
Abstract
Background
Surgical treatment of displaced proximal humerus fractures remains controversial. There is little guidance on which patients are likely to do well with humeral nailing. Therefore we present our study evaluating the Stryker T2 proximal humeral nail (T2-PHN).
Methods
Sixty-one consecutive patients with acute unilateral displaced proximal humerus fractures were treated with the T2-PHN and followed up for a mean of 19 months. There were 46 females and 15 males with mean age 68 (range 36–97). By Neer's classification there were 25 two-part, 28 three-part and 8 four-part fractures.
Results
Union occurred at a mean of 3 months. Fifty-five patients had Constant-Murley scores with a mean score of 64.9. Mean Constant-Murley was 59.9 for over 70s, 69.7 in under 70s, 68.0 in 2-part fractures, 67.5 in 3-part fractures, 36.6 in 4-part fractures, 50.6 in post-operative varus, 73.5 in post-operative neutral, 72.7 in post-operative valgus, 55.5 in medial metaphyseal comminution and 69.5 without comminution. Fifty-four patients had Oxford Shoulder scores with a mean score of 21.7.
Conclusions
The T2-PHN has a learning curve. Important points include adequate recessing of the nail tip and suturing of tuberosities. The best results can be expected in under 70s, 2 and 3-part fractures, patients without medial metaphyseal comminution and patients with neutral post-operative neck-shaft alignment.
INTRODUCTION
Fractures of the proximal humerus are extremely common and account for approximately 5% of all fractures [1]. They comprise the third most common fracture in patients over 65 years of age [2]. Epidemiological studies have predicted that proximal humeral fractures will increase the hospital workload significantly in the future [3]. A recent study from Finland estimates that the number of humeral fractures will triple during the next three decades [4]. The majority of undisplaced or minimally displaced proximal humerus fractures can be managed non-operatively with good functional results. However, displaced and comminuted fractures are associated with pain, deformity and functional disability [5, 6].
There are multiple surgical options available, including nails, plates, Kirschner wires, tension bands and hemiarthroplasty. A 2010 Cochrane review [7] concludes that there is insufficient evidence to inform the management of proximal humerus fractures. Similarly, a recent meta-analysis [5] reports that no one type of fixation has been proven to be most effective. The choice of implant continues to be controversial and there is growing interest in the use of locking proximal nails. Biomechanical studies have reported that nails are superior to Kirschner wires [8], superior to tension band wires [9] and also superior to plates with higher stiffness values in bending and torsional load [10 –12]. Hemiarthroplasty, often used to treat three- or four-part fractures in the elderly, has been associated with high rates of shoulder stiffness, tuberosity resorption, glenohumeral instability and marked limitation of function [13 –17]. Plate fixation is also associated with high complication rates, as shown by a recent meta-analysis reporting complications of 49% subsequent to plating [18]. The potential advantages of nailing include smaller incisions with less soft tissue disruption, preservation of the periosteal blood supply to the humeral head and a shorter operation time [19]. There are few studies available in the literature on proximal humeral nailing and the results are variable. There is little evidence regarding which groups of patients would be expected to do well with nails and which patients do badly. Therefore, the present study aimed, first, to present our experience with the Stryker (Stryker UK Ltd, Newbury, UK) T2-proximal humeral nail (T2-PHN) in 61 displaced fractures of the proximal humerus and, second, to identify which groups of patients are likely to do well and which groups have less favourable outcomes.
MATERIALS AND METHODS
The present study comprised 61 consecutive patients with displaced proximal humerus fractures treated with the T2-PHN and followed up for a mean of 19 months (range 6 months to 72 months). Inclusion criteria were acute, unilateral, displaced proximal humerus fractures in patients aged over 18 years. Exclusion criteria were minimally or undisplaced fractures, displaced head-splitting multi-fragmentary fractures needing primary hemiarthroplasty, patients aged under 18 years, open fractures, pathological fractures, and unfit patients whose medical co-morbidities precluded surgical treatment. A fracture was considered displaced if the fracture fragment had displaced more than 1 cm or if there was angulation greater than 45° [20]. All operations were carried out at the same hospital between 2004 and 2009. The operating surgeons were one upper limb consultant, three consultants with other specialist interests, four registrars and two associate specialists.
The T2-PHN is a cannulated 150-mm titanium alloy nail that provides angular-stable fixation. It has a standard diameter of 10 mm and allows placement of up to four multi-directional 5-mm proximal locking screws into the humeral head. The locking holes are threaded and have nylon bushings to maximize screw purchase in the humerus. This has the aim of preventing screw back-out. It is also possible to place a maximum of two distal locking screws in either static or dynamic mode. Screw placement is performed using a radiolucent targeting device.
Our operative technique was to place the patient in the beach-chair position and use a superior deltoid-splitting approach. The deltoid was split from the acromion to a point approximately 4 cm distally. The supraspinatus tendon was then split in line with its muscle fibre orientation. Our more recent technique has been to mobilize the fractured tuberosities with number 5 ethibond (Ethicon, Johnson & Johnson Medical Ltd, Livingston, UK) sutures in their tendons. The tuberosities were reduced onto the head and sutured to each other. Every attempt was made to restore the head/shaft angle and the medial reduction. The reduction can be helped with a bone lever onto the head. We found that the nail is best passed after the proximal humerus has been reconstructed. Using an image intensifier, the entry point of the T2-PHN was made medial to the greater tuberosity and posterior to the bicipital groove. We used hand-reaming and the nail was inserted after reduction of the fracture. Our practice is to use three proximal locking screws and one dynamic distal locking screw. The proximal screws were not used for tuberosity reduction but purely to achieve a secure fixation in the humeral head. The rotator cuff and deltoid were repaired during wound closure.
