
Abstract
Bone loss involving the articular surfaces of the shoulder joint is challenging to manage. We review the reconstructive options for the glenoid and humeral head using structural autografts.
Introduction
Bone loss is a challenging problem faced by orthopaedic surgeons. It may be the result of a primary loss that occurs at the time of trauma, secondary loss during surgery or tertiary loss subsequent to delayed infection. When bone loss involves the articular surface, the joint congruity could be affected, leading to instability and later degenerative changes. In the upper limb, there are unique circumstances of osteochondral bone loss that are amenable to reconstruction using autologous structural grafts. The suitable candidate will be a young patient with significant symptoms as a result of the articular injury. The patient must be highly motivated and willing to participate actively in the postoperative rehabilitation.
The use of autograft avoids the potential risks of disease transmission and the issue of limited availability associated with the use of allograft. An ideal autograft should render minimal or no donor site morbidity, afford long-lasting anatomical reconstruction, and provide mechanical stability, hence allowing early mobilization of the reconstructed joint. We review the available structural autograft options for reconstructing the glenoid and humeral head.
Biology of Structural Autografts
Structural autografts may be vascularized or nonvascularized. Nonvascularized grafts undergo revascularization and remodelling as new bone grows into the graft by creeping substitution [1], [2]. There may be temporary weakening of the subchondral bone as the necrotic bone is resorbed, which has been postulated as the cause of cartilage degeneration [1], [3]. By contrast, the vascularized graft maintains its blood supply and unites directly with the recipient bone, hence avoiding bone necrosis [2].
Animal studies have shown that systemic pre-treatment before harvesting [1] or direct local treatment [3] of the bone graft with bisphosphonates may reduce resorption of the grafted bone. The mechanical support afforded by the graft is thus maintained for a longer period, allowing in-growth and remodelling of new bone. This may help to reduce the risk of failure and collapse of load-bearing osteochondral graft [1]. However, bisphosphonate treatment before osteochondral bone grafting is yet to be accepted as routine surgical practice.
Reconstruction of the Anterior Glenoid
Traumatic shoulder instability, most commonly in the anterior direction, is often associated with bone loss involving the glenoid, the humerus or both [4]. Glenoid bony reconstruction is indicated when there is more than 25% of inferior glenoid defect in the anteroposterior dimension or after failed soft tissue stabilization [4]. Anterior glenoid bone grafting was first described by Eden [5] and subsequently by Hybbinette [6]. Initially, a tibial autograft was used and, later, an iliac crest graft was utilized [6]. The graft was placed into a periosteal pocket close to the glenoid rim and fixed by tightening the capsule in closing the capsular rent, including the subscapularis tendon [6]. Modern practice utilizes a tricortical iliac crest bone graft, which is secured with screws and contoured to replicate the anatomy of the native glenoid [7], [8]. Warner et al. reviewed 11 patients at a mean follow-up of 33 months [8]. The mean American Shoulder and Elbow Surgeons score improved from 65 to 94 and there was no recurrent instability. Rahme et al. reported the long-term results of Eden–Hybbinette procedure in 77 patients after a mean follow-up of 29 years [7]. Instability recurred in 20% of the patients but only eight required re-operations. Eighty-three percent were rated as good or excellent based on the Rowe scores. During the period of study, glenohumeral arthritis developed in almost half of them. However, there was no demonstrable association between the presence of arthritis and age at first dislocation, age at surgery or the duration of follow-up [7].
To avoid the morbidity associated with an iliac crest harvest, coracoid process may be used for a local transfer [9], [10]. Furthermore, it also functions as a vascularized graft. The Bristow procedure involves transplanting the terminal half inch of the coracoid process to the antero-inferior edge of the glenoid rim [9] (Fig. 1). The coracoid osteotomy is performed just distal to the insertion of pectoralis minor but proximal to the conjoined tendons. The cut end is then transferred to an abraded area at the neck of scapula through a slit in the subscapularis. However, the amount of bone grafted may not be sufficient in some cases. By contrast, the Latarjet procedure involves osteotomizing the coracoid from near its base and the graft is laid lengthwise to the glenoid [10] (Figs 2 and 3). The coracoid autograft should be laid flush to the glenoid because a more lateral position may be associated with the development of arthropathy, whereas a more medial position is associated with higher recurrences of instability [11] (Fig. 4). When a horizontal capsular shift is added to the coracoid transfer, it leads to a decreased rate of recurrence and improved subjective results [11].
