapularis repair. At 6 months postoperatively, the patient had a pain-free shoulder with > 80% range of motion in all planes except terminal internal rotation. He had returned to driving from 6 weeks postoperatively.
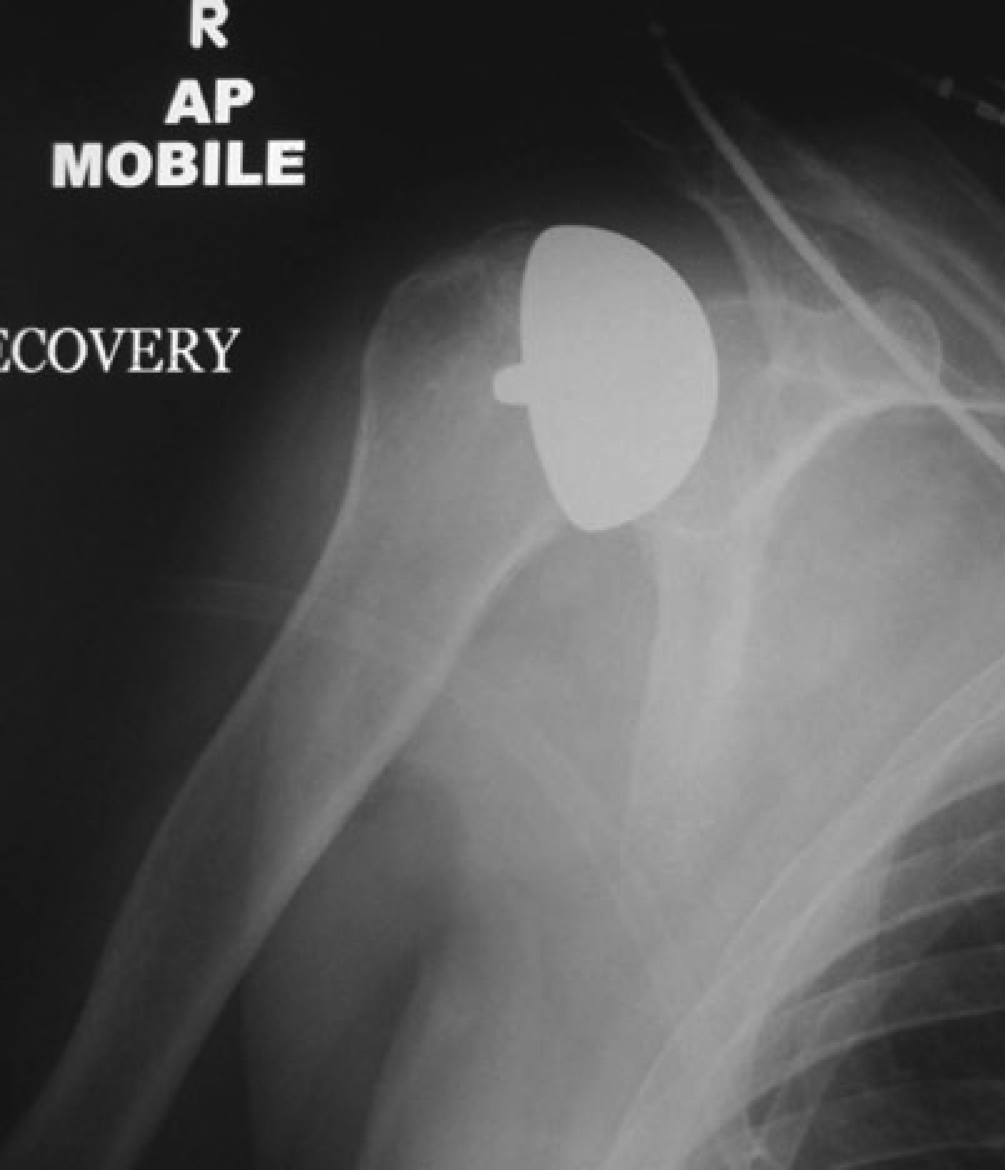
Postoperative anteroposterior view (Case 1).
Case 2
A 59-year-old right-hand dominant factory operative sustained a posterior dislocation of the right shoulder during a new onset grand-mal seizure induced by a space-occupying lesion of the right occipitoparietal lobe. The underlying diagnosis was glioblastoma multiforme. Investigation using CT revealed a locked posterior dislocation of the right shoulder with a large reverse Hill–Sachs lesion (Fig. 2). This lesion was found to comprise > 45% of the joint surface during open reduction. The joint was grossly unstable after reduction. The humeral head was resurfaced with a Copeland implant. Joint stability was restored after insertion of the implant. The patient made a satisfactory recovery with a painless stable joint. He was discharged the next day and resumed activities of daily living, including being able to drive from 6 weeks postoperatively.
