
Abstract
Over 60% of decedents in the United States have not given first‐person consent for tissue donation; thus, receiving consent from next‐of‐kin (NOK) is a potentially powerful way to improve access to donor tissues. As a more informed NOK is more likely to consent to tissue donation, we introduced the delivery of two alternative videos that discuss the benefits of donation as part of the donation request. One was an animated, freely available video developed by the US Health Resources and Services Administration, and the other was a customized interview‐based video made in partnership with the Nevada Donor Network. We focused our analysis on studying the effect on White donation rates; many historical factors (in the United States) make the kind of simple, minimal intervention we implemented unlikely to be sufficient to encourage non‐White donation. We found in the field experiment that NOKs were more likely to donate if they viewed either video but that the two videos were not statistically different in their effect. As those who viewed a video may have been predisposed to donate, we additionally performed an online experiment that does not suffer from this endogeneity concern. We found results parallel to those in the field, and based on written comments by participants, we found suggestive evidence that the informational content in the videos was the mechanism that led to increased donation willingness and not emotional connectivity. We have identified a cheap and easy‐to‐implement intervention that could improve tissue availability across the nation.
Keywords
INTRODUCTION
Donation of tissues after the death of just one decedent can improve the lives of dozens of people through the receipt of corneas, skin, or other tissues (Donate Life America, 2021a). Organ Procurement Organizations (OPOs) work to gather these types of life‐giving or life‐improving materials (in addition to organs) for those in desperate need. Tissues are important in improving the quality of life for those with diseases that have damaged important tissues (such as their cornea) or have been injured (such as in a fire). Though there is a significant and ongoing focus on increasing first‐person consent (FPC) through donation registration drives (and at Department of Motor Vehicles, DMVs), nearly 70% of the deceased in our setting (Nevada) had not given FPC to donate their tissues. Consequently, we focused on consent from next‐of‐kin (NOK) which is less than 50% in our setting (of the 70% without FPC). NOK consent is the NOK's agreement to donate a decedent's tissues when the decedent has not given FPC. Because the process of increasing FPC has already been studied substantially (Degenholtz et al., 2015; Gordon et al., 2016), our research investigated this other bottleneck in service operations supply management. We—and our OPO partner—saw this as an area ripe for meaningful improvement. An improvement would entail an increase in the overall yield of donated tissues and thus improve outcomes for many individuals waiting for tissues.
Key features that increase a NOK's willingness to donate are receiving useful information about the process (Gordon et al., 2016), easing concerns about body integrity (Sque et al., 2018), and spiritual or religious acceptability (Sque et al., 2018). The complexity of providing information about tissue donation to NOK is high because the donation conversation is entirely over the phone (unlike organ donation, where the interaction between the donor coordinator (DC) and NOK is face to face). In this paper, we investigate whether the willingness to donate tissues can be improved through the viewing of an informative video that is sent to the NOK after the initial call with the DC.
FPC and NOK donation rates are even lower in minority communities (as compared to Whites), who are known to be more skeptical of donation (Boulware et al., 2007; Siminoff & Sturm, 2000). Varied reasons for this hesitancy—distrust of institutions, historical exploitation, and so forth— potentially create additional hurdles difficult to overcome; we, therefore, focus on Whites in our hypotheses and analysis. Let us emphasize that we do not intend to suggest that tissue donation from non‐Whites is unimportant, merely that we believe that our approach just by itself was unlikely to be an effective tool for this group.
This paper describes a field experiment with the Nevada Sharing Network, the OPO for Nevada, which uses a script for the phone interaction between an OPO employee and a potential donor's family. We enhanced the existing script so that it offered families a video providing information about tissue donation. After the video link was offered, engagement with the link by the NOK could be tracked. The content of the video the family received was randomized between two videos that provided similar information but with different delivery mechanisms. The informational video was animated and provided details about the benefits and process of donation. The interview video contained interviews with families who had donated a family member's tissues or received donated tissues. We anticipated that these interviews would be more relatable to NOK because the information was coming from other NOK, with whom the focal NOK might identify. Thus, we anticipated that those who were assigned to watch the interview video would be more likely to donate. However, the field study contained issues such as endogeneity concerns. Thus, we conducted a randomized online experiment in which all participants viewed a video, to investigate the mechanisms that affected changes in an individual's willingness to donate after viewing the video. This online experiment was complementary to the field because it did not suffer endogeneity concerns, and it allowed us to investigate what specific elements of the videos affected donation willingness.
