
Abstract
Observing that patients with longer appointment delays tend to have higher no‐show rates, many providers place a limit on how far into the future that an appointment can be scheduled. This article studies how the choice of appointment scheduling window affects a provider's operational efficiency. We use a single server queue to model the registered appointments in a provider's work schedule, and the capacity of the queue serves as a proxy of the size of the appointment window. The provider chooses a common appointment window for all patients to maximize her long‐run average net reward, which depends on the rewards collected from patients served and the “penalty” paid for those who cannot be scheduled. Using a stylized M/M/1/K queueing model, we provide an analytical characterization for the optimal appointment queue capacity K, and study how it should be adjusted in response to changes in other model parameters. In particular, we find that simply increasing appointment window could be counterproductive when patients become more likely to show up. Patient sensitivity to incremental delays, rather than the magnitudes of no‐show probabilities, plays a more important role in determining the optimal appointment window. Via extensive numerical experiments, we confirm that our analytical results obtained under the M/M/1/K model continue to hold in more realistic settings. Our numerical study also reveals substantial efficiency gains resulted from adopting an optimal appointment scheduling window when the provider has no other operational levers available to deal with patient no‐shows. However, when the provider can adjust panel size and overbooking level, limiting the appointment window serves more as a substitute strategy, rather than a complement.
Keywords
Introduction
Appointment scheduling systems are widely used by healthcare providers to regulate their service capacity and patient demand. Providing patients with pre‐scheduled appointments reduces the variability in demand, and allows providers to better plan their daily operations. However, not every patient will show up for their scheduled services, creating the commonly known patient “no‐show” problem. Many health service providers report high no‐show rates which can range from 23% to 34% (Dreiher et al. 2008, Geraghty et al. 2007). No‐shows leave appointment slots wasted, and can result in significant financial loss (Atun et al. 2005, Moore et al. 2001). No‐shows also break continuity of care, and may lead to poor patient health outcomes (Nguyen et al. 2011, Schectman et al. 2008).
To mitigate the impact of no‐shows, healthcare providers can try directly improving patient attendance via sending reminders, providing transportation assistance or charging no‐show fees, but these interventions cannot completely eliminate no‐shows (Guy et al. 2012, Macharia et al. 1992). Some clinics still faced 20% or higher patient no‐show rates even after implementing appointment reminder systems (Geraghty et al. 2007, Hashim et al. 2001).
Facing high patient no‐show rates, providers can also consider adjusting their operations. One commonly adopted strategy is to overbook, that is, to schedule multiple patients in one appointment slot to hedge against the risk that some of them do not show up. The overbooking strategy has been studied extensively in the Operations Management (OM) literature; see, for example, LaGanga and Lawrence (2007), Muthuraman and Lawley (2008) and Zeng et al. (2010). The second operational lever often used by practitioners is to control the panel size, that is, the number of patients a practitioner considers as her “own” patients (Green and Savin 2008, Liu and Ziya 2014). This operational lever is motivated by observing that patients tend to have higher no‐show probabilities when their appointment delays are longer (Dreiher et al. 2008, Gallucci et al. 2005, Liu et al. 2010). The appointment delay is the scheduling interval, that is, the time between the day when a patient requests for an appointment and the actual appointment date given to her. By limiting the panel size, a provider can ensure that her patients will not wait too long for appointments and thus will be more likely to show up.
Though panel size selection and overbooking are widely used operational levers to cope with patient no‐shows, they may not be implementable in a large number of practices. For instance, 1128 community health centers in the U.S. are Federally Qualified Health Centers (FQHCs) as of 2011, and they receive government grants under the Public Health Service Act (Shin et al. 2013, U.S. Department of Health and Human Services 2014). In return for these grants, FQHCs have to serve all patients regardless of their ability to pay (Rural Assistance Center 2013). Consequently, providers in these centers cannot “dismiss” patients from or “reject” new patients to join their panels like their counterparts in private practices. In addition, providers in community health centers are often salaried, meaning that their incomes do not depend on the volume of patients they see and there is little financial incentive for them to work overtime. Overbooking, which often causes overtime work, is therefore unwelcome from these providers’ perspectives and can be difficult, if not impossible, to implement.
Without the options of overbooking or controlling panel size, one important and practical operational lever left to deal with appointment delay‐dependent patient no‐shows is to limit the appointment scheduling window. That is, patients are not allowed to make appointments beyond a certain day from the day when they make appointments. When there are no appointments slots available within the appointment window, providers usually have two ways to handle additional patient requests if any. One option is to simply advise patients to seek care elsewhere, for example, urgent care centers nearby. This option avoids overtime for providers. The other option is to accommodate these patients via working beyond the regular appointment hours. Although this option cannot circumvent overtime, it is still considered more acceptable by physicians than directly asking them to overbook. The reasons are mostly psychological. First, shortening the appointment scheduling window can be naturally phrased as a means to reduce delays and improve access to care, which are aligned well with healthcare providers’ professional pursuit. Second, overtime that may result from shortening the appointment window is not directly“built” into the system, and thus is less “repelling.”
In our discussion with health care professionals, we learned that controlling the appointment window is a commonly‐used operational lever in community health centers. Some centers have the same rule for all patients, while others may set different rules depending on patients’ no‐show behaviors. For example, one community health center in New York City faces 30–40% patient no‐show rates; it prohibits “frequent no‐show offenders” (defined as patients missing appointments more than five times in the past year) from making appointments one day ahead, but it is committed to serving these patients on an as‐needed basis (D. Rosenthal 2011, Columbia University, pers. comm.). Similarly, Wingra Family Medical Center, a large urban residency teaching clinic of the University of Wisconsin Family Medicine Residence Program, only permits patients who had demonstrated high appointment adherence in the past to schedule appointments in advance (DuMontier et al. 2013). However, there seems to be no consensus on when and how to use such an operational lever, and practices largely rely on trial‐and‐error approaches, often resulting in inefficiency and suboptimal management. It is the operational challenge faced by these practices that motivates our research.
Limiting the appointment scheduling window reduces appointment delays and thus no‐shows, leading to more efficient use of appointment slots. However, an overly restrictive scheduling window may leave too many patients unable to schedule their appointments. These patients may either seek care elsewhere or arrive at the clinic requiring service during overtime, resulting in some form of penalty to the provider either as loss of revenues, loss of goodwill from patients or unplanned overtime work for staff. Intuition seems to suggest that using a shorter appointment window for patients with higher no‐show rates would increase efficiency, but is this intuition correct? More generally, how does the choice of appointment scheduling window affect a provider's operational efficiency? Furthermore, how much efficiency gain can be achieved by adopting an optimal appointment window, when practices may (or may not) have the options to select panel size and overbooking level? This study seeks to answer these important questions unaddressed in the previous OM literature.