After operation, all patients were placed into a polysling in internal rotation. Pendulum exercises were commenced on day 1 as pain allowed. At 2 weeks, a physiotherapy appointment was made and passive exercises were commenced. Active exercises were started at 4 weeks. Both passive and active exercises were performed under close supervision from the physiotherapists. There was no restriction to the range of movement but forced stretches were only allowed from the sixth post-operative week onward. Patients were followed up in the outpatient clinic post-operation at week 2, week 6, week 12, month 6 and then every 6 months.
The demographic data collected included patient age, sex, Neer's classification and whether the fracture was of the left or right humerus. Neer's classification was based on two independent X-ray reviewers and was confirmed intra-operatively. Outcome was measured using Constant—Murley scores (CM) and Oxford Shoulder scores (OS), which were collected prospectively in the outpatient clinic. X-rays were critically assessed for the presence or absence of medial metaphyseal comminution, initial neck/shaft angle (NSA), immediate post-operative NSA, union NSA, the presence or absence of union, and complications. Medial metaphyseal comminution was defined as one or more butterfly fragments adjacent to the medial cortex on the anteroposterior X-ray with the shoulder in neutral rotation. NSA was measured according to the method described by Zhu et al. [19]. The angle was measured on anteroposterior X-ray with the shoulder in neutral rotation. A line was drawn from the superior to inferior border of the articular surface and then a second line was drawn through the centre of the humeral head at right angles to the first line. The angle between this second line and another line bisecting the humeral shaft was measured as the NSA. Mean (SD) anatomical NSA is known to be 134.7° (3.8°) [21, 22]. Therefore, in the present study, we defined varus alignment as NSA < 130°, neutral alignment as NSA 130° to 140°, and valgus alignment as NSA > 140°. Successful union was taken to be healing of at least three out of four cortices seen on the standard AP and lateral axillary X-ray views. Surgical complications were also noted with a retrospective analysis of both patient case notes and a Bluespier (Bluespier UK, Droitwich, UK) computer database of operation records.
Statistical analysis was performed on all results. The results are reported as the mean (SD). Differences between groups of data were analyzed using a two-tailed Student's t-test for continuous variables and the Mann—Whitney U-test for non-normal distributions. Categorical data were analyzed using chi-squared or Fisher's exact test when expected numbers were small. p < 0.05 was considered statistically significant.
RESULTS
Demographics and overall results
Our series comprised 61 consecutive patients. There were 46 females and 15 males with a mean age of 68 years (range 36 years to 97 years). In total, there were 33 patients aged over 70 years and 28 patients aged 70 years or under. Twenty-nine patients had a fracture of the right proximal humerus and 32 had fractured the left side. The mean follow-up period was 19 months. The length of follow-up ranged from 6 months to 72 months. All patients, except one who died, were followed up to radiological union, which occurred at a mean of 3 months (range 6 weeks to 6 months). By Neer's classification, there were 25 two-part, 28 three-part and eight four-part fractures. X-rays for analysis of medial metaphyseal comminution, initial NSA and union NSA were available for 60 patients. Nineteen patients had medial metaphyseal comminution and 41 patients did not. Initial varus was seen in 24 patients, valgus in 28 patients and neutral in eight patients. Union occurred in varus malalignment for 18 patients, valgus malalignment for 21 patients and neutral for 21 patients. There were 55 patients with CM scores. CM scores were not available for one patient who died from an unrelated cause and for five patients with dementia. The mean CM was 64.9. Overall, 74.5% of patients had excellent or satisfactory CM scores. Excellent scores (> 75) were seen in 21 patients and satisfactory scores (50 to 75) in 20 patients. Fifty-four patients had OS scores. OS scores were unavailable in the same patients who did not have CM scores. In addition, one patient attended clinic and had a CM score but no OS score was taken. Unfortunately, this patient died from an unrelated cause before an OS score could be taken. The mean OS score was 21.7. In total 42 (77.8%) of these scores were graded as satisfactory (12 to 20 points). Table 1 demonstrates the CM and OS outcome scores seen in different patient groups. An X-ray from a patient with an excellent CM score and an X-ray from a patient with a poor CM score are shown in Fig. 1.