This paper contributes to the literature on tissue donation in a few ways. Though other work has demonstrated that information‐sharing and behavioral nudges can benefit society broadly (Choudhary et al., 2021; Halpern, 2016; Krijnen et al., 2017; Thaler & Sustein, 2009), our paper brings this research to the context of tissue donation. Tissue donation is paramount, as a donor can improve the lives of up to 75 people (Donate Life America, 2021a). Providing a video to the NOK is a simple addition to the existing discussion process and therefore has a low cost to the OPO. Using an intervention to focus on NOK instead of FPC is both a novel and critical opportunity to increase overall tissue donation and is our main contribution.
Our paper also has implications for service operations management, especially healthcare, beyond this particular application. Persuasive marketing tactics toward public health for various customer segments have been long studied in that field (Wolf et al., 2014). Vaccine hesitancy is front and center in the current Coronovirus pandemic, highlighting the importance of seriously studying behavioral strategies to increase acceptance of public health measures such as vaccination, tissue donation, or tobacco cessation (to name a few).
Our paper is organized as follows. Section 2 provides a literature review on the setting and the major theoretical drivers that affected the design of the experiment. Section 3 discusses the specific setting where we conducted the field experiment. Section 4 describes the field experiment. Section 5 describes the online experiment, and Section 6 provides a general discussion as well as directions for future work.
LITERATURE REVIEW AND HYPOTHESES
A significant supply problem for donor tissue persists in the United States, partly because FPC rates are low, leading to long waiting lists (Kessler & Roth, 2014). Current initiatives aim to address this issue primarily by increasing the rate of FPC by prompting individuals to sign up as donors (Degenholtz et al., 2015; Harper, 2013; Razdan et al., 2016) or by reducing waiting time disparities (Ata et al., 2016). However, the NOK of the deceased often makes the final decision about tissue donation, especially in the 60% or more of cases without FPC (Halpern, 2016; Ralph et al., 2014; Rosenblum et al., 2012). Thus, if NOK rejects donations for potential donors, another source of supply for new tissues that could reduce waiting times and improve lives is also lost. A low NOK consent rate thus creates a bottleneck, which we hope to address, thereby potentially improving operational processes and increasing yield for OPOs. Each tissue donor has the ability to improve the lives of up to 75 others (Donate Life America, 2021a). Demand for corneas is such that only one is accessible for every 70 people in need, globally, and the global median wait time is over 6 months (Gain et al., 2016). Low and uncertain supply due to yield is a canonical problem addressed by operations management and is especially relevant in healthcare settings where the quality‐of‐life impact is even more direct, as in the case of tissues.
Being asked to donate a loved one's tissues is typically a novel situation where lack of information about the benefits or process of donation contributes to a lack of consent (Boulware et al., 2007; Gordon et al., 2016; Sander & Miller, 2005; Sque et al., 2018). Thus, we anticipated that providing additional information about the positives of tissue donation would increase donation willingness for NOK: As individuals seek out more information about tough decisions, they are typically able to make better decisions (Desender et al., 2018). When an OPO reaches out to NOK to discuss a donation, this is called an “approach.” The volume of tissue donation opportunities necessitates that approaches for tissue are conducted over the phone, where there is both more physical and social distance between the DC and the NOK—unlike approaches for organ donation, where DC typically engages with NOK in person. Thus, we anticipated that delivering information in a medium richer in content than just audio (which is used over the phone) or text (DCs already send text‐based material to NOK) could help overcome barriers of distance. Even small informational nudges can lead to behavioral and decision changes (Choudhary et al., 2021). We thus expected that information delivered in the form of a video might be more compelling and help make up for the lack of rich face‐to‐face interaction. Our first hypothesis is: Viewing an informational video about donation will increase donation for NOK.
Individuals are more willing to trust information from someone they perceive as similar to themselves, a consequence of social identity theory (Tajfel & Turner, 1985). We often look to those we consider “in our group” for making appraisals of what to do with the information (Harmeling et al., 2017). Recognition of even minimal similarities can induce positive associations and willingness to listen to others (Kane et al., 2005). Recognition of similarity can also be made situationally (e.g., this is another person who faced the same decisions as I did), as long as the identity category is salient at the time of decision making (Forehand et al., 2002). Thus, we anticipated that if the video providing information was able to signal a shared identity with the NOK through the acknowledgment of shared experiences, willingness to donate would increase. In our scenario, the shared experience being signaled was that the individuals in the video were also from Nevada (the field site) and had also made a decision about donating a decedent's tissues. Thus, our second hypothesis is: An interview video about donation featuring individuals who previously made NOK donation decisions will increase donation for NOK more than a purely informational video.
