
Abstract
Background
Transverse olecranon fractures are commonly fixed using a tension band wiring technique. This technique has a high rate of complications because of the prominent metalwork, frequently resulting in further surgery to remove the hardware. We investigated a new technique using two metal screw in bone anchors double loaded with Orthocord.
Methods
A tension band suture technique was employed in 22 patients (14 Mayo type IIA fractures and 8 olecranon osteotomies) using two double Orthocord loaded bone anchors in a standardised fashion. Twenty-one patients started mobilisation at 1 week. Patients were followed up until both clinical and radiological union was evident. Any problems with fixation hardware and complications were all recorded.
Results
The mean time of union was 6.4 weeks (range 5 weeks to 9 weeks). One patient developed an asymptomatic fibrous non-union and 20 achieved complete anatomical union. At a mean of 14.2 months, no patient had developed any hardware problem or required further surgery.
Discussion
Tension band suturing is a safe, easy and quick technique that avoids the risks associated with other methods of fixation. It provides a comparable union rate without any complications as a result of the hardware. In our series, no patients required further surgery.
INTRODUCTION
Olecranon fractures are common elbow injuries and occur from either direct trauma to the elbow, or indirectly as a result of the pull of the strong triceps. Furthermore, an olecranon osteotomy is often performed to obtain adequate surgical exposure when dealing with articular fractures of the distal humerus [1].
Fractures of the olecranon can be stabilised using tension band wiring, screw fixation, plate fixation or intramedullary locking nails [2 –7]. However, these modes of fixing both olecranon fractures and osteotomies are plagued with problems. Apart from the generic surgical associated morbidities, there is a high rate of metalwork complications. These vary in severity from discomfort and irritation caused by screws and wires to wound breakdown. These all necessitate further surgical intervention in the form of metalwork removal [3,4,8 –10]. Rare complications such as hand ischaemia have also been reported [11]. Some series have reported an extremely high rate of hardware complications, with tension band wiring requiring removal in 82.3% of patients [3]. These rates tend to be a little lower in fractures requiring plate fixation [5] but, often, those fractures fixed with a plate tend to be the more comminuted variety and are distinct from the standard transverse fracture or chevron osteotomy. The existence of numerous devices on the market for such a common fracture suggests that no ideal solution exists for their fixation.
The characteristics of an ideal device should avoid the problems of metalwork irritation or migration, avoid the risk of damaging anterior structures, have a low complication rate, be easily reproducible by different surgeons and provide comparable, if not superior, union and function rates, as well as be cost-effective.
We report a case series of patients who were treated with a novel surgical technique using suture anchors, which addresses the problems outlined above. We also present our early results for these cases.
MATERIALS AND METHODS
Surgical technique: Tension band suturing
The patients were placed in the lateral position after the induction of anaesthesia and prophylactic antibiotics. After draping and preparation, a curvilinear posterior midline incision was made (curved to the radial side over the olecranon to avoid placing an incision directly over the tip).
The fracture site was cleared and articular debris was removed. The fracture was reduced and held temporarily with a 2-mm K-wire. Two metal screw-in bone anchors double loaded with Orthocord (Fastin RC 5.0 mm; Depuy Mitek, Leeds, UK) were inserted into the medial and lateral surfaces of the ulna, approximately 5 cm distal to the fracture or osteotomy site after a pilot hole was drilled with a 2-mm K-wire. The two anchors were placed at slightly different levels and the tips aimed towards the centrovolar surface (although their size ensured that this surface was not penetrated). One suture from each pair of suture strands was passed through the full thickness of the triceps as close to the tendon's insertion as possible in a zig-zag fashion. They were locked using a Mason-Allen suture and then tied to its counterpart as shown in Fig. 1. One strand from each anchor (A and D) was orientated in a vertical configuration and the other strands (B and C) in a cross fashion. Sutures were then tightened with the elbow flexed at 45 °C to ensure that the sutures were not too tight or lax in flexion or extension.
