
Abstract
Introduction:
Propofol provides excellent sedation during colonoscopy. However, its application, namely when used together with an opioid, is associated with cardiopulmonary depression. Acupuncture is used nowadays for the treatment of pain and anxiety, and also to induce sedation. We hypothesised that electroacupuncture (EA) during colonoscopy would have sedative effects, thereby reducing propofol requirements to achieve an adequate level of sedation.
Method:
The study was designed and conducted as a single centre, patient and observer blinded, sham- and placebo-controlled randomised trial. Patients scheduled for elective colonoscopy under deep propofol/alfentanil sedation were randomly assigned to receive unilateral EA, sham-acupuncture (SA) or placebo-acupuncture (PA) at ST36, PC6 and LI4. The primary outcome parameter was the total dosage of propofol. Secondary outcomes included the patients’ and endoscopists’ satisfaction levels evaluated by questionnaires.
Results:
The dosage of propofol required (median [IQR]) was not significantly different between the three groups (EA group 147 μg/kg/min [109–193] vs SA group 141 μg/kg/min [123– 180] vs PA group 141 μg/kg/min [112–182]; P=0.776). There was also no significant difference in alfentanil consumption (P=0.634). Global satisfaction (median [IQR]) among patients (EA group 6.6 [6.0–7.0] vs SA group 6.8 [6.0–7.0] vs PA group 6.5 [6.0–7.0]; P=0.481) and endoscopists (6.0 [5.0–6.0] for all groups; P=0.773) did not significantly differ between the three groups. There was no significant difference in the number of cardiorespiratory events.
Conclusion:
For colonoscopy, the applied mode of EA did not show any propofol-sparing sedative effect compared with sham or placebo acupuncture.
Trial registration:
The trial is registered in the Netherland’s Trial Registry (NTR4325).
Introduction
The number of colonoscopies performed annually has increased in recent years and will continue to rise further due to national cancer screening programmes. Colonoscopy is known to be uncomfortable for patients. Pain, vasovagal reactions or uncooperative behaviour of patients can compromise screening effectiveness. 1 Therefore, sedation with analgo-sedative drugs is often requested for these procedures. 2
Propofol has become the standard for sedation during endoscopic procedures due to its rapid onset and termination of action.3–5 However, the most important disadvantage of propofol-based sedation is the risk of unintentional deep sedation leading to cardiorespiratory depression, especially when combined with a powerful opioid like alfentanil or fentanyl.6–9
Adjuvant methods might be suited to lowering the dosage of propofol while keeping an adequate level of sedation, thereby minimising the risk of cardiopulmonary side effects.
Acupuncture is used worldwide for various indications, with the most promising evidence shown so far for the treatment of pain and postoperative nausea and vomiting (PONV).10–17 Electroacupuncture (EA) facilitates standardisation of acupuncture and provides better analgesia compared with manual acupuncture. 18 Also, patients are happy to receive acupuncture as an addition to routinely used sedation or anaesthesia schemes even in the acute hospital setting. 19 Therefore, we designed a study format in which additional acupuncture treatment could easily be implemented next to clinical routine practice in outpatients undergoing colonoscopy.
We hypothesised that unilateral EA at ST36, PC6 and LI4 during colonoscopies has sedative effects, thereby reducing the dosage of propofol required to achieve an adequate level of sedation. The primary endpoint was the total dosage of propofol measured at the end of the procedure. The secondary endpoint was the patients’ and endoscopists’ satisfaction level with the combination of EA and propofol sedation for the respective procedures evaluated by questionnaires, which both groups had to fill in after the procedure.
Methods
We performed a prospective, patient and observer blinded, sham- and placebo-controlled randomised trial following the STRICTA (Standards for Reporting Interventions in Clinical Trials of Acupuncture) reporting guidelines 20 and the CONSORT (Consolidated Standards of Reporting Trials) statement. 21 The trial is registered in the Netherland’s Trial Registry (NTR4325). The study protocol was published in 2015. 22
The study took place at the Department of Gastroenterology and Hepatology at the Academic Medical Centre (AMC), Amsterdam, the Netherlands, between February 2014 and February 2017. Patients who were scheduled for an elective diagnostic or therapeutic colonoscopy with propofol sedation, were aged above 18 years, fell into American Society of Anesthesiologists (ASA) classes I–III, and gave written informed consent, were invited to participate in the study by an independent investigator. Patients were excluded if they were aged <18 years, were ASA class IV or V, had a nickel allergy, implanted pacemaker device, psychiatric or neurologic disorders, used anticoagulants or refused sedation.
