
Abstract
Objectives:
To investigate the effect of acupuncture at PC6 on cardiac hypertrophy in isoproterenol (ISO)-treated mice.
Methods:
48 male C57BL/6 mice underwent subcutaneous injection of ISO for 14 days and were randomly divided into four groups (n=12 each) that remained untreated (ISO group), received verum manual acupuncture (MA) treatment at PC6 (ISO+MA(PC6) group), sham MA at location on the tail not corresponding to any traditional acupuncture point (ISO+MA(tail) group), or propranolol (ISO+PR group). An additional 12 mice were given an injection of phosphate-buffered saline (PBS) and formed a healthy control (Normal) group. After performing echocardiography and measuring the ratio of heart weight (HW)/tibia length (TL) at 14 days, all mice were euthanased. Morphological examination was performed following haematoxylin and eosin and Masson’s staining of heart tissues. Ultrastructural changes were observed by electron microscopy. Cardiac protein expression of atrial natriuretic peptide (ANP) and tumour necrosis factor α (TNFα) were measured by immunohistochemical (IHC) staining and Western blotting.
Results:
Compared with the untreated model group, acupuncture at PC6 lowered the heart rate, reduced the ratio of HW/TL, improved the left ventricular (LV) anterior wall thickness (LVAWd), LV end-diastolic anterior wall thickness (LVAWs), LV end-systolic posterior wall thickness (LVPWd), LV end-diastolic posterior wall thickness (LVPWs), and fractional shortening (FS) as observed by echocardiography (ISO+MA(PC6) vs. ISO groups: P<0.05). Moreover, evidence from morphological studies demonstrated that acupuncture at PC6 inhibited myocardial hypertrophy and collagen deposition, and normalised the ultrastructural changes. In addition, ANP and TNFα expression were attenuated in the verum acupuncture group compared with the untreated model group (ISO+MA(PC6) vs. ISO groups: P<0.05).
Conclusions:
The results demonstrated that acupuncture at PC6 attenuates sympathetic overactivity. Additionally, it may improve cardiac performance by reversing adverse cardiac remodelling. Acupuncture has potential as a treatment for sympathetic hypertension.
Introduction
Cardiac hypertrophy is thought to be an adaptive response to haemodynamic stress that develops from elevated afterload, loss of contractile mass from a prior myocardial infarction, or mutated contractile proteins. It is the common pathological progression in many forms of cardiac disease, including ischaemic heart disease, hypertension, heart failure and valvular heart disease. Although it is believed to have a compensatory function to maintain cardiac performance and oxygen consumption within their normal ranges,1,2 echocardiographically demonstrated cardiac hypertrophy is an independent risk factor for cardiovascular mortality, with significantly increased risk of heart failure and sudden death stemming from malignant arrhythmia. 3
It is now widely accepted that sympathetic activation leads to cardiac overload, which is mediated through release of epinephrine and norepinephrine. When cardiac β-adrenergic receptors are activated in the heart, cardiac output and blood pressure increase accordingly to maintain peripheral perfusion. Moreover, excessive sympathetic activity and the withdrawal of vagal activity clearly contribute to the progression of ventricular remodelling and worsen heart failure. Therefore, β-blockers acting to reduce sympathetic hyperactivity are used as the first-line therapy in heart failure, and function by blocking activation of the β-receptor and alleviating the adverse cardiac remodelling. 4 Inhibition of sympathetic hyperactivity might be a rational therapeutic approach to reduce ongoing cardiac damage.
Acupuncture, a traditional Chinese treatment modality, is increasingly familiar to Western medicine. 5 It is well documented that acupuncture has been used empirically for centuries to treat symptoms related to cardiovascular diseases, such as angina, hypertension and myocardial hypertrophy, by enhancing vagal activity and suppressing sympathetic activity.6–8 The mechanism of acupuncture in cardiovascular disease has been extensively investigated. Torres-Rosas et al. and Eshkevari et al. reported that electroacupuncture (EA) at ST36 could stimulate vagal outflow and prevent the activation of sympathetic pathways, respectively.9,10 Li et al. demonstrated that EA at PC6 (Neiguan) is effective at lowering blood pressure in spontaneously hypertensive rats (SHRs). 11 It was also reported that EA at LR3 could reduce cardiac apoptosis in male SHRs. 12 However, it remains unknown whether acupuncture can prevent adverse cardiac remodelling and ameliorate cardiac performance following sympathetic overactivity.
We hypothesised that acupuncture would act on sympathetic outflow to improve cardiac performance by inhibiting β-adrenergic mediated adverse cardiac remodelling, such as cardiac hypertrophy and fibrin deposition. It has been reported that acupuncture at PC6 produces a slower heart rate than acupuncture at ST36, and needling at PC6 is generally thought to be more relevant to cardiovascular diseases in traditional clinical applications. Accordingly, in this study, we investigated the effect of acupuncture at PC6 on excessive sympathetic activity induced by the β-receptor agonist isoproterenol (ISO) in mice.