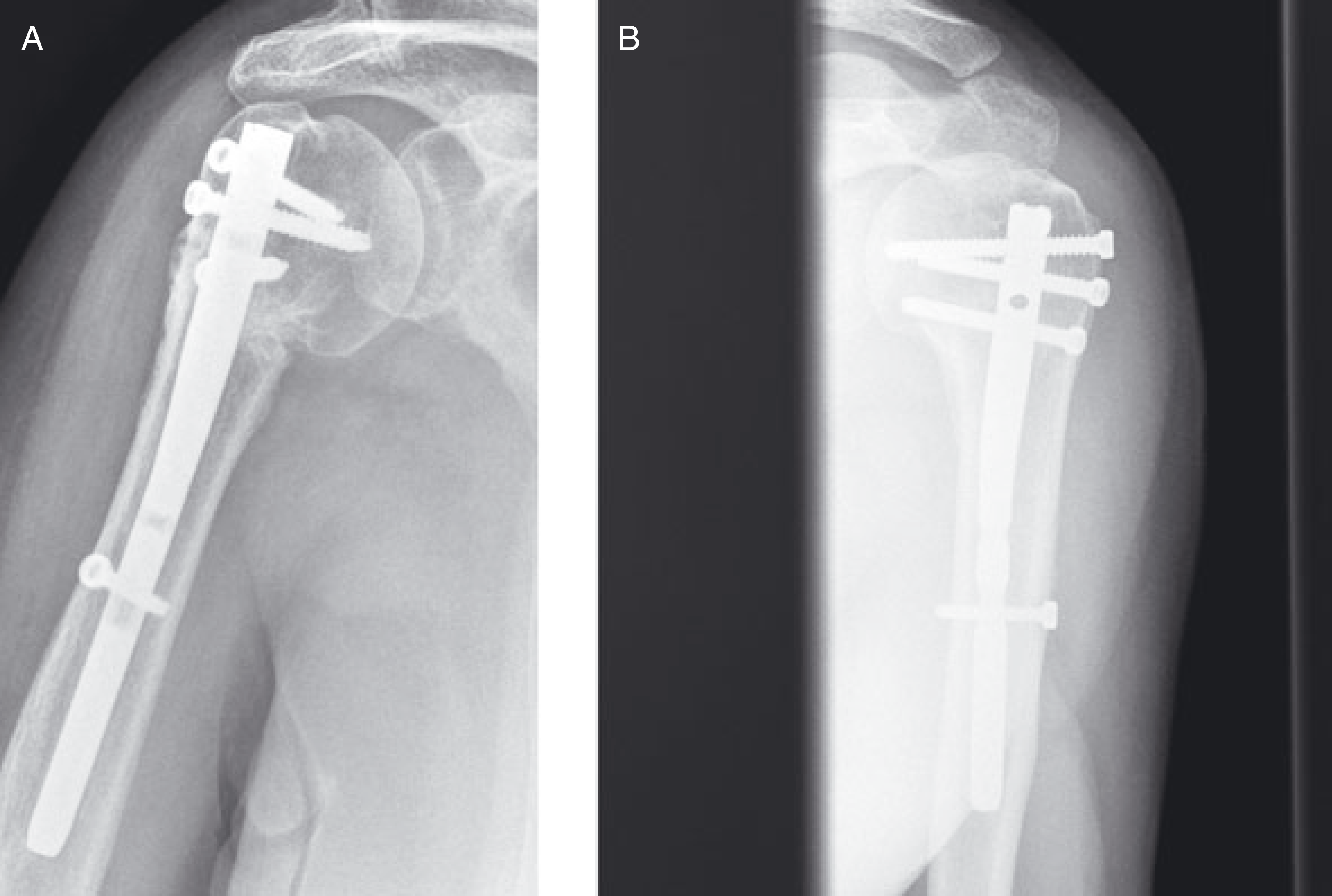
(A) X-ray of a patient with a poor Constant—Murley score. This patient was aged over 70 years, had medial metaphyseal comminution and was fixed in varus malalignment. (B) X-ray of a patient with an excellent Constant—Murley score. This patient was aged under 70 years and did not have medial metaphyseal comminution.
Outcomes seen following T2-PHN in different groups of patients
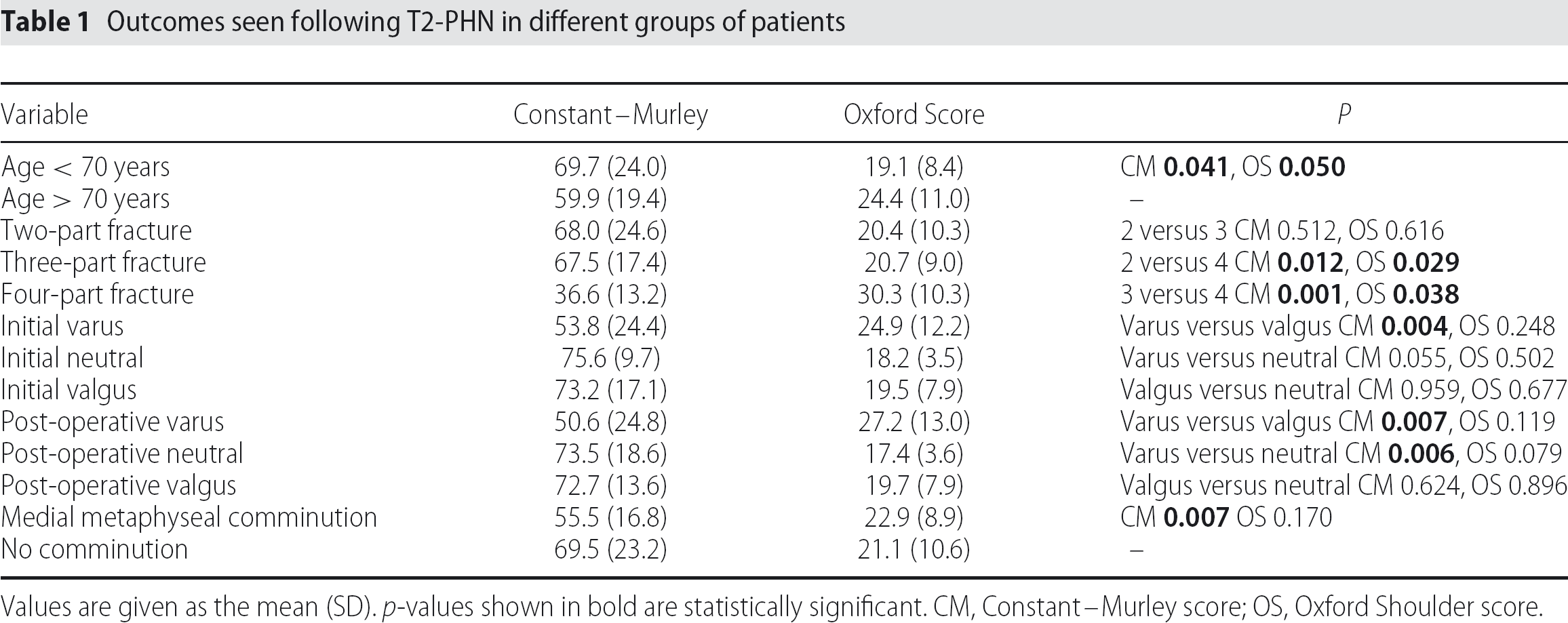
Values are given as the mean (SD). p-values shown in bold are statistically significant. CM, Constant—Murley score; OS, Oxford Shoulder score.
