
Abstract
Background
There are limited data available on the outcome of patients following isolated fractures of the greater tuberosity of the humerus. In this retrospective study, we looked at how differences with respect to the injury and subsequent management affected patient outcomes.
Methods
Forty-eight (28 men and 20 women) patients (mean age 45 years) who were treated at our institution between 1999 and 2009 matched our inclusion criteria. Thirty-five patients were treated surgically and 13 were managed conservatively. Functional outcome was assessed after a mean follow-up of 5.5 years using the Oxford Shoulder Score (OSS), the University of California and Los Angeles (UCLA) rating scale and the shoulder index of the American Shoulder and Elbow Surgeons (ASES).
Results
Post-fixation displacement of the greater tuberosity fragment of < 5 mm led to a significantly better outcome than displacement > 5 mm (OSS = 43 versus 37; ASES = 25.6 versus 17.7; UCLA 28.2 versus 21.3). Patients who had surgery > 2 weeks after the initial injury had a significantly worse outcome than those who had surgery in < 2 weeks (OSS = 37.4 versus 44.7; ASES = 18.9 versus 27.2). Patients with shoulder dislocation had worse outcome than those with no dislocation (OSS = 40.6 versus 44; ASES 22.9 versus 26) and rotator cuff tears were also associated with worse outcome scores than those without (OSS 42.8 versus 36.8; ASES 24.5 versus 20.5), although neither of these variables proved statistically significant.
Conclusions
Isolated fractures of the greater tuberosity have a worse outcome if there is a delay in surgical fixation of > 2 weeks and post-fixation displacement of > 5 mm.
Introduction
Fractures of the greater tuberosity account for 15% to 40% of all fractures of the proximal humerus [1]– [3]. However, in contrast to other fractures in this region, they are seen most commonly in healthy middle-aged patients [1]. They may occur as a result of two mechanisms of injury, which may be impaction or avulsion [1], [4]. Impaction fractures occur when the greater tuberosity is forced against the acromion or superior glenoid and are usually comminuted. Avulsion injuries occur when the proximal humerus is forced anteriorly, as occurs in anterior glenohumeral dislocation. There is no formal classification system for isolated fractures of the greater tuberosity. The Neer or the AO/ASIF (Association for Osteosynthesis/Association for the Study of Internal Fixation) classifications are most commonly used for fractures of the proximal humerus, although they are unsatisfactory because many fractures do not fit neatly with either system [1].
As a result, the degree of fragment displacement is most commonly used to decide on whether patients should have surgical or conservative management. It is generally accepted that, if the displacement of the greater tuberosity is < 5 mm, then conservative management is the correct option, although it has been suggested that < 3 mm should be the cut-off for certain patient groups [5], [6].
There is a limited pool of data regarding the outcome of patients with isolated fractures of their greater tuberosity, with most series concentrating on the degree of displacement that warrants surgical intervention [2]. The present study aimed to investigate other factors that may influence patient outcomes, including the fracture pattern, the presence of associated injuries and the time delay between injury and surgery.
Materials and Methods
All patients treated at Waikato Hospital, New Zealand, for isolated fracture of their greater tuberosity between January 1999 and January 2009 were identified. Patients were included in the analysis if they had an isolated fracture of their greater tuberosity and no previous fractures in the same arm, were alive at the time of data collection, had radiographs available for review, and at least 12 months had passed since the injury. From a total of 144 patients, 39 patients were excluded because they sustained other injuries, 17 patients had died, 11 patients had moved abroad, 10 patients had no radiographs available, 10 patients did not respond to the invitation to take part in the study and nine patients had a history of other injuries in the ipsilateral shoulder. A total of 48 patients therefore met the inclusion criteria.
The radiographs [which were anteroposterior (AP) and lateral shoulder views] at time of presentation of all eligible patients were anonymized and reviewed by the senior author: TH) and classified as simple (single fragment) or comminuted (multiple fragments) (Figs 1 and 2).