Methods
Animal model
Sixty male C57BL/6J mice (initial body weight ~25 g) were provided by the Department of Experimental Animal Sciences Centre, Heilongjiang University of Chinese Medicine. The mice were kept under a 12/12h light/dark cycle in a temperature-controlled (22°C) room and were given standard mouse chow and water ad libitum throughout the experiment. To induce cardiac hypertrophy, the mice were treated with subcutaneous injections of ISO, which has been used widely for such modelling purposes, for 14 consecutive days at a dose of 25 mg/kg/day. 13 All animal procedures were conducted in strict accordance with international ethical guidelines and the National Institutes of Health Guide for the Care and Use of Laboratory Animals, and were approved by the Animal Care and Use Committee of Heilongjiang University of Chinese Medicine.
Acupuncture methods and grouping
PC6 is located 3 mm lateral and distal to the wrist joint and between the radius and ulna in the forelimb. For acupuncture stimulation, a stainless steel needle (0.17 mm diameter, 7 mm length) was vertically inserted at PC6 to a depth of 2 mm, and retained for 30 min in the anaesthetised mouse. 14 Male mice were randomised into the following groups: (1) healthy control group (Normal, n=12)—injected with saline for 14 days and received no further pharmacological or acupuncture treatment; (2) untreated model group (ISO, n=12)—injected with ISO for 14 days and received no acupuncture treatment; (3) verum acupuncture-treated model group (ISO+MA(PC6), n=12)—received 30 min manual acupuncture (MA) treatment at PC6 followed by ISO administration once a day; (4) propranolol-treated model group (ISO+PR, n=12)— received oral treatment of 10 mg/kg propranolol once a day, followed by injection of ISO for 14 days; (5) sham acupuncture-treated model group (ISO+MA(tail), n=12)—received 30 min acupuncture treatment at a location on the tail (not corresponding to any traditional acupuncture point) once a day, followed by injection of ISO for 14 days.
ECG and echocardiography
All mice were anaesthetised with a mixture of ketamine (70 mg/kg) and xylazine (14 mg/kg) in solution. Electro-cardiogram (ECG; lead II) recordings were immediately performed after the injection of ISO and the heart rate was quantified on day 7. The electrodes were placed under the skin to record the conventional bipolar limb leads (II). In order to avoid errors in the position of the leads, the electrodes were always placed by the same person. The ECG was captured using a three-channel digital ECG recorder with a paper speed of 50 mm/s and sensitivity of 0.5 mV/cm. 14
After 2 weeks of treatment, the chest hair of the anaesthetised mice was shaved, and then echocardiograms were performed using a 30 MHz ultrasound system (VisualSonics Vevo2100). Two-dimensionally guided left ventricular (LV) M-mode images were recorded on the parasternal short axis at the papillary muscle level, and the maximal parasternal long-axis of the LV B-mode images was obtained. LV anterior wall thickness (LVAWd), LV end-diastolic anterior wall thickness (LVAWs), LV end-systolic posterior wall thickness (LVPWd) and LV end-diastolic posterior wall thickness (LVPWs) were measured from the M-mode images. Ejection fraction (EF, %) and fractional shortening (FS) of the left ventricle were calculated.
Euthanasia
At the end of the experiment, euthanasia was performed by appropriately trained personnel approved on the animal protocol. The mice were put into a commercial dessicator jar that included inlet/outlet ports that could be connected to a compressed carbon dioxide (CO2) gas cylinder. The flow of CO2 was adjusted to achieve a rate that displaced 20% of the chamber volume per minute, for at least 1 min after respiratory arrest. After the gas was turned off, mice were observed until all muscle activity and signs of life had been absent for at least 30 s, then cervical dislocation was performed to confirm death.
Morphological studies
For haematoxylin and eosin (H&E) staining, whole hearts (n=3 per group) were immediately fixed with 10% formalin after dissection, maintained at room temperature for 24 hours, dehydrated in an ethanol series, and paraffin embedded. Cross sectioned tissues (5 µm thickness) were deparaffinised in a xylene-ethanol series and dehydrated in an ethanol-xylene series. The sections were then stained with H&E, after which they were washed in deionised water, dehydrated via ethanol, cleared in xylene and then mounted onto slides. Each slide was examined by light microscopy. After deparaffination and dehydration, the sections were subjected to Masson’s trichrome staining to evaluate myocardial fibrosis. Myocardial cells were stained red and collagenous fibres stained blue.
Immunofluorescence staining
Immunofluorescence staining was carried out as described in the instruction manual of ABCAM. Briefly, after 2 weeks’ acupuncture treatment, hearts (n=3 per group) were removed, and then cryosections were prepared for further immunolabelling studies. 15 Rabbit polyclonal primary antibodies to atrial natriuretic peptide (ANP) and tumour necrosis factor α (TNFα) were used for immunofluorescence staining. The cryosections were incubated with these specific primary antibodies overnight at 4°C followed by fluorescence-labelled secondary antibodies for 1 hour at room temperature. Alexa Fluor 633–labelled phalloidin was used for F-actin, and DAPI was used for nuclear staining. The images were photographed using a laser confocal microscope (Leica, Germany) and digitised at 20x.