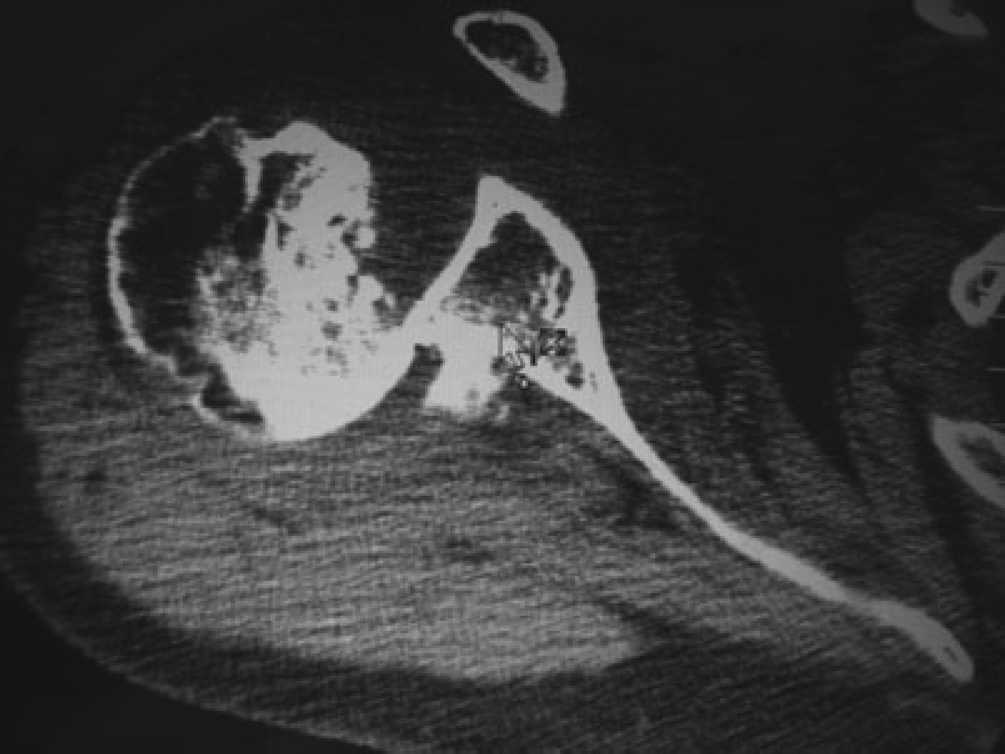
Axial computed tomography showing posterior dislocation with a reverse Hill–Sachs lesion (Case 1).
Discussion
Locked posterior shoulder dislocation is difficult to diagnose and treat [1]. The diagnosis is initially missed in up to 60% of cases on first examination [4]. Delays in the detection of the posteriorly dislocated humeral head significantly reduce the chances of success of closed reduction [5]. Epileptic seizures are a common cause of posterior shoulder dislocation, although anterior dislocation is equally as likely to occur [2]. The classical ‘lightbulb’ sign, where a symmetrically profiled humeral head seen on an anteroposterior view of the shoulder appears to articulate with the glenoid, is often a subtle radiological sign and may lead to a delayed diagnosis. Axillary lateral views and CT scanning of the affected joint represent essential imaging modalities for evaluating suspected cases of locked posterior dislocation [6].
The reverse Hill–Sachs lesion, defined as an anteromedial humeral head impression fracture of the affected humeral head [7], is a key factor influencing the choice of surgical intervention. It has been demonstrated that lesions comprising up to 20% of the humeral head are amenable to stabilization with soft tissue procedures involving the subscapularis and can sometimes be treated with closed reduction [3], [5]. For lesions > 50%, arthroplasty or an allograft has been shown to be successful [8]–[10]. Arthroscopic techniques have also been used to address posterior shoulder dislocation [11]. The outcome of these interventions is contingent on the patient being able to comply with restrictive postoperative rehabilitation programmes [5]. In these cases, we were able to treat the pathology with an implant that was readily available without needing to obtain additional equipment or material, as would have been the case with allografting or other types of shoulder prosthesis.
This case series represents an atypical presentation of acute locked posterior shoulder dislocation in that the most important outcome determinants for the respective patients were a swift return to functional activity with a stable shoulder joint not requiring intensive rehabilitation. The Copeland resurfacing procedure offered a one-stage stabilization option enabling the patient to mobilize in the immediate postoperative period. The quality of life for both cases was improved with instant pain relief and restoration of joint stability. Although acknowledging that this procedure is not applicable to all cases of this condition, we consider that it represents a useful adjunct where an immediate restoration of a stable pain-free shoulder is required.