In this study, we develop stylized models as a simplified version of reality, which allow us to draw high‐level managerial insights. This serves as a first step to tackle the challenges faced by those providers in using the appointment scheduling window as an operational lever to deal with patient no‐shows. Using a single server queue model motivated by the work of Green and Savin (2008) and Liu and Ziya (2014), we are able to fully characterize the optimal appointment window and show how this optimal appointment window should be adjusted in response to changes in other model parameters. These results inform the conditions under which a longer appointment window may benefit practices more (or less). In addition, we carry out extensive numerical studies, which are based on carefully chosen model parameters, to strengthen our analytical findings. In particular, we investigate the efficiency gain of adopting an optimal scheduling window when a practice has (or does not have) the options of selecting panel size or overbooking levels. Finally, we extend our analytical model to consider a patient population with heterogeneous no‐show behaviors.
Our work is particularly related to appointment scheduling literature that develops operational strategies to deal with patient no‐shows. Depending on the planning horizon, this literature can be grouped into the work on intra‐day scheduling and the work on inter‐day scheduling; see Cayirli and Veral (2003) and Gupta and Denton (2008) for an in‐depth review.
Intra‐day scheduling concerns the best timing and sequence of appointments within a given day in order to optimize the trade‐off between patient in‐clinic waiting and provider utilization (taking patient no‐shows into account); see, for example, Hassin and Mendel (2008) and Robinson and Chen (2010). Inter‐day scheduling literature considers patient scheduling in a multi‐day planning horizon. The decision maker determines how to allocate appointment requests arising on the current day into future days; see, for example, Patrick et al. (2008) and Liu et al. (2010). Our work departs from the previous literature in that we consider a fundamentally different decision problem and focus on a more strategic level of decision making. We determine the size of the appointment window, that is, we consider how long in advance an appointment should be allowed to be scheduled, when patients exhibit delay‐dependent no‐shows.
The two articles most relevant to ours are Green and Savin (2008) and Liu and Ziya (2014). Similar to ours, both articles use a single server queue to model an appointment system where patient no‐show probabilities increase with appointment delays. However, there are a number of crucial differences distinguishing our work and theirs. The objective of Green and Savin (2008) is to identify a panel size sustainable for a practice to use Open Access, but our motivation is to find a proper appointment window that maximizes the efficiency. Accordingly, the decision variable in Green and Savin (2008) is the patient demand rate, while ours is the capacity of the appointment queue. In terms of the analysis, Green and Savin (2008) develop approximate methods to evaluate system performance; we focus on deriving structural results and obtain insights on what affect the optimal decisions and the system performance. The models in Liu and Ziya (2014) have an objective that shares a similar flavor as ours. However, they seek to jointly determine the optimal panel size and overbooking level which maximize the system efficiency. They do not impose a limit on the appointment window. In contrast, we study completely different operational strategies to deal with no‐shows by controlling the appointment window. In addition, Liu and Ziya (2014) only consider a homogeneous patient population, whereas we also study a model in which patients are heterogeneous in their no‐show behavior. These distinctions lead to different models and analyses, and bestow new managerial insights.
The rest of the article is organized as follows. Section 2 describes our model and the analytical results. Section 3 presents our numerical study. Section 4 discusses the model extension with heterogeneous patients. Section 5 provides the concluding remarks. The proofs of all the analytical results can be found in Appendix S1.
Model
We consider a single provider service system where the provider can control the appointment scheduling window. Our objective is to investigate how the size of the scheduling window affects system performance. Following the earlier work in Green and Savin (2008) and Liu and Ziya (2014), we use a single server queue as a stylized model to represent the appointment schedule of a provider. In the rest of the article, we use the words patient(s) and customer(s) interchangeably.
Suppose that the provider has an established panel of patients. Appointment requests from any patient in this panel arise according to a Poisson process, independent from those of others. Thus, the overall demand to the provider also follows a Poisson process. We assume that the overall demand rate is λ > 0. We further assume that patients have strong preferences on speedy access to care, and thus they will be (offered and) scheduled to the earliest appointment slot available. Patients may have other preferences for appointments (e.g., time of day), but our model is likely to be a reasonable approximation for reality if most patients strongly desire shorter appointment delays. Although academic literature on patient preferences for appointment scheduling is relatively scant, one study by Murray and Tantau (2000) suggests that only 25% of patients who are offered same‐day appointments opt to see a physician at a later time, supporting our assumption.
We keep a track of the appointment backlog of the provider, and refer to it as the “queue.” This queue is in fact a virtual waitlist of scheduled patients yet to be seen by the provider. We assume that patients will not cancel their appointments, and thus the new appointment requests always join the queue from the very end. This assumption usually works well for community health centers, which motivate our research. As Medicaid does not allow patients to be billed for missed appointments, these practices do not charge patients for failing to cancel scheduled appointments early enough. As a result, patients often“forget” about making cancellations.
To better interpret how our model approximates reality, imagine for now that each appointment slot is deterministic with length 1/μ day. The actual service time may have some variability, but it suffices to assume that the provider can serve each patient within one appointment slot. Or equivalently, we can imagine that the provider has exactly μ appointment slots in a day, and she will not overbook.
Consider the following sequence of events in an appointment scheduling system. During the day, patients make requests for appointments. Because the length of each appointment slot is deterministic, the provider knows exactly when the next available appointment is, and she will schedule the incoming patient to that slot. As time passes, the provider serves the patients on the schedule and makes the queue shorter. When the provider is off duty, no patients call in to join the queue and no patients are served or leave the queue either; the queue remains unchanged. Observing this, we can “drop” the non‐office hours of the provider and “coalesce” the office hours together to consider a continuous queueing process.
When patient appointment times come, they arrive on time if they show up, but they may not show up for their appointments. We assume that if there are j patients in the system when a new patient makes the appointment request, this new patient will be scheduled as the (j + 1)th patient in the system and show up with probability