Protein extraction and Western blot analysis
Hearts (n=3 per group) were removed after 2 weeks’ acupuncture treatment, and the left ventricle was isolated. Tissues were sonicated in lysis buffer containing phosphatase and protease inhibitors and the protein content was quantified following the instructions of the manufacturer. SDS-PAGE was performed on Gradient NuPAGE 12% Bis-Tris gels. After samples had been transferred onto nitrocellulose membranes, the membranes were stained with Red Alert Western blot stain to ensure equal loading of lanes. According to the immunofluorescence staining, Western blot analysis was performed to quantify expression of proteins of interest; rabbit polyclonal antibodies to ANP (1:400) and TNFα (1:400) were used. The membranes were incubated with specific primary antibodies overnight at 4°C followed by fluorescence-labelled secondary antibodies for 1 hour at room temperature. Subsequently, immunoreactive proteins were detected using a Molecular Imager VersaDoc MP 5000 System (Bio-Rad) and analysed using a Odyssey Infrared Imaging System.
Ultrastructural analysis
After dissection, left ventricles (n=3 per group) were fixed in cold 2,5-glutaraldehyde in 0.1 M/L cacodylate buffer (pH 7.3), postfixed in 1% osmium tetroxide (OsO4), dehydrated, and embedded in Epon. Sections (about 1 µm thick) were stained with toluidine blue and observed by light microscopy in order to select fields. Ultrathin sections were mounted on copper grids, stained with uranyl acetate and lead citrate, and examined under an electron microscope (4200x).
Statistical analysis
All data are presented as mean±SEM. Statistical analysis was done using one-way analysis of variance (ANOVA) with a Tukey post-hoc test using Graph Pad Prism software (version 7.0; GraphPad Software, San Diego, California, USA). A value of P<0.05 was considered to be statistically significant.
Results
Acupuncture at PC6 prevented cardiac hypertrophy in IOS-treated mice