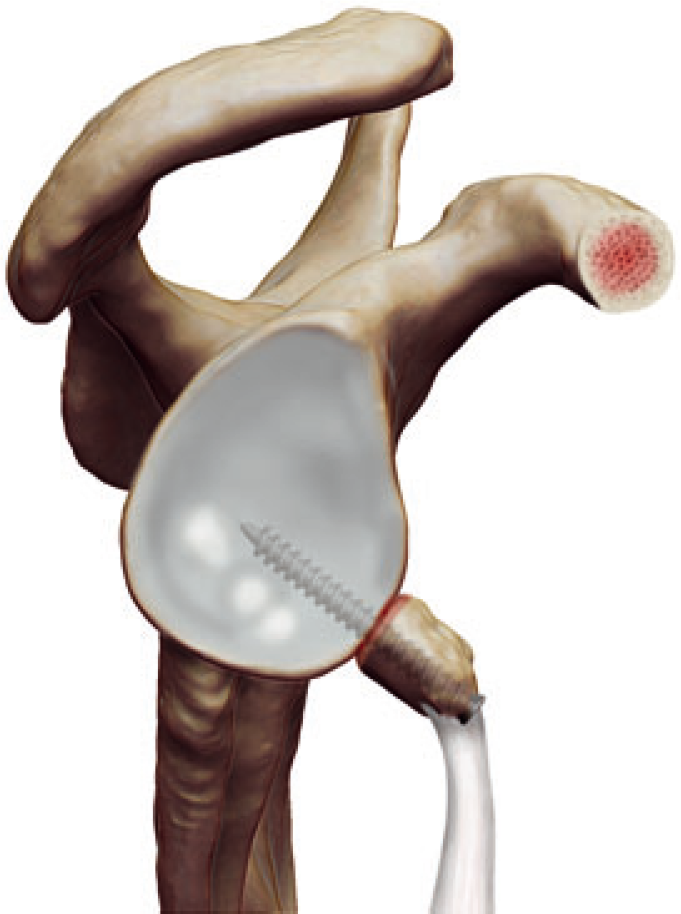
Showing the Bristow procedure with a vertical orientation of the graft.

In the Latarjet procedure, the graft is laid lengthwise to the glenoid.

Axial radiograph showing a Latarjet reconstruction.
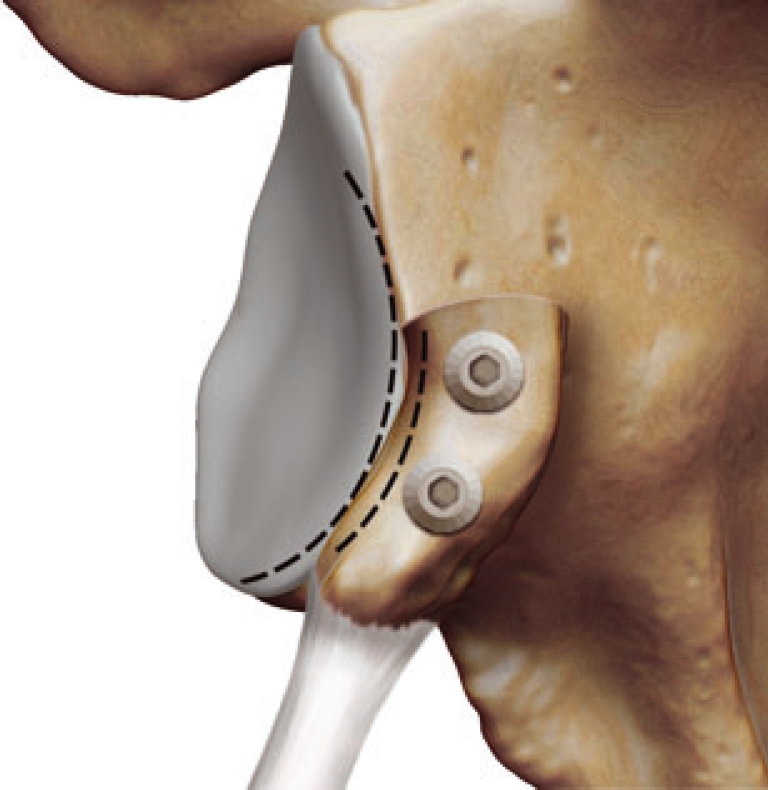
The key in glenoid reconstruction is to recreate a congruent arc with the graft lying flush to the glenoid articular surface.