Each scheduled patient who shows up brings in one nominal unit of revenue. If a patient does not show up, the provider cannot serve the next patient right away because every patient is scheduled and they will not come until their scheduled time slots. This can also be thought of as that the provider is “serving” the appointment slot of this no‐show patient before moving to the next one. Without loss of generality, we assume that if a patient does not show up or there are no patients scheduled in the current slot, the provider is able to fill in the slot by completing one ancillary task. Examples of these ancillary tasks include follow‐up service coordination for a patient, checking lab results, consulting with a patient's other providers and responding to a patient's email or phone call. These tasks may be billable to some (but not all) payers and typically with a lower reimbursement rate compared to that of direct patient care service (Merrell and Berenson 2010). To capture this, we assume that a revenue of ξ ∈ [0,1) is generated for each of these tasks (we call ξ the ancillary task revenue rate). We further assume that patient arrivals preempt ancillary tasks. That is, when an actual patient arrives, physician stop doing ancillary tasks if any and turn to serving the arriving patient. This assumption is certainly reasonable when ancillary tasks are interruptible as many are, such as replying to patients’ emails. We also make this assumption to keep our models tractable.
The service provider has control over the appointment scheduling window, that is, how far into the future a new appointment can be scheduled. Since the length of each appointment slot is deterministic, this is equivalent to controlling the queue capacity, which we denote by K. If the current length of the appointment queue is less than K, the provider will schedule new patients when they arrive. However, if there are already K patients in the queue (including the one in service), the provider will not schedule the incoming patient. This action incurs a penalty cost of θ ≥ 0 per patient. This is to capture the fact that this “rejected” patient may choose to seek care elsewhere resulting in loss of revenues to the provider or she may have to be accommodated using overtime work at additional cost (more on this below). The goal of the service provider is to maximize the long‐run average net reward, that is, revenue less cost, by choosing a proper queue capacity K. Put into the original operational context, setting a queue capacity K is equivalent to choosing an appointment scheduling window to be K/μ days.
Let T(K) denote the long‐run average net reward collected by the system. Define