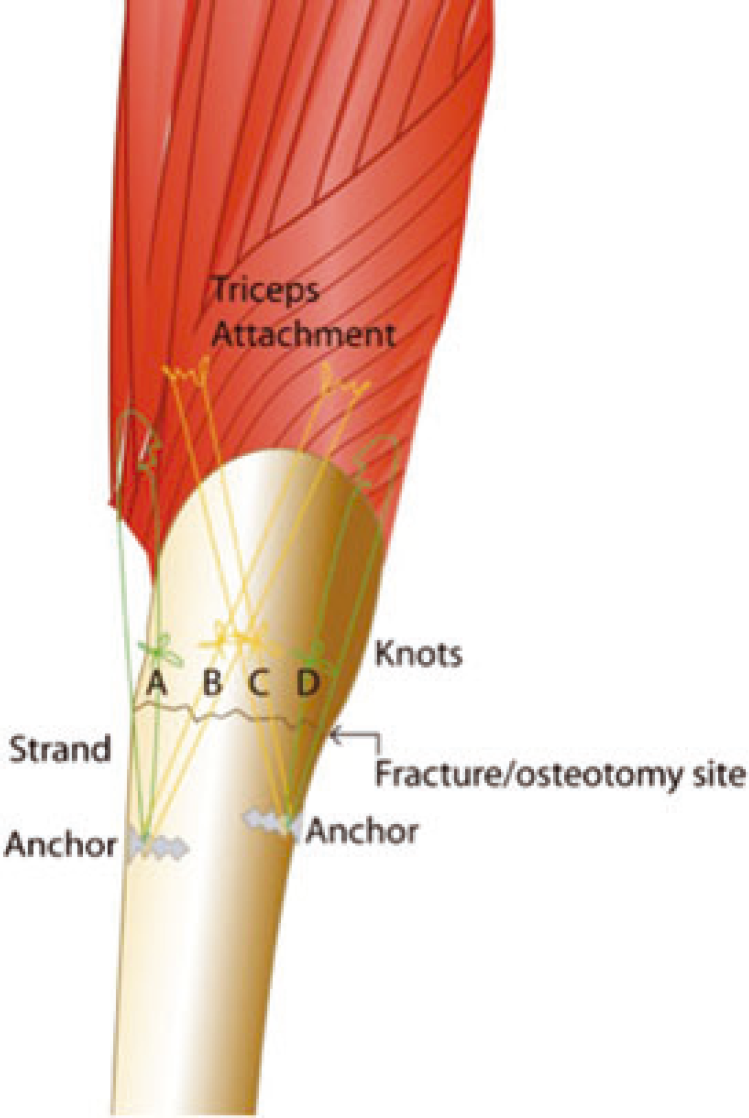
Schematic diagram illustrating the fixation technique.
The wound was irrigated and closed in the usual fashion using non absorbable interrupted stitches.
A bulky dressing was applied with a collar and cuff sling. A backslab was applied for the first week and range of motion exercises were encouraged after 1 week when the dressings were all removed. This was the senior surgeon's (MR) standard postoperative protocol when tension band wires were used for this procedure. Patients were advised against lifting heavy objects and exertional activities for at least 6 weeks. All patients were followed up until union. Union was assessed on the basis of radiological and clinical examination (i.e. an absence of pain and bony tenderness at the fracture site).
We present a case series of 22 patients who underwent tension band suturing with bone anchors. All patients had either Mayo type IIA fractures (displaced noncomminuted transverse fractures) or needed olecranon osteotomy to address a fracture of the distal humerus. All patients underwent the procedure and the post-treatment protocol as described above.
RESULTS
Our case series consisted of 14 olecranon fractures (Mayo type IIA) and eight patients who underwent olecranon osteotomy fixation. The mean age of the patients was 54.4 years (range 14 years to 82 years).
All patients were allowed to mobilise the elbow 1 week postoperatively except one. This patient had extremely soft bone as a result of long-term steroid treatment for rheumatoid arthritis. Because of the soft nature of the bone, the patient was immobilised in a plaster for a further2 weeks prior to starting active mobilization.
The mean time to union was 6.4 weeks (range 5 weeks to 9 weeks). All except two cases achieved anatomic reduction without distraction at the fracture site. The first case was the patient with rheumatoid arthritis mentioned above whose anchors pulled out as a result of poor bone quality. This resulted in distraction at the fracture site and a fibrous non-union. However, the patient remained asymptomatic and no further surgical action was required. The second patient was a wheelchair ambulatory. They had started active elbow extension immediately postoperatively because it was needed for transferring into and out of their wheelchair. This patient also had some distraction at the fracture site and took 9 weeks to achieve union.
All patients returned to their pre-injury level of activity. At a mean follow-up of 14.2 months (range 7 months to 24 months), no patient had required further surgery or had any problems with the hardware. Figures 2 –4 demonstrate cases from this series.