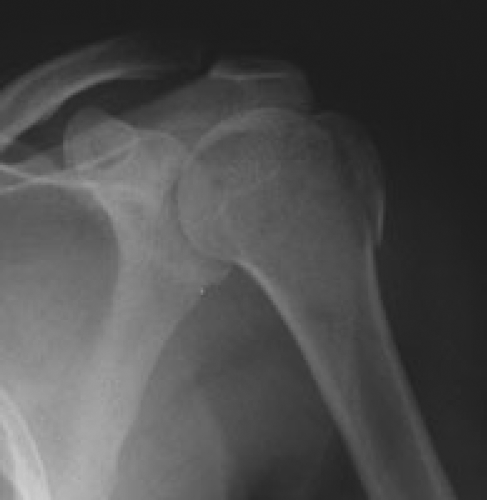
Radiograph showing non comminuted single fragment fracture of the greater tuberosity.
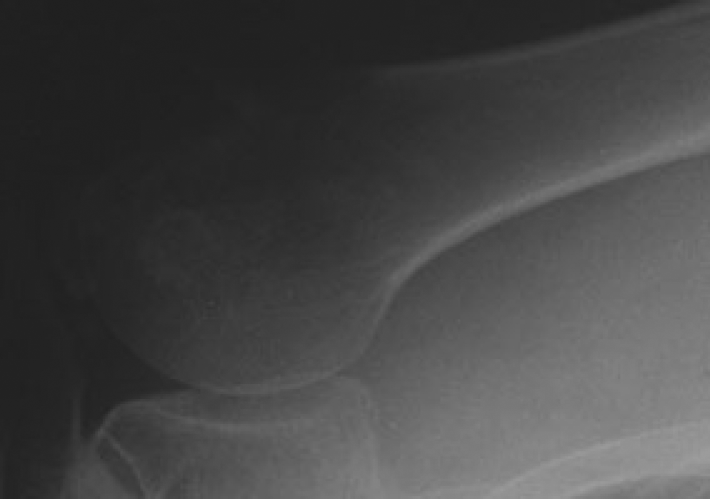
Radiograph showing comminuted fracture of greater tuberosity.
The patients who were managed conservatively all had a fracture with minimal (< 5 mm) displacement of the fragment. They were kept in a collar and cuff sling for 6 weeks and started pendular exercises after 2 weeks and, at 6 weeks, progressed from passive to active range of movement under the guidance of the physiotherapist. Radiographs were taken after 2 weeks and, if there was evidence of further fragment displacement, then they were offered surgery (four patients), radiographs were repeated again at 6 weeks and at the final follow-up appointment.
The surgical approach was a transdeltoid lateral approach in all patients. The methods of surgical fixation included tension band wiring alone (seven patients) or with screws (19 patients) and other methods such as T-plate fixation (one patient) (Figs 3– 5). Rotator cuff repair was performed if required following intraoperative assessment of the rotator cuff (eight patients). Postoperative rehabilitation was the same as described for the conservative group.
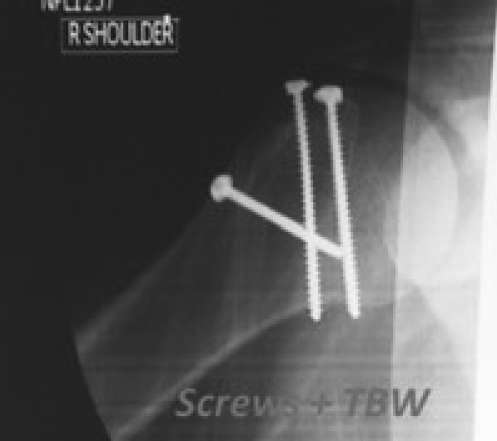
Postoperative radiograph showing tension band wiring and screw fixation of greater tuberosity fracture. TBW, Tension band wiring.

Radiograph showing rotator cuff repair (RCR) and tension band wiring (TBW).
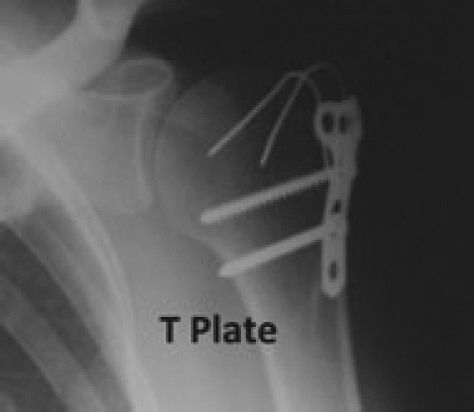
Radiograph showing T-plate fixation of greater tuberosity fracture.