The first term on the right side of Equation 2 is the revenue obtained from patients who showed up for their scheduled appointments and ancillary tasks completed in place of no‐show patients. The second term is the revenue obtained from ancillary tasks when there are no scheduled patients in the queue. To be specific, we note that the steady‐state probability that the server has no scheduled customers waiting is






Although we can numerically calculate





Optimal Capacity for the Appointment Queue
In this section, we derive the optimal capacity for the appointment queue. For ease of discussion, we let

For any fixed λ,μ > 0, net reward T(K) is a quasi‐concave function of K over




Our intuition suggests that there exists a trade‐off between choosing a larger K vs. a smaller K. When the appointment queue capacity is larger, fewer patients are “rejected” but patient delay is longer leading to more no‐shows and diminishing efficiency. When K is smaller, patients scheduled are more likely to attend their appointments but the provider leaves a larger proportion of patients unscheduled, resulting in lower revenues and more non‐scheduling penalties. Proposition 1 confirms our intuition above and establishes that the net reward is a weakly unimodal function of the appointment queue capacity K. To give an intuitive explanation, recall from Equation 1 that the expected revenue from scheduling a patient with j appointments ahead is






As a direct result from Proposition 1, we obtain the following Corollary, which identifies a necessary condition for

If


Corollary 1 implies that the optimal appointment queue capacity occurs at some integer K where the value of








Sensitivity Results
The last section investigates the property of the net reward function and how to find the optimal appointment queue capacity



We first investigate how the adoption of a new intervention (e.g., use of a reminder system) that is expected to change no‐show probabilities affects the optimal appointment queue capacity. We use






Intuition might suggest that if patients have higher show‐up probabilities, then the system can use a longer appointment queue to optimize the system performance because patients are more “reliable.” The argument is that, since patients are more likely to attend the appointment given the same appointment delay, the clinic can have a longer appointment queue to keep scheduled patients. It is true that keeping a longer appointment queue in a system with higher patient show‐up probabilities might still achieve an equal or even better net reward compared to a system with lower patient show‐up probabilities, because scheduled patients are more likely to come and the non‐scheduling penalty is smaller with a longer appointment window. However, the objective here is not to maintain or simply beat the same reward level as a system with low patient show‐up probabilities, but rather to optimize the reward rate under high patient show‐up rates. Thus, the intuition above is flawed, as demonstrated by the following example.
Suppose that the average daily capacity of the clinic is 20, that is, μ = 20 and appointment arrival rate λ = 17. Let









Example 1 implies that following one's intuition to adjust appointment queue capacity can be counterproductive. Then, one question arises naturally: what conditions, if any, would ensure that










Condition 1 requires that after the intervention, the decrease in show‐up probability with additional appointment delays is smaller compared to that under the original system. That is, patients are less “sensitive” to additional delays in the new system. Condition 1 also implies that

If condition 1 holds and other model parameters are fixed, then

It is interesting to note that when θ = 0, that is, when the non‐scheduling penalty is zero, the following condition, slightly weaker than condition 1, guarantees Proposition 2 to hold.

Condition 2 requires that






We now study how the provider should adjust the capacity of appointment queue in response to changes in other model parameters, including the demand level λ, service rate μ, non‐scheduling penalty rate θ and ancillary task revenue rate ξ. We are able to establish the following monotonic relationships.
Other model parameters being fixed, the optimal capacity for the appointment queue, decreasing in the demand rate λ; increasing in the service rate μ; increasing in the non‐scheduling penalty rate θ; increasing in the ancillary task revenue rate ξ.