All included patients were randomised by computer selection (RITA version 1.31) to receive unilateral EA, sham acupuncture (SA) or placebo acupuncture (PA). A second investigator who was not involved in the study performed computer randomisation and preparation of the numbered randomisation envelopes. One of the two acupuncturists who subsequently provided acupuncture opened these envelopes. All three groups received sedation with propofol and alfentanil from specialised sedation anaesthesia nurses. Colonoscopies were performed either by a Gastroenterology resident or staff member.
All involved parties (patient, sedation anaesthesia nurse, endoscopist, endoscopic nurse and the independent investigator)—with exception of the acupuncturist—were blinded to the intervention.
Procedure
After randomisation the patients received an intravenous line, and glycopyrrolate 0.2 mg and lidocaine 50 mg were given intravenously. Patients were provided with 2 L/min of oxygen via a nasal cannula and underwent monitoring of heart rate (HR), electrocardiogram (ECG), non-invasive blood pressure (NIBP), oxygen saturation (SpO2) and end-tidal carbon dioxide tension (etCO2) as well as respiratory rate (RR). All parameters were documented at 5 min intervals.
Each group received sedation with propofol using a target controlled infusion (TCI) system that has a weight and age adapted algorithm to attain a pre-set propofol plasma target level. Sedation level was evaluated by the sedation anaesthesia nurses using the observer’s assessment of alertness/sedation (OAA/S) scale. 23 Before starting colonoscopy, the patient’s level of sedation was confirmed to be consistent with an OAA/S score <3, which means patients responded with maximal lethargy if their name was called loudly and/or repeatedly. If the patient was still too alert, additional sedation was provided with step up of the TCI. In addition, patients were given 1.5 µg/kg alfentanil at the beginning of the colonoscopy. Pain during the procedure was rated by the anaesthesia nurse using the behavioural pain scale for non-intubated patients (BPS-NI). 24 This scale evaluates three behavioural domains (facial expression, movements of upper limbs and vocalisation) with values ranging from 3 (no pain) to 12 (most pain). Patients received an additional dose of 1.5 µg/kg alfentanil during the procedure if the BPS-NI was ⩾7.
The EA intervention took place immediately after starting propofol sedation and during the colonoscopy procedure. Haemodynamic or pulmonary changes were classified as cardiorespiratory events if they lasted longer than 5 min. Cardiorespiratory events were defined as: a decline in SpO2 <90% or breathing frequency <6/min; a change in HR ±20% or NIBP ±20% of baseline; or occurrence of any arrhythmias.
After the procedure the patients were transported to the recovery unit and monitored with ECG, NIPD and SpO2. Level of recovery from sedation and the return of physical fitness were assessed using the modified Aldrete score 25 at 10, 30 and 60 min after arrival in the recovery room. Discharge criteria were considered to have been met when the Aldrete score was ⩾9 or equivalent to the pre-procedure score, and the patient was alert and mobile with stable haemodynamics.
Intervention
To integrate acupuncture without delay into our routine colonoscopy programme, the acupuncture needles were placed unilaterally on the right hand side immediately after starting propofol sedation by the acupuncturist according to treatment group allocation, and connected to a six-channel programmable electrical stimulator (SVESA 1031, SVESA GmbH, Germany, Munich); needles were fastened with tape.
Patients in the EA group were treated with real stainless steel acupuncture needles (asia-med, Germany, Special No. 16 (0.30×30 mm/gauge 8×1.2′), inserted unilaterally on the right hand side at PC6, ST36 and LI4 (Figure 1) to a depth of approximately 0.5 cm, 1 cm and 0.5 cm, respectively. Since sedated patients could not report the de qi sensation— which awake patients describe as a feeling of heaviness or numbness—we relied on the phenomenon of ‘needle grasp’ which means that the acupuncturist felt increased resistance of the surrounding tissue during needle manipulation. 26 For electrical stimulation we aimed for a stimulation frequency of 10 Hz and intensity of 2.5 mA. Pulse width was 0.5 ms.