Shah et al. detailed early complications after the Latarjet procedure in 48 shoulders [12]. A superficial infection developed in three shoulders (6%) and all resolved after irrigation and debridement and administration of antibiotics. Four shoulders (8%) developed recurrent glenohumeral instability (two occurred within 8 months, one at 19 months and one at 42 months postoperatively). Five (10%) were complicated by a neurological injury (two involved the musculocutaneous nerve, one involved the radial nerve and two involved the axillary nerve). The musculocutaneous and radial nerve injuries involved sensory neurapraxia that resolved fully within 2 months. Of note, the patients with axillary nerve palsy continued to have persistent sensory disturbances and one continued to have residual weakness. Although most of the early complications are likely to resolve, patients undergoing this procedure should be counselled appropriately regarding the potential risks and their sequelae [12].
Yamashita et al. reported the results of 126 patients at a mean follow-up of 41 months after undergoing a combined Bankart–Bristow procedure for recurrent shoulder instability [13]. Ninety percent of patients reported good to excellent outcomes. Only two patients had recurrent subluxations. The mean loss of external rotation was 13° compared to the contralateral shoulder. Hovelius et al. performed a long-term review of 118 patients treated with the Bristow procedure [14]. During a mean follow-up period of 15 years, instability recurred in 16 (14%) patients but only one of them required revision surgery. Notably, 98% of patients were satisfied. Moderate or severe glenohumeral arthritis was observed in 14% of shoulders, whereas milder changes were noted in 35% [15], which were comparable with the incidence reported by Rahme et al. [7].
Allain et al. retrospectively reviewed 56 patients (58 shoulders) at a mean of 14 years after undergoing the Latarjet procedure [16]. None of them had sustained a recurrent dislocation but seven patients described symptoms of residual instability. By the final review, 62% had developed glenohumeral arthritis and the mean loss of external rotation, compared to the contralateral side, was 21°. Despite that, 88% reported good or excellent results. Burkhart et al. reported on 102 patients who underwent a modified Latarjet procedure for shoulder instability associated with at least 25% loss of inferior glenoid [17]. Forty-seven patients were reviewed clinically and 55 by telephone interview. Over a mean follow-up period of 59 months, there was a 5% recurrence rate and the mean loss of external rotation was 5°. The mean Constant score was 94.
The open anterior glenoid reconstructions using the coracoid process have been shown to achieve satisfactory results in the treatment of recurrent instability. With the advancement of arthroscopic skills and instrumentation, arthroscopic techniques for the Bristow [18] and Latarjet [19] procedures have both been developed. Currently, they are performed only by a small number of surgeons. Nonetheless, with further refinement of the techniques, arthroscopic reconstruction of the glenoid may become the established practice for the experienced shoulder arthroscopists.
The primary aim of anterior glenoid reconstruction is to restore stability of the glenohumeral joint. However, it remains debatable whether surgery would influence the development of arthritis over the long term. Buscayret et al. retrospectively reviewed 570 patients with a mean follow-up of 6.5 years after undergoing a stabilization procedure (soft tissue or bony) [20]. Older age at initial presentation and at surgery, recurrence and longer follow-up were associated with a higher prevalence of arthritis. Notably, there was no significant difference in the rate of postoperative arthritis between patients who had a coracoid transfer and those who had an open soft tissue procedure [20]. Hovelius and Saeboe reported the incidence of arthropathy after a first-time anterior dislocation in 223 shoulders that had been followed up prospectively for 25 years [21]. Age at primary dislocation, recurrence, high-energy sports and alcohol abuse were identified as risk factors for the development of arthropathy. Although there was a background risk of arthropathy after dislocation, surgically-stabilized shoulders appeared to have less arthropathy than those that were not operated on with recurrent instability [21].