Other research approaches have used video interventions directed at increasing FPC (Alvaro et al., 2010). However, though videos are already used in this context, they have not been directed toward our population of interest. Our approach is therefore unique in that the videos are directed specifically at NOK who are making donation decisions for those who have not given FPC. Additionally, NOK consent is particularly important for some of the best candidates for tissue donation such as those who died young or suddenly and may not have had an opportunity to become a registered tissue donor. As videos are already used in other ways by OPOs, we anticipated that this type of intervention could be quickly adopted.
FIELD SETTING
The OPO for the state of Nevada is the Nevada Donor Network. This OPO, as is typical within OPOs, has different organizational branches for tissue procurement and organ procurement. The majority of the population are not registered donors, and tissues are collected from decedents (via NOK consent) in many cases. See Table 1 for demographic information from the experimental period.
Nevada Field Experiment–demographic characteristics of participants
Note: The full sample includes all decedents who were considered by the Organ Procurement Organization. The nudgeable sample includes only those who had not previously given consent for donation. For next‐of‐kin (NOK) gender, data are not available for 710 cases in the full sample, 500 cases in the nudgeable subset, 430 cases in the not sent subset, and 70 cases in the sent subset. Donor coordinator (DC) gender data are missing for four cases in the Full sample, 3 cases in the Nudgeable subset, and 3 cases in the Not Sent Sample. For all subsets, the average of the available cases is presented.
Prior to the experiment's initiation, a typical approach for tissue donation would proceed as follows. A patient is admitted to the hospital and assigned a nurse. If the patient dies and is a tissue candidate, the nurse contacts the OPO. Once informed, the OPO calls the NOK—unlike the case of organ donation, which is an in‐person meeting—to inform them of the decedent's FPC status (e.g., the person had registered as a donor at the DMV) and request a donation. Most donation coordinators ask the family if they have thoughts about donation, discuss that tissue donation does not prevent traditional burials, and answer the family's questions. DC notes from these discussions indicate that many families are emotional and frequently are not interested in speaking with the donation coordinator. If the family does not immediately consent to or reject donation, then the donation coordinator will often schedule a call for a few hours later. This is often framed as an opportunity for family members to discuss, but with the insistence that a decision must be made soon while tissues remain viable. Some families accept or reject donations on the follow‐up call, though sometimes the families are not reachable, either because they do not want to speak with the donation coordinator again or for some other reason (e.g., the lateness of the hour). In the next section, we describe the strategy we developed to improve the donation process for over‐the‐phone tissue requests in Nevada.
FIELD EXPERIMENT
Video design
The primary innovation in our study was the systematic delivery of videos to NOK during the DC's telephone approach for tissue consent, in an attempt to provide additional information and improve donation likelihood. All videos that we used in this study were available in spoken English or Spanish with similar content regardless of language. We identified an animated video, produced by the US Health Resources and Services Administration as a good baseline video to determine if an informational video alone would improve existing consent practices. This video described the process through which someone gets on the waiting list for organs and tissue, indicated that the long wait can be hard on families, and explained that donation of either organs or tissues can help many people. The English video was 4 min long; the Spanish translation was 5 min long and contained identical information. More detailed descriptions and links to both are available in Appendix A1.
The Nevada Donor Network also hypothesized that a further increase in consent rate was likely through a second customized video with OPO‐identified interviewees from Nevada who had all been previously affected by tissue donation (either as recipients or donors). In this interview video, NOK discussed who their decedent was, mentioned their initial concerns about donation, and reflected on their decision. Recipients described how their lives had improved after receiving a donation and mentioned that many people can be helped by donation. The English video was 3 min long; the Spanish video was 2 min long. More information on these videos is available in Appendix A1. English was chosen as the preferred language 98.3% of the time.
Experimental design
A typical tissue approach during the experimental period proceeded as shown in Figure 1. The script that DC already used during an approach was provided to the authors, who created sample language that was integrated into the existing language used with the assistance of managers at the OPO. The DCs were then trained to use the videos by their managers, using the provided scripts. The authors also provided “testing” links so that DC could practice and be aware of what the experience for the NOK would be.