Postoperative radiographs were taken at the 2-week follow-up appointment after surgery and were reviewed blindly by the senior author. The amount of residual fragment displacement defined as the point at which there was maximum separation between the fragment and the humerus on the AP radiograph was recorded.
Outcome measures used were the Oxford Shoulder Score (OSS), the American Shoulder and Elbow Surgeons (ASES) shoulder score and University of California and Los Angeles (UCLA) shoulder rating scale. The amount of time taken off work and time on Accident Compensation Corporation (ACC) support were also analyzed. Patients were invited to attend an outpatient clinic for review or if unable to attend were interviewed by telephone.
Statistical analysis
We used an unpaired t-test to compare the clinical outcomes of the two different groups of patients for each variable where the data was parametric and the Mann – Whitney U-test where the data was nonparametric.
Results
Demographics
A total of 48 eligible patients were identified. Twenty-eight male and 20 female patients with a mean age of 45 years (range 16 years to 81 years) were therefore included in the analysis. The mean time elapsed from injury to completion of the questionnaire was 5.5 years.
The mechanism of injury was a direct fall on the shoulder in 35 patients, motor vehicle accident (direct hit) in nine patients and a fall on the outstretched hand in four patients. Thirty-seven out of 48 patients had associated shoulder dislocation.
Surgical complications
Thirty-five of the 48 patients were treated with surgery. The mean age of this group was 51 years. Twenty-one patients were classified as having a simple fracture, with the others being classified as comminuted.
Postoperative complications included stiffness and a reduced range of movement in seven patients, axillary nerve palsy in four patients (three had nerve palsy pre-operatively) and pain in five patients. Three patients required a second operation; one patient for stiffness and a reduced range of movement, as well as one patient who had a rotator cuff tear and an axillary nerve palsy pre-operatively and who suffered pain and impingement syndrome postoperatively and required a sub-acromial decompression. The third patient was an 80-year-old female patient with a comminuted fracture who underwent rotator cuff repair and tension band wiring. The fixation failed and she required an inverse shoulder replacement 10 months later but continued to have pain in her trapezius and required further surgery with bone grafting of an insufficiency fracture in the left acromion.
The median time that patients were followed up in clinic after surgery was 161 days compared to 69 days for patients who were managed conservatively (p = 0.01). In the surgical group, patients who had a comminuted fracture were followed up for a median of 204 days compared to 135.5 days for patients who had a simple fracture (p = 0.13).
Thirteen patients with a mean age of 42 years were managed conservatively, 10 of the patients had associated dislocation. Two patients experienced long term problems with stiffness and reduced range of movement and one patient experienced impingement syndrome.
Outcome measures
Surgical versus conservative.
The mean ASES and OSS were better in the conservative group compared to the surgical groups, respectively, although this difference did not reach statistical significance (Table 1). The median number of weeks taken off work was 18 weeks for the surgery group versus 11.5 weeks for the conservative group (p = 0.19) and the median time on ACC was 24 weeks for the surgery group versus 23 weeks for the patients who were managed conservatively (p= 0.9). There was also no difference observed between patients who had different methods of fixation.
Surgical versus conservative treatments
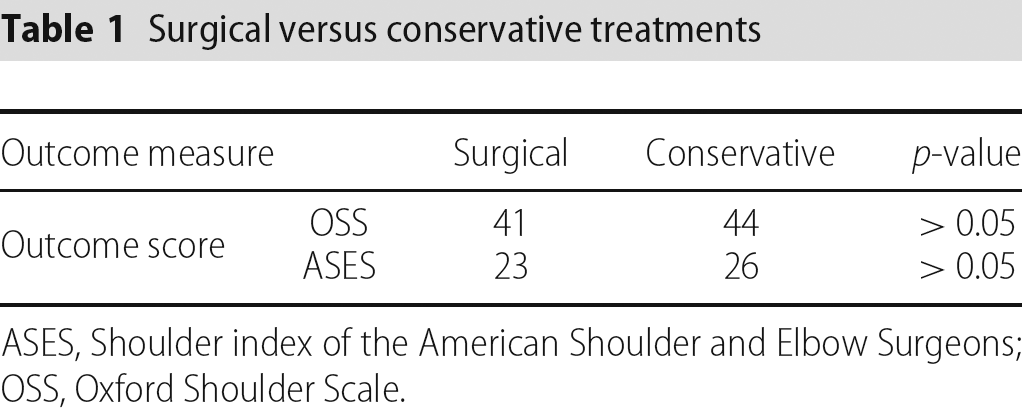
ASES, Shoulder index of the American Shoulder and Elbow Surgeons; OSS, Oxford Shoulder Scale.