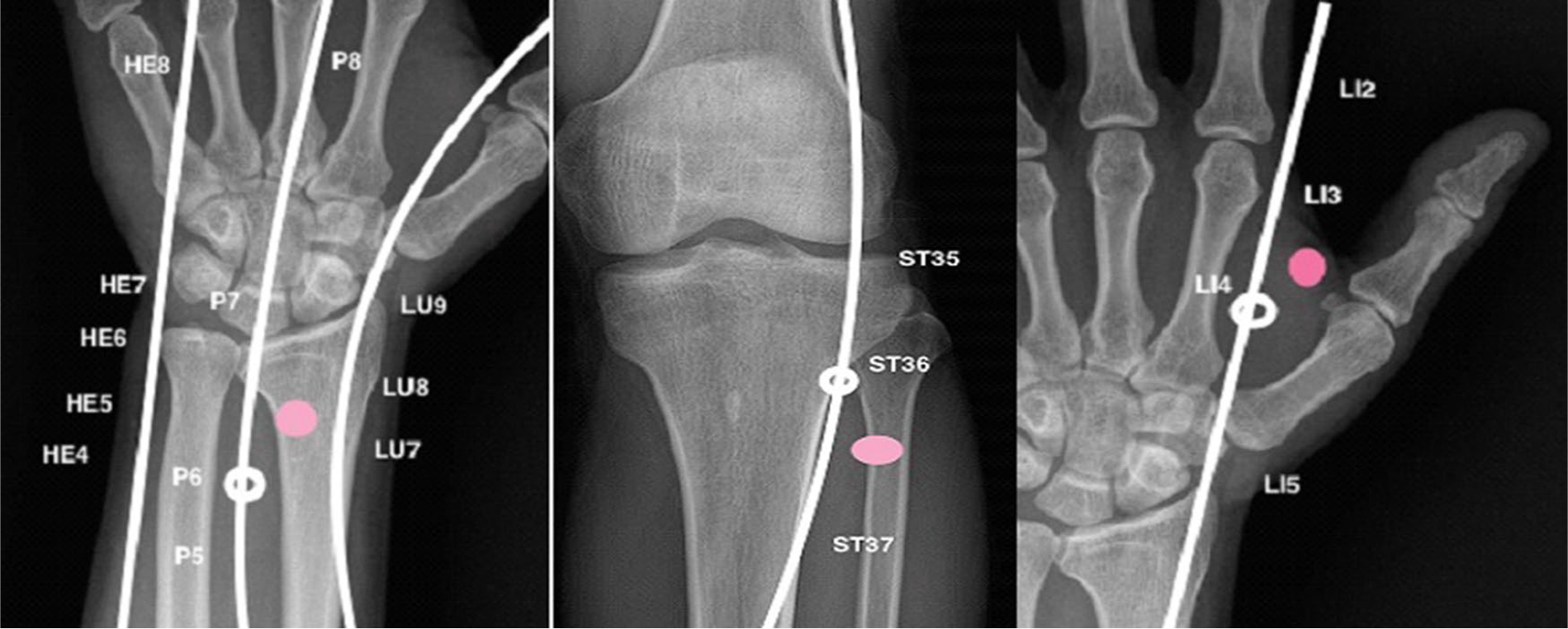
Traditional acupuncture points (white) versus sham acupuncture points (pink).
The combination of PC6, ST36 and LI4 is considered to be relevant for providing sedation and analgesia and diminishing abdominal distension. 27
PC6 is targeted for the prevention and treatment of nausea and vomiting, stimulation at ST36 is supposed to have the greatest influence on the gastrointestinal tract, and LI4 is one of the most used traditional acupuncture points for the treatment of pain and intestinal diseases. 28
The SA group was treated with the same sort of needles. In contrast to the EA group the needles were inserted 1 cm distal and lateral to the verum traditional acupuncture points (PC6, ST36, LI4) at ‘non-point’ locations that did not correspond to the location of any traditional acupuncture points. Insertion depth was approximately 0.5 cm.
The PA group received placebo needles (stainless steel Streitberger needles, asia-med, Germany, 0.30×30 mm/gauge 8×1.2′) at the same points used for sham acupuncture to exclude an acupressure effect at the verum acupuncture needling locations.
The Streitberger needle is a lookalike of a real acupuncture needle but has a blunt tip whose shaft telescopes into the handle during application without penetrating the skin. 29
In the control groups (SA and PA), the stimulator was likewise connected but without electrical stimulation. The intervention with EA was stopped as soon as the colonoscopy was finished. In all groups the needles were removed at the end of the colonoscopy procedure.