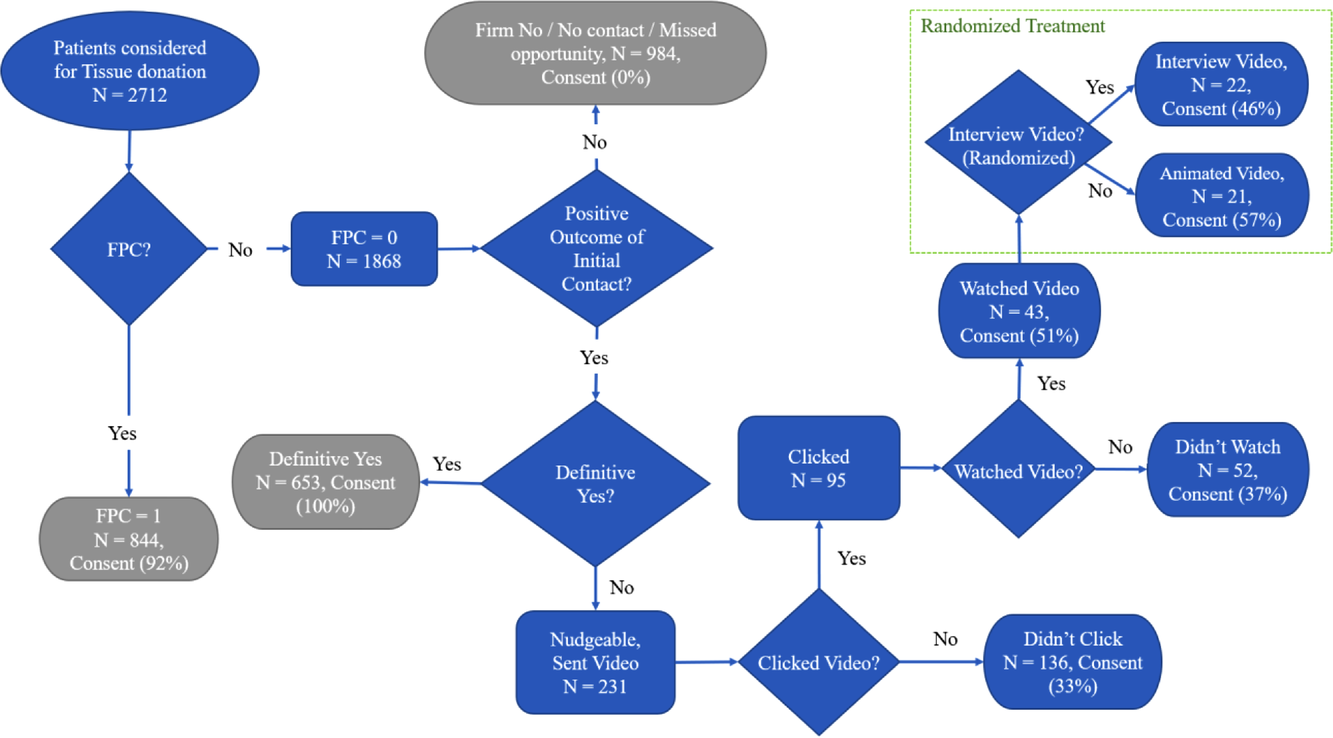
Nevada Field Experiment–Flow chart of approaches. Note: This figure includes all (next‐of‐kin) NOK approached, not just White NOK
If in the interaction with the DC, NOK responded with a definitive “yes” or “no” in response to tissue donation requests, that was the end of the interaction, no different from the standard process. If the NOK did not respond with a definitive “yes” or “no” about donation willingness, the DC offered the NOK a unique video link, which the NOK could accept or decline. The suggested language was to the effect of, “I would like to offer you a video with some more information about donation,” if the NOK agreed to accept the video, they were sent a link via text message or email and scheduled a follow‐up call. Though we do not describe non‐White NOK responses in detail in this paper, we did not exclude non‐White NOK from receiving the videos. The unique video link led to a page developed in the online survey platform Qualtrics, where NOKs chose their preferred language (English or Spanish) and were then randomly presented with one of the two videos. Importantly, the video the NOK saw (informational or interview) was determined by a random number generator after they chose a language. Thus, about half of those who participated by clicking on the survey link and choosing a language were assigned to view the interview video and half to the informational video. After the case was closed, the OPO provided the authors with data on decedents, NOK, and outcomes. Since each link was unique, clicking of a link could be monitored through the delivery software Qualtrics. This provided us information on which NOK clicked on the video link, whether NOK chose a language and thus could watch the video, and which video they watched (informational or interview), which was randomly assigned by the survey software. See Figure 1 for a summary of the flow of NOK in this process. See Appendix A2 for regressions investigating the relationship between demographics, FPC, and engagement with the experiment.