According to the experimental procedure, ISO was administered by subcutaneous injection after the acupuncture and propranolol treatments. The ECG in each group was recorded for 15 min after the ISO infusion on day 7, and the representative ECG diagrams (see Figure 1A for examples) were selected for the analysis of heart rate (Figure 1B). Acupuncture at PC6 significantly inhibited the increase in heart rate induced by ISO infusion. Conversely, acupuncture of the tail (ISO+MA(tail) group) demonstrated no such potential to decrease the heart rate stimulated with the β-adrenergic agonist. After 2 weeks of treatment, hearts were harvested to quantify cardiac hypertrophy, and the ratio of heart weight normalised for tibial length (HW/TL) was calculated. Those mice in the untreated model (ISO) group demonstrated aggravated cardiac hypertrophy, as indicated by the higher HW/TL ratio. Figure 1C shows that acupuncture at PC6 achieved an effect comparable to propranolol in terms of inhibition of cardiac hypertrophy in the ISO-treated mice, and acupuncture of the tail failed to reverse the cardiac hypertrophy.
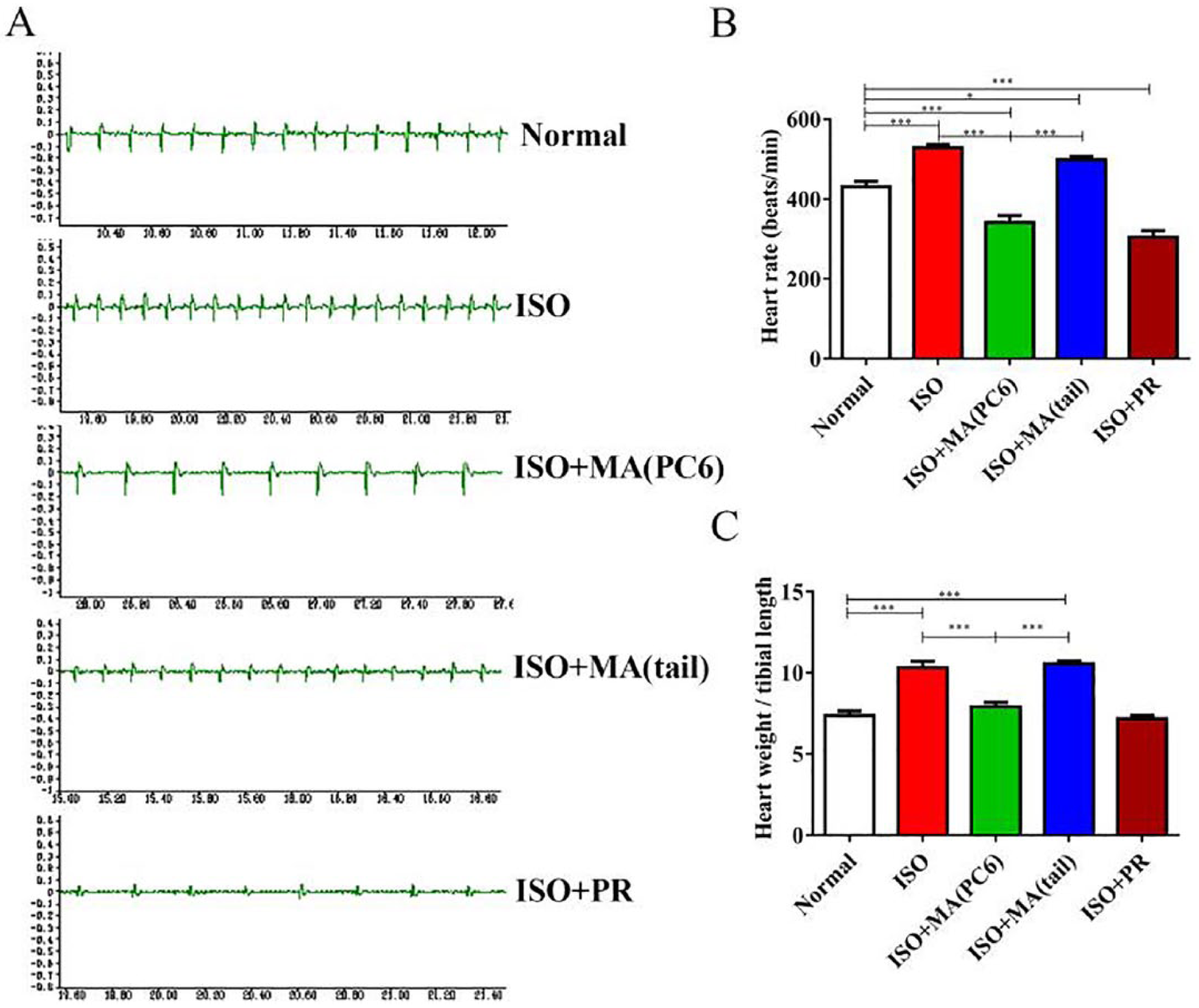
Effects of acupuncture at PC6 on electrocardiogram (ECG) and ratio of heart weight (HW)/tibia length (TL). (A) Representative ECG recordings. (B) Compared with the ISO and ISO+MA(tail) groups, the ISO+MA(PC6) group showed a significantly reduced heart rate equivalent to propranolol-treated mice (ISO+PR group). (C) Acupuncture at PC6 inhibited the increase in relative cardiac mass seen in mice in the untreated model group. Data are presented as mean+SEM; * P<0.05; *** P<0.001. MA, manual acupuncture; ISO, isoproterenol; PR, propranolol.
Acupuncture at PC6 improved cardiac function in IOS-treated mice
To measure cardiac performance, echocardiography was performed at 14 days post-sustained exposure to ISO. Representative echocardiograms are shown in Figure 2A. In accordance with the HW/TL ratios and H&E staining, ISO administration increased LVAWd, LVAWs, LVPWd and LVPWs (Figure 2B), indicating the induction of concentric hypertrophy in this mouse model. We found that the thickness of the LV septum and posterior wall was decreased by acupuncture at PC6 and propranolol treatment for 14 days. However, ISO treatment for 14 days did not cause a reduction in LV EF in the model group, which could be explained by compensatory hypertrophy of the heart. FS (%) is widely used to evaluate LV global systolic function. Loss of FS was prevented in both the verum acupuncture and propranolol treatment groups. Taken together, these observations indicate that acupuncture at PC6 rescued cardiac dysfunction and performance, restoring them to control group levels (Figure 2B).