Questionnaires
Patients were asked to fill in questionnaires before discharge and 24 hours later by telephone call. The questionnaires for patients (patient satisfaction with sedation instrument (PSSI)) and endoscopists (clinical satisfaction with sedation instrument (CSSI)) were developed by Vargo et al. 30 and translated into Dutch by our own research group. The PSSI contains 20 questions with four subscores to describe patient satisfaction. Question 1 to 15—concerning sedation quality, side effects and recovery—were filled in directly before discharge home by the patient; questions 16 to 20—concerning global satisfaction, return to daily activity and comparison with other sedation experiences—were inquired about the following day by telephone. Endoscopists had to fill in their questionnaire immediately after the colonoscopy. The CSSI also has four subscores with one of them relevant for global satisfaction. In these questionnaires, patients and endoscopists could classify their satisfaction or dissatisfaction with the procedure from 7 (very satisfied) to 1 (very dissatisfied). 30 Pain was assessed post-procedurally by means of a numeric rating scale (NRS) ranging from 0 (no pain) to 10 (worst pain).
Statistical methods
Sample size calculation was based on observational propofol data from previous colonoscopies collected in our hospital sedation database. The mean±SD dosage of propofol administered during colonoscopy in this database was 441±176 mg. 31 At 80% power and alpha level of 0.05, it was estimated that 47 subjects in each group would be needed to detect a 25% reduction in propofol dosage. Considering a dropout rate of 10%, the target sample size was 51 patients per group.
Statistical analyses were performed using SPSS (version 23.0). All data were checked for normal distribution using the Kolmogorov test, Q-Q plots and histograms. For normally distributed continuous variables, one-way analysis of variance (ANOVA) was used and the variables presented as mean±SD. For normally distributed categorical variables Pearson’s Χ2 test was applied and variables were allegorised as number and/or percentage. Skewed data were compared using multifactorial ANOVA (Kruskal Wallis) and the variables presented as median and IQR. A value of P<0.05 was considered statistically significant.
Results
In total, 222 patients were assessed for eligibility; 69 patients were not willing to participate or were excluded for other reasons. The remaining 153 patients were allocated randomly to receive EA (EA group, n=51), sham acupuncture (SA group, n=51) or placebo acupuncture (PA group, n=51). In the PA group data collection from one patient was incomplete, but we decided to perform an intention-to-treat analysis and to include their data in the final analysis. The study flow chart is shown in Figure 2.