Outcome by age
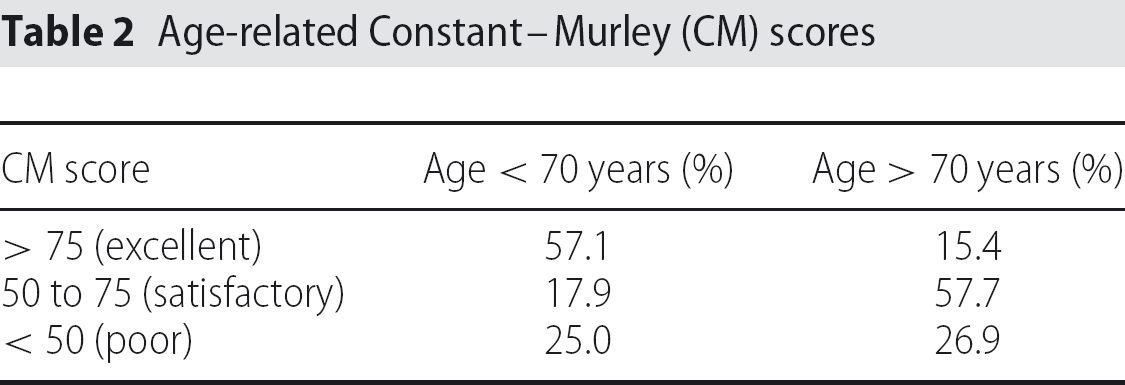
Age-related analysis of the CM scores demonstrated that patients under 70 years were more likely to have good outcomes. The mean (SD) CM for patients of 70 years or under was 69.7 (24.0) compared to 59.9 (19.4) for those aged over 70 years. This difference is significant (p = 0.041). Table 2 shows the percentage of patients achieving excellent, satisfactory and poor CM scores in the under and over 70-year-olds. Again, it is clear that better results were seen in the under 70-year-olds. There were excellent results in 57.1% of under 70-year-olds compared with only 15.4% of over 70-year-olds. Using the chi-squared test, the differences seen in Table 2 are statistically significant (p = 0.002; χ2 = 12). The CM pain score component, where 15 points signifies no pain, showed a mean (SD) of 11.1 (3.7) in under 70-year-olds compared to 10.0 (3.9) for over 70-year-olds (p = 0.366). Similar to the CM scores, the OS scores were also improved in the under 70-year-olds. The mean (SD) OS score for patients aged 70 years or under was 19.1 (8.4) compared to 24.4 (11.0) for the over 70-year-olds. Again, this difference is statistically significant (p = 0.050).
Age-related Constant—Murley (CM) scores
Outcome by Neer fracture type
The mean (SD) CM for two-part fractures was 68.0 (24.6) compared to 67.5 (17.4) for three-part fractures and 36.6 (13.2) for four-part fractures. The difference between two- and three-part fractures was not statistically significant (p = 0.512). However, the difference between two- and four-part was significant (p = 0.012), as was the difference between three- and four-part (p = 0.001). The CM pain score component was a mean (SD) of 11.0 (3.9) for two-part fractures, 11.0 (3.5) for three-part fractures and 6.0 (2.2) for four-part fractures. The difference between two and four-part (p = 0.014) and between three and four-part fractures (p = 0.005) was significant. The mean (SD) OS for two-part fractures was 20.4 (10.3), compared to 20.7 (9.0) for three-part fractures, and 30.3 (10.3) for four-part fractures. Again, the difference between two- and three-part fractures was not significant (p = 0.616), although the difference between two-part compared to four-part (p = 0.029) and between three-part compared to four-part (p = 0.038) was significant.
Outcome by medial metaphyseal comminution
In patients with comminution, the mean (SD) CM was 55.5 (16.8) and the mean (SD) OS was 22.9 (8.9). Without metaphyseal comminution, the mean (SD) CM was 69.5 (23.2) and the mean (SD) OS 21.1 (10.6). The CM difference reached statistical significance (p = 0.007) but the OS difference did not (p = 0.170). The mean (SD) CM pain component was 8.3 (2.4) with comminution compared to 11.1 (4.1) without comminution (p = 0.010).
Outcome by initial NSA
Patients with an initial varus NSA had a mean (SD) CM score of 53.8 (24.4) and a mean (SD) OS score of 24.9 (12.2). Initial valgus patients had a mean (SD) CM of 73.2 (17.1) and OS of 19.5 (7.9). Outcome scores were worst for the initial varus patients, although only the CM score in the varus compared to valgus group achieved statistical significance (p = 0.004). No difference was seen between valgus and neutral CM scores (p = 0.959) or OS scores (p = 0.677).
Outcome by post-operative and union NSA
The overall mean (SD) immediate post-operative NSA was 137.8° (18.1°). Mean (SD)NSA at time of union was 136.1° (18.8°). With the paired t-test, this 1.7° reduction is significant (p < 0.001). Initial varus NSA fractures healed at a mean (SD) of 122.4° (13.0°), initial neutral at 134.1° (9.2°) and initial valgus at 148.8° (16.2).
Demographics of the varus, valgus and neutral union groups of patients were comparable by age (p = 0.698), Neer fracture type (p = 0.419), medial metaphyseal comminution (p = 0.557) and sex (p = 0.588). At union, varus NSA was associated with mean (SD) CM of 50.7 (24.8) and a mean (SD) OS of 27.2 (13.0). Valgus union had a mean (SD) CM of 72.7 (13.6) and a mean (SD) OS of 19.7 (7.9). Neutral union had a mean (SD) CM of 73.5 (18.6) and a mean (SD) OS of 17.4 (3.6). The difference between varus and neutral CM was significant (p = 0.006) but the OS difference did not quite reach statistical significance (p = 0.079). When comparing the neutral and valgus groups, neither the CM difference (p = 0.624), nor the OS difference (p = 0.896) were significant.