In this study, we use the terms “increasing” and “decreasing” to mean “non‐decreasing” and “non‐increasing,” respectively. Proposition 3 states that as the appointment demand increases, the service provider should be stricter and allow fewer outstanding appointments. This might sound counterintuitive at first. In response to a surge in demand, one might be tempted to allow more appointments to benefit from the increase. However, in fact, the increase in demand is all the more reason to limit the size of the appointment queue. Higher demand means less need to accumulate customers in the queue since the service provider has less trouble filling the empty appointment slots. For a fixed appointment queue capacity, higher demand means longer customer wait time and thus higher no‐show rates. Reducing appointment queue capacity in this case leads to shorter appointment delays and thus reduces no‐shows. The revenue gains outweigh the cost of having more patients unscheduled due to reducing the appointment window. In short, this result suggests that for efficiency‐maximizing service providers who experience high demand, there may be fewer incentives to offer appointments far into the future.
The other three monotonic relationships seem to follow our intuition well. As the provider improves her service rate, she can tolerate longer appointment queues because customers will wait less and thus have lower no‐show rates. When the non‐scheduling penalty rate increases, there are more incentives to accommodate customer requests and thus the provider inclines to have a larger appointment queue capacity. When the reimbursement for value‐added tasks increases, the impact of no‐shows on system efficiency decreases and a longer appointment queue appears more preferable to the provider.
Numerical Study
In this section, we present our numerical study and results. The most important parameters in our numerical study are patient no‐show probabilities, and we start by discussing how we chose these parameters for our study in section 3.1.
Our numerical study has two main purposes. First, we will check if the M/M/1/K model is a reliable approximation for the M/D/1/K model in section 3.2. As discussed earlier, the M/D/1/K model appears more realistic in representing an appointment system compared to the M/M/1/K model, and our structural results in section 2 are all developed based on the M/M/1/K model. Thus, we will first examine whether Propositions 2 and 3 would continue to hold under the more realistic M/D/1/K model. In addition, we will investigate how “close” the M/M/1/K model approximates the M/D/1/K model in suggesting the optimal appointment window, the key decision variable of interest to us.
The second purpose of our numerical study is to answer an important question set forth earlier: how much efficiency gain can be realized by adopting an optimal appointment window when a practice may or may not have other operational levers (e.g., panel size selection and overbooking) available to deal with patient no‐shows? Insights to this question can inform practitioners the conditions, if any, under which it is worth considering putting a limit on the appointment scheduling window. We discuss these insights in sections 3.3 and 3.4.
Patient No‐Show Probabilities
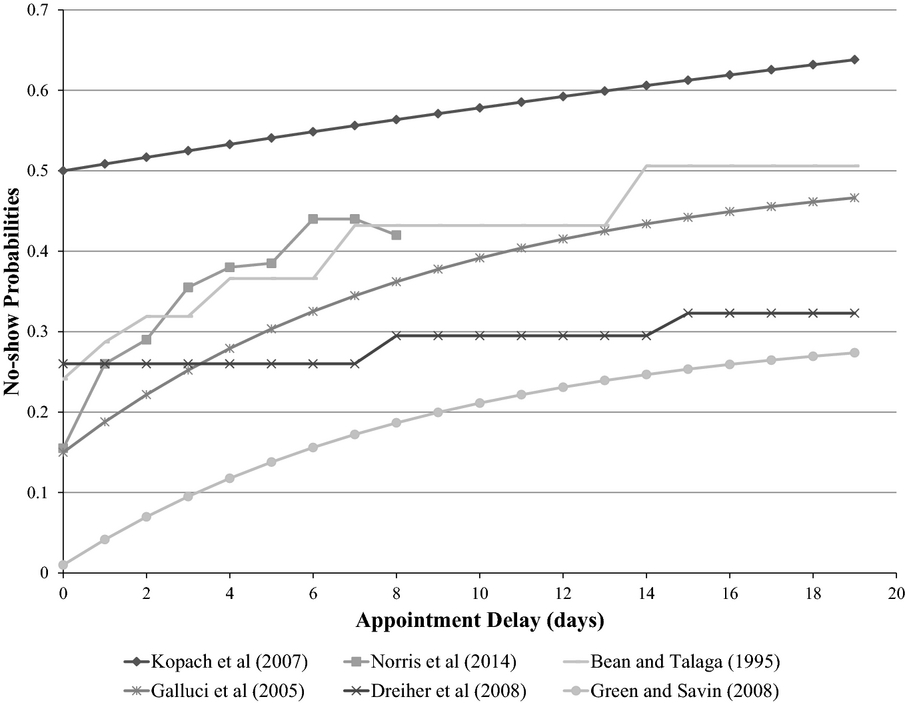
We envision our model can be helpful for any appointment‐based ambulatory care services that consider adjusting appointment scheduling windows as a means to improve their operational efficiency. To this end, we plan to test our model on a representative set of patient no‐show probabilities in ambulatory care settings, rather than on a single organization's data. To obtain realistic and representative parameters for patient no‐show rates, we surveyed recent healthcare OM as well as medical literature that explicitly reports the relationship between patient no‐show probabilities and patient appointment delays in ambulatory care services. This survey is by no means comprehensive, but it gives some idea on the range of patient no‐show probabilities. Interestingly, we find significant variation in patient no‐show probabilities reported in the literature. Figure 1 shows how patient no‐show probabilities change as appointment delays increase in various settings, including intercity primary care clinics (Kopach et al. 2007), primary care practices affiliated with academic medical centers (Norris et al. 2014), OB/GYN care settings (Dreiher et al. 2008), mental health facilities Gallucci et al. (2005), health care referral services (Bean and Talaga 1995) and MRI facilities (Green and Savin 2008). Among these settings, patient no‐show probability for same‐day appointments ranges from 1% to 50%, while that for an appointment 2 weeks from the request date varies between 25% and 61%.
Survey of Patient No‐Show Probabilities
To capture such a wide spectrum of patient no‐show probabilities, we base our numerical experiments below on patient no‐show probabilities reported in Kopach et al. (2007), Gallucci et al. (2005) and the MRI facility of Green and Savin (2008), which represent scenarios of high, medium and low no‐show probabilities, respectively. To be specific, patient show‐up probabilities