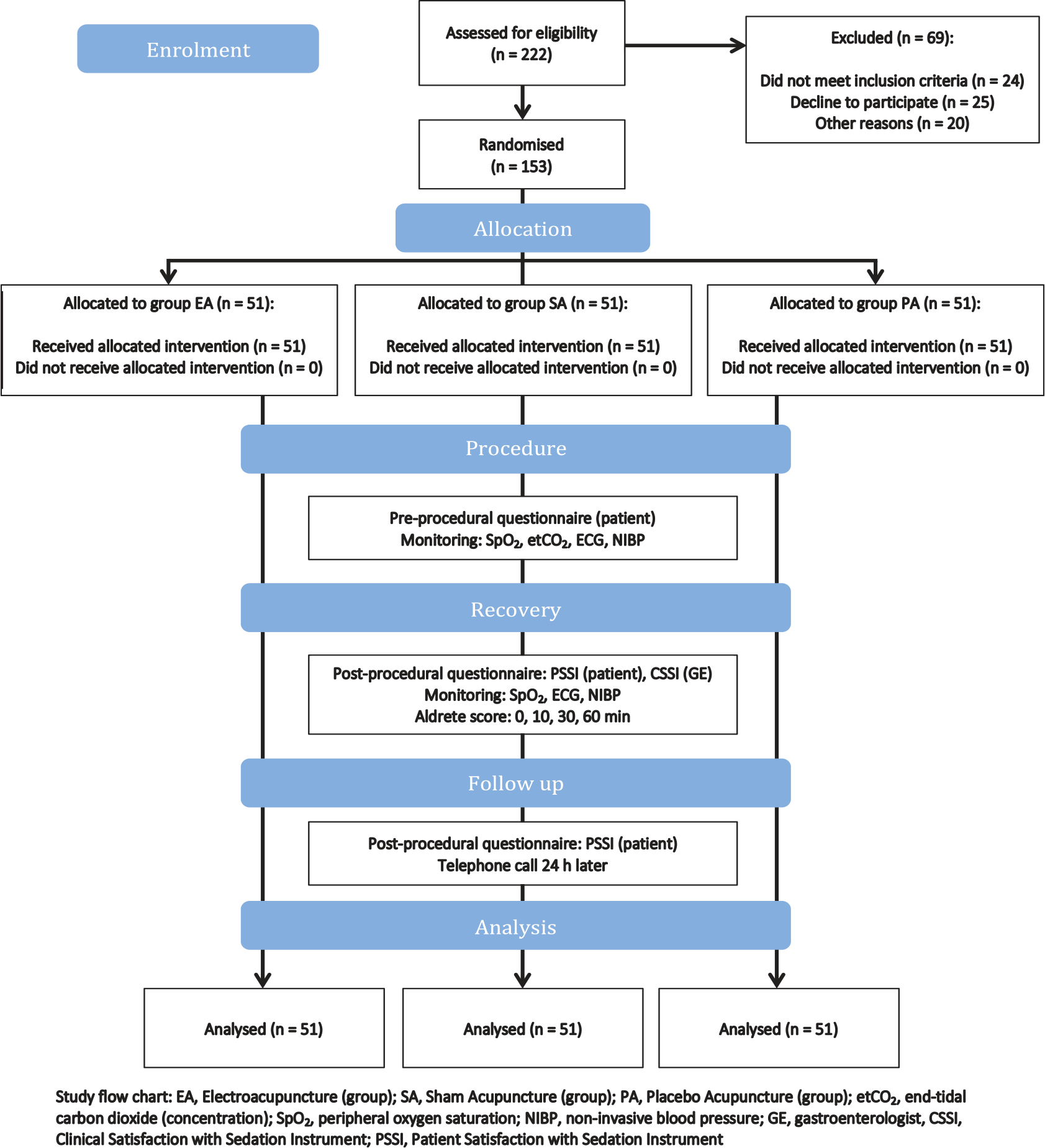
Flow chart of the study.
All three groups were comparable with regard to their baseline characteristics, indication for and length of the colonoscopy procedure (Table 1).
Patients’ baseline characteristics, indication for colonoscopy and length of procedure.
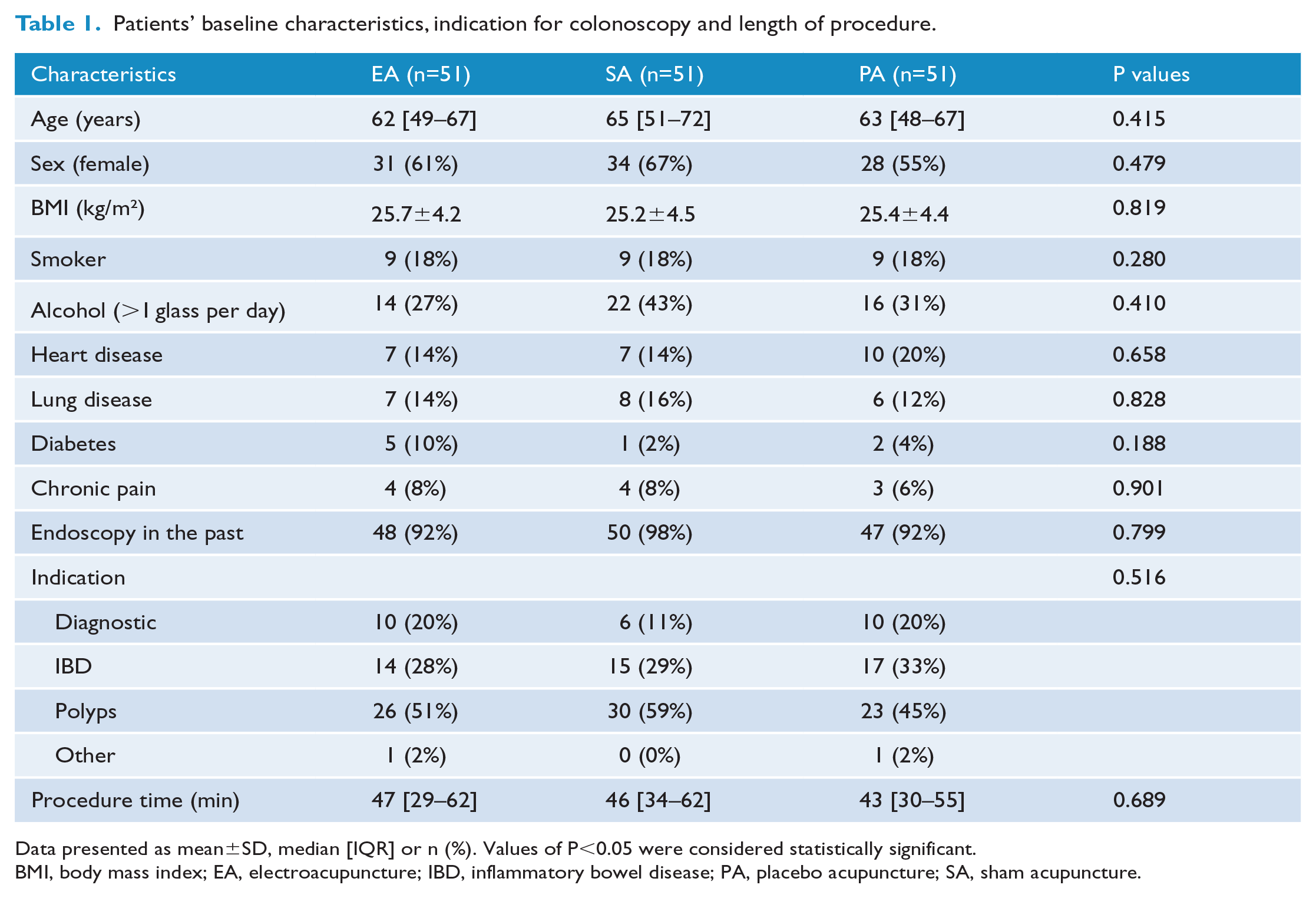
Data presented as mean±SD, median [IQR] or n (%). Values of P<0.05 were considered statistically significant.
BMI, body mass index; EA, electroacupuncture; IBD, inflammatory bowel disease; PA, placebo acupuncture; SA, sham acupuncture.
The dosage of propofol (median [IQR]) in the EA group (147 µg/kg/min [109–193]), SA group (141 µg/kg/min [123–180]) and PA group (141 µg/kg/min [112–182]) were not significantly different (P=0.776). There was also no significant difference in alfentanil consumption (P=0.634), observed pain (P=0.236) or in attained OAA/S score (P=0.647) during the procedure (Table 2).
Primary endpoint: dosage of propofol, alfentanil, pain, OAA/S.
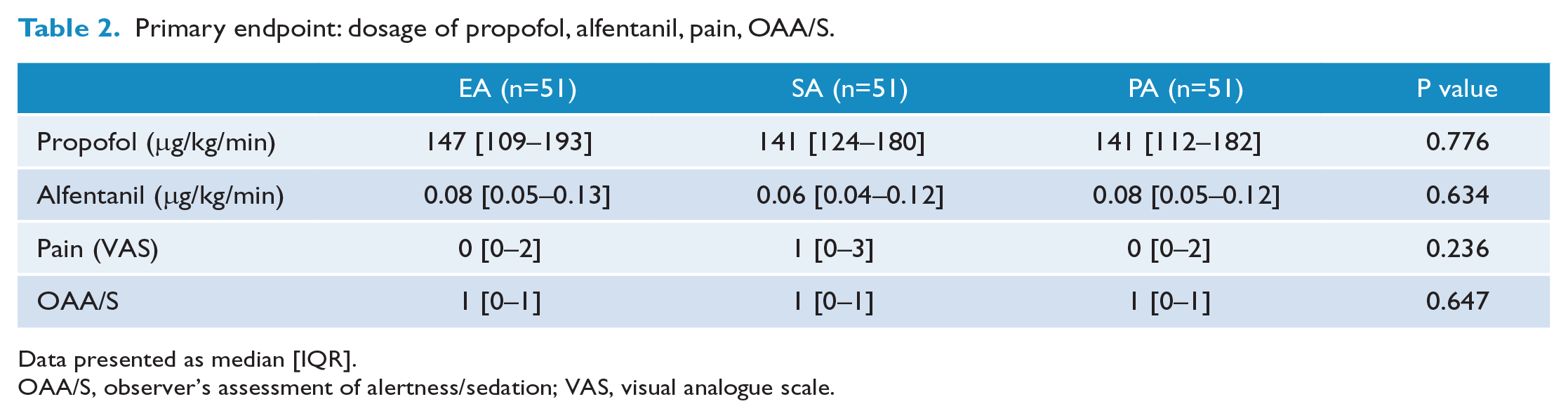
Data presented as median [IQR].
OAA/S, observer’s assessment of alertness/sedation; VAS, visual analogue scale.