The main dependent variable in this experiment was consent for tissue donation by the NOK as obtained by the DC and reported to us through the OPO. The OPO also collected details on the self‐reported demographic characteristics of the decedent and the NOK. This study was approved by the institutional review boards at each of the authors’ respective institutions. As this study was approved as a minimal risk by both IRBs, no informed consent in the field experiment was obtained from NOK.
Results
Population
Between July 1, 2017, and July 6, 2018, 2812 decedents were considered for tissue donation. One hundred cases were removed due to missing data in registry status, donation outcome, decedent demographics, or inconsistencies in dates of the approach and video activation, potentially due to inadvertent DC‐link activation. This left a final number of 2712 cases of NOK who were approached for tissue donation, of which 1868 cases had no FPC. See Table 1 for a breakdown of demographic information of decedents by subset and Table 2 for correlations for each variable investigated.
Nevada Field Experiment–means, standard deviations, and correlations for White decedents
Note: The pattern of means and correlations are very similar for the full sample (not shown).
Abbreviation: FPC, first‐person consent.
*p < 0.05, **p < 0.01, ***p < 0.001.
The OPO also provided information for several years preceding the experiment. The year prior had a nearly identical number and distribution of decedents. The only notable trend across the year of experiment and the 3 years prior is a steady increase in the number of decedents considered; only 1947 were approached in our first year of available data. This suggests that the OPO has sought to consider more and more decedents each year.
Likelihood of being sent the video
For our analyses, we focused on the 100 White NOK who were sent the video. We predicted the likelihood of being sent the video for NOK of White decedents without FPC based on decedent demographic characteristics and controlling for the DC to test for non‐randomness in the link distribution. Decedent age was the only variable that affected the likelihood that NOK would be sent the video (
Effect of the video on consent likelihood
Our first hypothesis was that NOK would be more likely to consent to tissue donation when they viewed an informative video. These analyses are presented in Table 3 and visualized in Figure 2. The results for Model 1, the likelihood of NOK consent for tissue donation where FPC = 0, showed no significant effect of sent the video. In Model 2, however, we see a significant positive effect if NOK were sent the video and watched it. A calculation of a Cohen's D effect size based on the mean difference between those who were sent the video and watched it, compared to those who were sent the video and did not watch it, was 0.75, suggesting a strong effect of watching the video. These analyses provide support for Hypothesis 1 that NOK who viewed a video about donation were more willing to donate the decedent's tissues. For illustration, the predicted probability of consenting for the NOK based on the regression was such that a 55‐year‐old male decedent was 42.2% if they clicked on the video and did not watch it but was 77.1% if they watched the video.
Nevada Field Experiment–predictors of NOK consent for tissue donation—White decedents
Note: All models use logistic regression to predict consent to donate tissue from NOK. Values in parentheses are standard errors. The nudgeable sample in Models 1 through 3 is the subset of the data in which there was no FPC.
†p < 0.1, *p < 0.05, **p < 0.01, ***p < 0.001.
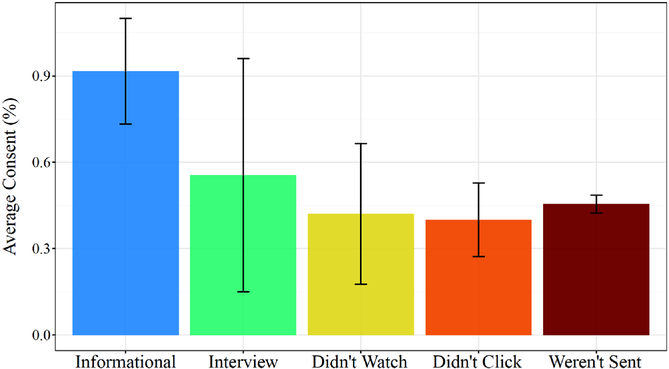
Nevada Field Experiment–Mean consent by video type and engagement for White decedents. Note: The error bars presented are 95% confidence intervals
Differing effects of video‐type
In the above analyses, we investigated the overall effect of watching a video without investigating any differences between the video approaches. We anticipated that the video containing interviews with NOK who had made donation decisions would be more influential than the animated informational video because those who watched the video would be able to identify with the interviewees since they had been in that same situation. In Model 3, we included a variable to compare the efficacy of the two videos on family outcomes. We see that the interview‐based video was marginally worse, compared to the informational video in convincing participants to donate their NOK's issues. Note that the overall effect of receiving the video was still positive (see the positive effects of clicking the link and watching the video) even for those who received the worse performing interview‐based video. Thus, we did not find evidence for Hypothesis 2 that the interview‐based video would be better performing. A post hoc power analysis suggests that our observed power for the test of Hypothesis 2 was 0.52, well below the traditional 80% cut‐off for power. Thus, due to relatively few participants opting to view the video, we are unable to make firm differentiation between the effects of the two videos.