Pre-operative and postoperative X-rays of olecranon fracture in an elderly lady (age 67 years) treated with suture anchors that united uneventfully.

Pre-operative and postoperative X-rays of olecranon fracture in an elderly lady (age 74 years) treated with suture anchors that united uneventfully.

Pre-operative and postoperative X-rays of a skeletally immature patient (age 14 years) that healed uneventfully.
DISCUSSION
We consider that this novel technique offers numerous advantages over traditional tension band wiring, screw fixation, plate fixation or intramedullary locking nails of olecranon fractures/osteotomies. First, there is no significant metalwork used, which eliminates the complications associated with metalwork and subsequent re-operation rates to remove it. There are no permanent K-wires present, which could allow the penetration of anterior structures, and it also avoids the need for peri-operative radiographs. The technique can be used efficiently and quickly, which reduces operating time.
Furthermore, it can be used successfully in children because it avoids crossing the physis with any hardware. One case in our series was a 14-year-old patient with a physeal fracture.
If failure is defined as loss of reduction of the initial fracture fixation, then we have a 9% (n = 2) failure rate. Failure defined by non-union was only 4.5% (n = 1). Failure of the tension suture technique occurred in one patient whose anchors pulled out (the same case as the non-union). This gives a technical failure rate of 4.5%, although this patient did well with no further surgical intervention. Because the success of bone anchors rely on their hold into cancellous bone, this technique should be relatively contraindicated in patients where bone quality is extremely poor, such as significant osteoporosis.
Failure defined by the need for re-operation to remove problematic metalwork was 0%
Patient compliance is also important with respect to avoiding strenuous activity using the triceps for at least 6 weeks. Therefore, a patient who relies heavily on using their triceps to transfer is likely to exceed the normal physiological loads recommended during the early healing period. It would be fair to suggest that these two patients would have presented a challenge to any given technique.
It should be noted that we have only employed this technique for olecranon osteotomies or Mayo type IIA fractures (displaced, noncomminuted transverse olecranon fractures). Our technique relies on the tension band theory and therefore any fracture that demonstrates comminution or is significantly oblique is unlikely to be able to transfer or withstand the compressive forces applied from the tensile side and should therefore be plated.
Several studies have investigated the biomechanical strengths of different tension band wire materials and constructs [12,13]. Carofino et al. investigated the biomechanical strength of ultra high tensile suture material (FiberWire; Arthrex, Naples, FL, USA) against 18-gauge metal wire in a tension band construct [12]. They biomechanically tested four fixation methods: (1) 2 K-wires with an 18-gauge metal wire tension band; (2) K-wires with a FiberWire tension band; (3) an intramedullary screw with an 18-gauge metal wire tension band; and (4) an intramedullary screw with a FiberWire tension band. They concluded that the biomechanical strength of high tensile suture material in tension band techniques is equivalent to 18-gauge metal wire. In the present study, we utilized Orthocord rather than FiberWire for the ultra high tensile suture. The knot breaking strength of the two suture materials are similar (Orthocord 29.6 lbs; Fiberwire 28.5 lbs). There is no direct comparison of Orthocord to 18-gauge metal wire, although we consider that Orthocord would behave in a similar way to FiberWire becauese of their similar strength characteristics.
There are also economic implications. The cost of two anchors is approximately £300 compared to the £26 needed for hardware in the traditional K-wiring method. However, this initial cost is somewhat offset by the cost of re-operation to remove the metalwork used in traditional techniques, which has caused complications. Reviews suggest that between 40% and 80% of tension band wire cases will need a second operation [3,10]. Furthermore, there is a significant additional morbidity associated with a second operation to take into consideration. To date, our short-term results have a zero re-operation rate at 24 months, which surpasses the rates given for traditional techniques.
Longer follow-up will no doubt demonstrate whether there are complications to be taken into account associated with the hardware, although, given that the anchors are deeply buried, we feel this to be extremely unlikely. Complications of the fracture are likely to be independent of the technique used for fixation.
We appreciate that our case numbers are small, the follow-up is short, and that there is an associated learning curve for performing the technique. However, our early data for this technique appear to offer short-term results that, at the very least, are equivalent to the other techniques described, and possibly superior in view of the zero re-operation rate to date. We propose that this initial data should be used to formulate the basis of a randomized controlled trial for comparing tension band wiring and tension band suturing in the fixation of simple transverse olecranon fractures.