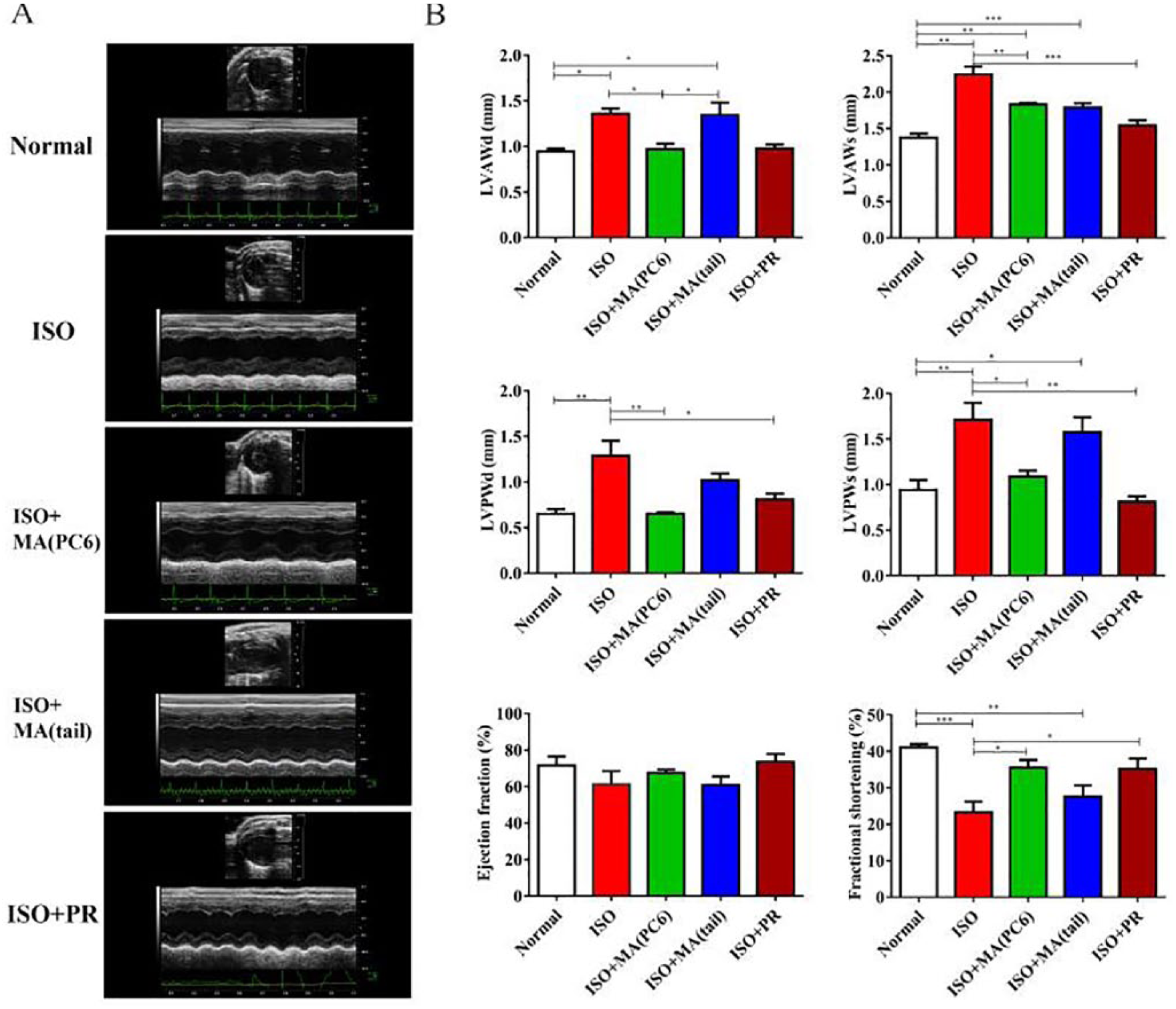
Cardiac performance assessed by echocardiography. (A) Representative echocardiographic images (M-mode) on day 14 from each group. (B) Quantitative measures of cardiac function and hypertrophy. LVAWd, LVAWs, LVPWd and LVPWs were measured, and the EF and FS were calculated. Data are presented as mean+SEM; * P<0.05; ** P<0.01; *** P<0.001. MA, manual acupuncture; EF, ejection fraction; FS, fractional shortening; ISO, isoproterenol; LVAWd, left ventricular (LV) anterior wall thickness; LVAWs, LV end-diastolic anterior wall thickness; LVPWd, LV end-systolic posterior wall thickness; LVPWs, LV end-diastolic posterior wall thickness; PR, propranolol.
Acupuncture at PC6 improved histomorphometry in ISO-treated mice
As shown in Figure 3, H&E staining consistently revealed myocardial hypertrophy and disordered cell arrangement in hearts of the untreated model (ISO) group compared to samples from the PC6 acupuncture and propranolol treatment groups. Heart sections stained with Masson’s trichrome stain revealed that the extent of cardiac fibrosis was significantly reduced in hearts from the PC6 acupuncture group compared with untreated mice after 14 days of ISO treatment. Electron microscopy images of the ISO-treated hearts demonstrated a significantly higher number of cardiomyocytes with disassembled sarcomeres, and an increased number of swollen and/or fused mitochondria, which were partly attenuated by PC6 acupuncture and propranolol treatment.
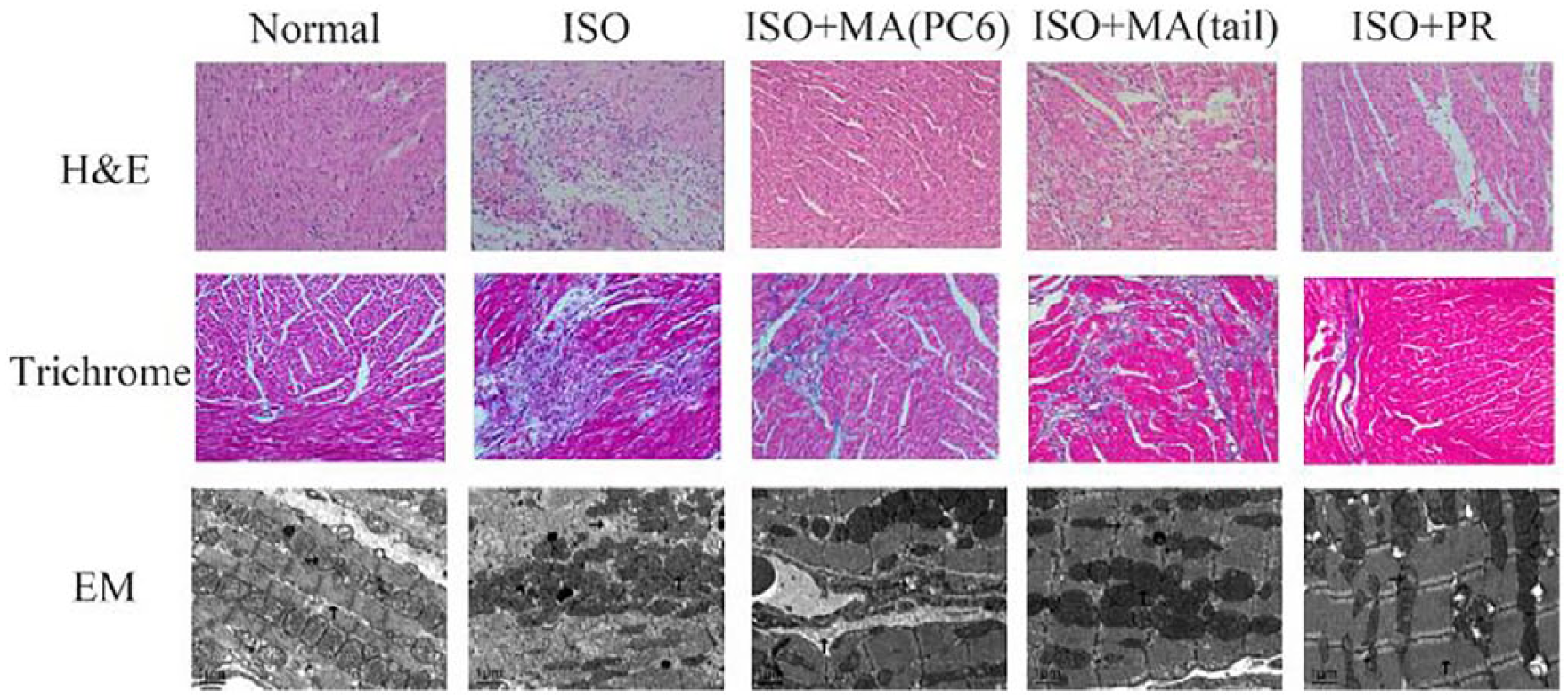
Representative photomicrographs obtained from H&E and Masson’s stained cardiac tissues, indicating that acupuncture at PC6 attenuated myocardial hypertrophy and fibrosis deposition, compared with mice in the untreated model (ISO) group. Representative images of ultrastructure captured by EM, indicating that acupuncture at PC6 normalised the disassembled sarcomeres and swollen mitochondria. MA, manual acupuncture; EM, electron microscopy; H&E, haematoxylin and eosin; ISO, isoproterenol; PR, propranolol.