Reconstruction of the Posterior Glenoid
Traumatic posterior dislocations account for approximately < 3% of all shoulder dislocations [22]. Bone loss involving the posterior glenoid is correspondingly uncommon but is more demanding to manage. The threshold for posterior bony augmentation is less well defined compared to anterior bone loss. It may be indicated in the presence of persistent instability despite reconstructions of the soft tissue structures and associated humeral head defect. Similar to anterior glenoid reconstruction, distant grafts from the tibia [23] or the iliac crest [24], [25] were used initially. Mowery et al. reported their results of posterior bone block procedure in five patients aged between 17 years and 44 years, who were followed up for 2.5 years to 8 years [26]. The graft was harvested from the posterior superior iliac spine and was placed such that it extended 1.5 cm laterally over the humeral head. One patient subsequently developed an anterior dislocation of the shoulder, although the other four were reported to achieve excellent results. By contrast, Barbier et al. first positioned the monocortical iliac crest graft so as to project by 5 mm lateral to the glenoid edge. The graft was then trimmed down using a burr, so that it was flush with the remaining glenoid surface [27]. They retrospectively reviewed eight patients who had undergone the reconstruction after a mean follow-up of 34 months. There was no recurrent instability. Subsequent X-ray or computed tomography showed a 100% union rate without any evidence of arthritis. However, three patients lost a mean of 20° of external rotation compared to the contralateral shoulder and one patient had deltoid detachment requiring repair. Technical issues as a result of an in appropriate length or position of the screws, as well as the incorrect positioning of the graft, have been reported [27]–[29].
A local vascularized graft using the acromion with a deltoid flap pedicle was described by Kouvalchouk et al. [30]. The muscle flap plays a supplementary role in preventing posterior instability. Five patients with a mean age of 32.5 years were treated with this technique and no recurrence of instability or resorption of the graft occurred during the mean follow-up of 1.5 years [30]. Sirveaux et al. reported their experience in treating a heterogeneous group of patients with posterior instability [29]. Nine patients were treated with an iliac bone block, whereas the other nine were treated with an acromial pedicled graft. After a mean follow-up of 13.5 years in the former subgroup and 3.5 years in the latter group, no recurrent dislocation or subluxation was noted but six patients still described apprehension.
The senior author has harvested the posterolateral corner of the acromion (as a nonvascularized graft) to reconstruct the posterior glenoid in three patients with recurrent posterior instability (Figs 5–7). All of them have been stable postoperatively, with one returning to professional rugby.
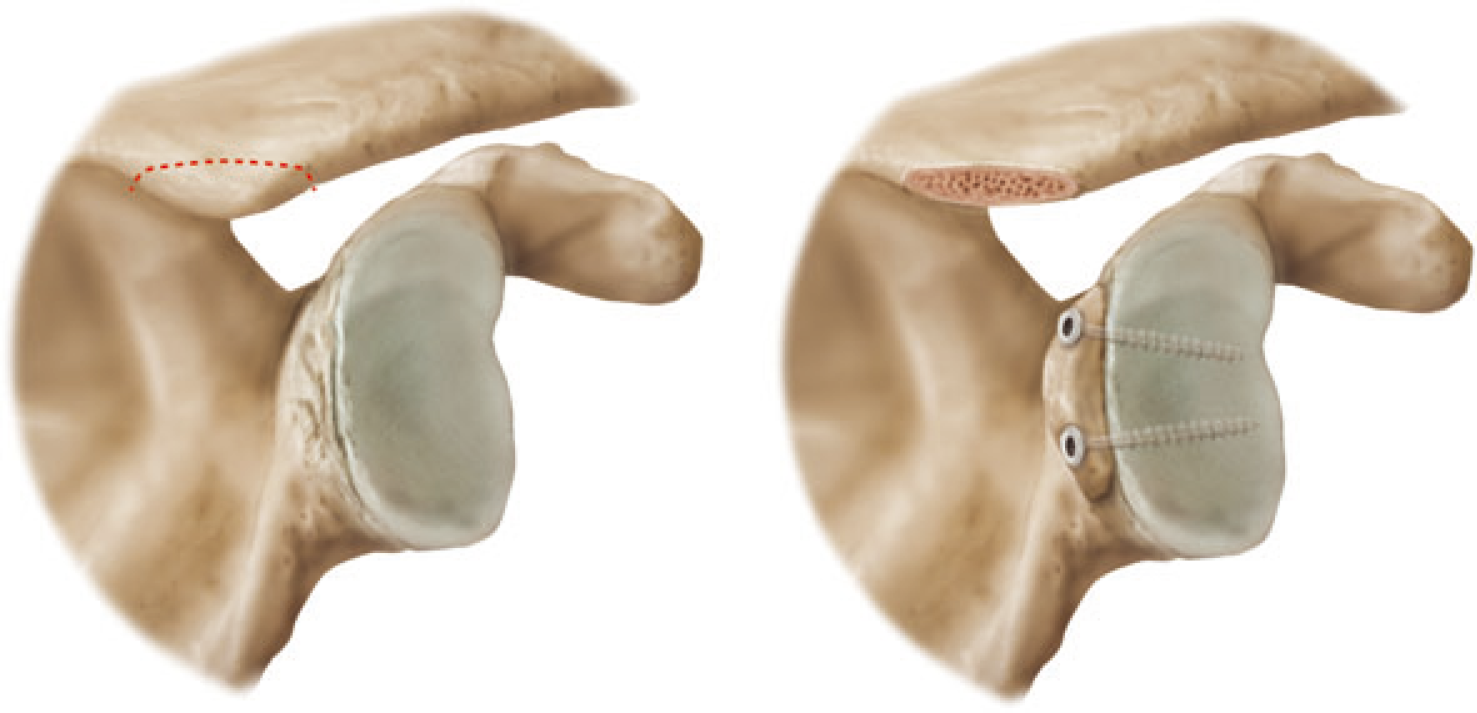
Showing posterior glenoid bone grafting using the posterolateral corner of the acromion.