Comparison of M/M/1/K and M/D/1/K models
In the comparison of M/M/1/K and M/D/1/K models, we use three different sets of patient show‐up probabilities given in Equation 9. We fix the daily service rate μ = 20, but vary the level of demand rate λ ∈ {18,18.5,19,19.5,19.9,19.99} to study the impact of system workload. We consider different combinations of the ancillary task revenue rate ξ and the “rejection” penalty θ. Medical reimbursement data show that ξ is usually smaller than 1. For instance, a 2013 non‐facility Medicare fee for an 11–20 minute phone consultation is $19.25 (CPT code 99442), about one third of that for an office outpatient visit, which costs $53.25 (CPT code 99213). In our experiments, we allow ξ ∈ {0,0.3,0.5}. The parameter θ can be understood as the extra relative cost compared to revenue that the provider would be willing to pay in order to accommodate a patient who would otherwise be rejected. We consider θ ∈ {0,1.0,1.5}, corresponding to three hypothetical cases: the provider is unaffected by rejecting patients due to a full schedule; the provider would be willing to pay an amount equivalent to the revenue generated from serving the patient to avoid a rejection; or the provider would be willing to pay 50% more than an office visit revenue to avoid a rejection. In total, we consider 162 =3 × 6 × 3 × 3 scenarios for each of the two queueing models. Table 1 shows a subset of the optimal appointment queue capacities in these scenarios. We choose not to include results pertaining to ξ = 0.3, θ = 1.0 and λ ∈ {18.5,19.5} because adding these results would not contribute much to the discussion.
Comparison Results between the M/M/1/K and M/D/1/K models






The optimal appointment queue capacity is denoted by 
We can make a few important observations here. First, under the M/D/1/K model, the optimal appointment window becomes smaller when the demand rate λ increases with θ and ξ fixed. However, when θ or ξ increases with other parameters fixed, the optimal appointment window gets larger. These are consistent with Proposition 3, proved under the M/M/1/K setting.
In addition, one can numerically verify that according to Condition 1, patients in MRI facilities of Green and Savin (2008) are less sensitive to delays compared to patients in Gallucci et al. (2005). When j ≤ 300 (see Equation 9 for definition of j), sensitivity of patients in Kopach et al. (2007) is higher than that in Green and Savin (2008) but lower than that in Gallucci et al. (2005). Based on this ranking information of patient sensitivity as well as Proposition 2, it is not surprise to see that 

We also note that all the optimal appointment queue capacities are multiples of 20. Recall Corollary 1 which implies that the optimal appointment queue capacity only occurs at the point where patient show‐up probability has a strictly positive decrease. In our case, patient show‐up probabilities drop only at the queue capacities of multiples of 20, the daily service capacity. For example, 
To examine how “close” an M/M/1/K model approximates an M/D/1/K system in making suggestions for the optimal appointment scheduling window, we note that the M/M/1/K model is able to make exactly the same suggestion as the M/D/1/K model in 28 out of the 72 scenarios we studied. For the rest of 44 cases, we evaluate the efficiency loss in the M/D/1/K Model due to using the optimal appointment window suggested by the M/M/1/K model. Specifically, the efficiency loss is evaluated as 