Global satisfaction among patients (median [IQR]: EA group 6.6 [6.0–7.0] vs SA group 6.8 [6.0–7.0] vs PA group 6.5 [6.0–7.0]) and sedation side effects (median [IQR]: EA group 6.2 [5.6–6.6] vs SA group 6.4 [6.0–6.8] vs PA group 6 [5.5–6.6]) was not significantly different between the three groups (P=0.155–0.481). Global satisfaction (median [IQR]) among gastroenterologists was similar in all groups: (EA, SA and PA groups: 6.0 [5.0–6.0]; P=0.773) (Table 3).
Secondary endpoint: satisfaction and side effects.
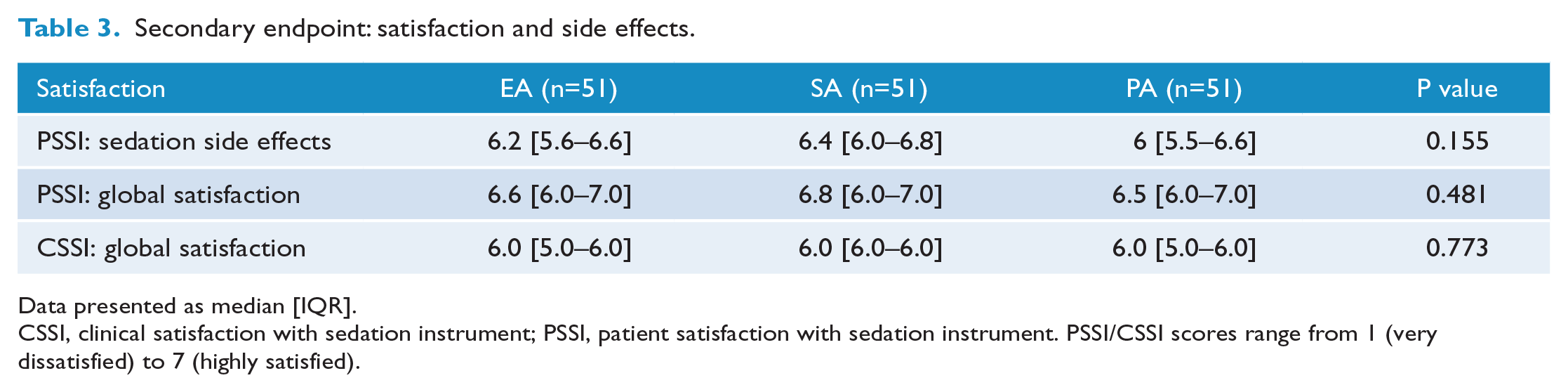
Data presented as median [IQR].
CSSI, clinical satisfaction with sedation instrument; PSSI, patient satisfaction with sedation instrument. PSSI/CSSI scores range from 1 (very dissatisfied) to 7 (highly satisfied).
The number of cardiorespiratory adverse events (data not shown), and also haemodynamic parameters during recovery (HR, NIBP, SpO2 and Aldrete score) (data not shown), were not significantly different between the three groups.
Discussion
In our study, EA neither reduced the dosage of propofol that was necessary to achieve an adequate level of sedation during colonoscopy, nor significantly lowered the number of adverse cardiorespiratory events. In addition, there was no significant difference in satisfaction among patients and gastroenterologists between the EA group and the two control groups.
Start, level and administration of sedation
In contrast to our findings, Lee et al. concluded from a systematic analysis of studies of acupuncture for gastrointestinal procedures that acupuncture might have a greater sedative effect during gastrointestinal procedures than sham acupuncture, and efficacy similar to premedication with a combination of an opioid and a benzodiazepine. 32 This result is supported by three other trials showing that acupuncture significantly reduces the required dosage of sedative drugs and pain during colonoscopy.33,34 Ng et al. 34 used patient-controlled analgo-sedation with propofol and alfentanil (n=128 patients). In the studies of Ni et al. 35 (n=60 patients) and Fanti et al. (n=30 patients) 33 midazolam was given on demand if the patient was complaining of pain or felt uncomfortable. Both studies used mild or moderate sedation aiming for a conscious patient. In our study, all groups were sedated with propofol by specialised sedation nurses until they showed a NRS score of 0 (0–2) and an OAAS score of 1 (0–1), which means patients were deeply sedated with marginal reactions to mild or even moderate prodding and shaking.