Acupuncture at PC6 attenuated the expression of ANP and TNFα
The qualitative analysis of ANP and TNFα expression in the heart tissues was determined by immunofluorescent staining, and the protein levels of ANP and TNFα were quantified by Western blot analysis. The results indicated that ANP and TNFα were significantly higher in the cardiac tissues of ISO-treated mice, suggesting activation of fibrosis associated with the pathways described previously. Acupuncture at PC6 significantly decreased protein expression of ANP and TNFα in ISO-treated mice (Figures 4 and 5).
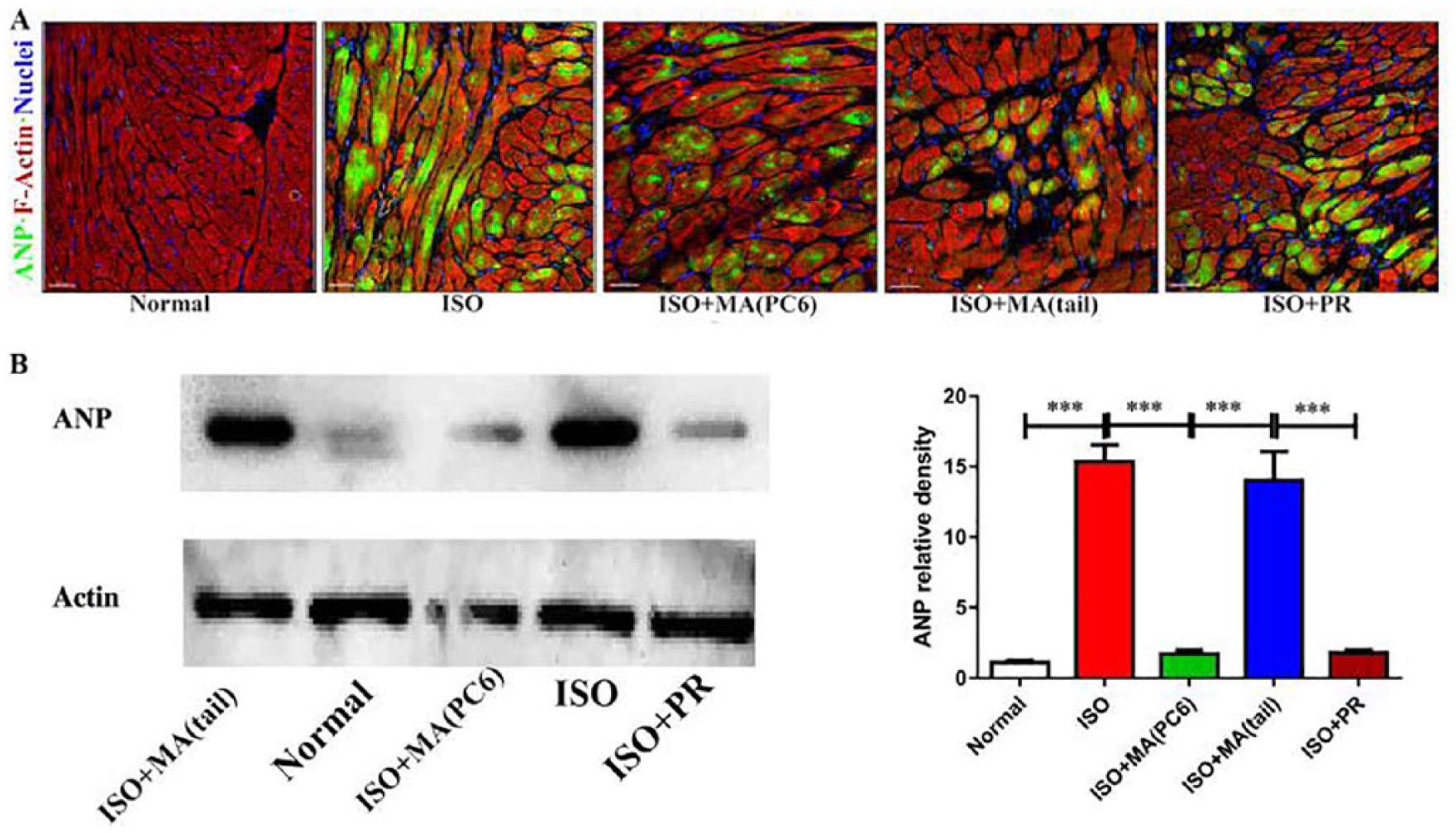
Effect of acupuncture on the production of ANP in an experimental mouse model of hypertrophy. (A) Representative images of immunofluorescent staining in each group, indicating that acupuncture at PC6 decreased the expression of ANP. (B) Representative Western blots of ANP in each group. Data are presented as mean±SEM. *** P<0.001. ANP, atrial natriuretic peptide; MA, manual acupuncture; ISO, isoproterenol; PR, propranolol.