Efficiency Gains Resulted from Adopting

In this section, we study how much efficiency gain can be achieved by adopting an optimal appointment scheduling window when practices may or may not use other operational levers.
Cases when Practice Cannot Adjust Panel Size or Overbooking Level
This section deals with the case in which a practice cannot adjust its panel size or overbooking level. Our numerical experiments use similar parameter settings as in section 2. Specifically, we use three different sets of patient no‐show probabilities defined in Equation 9. We fix μ = 20 and vary λ ∈ {18,19,19.9,19.99}, ξ ∈ {0,0.3,0.5} and θ ∈ {0,1.0,1.5}. Different arrival rates λ represent different levels of workload ranging from lightly utilized to extremely congested. We evaluate the efficiency gains based on both M/M/1/K and M/D/1/K Models.
For a given queueing model and a fixed set of parameters, we assess the long‐run average net reward obtained by the system when patients can be scheduled any time into the future, that is, we calculate T(K) defined in Equation 2 for K = ∞. Then, we evaluate the long‐run average net reward when an optimal appointment window is used. That is, we calculate 


Efficiency Gains Resulted from Adopting 








From Table 2, we find that adopting an optimal appointment scheduling window does not improve efficiency much when patient demand is relatively low compared to daily service capacity (see cases when λ = 18 or 19). However, when patient demand increases, the efficiency gain can be substantial, more than 40% in some cases. To further explore this, we evaluate the probability of a random patient seeing no more than 



We also note that the efficiency gains become smaller when the “rejection” penalty θ or the ancillary task revenue rate ξ is larger. These observations are in line with what Proposition 3 suggests. As θ or ξ increases, 

Cases when Practices May Adjust Panel Size and Overbooking Level
In this section, we consider the cases in which practices can adjust their panel size and overbooking level freely. We adopt the same three sets of patient no‐show probabilities as above, and vary θ ∈ {0,1.0,1.5} and ξ ∈ (0,0.3,0.5) in our experiments. We consider both the M/M/1/K and M/D/1/K queueing models. Given a queueing model and a fixed parameter setup, we assume that the practice first optimizes its panel size and overbooking level following the model of Liu and Ziya (2014), which we briefly recapitulate below. In particular, the practice solves the following optimization problem first.


After the practice solves the optimization problem (9) above and obtains the optimal patient demand rate 




Performance Results of Adopting 















From Table 3, we observe that once the panel size (and the overbooking level) is optimized, the efficiency gains by further adopting an optimal appointment scheduling window are limited (less than 1% in all scenarios). To explain this, we evaluate based on both queueing models, the service level defined as the probability of patients seeing no more than 

Efficiency Gains Due to Jointly Optimizing All Operational Levers
To further explore the efficiency gain by controlling the appointment scheduling window, we consider cases when practices can jointly optimize all operational levers: panel size, overbooking level and appointment scheduling window. Specifically, the practice solves the following optimization problem.




Extension to Heterogeneous Customers
The previous sections deal with models with homogeneous customers. However, customers with different personal characteristics may differ in their no‐show probabilities. For instance, patients who had missed their prior appointments tend to have a higher chance of breaking their future appointments (Norris et al. 2014). Observing this phenomenon, providers may use different appointment windows for patients depending on their no‐show behaviors (D. Rosenthal 2011, Columbia University, pers. comm., DuMontier et al. 2013). In this section, we consider a simple stylized model with heterogeneous customers to study such decision making. In particular, we assume that there are two types of patients who differ in their arrival rates and show‐up probabilities. Type i patients join the queue according to a Poisson process with rate 





Except for the differences above, these two types of customers are the same in other aspects and model assumptions are also similar to those of the M/M/1/K model with homogeneous customers considered in section 2. The service times of each customer are i.i.d. exponential random variables with mean 1/μ. If the scheduled customer does not show up for an appointment slot or there is no customer scheduled for that slot, the provider is able to fill it by an ancillary task which yields a reward ξ ∈ [0,1). Each patient served brings in one nominal unit of reward and each unscheduled patient incurs a cost θ to the system. The provider's objective is to maximize the long‐run average net reward by choosing 

One can show that for this stylized model, the long‐run average net reward given 


















Case that Requires K1 = K2
When the service provider choose to use the same appointment window, she simply sets 