Complications
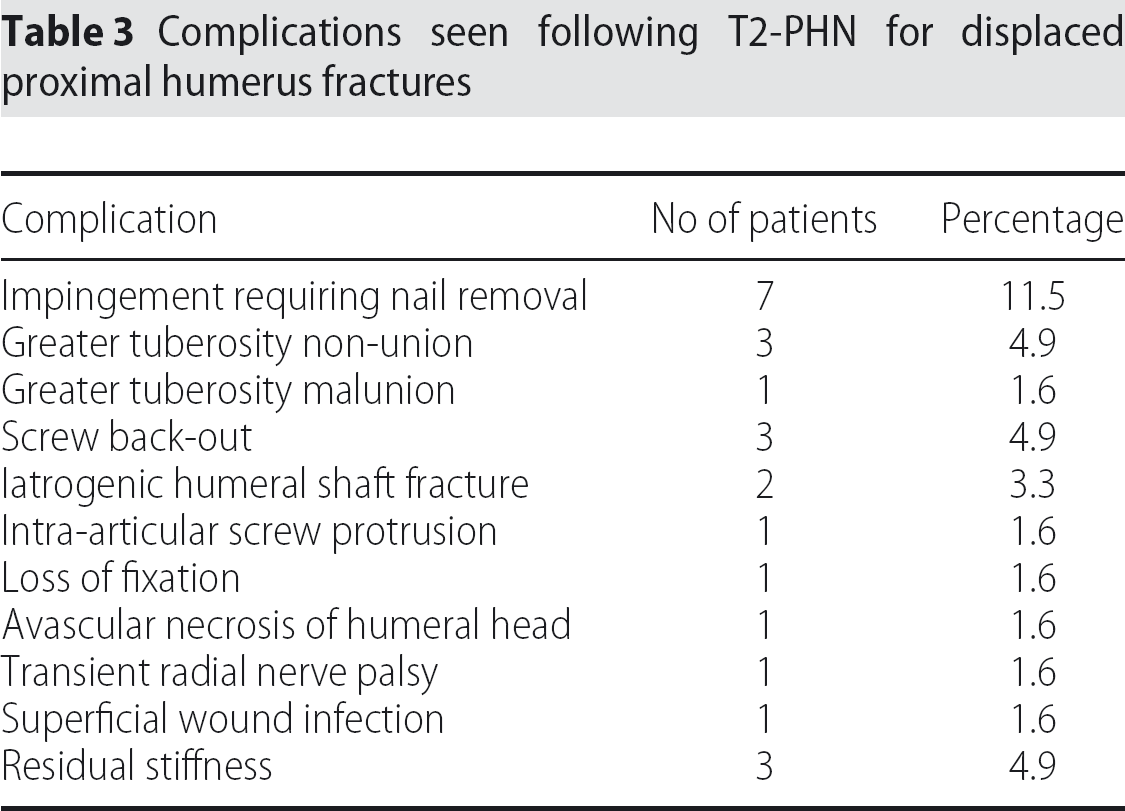
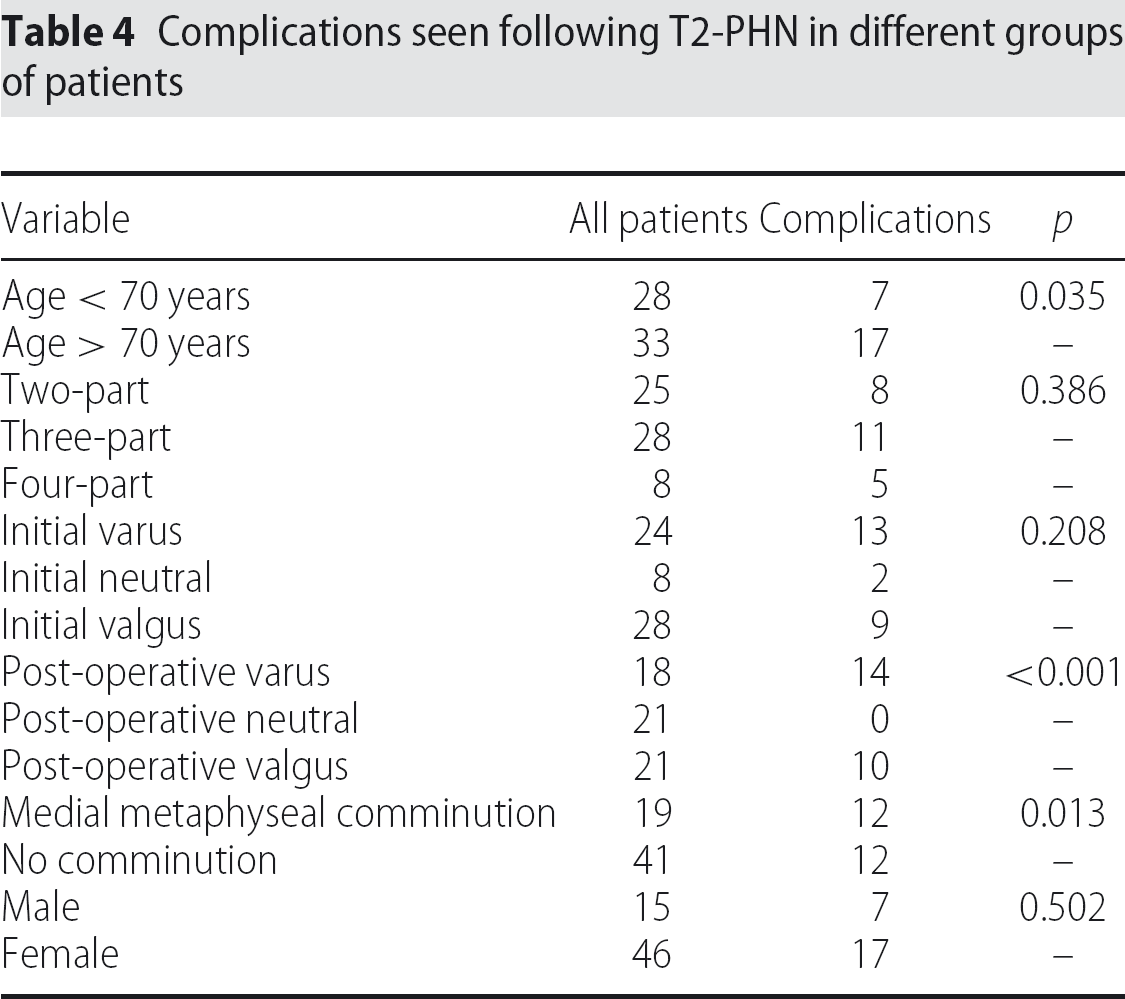
Our complications are displayed in Table 3. The overall complication rate was 39% (24 of 61 patients) with a re-operation rate of 21.3% (13 of 61 patients). Our complication rates by age, Neer fracture type, medial metaphyseal comminution, initial NSA, union NSA and sex are shown in Table 4. Statistically significant increases in complications were seen for patients aged over 70 years (p = 0.035), medial metaphyseal comminution (p = 0.013) and post-operative varus malalignment (p < 0.001).