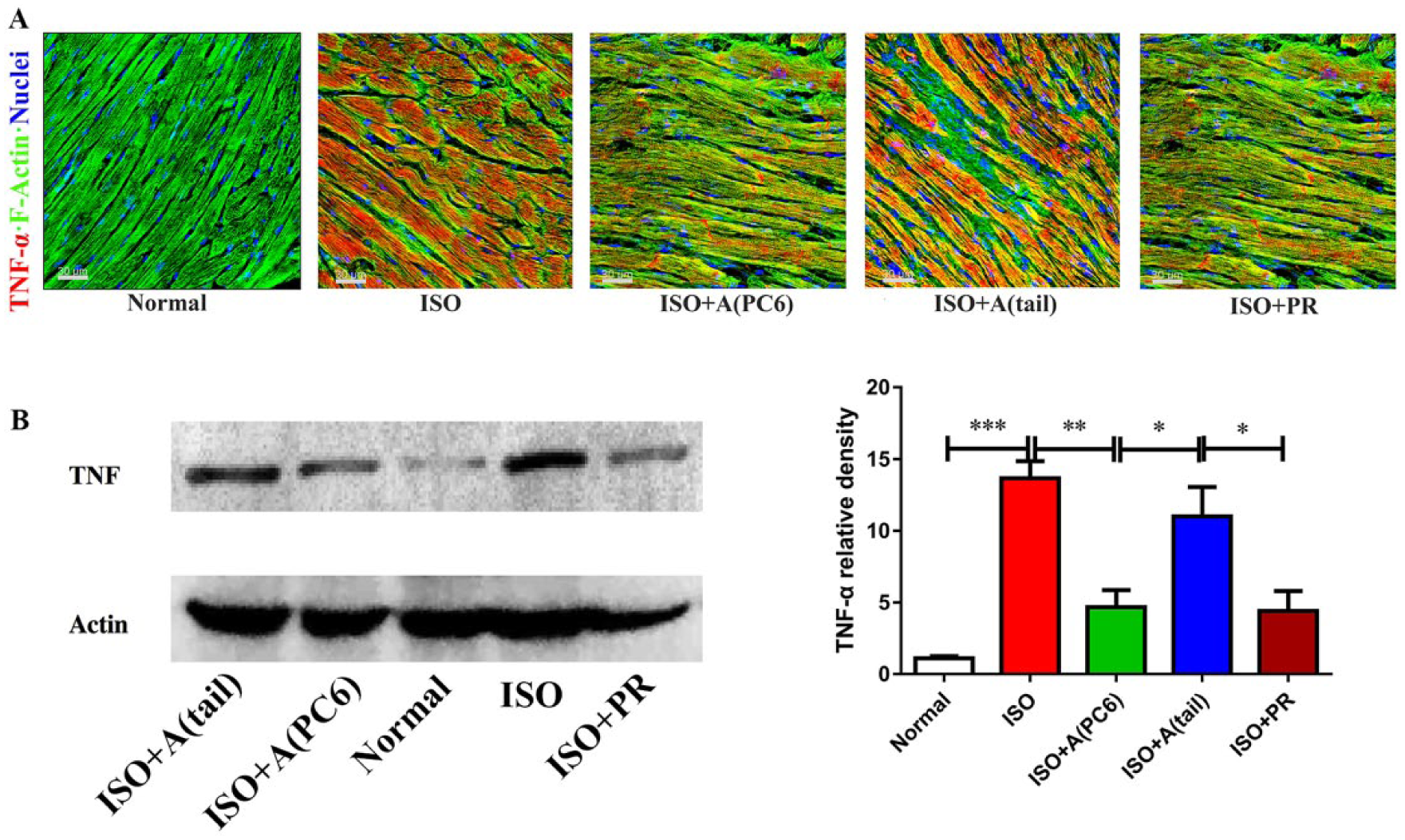
Effect of acupuncture on the production of TNFα in an experimental mouse model of hypertrophy. (A) Representative images of immunofluorescent staining in each group, indicating that acupuncture at PC6 decreased the expression of TNFα. (B) Representative Western blots of TNFα in each group. Data presented as mean±SEM. * P<0.05; ** P<0.01; *** P<0.001. MA, manual acupuncture; ISO, isoproterenol; PR, propranolol; TNFα, tumour necrosis factor α.