Case that Allows K1≠ K2
When the provider can freely choose appointment windows, intuition suggests that the provider would be better off by offering a longer appointment scheduling window for customers who have higher show‐up probabilities, because these “better behaved” customers can be held longer in the system while still having the same or higher show‐up probabilities. Indeed, such a scheduling paradigm is widely adopted in practice to deal with frequent no‐show offenders by offering them very short appointment windows (see D. Rosenthal 2011, Columbia University, pers. comm., DuMontier et al. 2013). However, we have seen that the intuition above fails when customers are homogeneous (or equivalently, when the provider does not know the patient type information but can only treat every patient as a random draw from a patient population with a common no‐show probability distribution). In that case, solely improving customer show‐up rates does not guarantee a larger appointment scheduling window to be optimal (see Example 1). Customer sensitivity to delays plays a more important role there. Could customer sensitivity to delay play a similar role when customers are heterogeneous in their no‐show behavior and the provider knows exactly their type?
The following proposition provides some answer to the question above. It actually points to a different result to the homogeneous case. When patients are heterogenous and the provider knows exactly their type, it would be optimal for the provider to set a longer appointment window for patients with higher show‐up probabilities, irrespective of their sensitivity to delays.
If 


To give an intuitive explanation for Proposition 4, imagine that the provider sets an appointment window 



In the proposition above, 


Conclusion
Patients’ no‐show behavior presents a significant problem faced by many health care providers. Since patient no‐show rates usually increase with their appointment delays, one commonly‐adopted operational strategy by providers is to control the length of the appointment window. By limiting patients from making appointments too far away into the future, the provider reduces patient appointment delays and thus no‐show rates. Although there is a growing body of literature on various operational strategies to deal with patient no‐shows, little is known about the impact of varying appointment scheduling windows on a provider's operational efficiency. This study is directed to fill this knowledge gap.
The key trade‐off here is between the efficiency loss due to high no‐show rates following from allowing a longer appointment window and the “penalty” resulted from an overly restrictive appointment window driving too many patients unable to schedule their appointments. We capture this trade‐off by using a single server queue to model the appointments registered in a provider's work schedule. The capacity of the queue serves as a proxy of the length of the appointment window. The provider wants to set a common appointment window for all patients, who have higher no‐show probabilities when their appointment delays are longer, to maximize her long‐run average net reward. Using a stylized M/M/1/K queueing model, we provide analytical characterizations for the optimal appointment queue capacity, and study how the optimal scheduling window should be adjusted in response to changes in other model parameters. Through extensive numerical experiments, we confirm that our analytical results continue to hold in more realistic settings. In addition, one particularly useful message from our numerical study to practitioners is that adopting an optimal appointment scheduling window can lead to substantial efficiency gains if the provider has no other operational levers at hand to deal with patient no‐shows. However, when the provider can adjust panel size and overbooking level, limiting the appointment scheduling window serves more as a substitute strategy, rather than a complement.
Our work points to several directions for future research. First, our model extension studies a single server queue with two types of patients differing in their no‐show probabilities. The provider knows the type of each incoming patient, and may set different appointment windows depending on patient type. These patient type‐specific appointment windows, however, are static over time and independent of the system state. A dynamic admission policy which depends on the current patient composition in the queue or a policy that sets a limit on the number of each type of patients in the system holds the promise of further improving system efficiency. However, these variations would lead to completely different and likely more challenging optimization problems, which we leave for future research. Second, in our model with heterogeneous patients, we assume that providers can perfectly segment patients based on their no‐show probabilities. However, misclassification errors may occur in reality and it is important to study how such errors can affect our analysis and results. Third, our model is stylized in nature mainly for deriving managerial insights and more research is needed to develop decision support tools for practical use. For example, patients may have stronger preferences for convenient times of day rather than shorter appointment delays, and thus they may not accept the earliest available appointment. In addition to no‐shows, patients may cancel in advance or reschedule their appointments. These patient behaviors can leave “holes” in the appointment queue. In this case, a first‐come‐first‐served queue may not be an accurate representation. Thus, one avenue for future research is to examine the connection between the appointment window size and the operational efficiency in a more realistic setting. Analytical study based on stylized queueing models may be difficult, but simulation experiments are likely to yield useful results.
Footnotes
Acknowledgments
The author is grateful to the departmental editor, the senior editor and the anonymous referees, whose comments and suggestions have helped improve this work. The author also thanks the audience at the workshop on Data‐Driven Decisions in Healthcare, organized by the Statistical and Applied Mathematical Sciences Institute (SAMSI) in 2013 for their useful feedback. This work was partially supported by the Calderone Junior Faculty Research Award, Mailman School of Public Health, Columbia University.