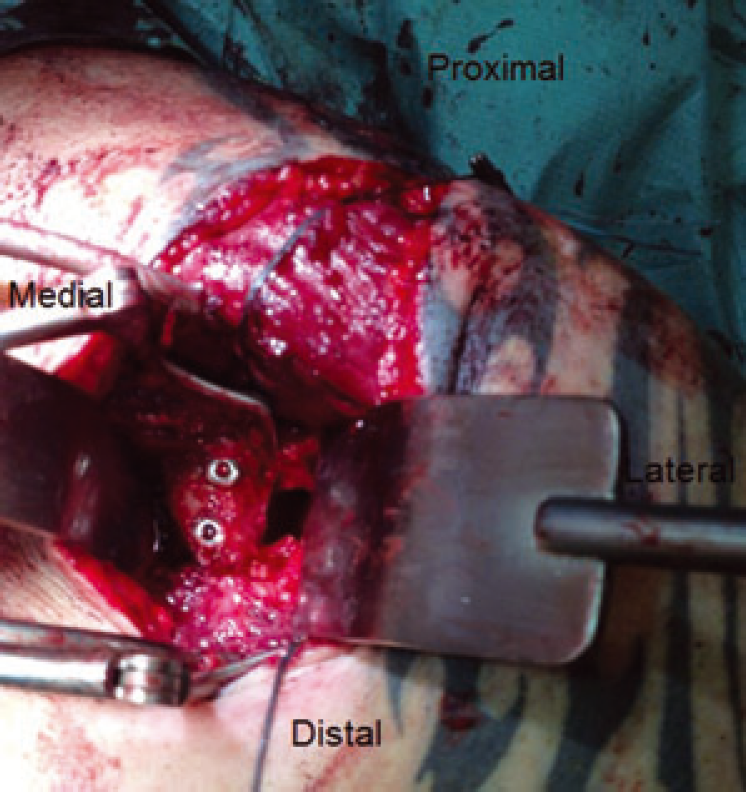
Intra-operative image showing the posterior view of a right shoulder with the acromial autograft in situ.
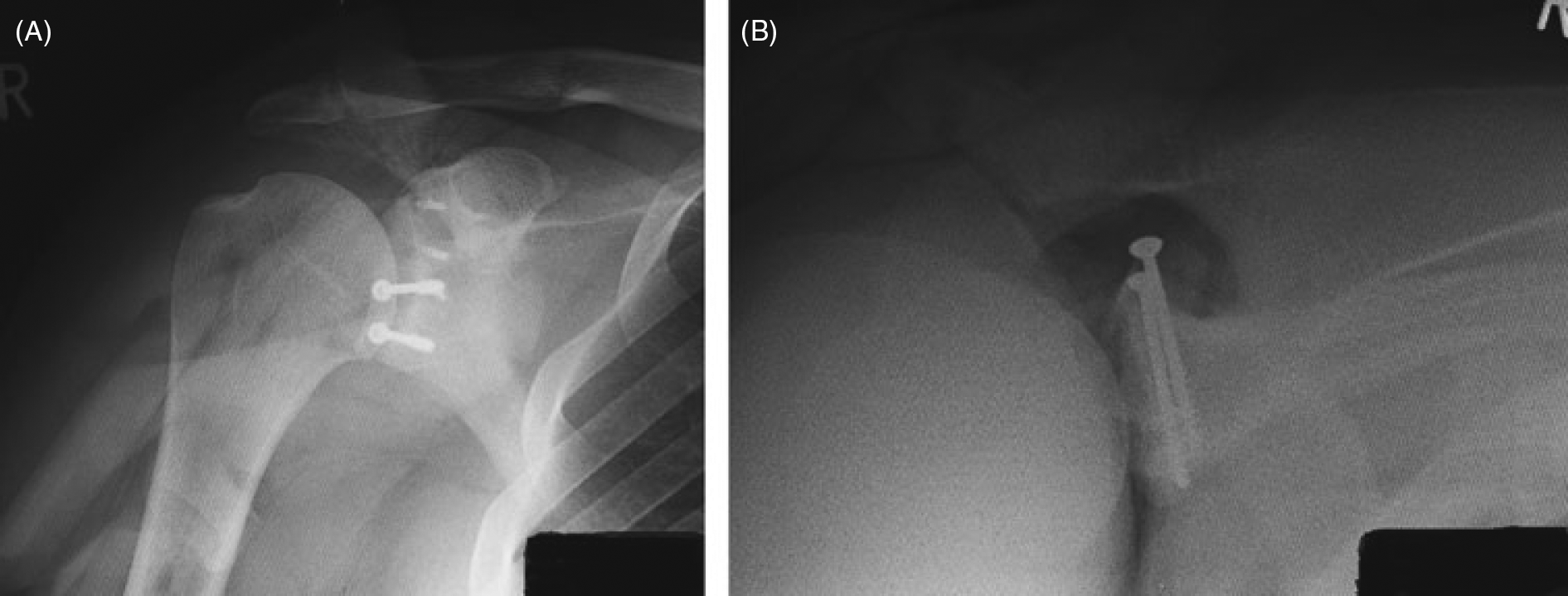
Postoperative (A) anteroposterior and (B) axial radiographs of a posterior glenoid autograft reconstruction.
Reconstruction of the Humeral Head
Osteochondritis dissecans of the humeral head is an exceedingly rare condition and only several cases have been reported in the literature [31]. Park et al. employed the technique of mosaicplasty to reconstruct a posterosuperior osteochondral defect of the humeral head in a 13-year-old boy [32]. At a second-look arthroscopy 5 months after reconstruction, the graft appeared to have healed and biopsy then showed a normal pattern of hyaline cartilage. At 2 years and 7 months, the patient was reported to be asymptomatic.
Posterior dislocation of the shoulder may be associated with an anteromedial impaction fracture of the humeral head (reverse Hill–Sachs lesion). McLaughlin described a technique of stabilization by transposing the subscapularis tendon into the defect [33]. This was modified by Neer where the lesser tuberosity with the attached subscapularis tendon was transferred instead [34]. Finsklestein et al. reported satisfactory results employing this technique in seven shoulders that were unstable in internal rotation and had an impaction fracture occupying 25% to 40% of the articular surface [35].
Shenoy and Kamineni reported a case of reverse Hill–Sachs defect successfully reconstructed using a lateral clavicular autograft [36]. This was in a 78-year-old man who developed recurrent posterior dislocation subsequent to a fall. He had an engaging reverse Hill–Sachs lesion and incidental arthritis of the ipsilateral acromioclavicular joint. The distal 1 cm of the clavicle was harvested without impairing the stability of the acromioclavicular joint and the graft was fixed with a screw. No further dislocation was reported at the final 18-month review.