Effect of dislocation on surgical outcome.
In the patients who were treated surgically, 27 of the 35 patients had associated dislocation. These patients had worse outcome scores than patients with no associated dislocation (Table 2), although the differences were not statistically significant. There was no significant difference in the time taken off work between the two groups (p = 0.49).
Association versus no association with dislocation
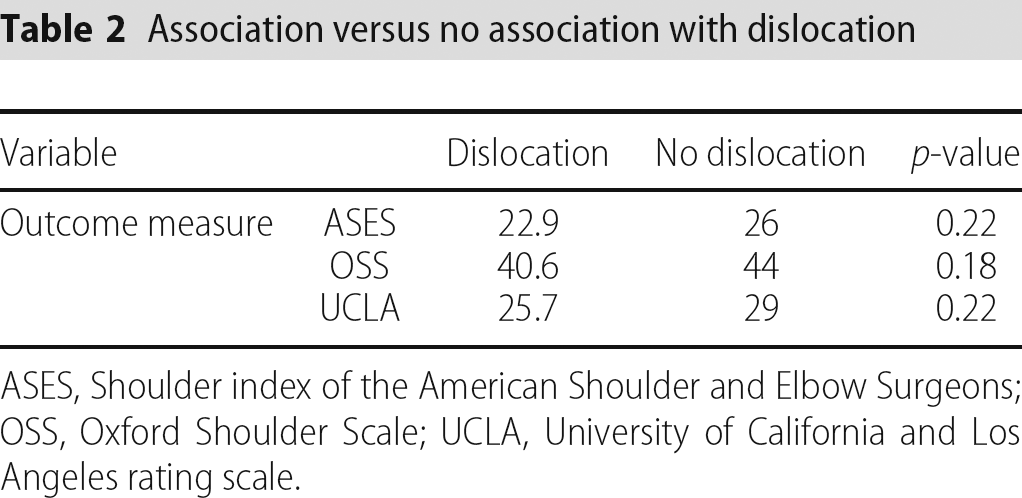
ASES, Shoulder index of the American Shoulder and Elbow Surgeons; OSS, Oxford Shoulder Scale; UCLA, University of California and Los Angeles rating scale.
Effect of rotator cuff tear on surgical outcome.
The eight patients in the surgical group who sustained associated rotator cuff tears did worse than those who did not require rotator cuff repair, with all mean outcome scores being lower, although the difference was not statistically significant (Table 3). There was no difference in the time taken off work or on ACC.
Association versus no association with rotator cuff tear
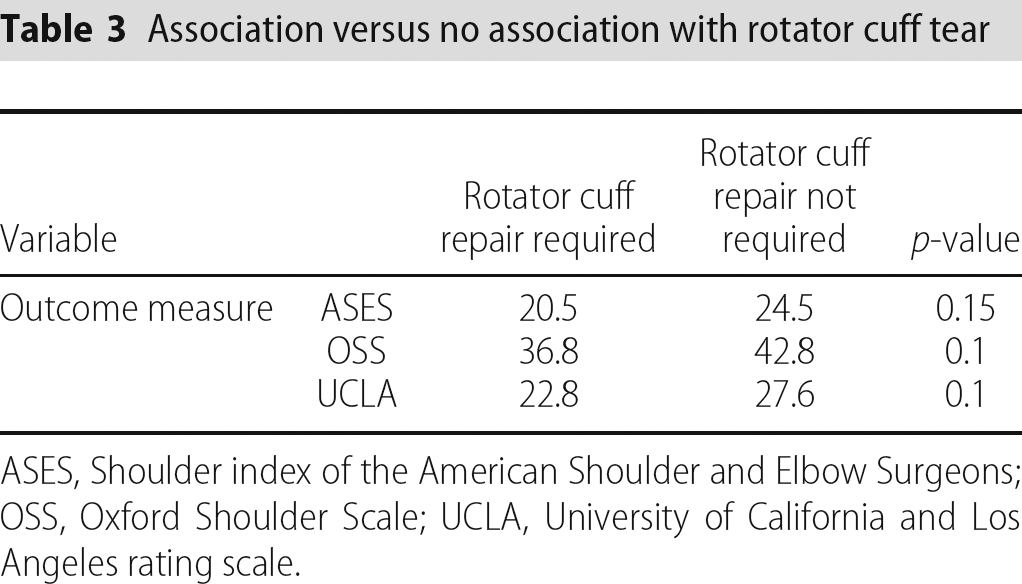
ASES, Shoulder index of the American Shoulder and Elbow Surgeons; OSS, Oxford Shoulder Scale; UCLA, University of California and Los Angeles rating scale.