An estimate of the population‐level impact of this intervention is the number of additional tissues available for donation. Adapting a method from Chanfreau‐Coffinier et al. (2015), we estimated the number of additional tissues we might expect to be donated if the whole population had been treated. The consent rate of the treated group (those who watched the video) was 76.2%, whereas those who clicked the video but did not watch it was 42.1%. If we assume that this 34.1% additional likelihood of donating would extrapolate to the rest of the population that was not sent the video, we can determine the estimated number of additional donations by multiplying the number of cases who were not sent the video (1007) by the additional likelihood (34.1%) and the rate at which participants watched the video (52.5%). This suggests that we might have expected an additional 180 cases of tissue consent had the rest of the population been treated. As each tissue donor has the possibility of improving the lives of up to 75 recipients (Donate Life America, 2021a), this could mean increased sightedness for those receiving cornea transplants, decreased healing times for burn victims, or other societal benefits (Donate Life America, 2021b).
Robustness of findings with statistically matched cases
We conducted a statistical matching analysis in which a control group was created by choosing a subset of cases from the treated condition that matched a subset of the untreated condition on traits such as gender and age (Wu et al., 2018). When repeating the regressions reported above with the statistically matched cases, the results are parallel to those reported above. More details are provided in Appendix A3.
Field experiment discussion
This field experiment highlighted that a video intervention could have a positive effect on the donation rates of NOK. We did not find evidence for Hypothesis 2, which posited that a customized interview‐based video would be superior. As the field experiment allowed for participants to opt into being treated, it is possible that the effects we saw are based on internalized preferences and thus endogenous. Our method to manage this self‐selection issue, in addition to the matching analyses above, was to conduct a fully randomized online experiment.
ONLINE EXPERIMENT
Design
Between July 16 and August 17, 2019, Qualtrics Panels recruited 620 participants from Nevada using quotas to ensure demographic representation of the state according to data from the US Census. Each participant received approximately $1 for participation. Participants were prescreened to include only those over 18 who understood the informed consent, committed to give honest answers, and were from zip codes in Nevada. After providing informed consent to participate, participants were presented with a scenario where they imagined that a loved one had been hospitalized. They then reported their loved one's demographic characteristics and thoughts on tissue donation, as well as their own thoughts on tissue donation. 1 Next, participants were asked to imagine that their loved one had died and that they could decide whether to donate the loved one's tissues. Participants responded to a question about how likely they would be to donate the loved one's tissues on a 5‐point scale from “extremely unlikely” to “extremely likely.” Participants were then randomly presented with the interview video or the informational video. We chose to provide only the English language video, as 98.3% of participants chose this version in the field experiment. We then asked the same question about donation willingness on the same 5‐point scale. The change in these ratings from before and after watching the video was our dependent measure. We also assessed (as is not uncommon in survey research) willingness to donate money to organize a non‐profit that helps inform NOK about donation options as a secondary more behavioral outcome. We asked participants what proportion of $1 they would like to donate. Participants could choose between $0 and $1 in $0.25 increments; they receive any remainder. To capture potential mechanisms, we asked participants to reflect on whether the video affected their opinions (in a text box), the positive influence of the video they saw on their feelings about donation (survey), and (for those who saw the interview video) the effect of individual interviewees on their feelings (survey). These two survey questions both used a 5‐point scale from “very negatively” to “very positively.” We last measured the Big 5 personality characteristics (Gosling et al., 2003) as a control as well as basic demographics. This study was approved by the institutional review boards at each of the author's respective institutions.