Reconstruction using autologous grafts requires creativity and the tissue bank concept should always be remembered when dealing with complex cases. A unique circumstance arose in a patient with bilateral posterior fracture-dislocations of his shoulders after a grand mal seizure [37]. The left proximal humerus was not reconstructable; hence, a hemiarthroplasty was performed. There was, however, a large anteromedial impression defect of the right humeral head that was then reconstructed with an osteochondral fragment removed from the contralateral shoulder. At his 2-year review, he reported no pain or limitation in his right shoulder. Radiographs and magnetic resonance imaging showed incorporation of the graft without evidence of collapse.
Conclusions
The success of articular reconstructions using autologous bone grafting relies on the immediate mechanical stability and the long-term biological fate of the graft [38]. Coracoid transfer to the anterior glenoid has proven to be a reliable reconstruction. By contrast, posterior glenoid bony augmentation is rarely performed and few surgeons would have extensive experience on the procedure. Indications for reconstruction of the humeral head using structural autograft are limited. When the defect is large, reconstruction using allograft [39] or prosthetic replacement may be required [40], [41]. Evidence-based application of autograft reconstruction of the shoulder joint is difficult to devise as a result of the complexity of the conditions necessitating such a consideration. Decision-making is influenced by the experience and skills of the surgeon and treatment is individualized to the specific patient.