Postoperative fragment displacement.
Postoperative displacement of the greater tuberosity was measured and a significant difference in all outcome scores was noted between patients who had over 5 mm of displacement compared to those who had < 5mm of displacement (Table 4). The median time taken off work in patients with > 5 mm of displacement postoperatively was 27 weeks versus 18 weeks for those with < 5 mm displacement (p = 0.15).
Displacement of greater tuberosity fragment
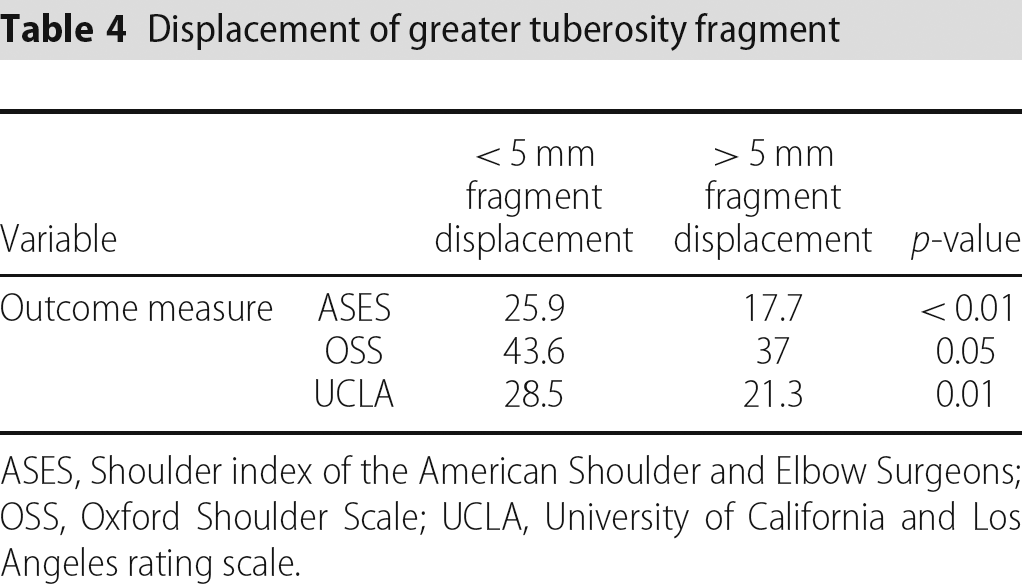
ASES, Shoulder index of the American Shoulder and Elbow Surgeons; OSS, Oxford Shoulder Scale; UCLA, University of California and Los Angeles rating scale.
Time delay to surgery.
The mean delay between injury and surgery was 16 days. Our results show that the delay does impact on outcome because all mean outcome scores were significantly higher in the patients who were operated on within 2 weeks of their injury compared to those in whom the delay was over 2 weeks (Table 5). The median time taken off work for patients waiting > 2 weeks for surgery was 32.5 versus 16.5 in those who waited < 2 weeks (p= 0.08).