Results
Study population
Of the 620 participants in the survey, 85 were removed due to misalignment in their responses to two questions—a text response on whether they would donate NOK tissues and a scale indicating donation willingness—which indicated confusion about the scale; these are both attention checks that allow for low‐quality responses to be removed (Abbey & Meloy, 2017). Thus, our final sample size for the online experiment was 535 participants of whom 51.4% were female and a representative racial makeup (49.9% White, 30.1% Hispanic, 10.8% Asian, and 9.2% Black). Age was captured in ranges, with 26–35 and 65+ being the most common, at 20% each and 12%–17% in each of the four other categories. Means and correlations are provided in Table 4.
Online Experiment–means and correlations for White participants
Note: The pattern of means and correlations are very similar for the full sample (not shown).
*p < 0.05, **p < 0.01, ***p < 0.001.
Thirty‐three percent (N = 89) reported not having had conversations with their family about donation and were not certain that their family member had given FPC. We refer to them as the “unaware” sample, the best match to the subset in the field experiment who would be sent a video link. We performed the majority of the analyses on this sample, though the results are identical (unless otherwise noted) when the full sample is used.
Analyses on change in willingness to consent
Our first hypothesis was that viewing a video would increase participants’ willingness to donate. Using a paired samples t‐test, we found clear evidence that within the unaware sample, there was a significant positive effect of watching a video on increased willingness to donate tissue based on a 5‐point scale (Δ = 0.44, t(88) = 4.64, p < 0.001). An advantage of the paired samples t‐test is that each individual acts as their own control (as they made two reports of willingness to donate); thus, the power of this test is much higher than in the field setting. These analyses support Hypothesis 1 that viewing a video would increase donation willingness.
Hypothesis 2 posited that participants would be more positively affected by the interview‐based video than the informational video. We did not find a significant difference in the positive effect of the two videos on individuals’ willingness to donate. Those who watched the informational video had a change in overall donation willingness of 0.43 points, compared to 0.45 points for those who saw the interview video (t(87) = −0.10, p = 0.924). It may be more informative to compare percentages of individuals who moved from not choosing to donate to donation based on the video viewed. For those who viewed the informational video, an average of 9.5% increased to “extremely likely” from some lower value, whereas 2.1% of those who viewed the interview video experienced this, though these changes were not statistically significant (t(87) = 1.26, p = 0.209). Thus, in both the field and online experiments, we found no significant difference between the efficacy of the two videos. We also performed ordinal regression analyses, reported in Table 5, using the change in donation willingness as the dependent variable to provide comparable analyses to Table 3.
Online Experiment–predictors of change in donation willingness for White participants
Note: All models use ordinal regression to predict change in willingness to donate from before and after watching the video. Values in parentheses are standard errors.
*p < 0.05, **p < 0.01, ***p < 0.001.
The secondary dependent variable was the amount of money donated to organize. A small variance was reflected in this variable: 80.1% of participants in the total sample and 79.8% in the “unaware” sample chose not to donate any monies. Neither hypothesis was supported in analyses with this variable, suggesting that neither video outperformed the other in motivating monetary donation. There was no statistical difference between the amount of money donated based on demographics of the NOK, decedent, or which video was shown.
Analyses on mechanisms
The average participant said the video “positively” affected their feelings about donation (m = 3.9, sd = 0.8). If this video influence variable is included in the regression analysis in Table 5, it is a significant predictor of the change in donation willingness from before and after watching the video. Thus, unsurprisingly, if the participant reported that the video had a positive influence on their feelings about donation, they increased their donation willingness after watching the video.
Participants also provided written comments about whether and how the video changed their opinions about donation. Many of the written comments noted that the video did not influence their opinions because they already had strong positive or negative feelings before watching the video. We categorized these written comments into one or more codes: video had a positive effect, video provided information, video provided information on need, video provided information on body integrity, video reinforced my existing opinions, or video provided emotional support. Within the sample of nudgeable Whites, 22.5% stated that the video had positively changed their opinions. The most common reasons given were information (20%) and emotional support (15%). Not surprisingly, only the interview video was reported to provide emotional support, while both videos were reported to have provided information. Notably, the interview video was not seen as superior in improving willingness to donate in the prior analyses as in the field experiment. We have some direct evidence, therefore, that the informational content of the videos, as opposed to the emotional content, was a reason for a positive impact on donation willingness among those who were not pre‐disposed one way or the other.