Complications seen following T2-PHN for displaced proximal humerus fractures
Complications seen following T2-PHN in different groups of patients
The most common surgical complication, with seven (11.5%) of our early patients affected, was impingement requiring nail removal after fracture union. Impingement was the result of a prominence of the nail tip. An example of this can be seen in the X-ray shown in Fig. 2. All patients improved after removal of the nail. There were also three greater tuberosity non-unions. Two of these had not been sutured at the time of operation. The third patient was sutured using vicryl (Ethicon, Johnson & Johnson Medical Ltd) rather than ethibond. One additional patient had malunion of the tuberosities that was asymptomatic and did not require any treatment.
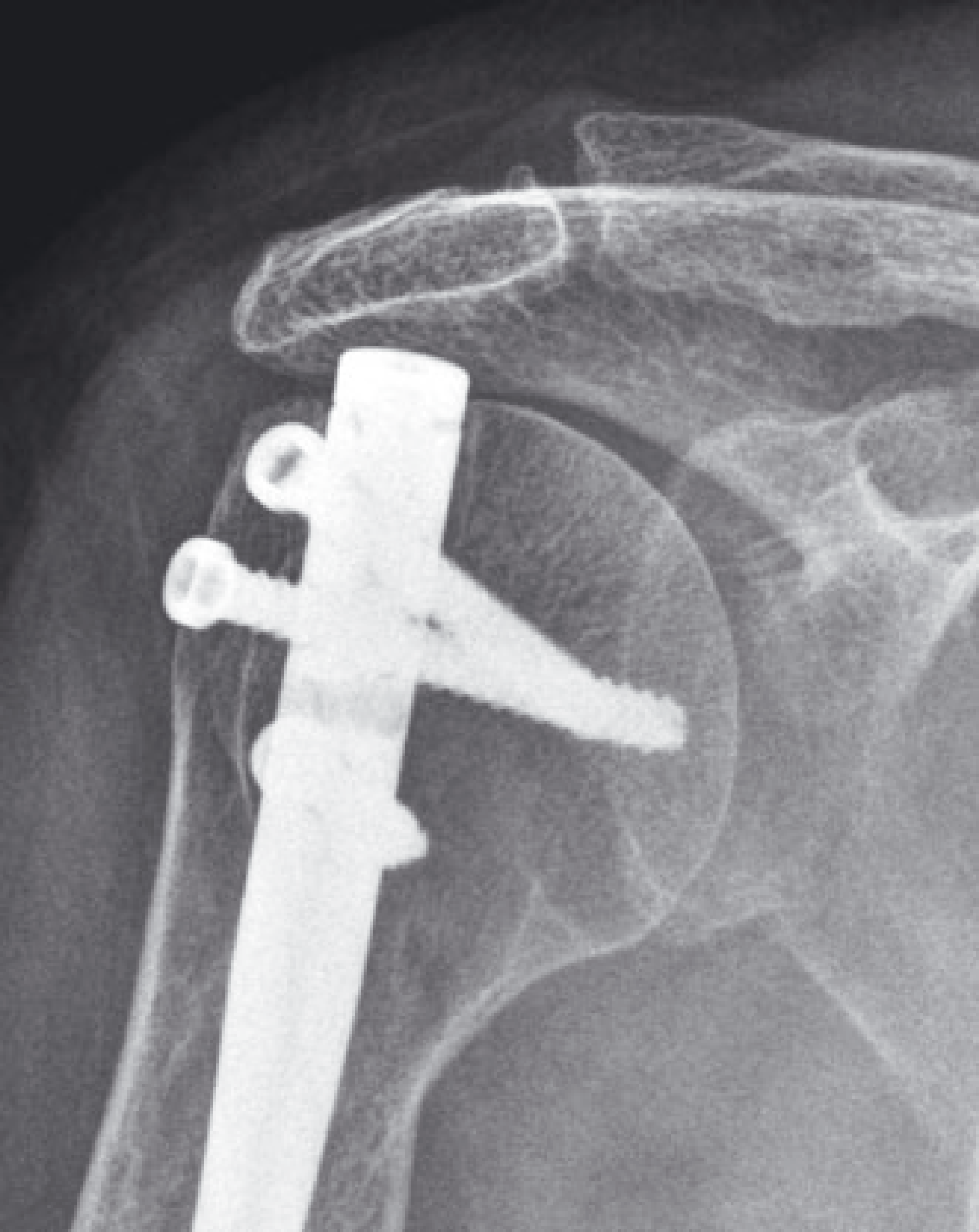
X-ray of a patient with impingement as a result of inadequate recessing of the proximal nail end.