Delay in surgical treatment
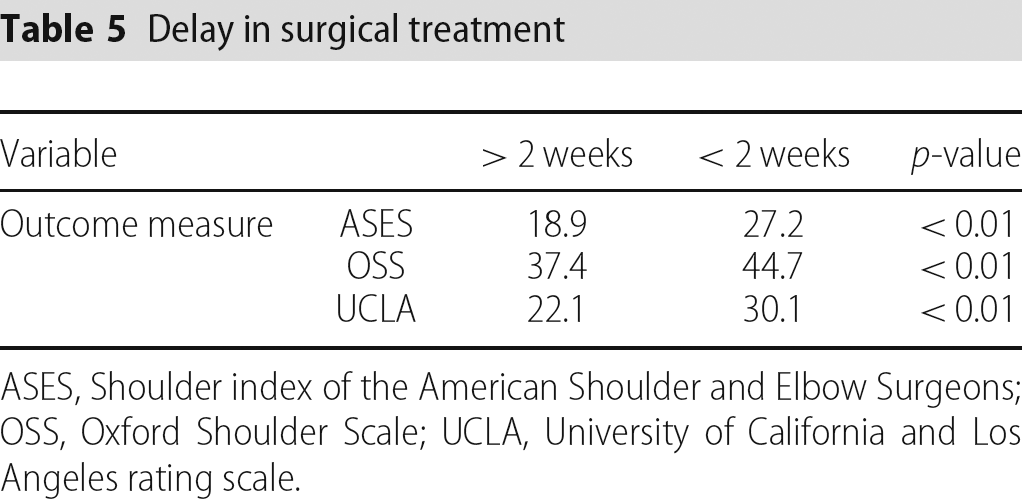
ASES, Shoulder index of the American Shoulder and Elbow Surgeons; OSS, Oxford Shoulder Scale; UCLA, University of California and Los Angeles rating scale.
Effect of fracture pattern.
Twenty-one surgical patients sustained a simple fracture and 14 patients sustained a comminuted fracture. The mean ASES, UCLA and OSS for patients with simple versus comminuted fractures are shown in Table 6. There was no significant difference between them. The median number of weeks taken off work was 18 in both groups and the time on ACC was equivalent in each group.
Simple vs comminuted greater tuberosity fragment
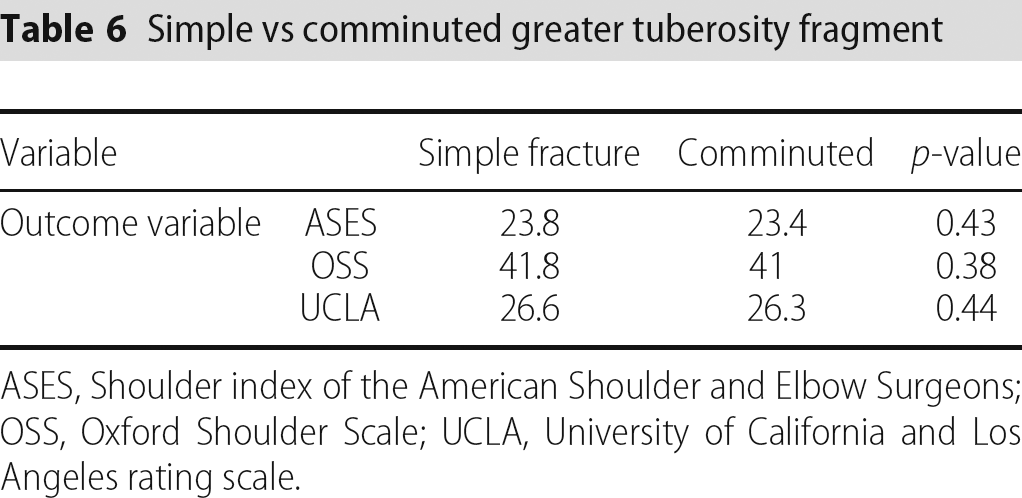
ASES, Shoulder index of the American Shoulder and Elbow Surgeons; OSS, Oxford Shoulder Scale; UCLA, University of California and Los Angeles rating scale.
Discussion
This is a retrospective study and therefore does have the shortcomings associated with that study type. We acknowledge that our follow-up rate is rather low; however, the reasons for patient exclusion are clearly documented. Isolated greater tuberosity fracture is not a common injury and the number of patients included in this series is higher than in many similar series.