Discussion
It has long been established that chronic activation of the sympathetic nervous system is a major contributor to systemic hypertension, and is followed by adverse cardiac remodelling including myocardial hypertrophy and deposition of connective tissue. Losartan, an angiotensin II receptor blocker, decreased blood pressure to a near normal level, but it was found to be insufficient to reverse the adverse cardiac remodelling in the presence of ISO. 16 It was reported that activation of the Gs coupled β-adrenergic receptor gave rise to Erk 1/2 activation and accumulation in the nucleus, causing adverse cardiac remodelling. 17
Acupuncture, an important alternative therapy in China, has been shown to have beneficial effects on a variety of cardiovascular dysfunctions. Although the cellular and molecular mechanism have not been fully elucidated, increasing evidence shows that acupuncture activates underlying sensory neural pathways that project to a number of regions in the central nervous system, which ultimately regulate autonomic outflow, improve cardiovascular function, and even reduce myocardial apoptosis in SHRs.6,12 Acupuncture at PC6 has been found to be effective at lowering blood pressure, relieving chronic chest pain and preventing recurrences of atrial fibrillation in clinical trials.18–20 In an experimental study, acupuncture at PC6 improved cardiac function in rats with myocardial hypertrophy by modulating upstream neuroendocrine cytokines that regulate the Erk signalling pathways, 11 indicating that acupuncture at PC6 might have great potential to prevent the adverse cardiac remodelling induced by a β-adrenergic receptor agonist.
In our study, the mice were treated for 2 weeks with a subcutaneous infusion of ISO to boost sympathetic activity, which resulted in obvious structural impairments in the myocardial tissue, including massive fibrin deposition, increased myocyte diameter, cross-sectional area, and anterior and posterior wall thickness, as well as reduced FS. However, EF was maintained at the normal range in the model group, indicating that the compensatory hypertrophy could increase cardiac contractility to keep the EF value within the normal range. It is well recognised that LV hypertrophy and thickening are common pathological manifestations in ISO-treated mice. Our results demonstrated that acupuncture significantly reduced HW/TL ratios via reversal of LVAWd, LVAWs, LVPWd and LVPWs. We also found an enlarged cardiomyocyte cross-sectional area in the ISO-treated mice on electron microscopy, which was also alleviated by acupuncture. These results suggest that acupuncture at PC6 prevents cardiac hypertrophy. On the other hand, Masson’s staining revealed that the deposition of fibrin increased in ISO-treated mice, and acupuncture also reversed this increase in myocardial fibrosis. In keeping with our hypothesis, acupuncture at PC6 significantly reduced the heart rate of these ISO-treated mice, suggesting that the beneficial effects could be associated with modulation of autonomic outflow.
Although the signalling pathways involved in β-adrenergically induced cardiac remodelling are not well understood, evidence suggests that ANP, an important neurohumoral factor excreted by the heart, is elevated in conditions of ventricular volume and pressure overload, and plays an important role in cardiac hypertrophy and fibrosis.21,22 Acupuncture at PC6 could inhibit the expression and production of ANP, which points to a potential molecular mechanism underlying the alleviation of adverse cardiac remodelling. In addition, our electron microscopy results showed that the hypertrophic myocytes were accompanied by swollen mitochondria and disassembled sarcomeres. Indeed, over-activation of the β-adrenergic receptor has been proposed as an important contributing factor in stress cardiomyopathy, which results in increased inflammatory and oxidative responses.23,24 It was reported that chronic β-adrenergic stimulation using ISO was sufficient to induce expression of several myocardial proinflammatory cytokines, including TNFα, interleukin 1b (IL-1b) and IL-6, 25 mediating adverse cardiac remodelling in vivo in a receptor specific manner. 26 Moreover, TNFα also provoked a hypertrophic growth response in a dose-dependent manner and increased actin and myosin heavy chain synthesis in cardiomyocytes. 27 Our findings demonstrate that acupuncture at PC6 could inhibit the expression and production of TNFα, and provide evidence that acupuncture might reduce adverse cardiac remodelling by inhibiting chronic inflammation.
Taken together, our results demonstrate that acupuncture at PC6 could antagonise β-adrenergic receptors to improve cardiac remodelling by reducing the deposition of fibrin and normalising myocardial hypertrophy. Moreover, acupuncture at PC6 might exert a beneficial effect through the regulation of ANP and TNFα at a cellular molecular level, which justifies further intensive study of potentially related downstream signalling pathways. Nevertheless, it can be concluded that acupuncture may have significant potential as an adjuvant therapy for the treatment of sympathetic hypertension, providing benefits to patients by reversing adverse cardiac remodelling. Its clinical efficacy therefore deserves further evaluation through randomised controlled trials.
Footnotes
Acknowledgements
The authors would like to thank the Harbin youth innovative talents of science and technology project for its support.
Contributors
MZ contributed to the design of the work and data acquisition/analysis. QD, FY and YG contributed to data acquisition/analysis. YH analysed the data and drafted and revised the paper. PZ contributed to the conception and design of the work and drafted and revised the paper. All authors approved the final version of the manuscript accepted for publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Chinese postdoctoral science foundation project (ref. 2016M591555), Heilongjiang post-doctoral science foundation project (ref. LBH-Z16143), Heilongjiang provincial natural science funds general project (ref. H201315) and Harbin outstanding youth talent project (no. 2016RAYYJ006).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Provenance and peer review
Not commissioned; externally peer reviewed.