DISCUSSION AND FUTURE DIRECTIONS
Our innovation was the introduction of a video to existing OPO activities related to obtaining tissue consent from NOK. This was complementary to existing initiatives to increase FPC. In both the field and survey experiments, we found clear support that NOKs were positively affected by being shown a video. We did not find strong evidence that one video was superior to the other in increasing donation willingness. Thus, we found that the use of a freely available informational video is an enhancement over just a phone discussion to increase the willingness of NOK to make positive donation decisions, increasing the total tissues available for donation. This initiative improves the performance of a bottleneck in tissue transplantation, which is the supply of tissues. Though our minimal intervention was investigated only for White decedents, an increased consent rate from these NOK was obtained with minimal DC resources, thereby allowing DCs to spend more time on improving donation rates for non‐White NOK in addition to the use of informational videos.
Our field experiment has several limitations. We identified some non‐randomness in the distribution of video links. Individuals in the field experiment who were positively predisposed to donate before being contacted by the OPO may have been more likely to accept or watch the video. The online experiment did not suffer from these endogeneity concerns, which was a primary reason we conducted this experiment, and we found substantively identical findings.
We recognize that the two videos we used were not identical. Some characteristics of the videos—the specific information shared, the language, the interviewees, and so forth—could each have independent and differing effects on the likelihood that the video would positively impact NOK donation. Our partner OPOs assessed the quality of both videos as equally high, but the OPOs expected that the interview video would be superior to the animated video. The experiments above seem to suggest, however, that these two videos were not statistically different in their positive effect on donation. Additional research would help identify whether the production costs of an interview‐type video are justified considering our results, or if a differently constructed interview video would be more effective, which we elaborate on later.
Our experiment prompts several possibilities for future research. Though we did not hypothesize the effects of the videos on non‐White NOK, reducing donation hesitancy among non‐White NOK is certainly valuable. We believe that viewing a video alone may not be sufficient to increase donation substantially within this community. Future experiments should focus more directly on meeting non‐White NOK needs. An unexpected learning upon sharing this work within the donation community was that although we anticipated that the animated video would be viewed as race‐neutral or race‐inclusive, experts on issues of race suggested that the animated video may have been viewed by non‐White NOK as sharing the information in a majority‐race (i.e., White) perspective through the diction as well as the choice of animation. Relatedly, during a similar study we conducted in Georgia that used the same interview videos, we learned that the Spanish language interview video was viewed as not representative of Spanish speakers in Georgia because the Spanish accents in the video (from residents of Nevada) were regionally different from that of a typical Georgia resident. Therefore, future studies must be far more aware of these nuances in developing, designing, and implementing video‐based initiatives to increase donation.
Future work should also investigate the use of videos directed at NOK of potential organ donors. As with tissue, there is more demand than supply for organs, and organs are more perishable than tissues, making the attainment of consent to donate somewhat more time‐constrained (Donate Life America, 2021b). We saw in both the field and online setting that uncertainty about the process and a loved one's desires were common themes in tissue donation as in organ donation (Ralph et al., 2014). Some participants in the online experiment noted that they appreciated watching the video, as it prompted them to plan a conversation with their loved ones. Thus, we encourage future research to focus on showing a video like ours pre‐emptively at sites including religious or community centers, as a way to encourage communities to be mindful of the end‐of‐life donation as NOK. Pre‐emptive engagement of potential donors using text (Murphy et al., 2020) or television advertisements (Alvaro et al., 2010) has been successful in increasing non‐White interest in FPC and living donation, so we encourage future research to investigate the efficacy of these techniques on tissue donation and NOK consent as well.
Inspired by our video efforts, OPOs have recently started to use “comfort videos” in Louisiana (Michael Clay, San Diego, personal communication, February 18, 2020). These videos attempt to encourage NOK to “join the family of donors” in activities beyond the act of donation, with a focus on belonging to the community and the shared identity of donor families. Future research should evaluate the efficacy of such strategies on both White and non‐White NOKs.
For now, we are pleased that the use of a freely available and informational video increased consent from White NOK in our field experiment. The comments from the online experiment suggested that those who were persuaded were so because of the informational content (as opposed to the emotional content) of the videos. We demonstrated that video interventions are easy to integrate into current processes and can be a tool to increase the number of tissues available for transplantation. We hope that our work here inspires other researchers to propose and evaluate innovations that improve the overall supply of tissues and organs.
Footnotes
APPENDIX
ACKNOWLEDGMENTS
We would like to thank Nevada Donor Network for partnering with us in the field study and Alan Scheller‐Wolf for providing detailed feedback on this manuscript.
1
Two questions—whether participants had given consent to donate tissue and whether they had spoken to their family about donation—allowed for a “rather not say” response. These values were treated as “No” for the 39 cases where this occurred.