Our patient population reflects what is known about greater tuberosity fractures, namely that they occur in a younger population relative to other fracture types of the proximal humerus. Because they will be of working age, it is extremely important that their ability to resume their employment is not hampered by in appropriate management of their fracture.
The surgical complications reported in the present study are in keeping with the published literature. Flatow et al. reported pain in 50% of patients who underwent surgery [7]. In this series, postoperative axillary nerve palsy occurred in one out of 35 surgical patients. Nerve injuries are reported to occur in approximately one-third of greater tuberosity fracture-dislocations, with the majority of cases recovering after a few months, suggesting that they are mainly neurapraxias or low grade axonotmesis [8], [9]. This complication is rare after surgery and was reported in just one of 12 patients in the series reported by Flatow et al. [7] and no patients in the series reported by Resch et al. [10]. The axillary nerve crosses the underside of the deltoid muscle and it can lie in the line of approach for inserting screws to fix fractures of the greater tuberosity. It can also be damaged if a suture is not placed once the deltoid has been split to stop the split inadvertently extending. Other methods to avoid axillary nerve damage have been recommended and include placing the screws at a slightly anterolateral angle with the arm held in internal rotation, using screws without a washer to avoid trapping the nerve under the washer, or using the trocar sheath to push the axillary nerve out of the way [10].
Although fractures that were managed conservatively showed a tendency for better outcome scores than the operative group, there was no significant difference between them suggesting the widely accepted use of 5 mm as the cut-off for surgical intervention is satisfactory. This is not in keeping with all of the published results, with Platzer et al. reporting a better outcome in patients treated operatively compared to those managed conservatively [11]. Stiffness is a frequently reported complication and can occur if passive exercises are delayed. Impingement syndrome occurs if the fragment becomes more displaced and requires surgical intervention.
This is the first study to investigate whether the fracture pattern affects surgical outcome and there is no evidence in this series that it does, although the power of the study to detect a difference was only 65%, with twice the number of patients that would have been required to reach a power of 80% to detect a difference. The patients who sustained a comminuted fracture were followed up in clinic for longer but returned to work sooner than those with simple fractures. This apparent discrepancy is likely to simply reflect the belief held by the doctor that these patients have a worse outcome and therefore should be followed up for longer, which is not borne out by the the results of the present study.
A delay in the surgery of more than 2 weeks did make a significant difference to surgical outcome in this series. It was standard practice in our institution for patients with an isolated fracture of their greater tuberosity to be sent home from the emergency department with a review in the fracture clinic booked for the following week. This explains why the mean time from injury to surgery is 16 days in the present study. The delay between injury and surgical fixation has not been reported in other surgical series. The reason for the poorer outcome is not clear. It may be a result of the formation of scar tissue making the surgery technically more challenging.
Patients who sustained a fracture dislocation had a tendency towards worse outcome scores than those who sustained an isolated greater tuberosity fracture, although the difference was not statistically significant. The rate of the incidence of glenohumeral dislocation was higher in this series than the rate of 10% to 30% reported in the literature [4], [9]. The incidence of neurological injury is higher in fractures associated with shoulder dislocation.
Patients who sustained rotator cuff tears also had worse outcome scores overall in this series but, again, these did not reach statistical significance. There was no attempt made to establish the status of the rotator cuff before surgery using arthroscopy or imaging. Partial thickness articular sided rotator cuff tears are frequently associated with isolated greater tuberosity fractures and are not necessarily obvious at the time of injury [12]. Gallo et al. reported an increasing severity of rotator cuff injury associated with an increased displacement of the greater tuberosity fragment (> 5 mm) [13].
This series supports the view that patients with displacement of < 5 mm of the greater tuberosity fragment do better than those with more displacement, and this rule also applies in the postoperative setting. Repeat surgical intervention was not considered because the postoperative radiographs were taken 2 weeks after surgery.
Conclusions
A delay of more than 2 weeks from initial injury to surgery and postoperative fragment displacement > 5mm are negative prognostic factors with respect to greater tuberosity fractures. Further studies with greater power are required to determine whether there is statistical difference in the results obtained regarding comminuted and noncomminuted isolated greater tuberosity fractures.
Footnotes
Conflicts of Interest
None declared
Acknowledgements
Dr Joanna Lynch is thanked for her advice regarding the preparation of the manuscript.