There were two iatrogenic intra-operative humeral shaft fractures. Both of these patients were elderly females, one aged 77 years and the other aged 82 years, with three-part fractures and medial metaphyseal comminution. One of the fractures occurred when trying to reduce the proximal fracture and the other fracture occurred when introducing the nail. Both fractures were treated with the use of a longer nail to stabilize both the proximal and shaft fractures. Both went on to achieve union and good function with CM scores above the series average.
There was one loss of fixation in another elderly female with very osteoporotic bone. The loss of fixation was revised to a Philos plate (Synthes Ltd, Welwyn Garden City, UK) and subsequently had an uneventful recovery. Three screw back-outs were also seen. One of these was the result of surgical error with the insertion of a 4-mm screw rather than a 5-mm screw. The screws were removed via stab incisions and all the patients went on to achieve a good functional result. Additionally, we had one intra-articular screw protrusion that was treated with screw removal. Other complications were avascular necrosis of the humeral head in a 71-year-old female with diabetes, transient radial nerve palsy in a 77-year-old female, and a superficial wound infection in a 58-year-old male. The infection resolved with a 1-week course of oral flucloxacillin. In addition, three patients suffered from residual stiffness for which no cause could be identified. One of these patients had some improvement following manipulation under anaesthesia. The other two patients achieved a functional range of movement with physiotherapy.
DISCUSSION
There have been a number of proximal humeral nailing studies with relatively small patient numbers and highly variable outcomes [19, 23 –33]. There are three studies reporting outcomes with the T2-PHN. Popescu et al. reported outcome scores for 18 patients with mean CM of 65.7 and mean OS of 21.7 [25]. Sosef et al. reported outcome scores for 16 patients with mean CM of 62 [32]. These results are very similar to our overall results of a mean CM of 64.9 and a mean OS of 21.7. A third study by Hatzidakis et al. reported the best outcome for the T2-PHN with a mean CM of 73 in 29 patients with two-part fractures [33].
Our data showed significantly improved CM and OS scores in the under 70-year-olds. Kazakos et al. also found significantly better results in their younger patients [30]. In addition, the studies with the lowest mean age tend to have the best outcomes [19, 29] whereas the studies with the highest mean age tend to have worse outcomes [23, 32].
There are only a limited number of studies evaluating the use of nailing in four-part fractures because many studies [23,26,29 –31] excluded patients with four-part fractures. Popescu et al. included only a single patient with a four-part fracture [25]. It is logical to expect a worse outcome for the more severe fractures. In the present study, both two- and three-part fractures had significantly better CM scores and OS scores than four-part fractures. Zhu et al. state that their indication for proximal humeral nailing is limited to two-part fractures and that this may be the reason for their results being the best reported in the literature with a mean CM of 88 at 1 year follow-up [19]. Sosef et al. reported poor CM scores in three four-part fractures with a mean CM of only 23 compared to 62 for 10 three-part fractures and 72 for seven two-part fractures [32].
Four-part fractures are difficult to treat. Our results were relatively disappointing in these patients. This could be partly because reduction of the displaced tuberosities is technically challenging. We have shown increased complications in patients fixed in varus and valgus malalignment. In the four-part fractures, a lack of anatomical alignment in the fixation could then predispose to failure. Good results have been reported with angle-stable plates for unstable fractures [34, 35] and so perhaps plate fixation might be more appropriate for these patients. Hemiarthroplasty has also been advocated for highly comminuted fractures [36]. Gronhagen et al. reported reasonable outcomes at a mean follow-up of 4.4 years [17]. Therefore, hemiarthroplasty might also be a better option than nailing for these fractures. However, both plating and hemiarthroplasty have been associated with high rates of complications [13 –18], which were also seen in the present study. Consequently, perhaps we should also be re-considering non-operative management in this difficult group of fractures.
To our knowledge, our study is the first to assess outcome and complication rate for nailing in patients with medial metaphyseal comminution. Krappinger et al. reported increased failure in patients with comminution treated with the Synthes Philos plate and humerusblock (Synthes, Oberdorf, Switzerland) [37]. However, their increase did not reach statistical significance (p = 0.13). Other studies have also found medial column support to be important in maintainance of reduction following plate fixation [38]. Our study helps confirm the poorer prognosis associated with medial metaphyseal comminution.
To our knowledge, there are no studies critically assessing the effect of pre-operative and post-operative alignment in nailing. However, Sosef et al. reported that four of 34 patients had dislodgement of the T2-PHN from the humeral head and that all of these patients had varus malalignment [32]. In plating, it has been reported that varus malreduction increases the lever arm of the rotator cuff resulting in higher stresses and increased likelihood of failure [38]. A plating study by Solberg et al. also found worse outcomes and more complications in patients with initial varus head angulation [39]. Therefore, it is logical that nailing patients with initial and post-operative varus malalignment would also suffer similar consequences, thereby accounting for our poorer outcome scores and higher complication rates in these patients. The fact that there were no complications in our 21 patients with a neutral post-operative alignment compared to complications in 14 of the 18 varus malalignment patients (p < 0.001) demonstrates the importance of achieving good post-operative alignment.
Our complications have all been previously reported with intramedullary nailing and are displayed in Table 3. It is important to note that, despite our re-operation rate, our other complication rates are better than most published series. Our re-operation rate of 21.3% compares to values of 17.2% to 38.9% [23,25,32]. Impingement has been reported in 1.9% to 38.9% of patients [23,26,27,32], greater tuberosity non-union or malunion in 3.7% to 55.6% [23 –27], screw back-out in 3.4% to 7.4% [25,27,30], avascular necrosis (AVN) in 2.8% to 3.7% [25,26,30], intra-articular screw protrusion in 7.4% to 17.6% [26, 32], iatrogenic fracture in 17.2% [25], stiffness in 3.7% [30], infection in 0.9% to 8.8% [26,27,32] and transient radial nerve palsy in 4.2% [24].
Our complication rate of 39% does appear to be rather high. However, numerous complications have been reported with other proximal humerus fixation techniques. Zhu et al. found significantly fewer complications in patients treated with nailing rather than plating [19]. Recent meta-analysis [18] of plate fixation reported an overall rate of complications following plating of 49%, including 14% reoperation, 10% AVN, 8% screw perforation of the humeral head into the joint, 6% subacromial impingement and 4% infection. Percutaneous pins have been associated with loss of fixation, pin track infection, pin migration and excessive X-ray exposure [40, 41]. Tension band wiring can result in breakage of the cerclage wire, and also in very high rates of both AVN and impingement requiring re-operation [42, 43]. Hemiarthroplasty has been associated with stiffness, tuberosity resorption, instability and marked loss of function [13 –17].
We consider that the T2-PHN has a steep learning curve, which was demonstrated by fewer implant-related complications in our later cohort of patients. Our most common complication was impingement. It is important to recess the tip of the nail below the cortical surface of the humeral head to prevent impingement. As part of the learning curve, for our later patients, we were careful to achieve adequate recessing of the proximal end of the nail, thereby reducing the rate of impingement. Furthermore, rather than using all four proximal locking screws, we now avoid the most proximal locking screw placement to reduce the risk of impingement. Our second most common complication was tuberosity non-union and malunion. Tuberosity displacement is common as a result of the pull of the rotator cuff muscles. Our tuberosity non-unions included two patients where the tuberosities were not sutured and one malunion when the suturing technique was not as robust. More recently, we have used ethibond to suture the tuberosities and, subsequent to this modification of technique, our complication rate has reduced. Other studies have also reported the importance of suturing the tuberosities. For example Krivohlávek et al. report that their number of complications decreased after introducing osteosuturing of the tuberosities [28]. We also favour dynamic, rather than static, distal locking. Placing the distal locking screw in dynamic mode allows for a small amount of fracture collapse as the metaphyseal bone heals. Other learning points include considering bone grafting in cases of significantly reduced bone stock and careful attention to achieve accurate measurement of screw lengths. Inaccurate measurement of proximal screw length can result in overly long screws causing penetration of the joint.
Iatrogenic fracture of the humeral shaft was a serious complication and calls into question whether these patients should have been treated with nailing at all. Both patients were elderly females with osteoporotic bone, medial metaphyseal comminution and three-part fractures. One had a varus angulation of the head fragment and the other a valgus angulation. Following treatment with a longer nail, both patients went on to achieve union and CM scores above the series average, and so perhaps it was appropriate to treat them with nailing. On the other hand, the risk of shaft fracture is higher with the thinner cortices of osteoporotic patients and could have been anticipated. As a result of these fractures, we modified our operative technique and now routinely hand-ream when initial passage of the nail by hand is tight.
Our AVN rate was low compared to other studies. It is possible that the smaller incision for nailing allows less damage to the periosteum and the intramedullary approach also helps avoid damaging the important anastomosis around the humeral neck, which is vital for supplying the humeral head [44]. This might result in a lower rate of AVN following nailing. However, our AVN rate may be underestimated because it was only through radiographs and also magnetic resonance imaging of symptomatic patients that this complication was identified.
The strengths of the present study include the relatively high patient numbers covering a variety of fracture types and the relatively high rate of prospective outcome scoring. Some authors have excluded patients with poor bone stock from their studies [27]. We consider that our inclusion of osteoporotic fractures, our mean age of 68 years, and our inclusion of both three- and four-part fractures, as well as two-part fractures, is more representative of typical patient populations seen in orthopaedic departments throughout the UK. Our results were obtained from a wide variety of surgeons and represent a technique that is easily transferable and reproducible. However, the present study has some clear limitations. A longer period of follow-up would improve data accuracy and might have improved our outcome scores because Zhu et al. reported improved CM scores at 3-year follow-up compared to 1-year follow-up [19]. In addition, we did not normalize the CM scores for age or sex. Another limitation of the present study is that the patients aged under 70 years and over 70 years were not matched for medical co-morbidities. Further research and prospective randomized studies would help validate the advantages of nailing.
We believe that the T2-PHN with suturing of the tuberosities provides a stable fixation with minimal soft tissue disruption and also allows preservation of the periosteal blood supply. This facilitates early motion, rehabilitation and return to function. The best results can be expected in patients under 70 years old, two- and three-part fractures, patients without medial metaphyseal comminution and patients with a post-operative neutral neck-shaft alignment. For these patients, the T2-PHN is a good management choice. However, relatively poor results can be expected for over 70-year-olds, four-part fractures, medial metaphyseal comminution, initial varus NSA and post-operative varus malalignment. For patients in this latter group, especially those fulfilling several categories, it is probably better to consider plate fixation, hemiarthroplasty or conservative treatment. The complication rate is comparable to other surgical fixation methods and can also be significantly reduced as part of the learning curve as the surgeon becomes more experienced and uses modified techniques, such as adequate recessing of the nail with suturing of the tuberosities, and achieves a neutral post-operative alignment.