Deep sedation as well as general anaesthesia or even local anaesthesia can inhibit the effect of acupuncture.36,37 During EA, serotonin pathways in the central insula, and mood and affect in higher cortical centres, are modulated. This was demonstrated by Chu et al. 38 using functional MRI during CT colonography in completely awake patients without any form of sedation or analgesia except for acupuncture. Wang et al. 37 found in their MRI studies that propofol-based general anaesthesia reduced the neurophysiological response to acupuncture. As in our study, Wang et al. applied acupuncture after starting general anaesthesia.
It is possible that brain reactions to noxious stimuli, and the interaction of these stimuli with the acupuncture-evoked effect, are inhibited in deeply sedated patients.
Electroacupuncture
Besides the drug used, method and start of drug administration and the corresponding level of sedation and analgesia, laterality and timing of EA are important discussion points.
Ni et al. 35 and Fanti et al. 33 administered acupuncture at four more traditional acupuncture points in their studies and also treated bilaterally: ST37, SP6, SP9 and auricular Shenmen. We used a pragmatic unilateral acupuncture approach comprising three traditional acupuncture points (PC6, ST36, and LI4) on the right-hand side.
During colonoscopy patients are positioned on their left hand side. Therefore, traditional acupuncture points on the right hand side of the patient were easier to access during the procedure and less influenced by the rotations of the patient that were eventually necessary. Furthermore, different groups have shown that the unilateral acupuncture approach might be as effective as the bilateral approach.39–41
Another argument for the unilateral approach is the hypothesis that the acupuncture effect is mediated via β-endorphins. Leung et al. found that, in blood samples of EA-treated patients, 45 min after the start of EA, β-endorphins were significantly higher than in a SA group. 42 It might therefore be necessary to start EA 20–45 min pre-procedurally to allow the maximum level of endogenous opioids to be reached before starting sedation or colonoscopy. This hypothesis is also supported by Gao et al., 43 who showed an increased tolerance to bupivacaine-induced cardiotoxicity after EA pre-treatment lasting 60 min in rats.
We aimed to perform a placebo-controlled trial. Starting acupuncture and EA before starting sedation would likely have provoked de qi or EA sensation in an awake patient. This could have led to the patients in the EA group being de-blinded. Therefore, we decided not to start the intervention (acupuncture and EA) before starting sedation.
Nevertheless, timing, length and type of EA stimulation seem to be important points for the combination of acupuncture and deep sedation/anaesthesia. 44
Therefore, we cannot exclude the possibility that an acupuncture strategy different to the one chosen in the current study could have had a sedative drug-sparing effect.
Zhang et al. 45 added important (non-pharmaceutical) arguments to the discussion of acupuncture before or during anaesthesia. Considering the fact that a board-certified acupuncturist and additional devices are necessary for (bilateral) multipoint transcutaneous electrical acupuncture point stimulation at least 30–45 min before induction of anaesthesia, not only should the effectiveness of acupuncture be investigated in future studies, but also cost-effectiveness and optimisation of standard anaesthesia management 46 .
Limitations
General
Our study was designed as a single centre trial in the Academic Medical Centre, an academic teaching hospital treating highly complex patients out of the region of Amsterdam. Despite having experienced gastroenterologists, training of residents to perform colonoscopies probably resulting in longer lasting and more complex procedures with the need for deep sedation to facilitate the procedure, which may have counteracted the possible effects of EA.
Acupuncture points
In Western medicine, acupuncture is not explained by traditional concepts of Yin and Yang, but by release of neuropeptides through local antidromic axon reflexes and increased local nutritive blood flow.47,48 In our trial, locations of the ‘non-acupuncture points’ in the SA and PA groups were chosen with the intention that stimulation of the traditional acupuncture point locations should be minimal. However, according to the definition of Western medical acupuncture, our non-acupuncture points were also in high-density neural fibre areas, and needling at these nearby locations may have resulted in axon reflexes leading to release of neuropeptides, thereby modifying pain sensation.
Electrical stimulation
Another point of discussion is temporal adaption to the electrical stimulator. The cited studies differed in their choice of frequency of stimulation from low (eg, 2 Hz) to high (eg, 100 Hz). Low frequency EA seems to involve central pathways different to those of high frequency EA. 49 Therefore, different patterns of frequency might have different effects on the usage of sedatives. Leung et al. showed that the level of β-endorphins declined after reaching the aforementioned peak value after 25–30 min of treatment. 50 In our trial we used a constant low frequency stimulation of 10 Hz for the electrical stimulation during the entire procedure, which could eventually have lead to habituation to the stimulus.
Strengths
One might ask whether the sample size of our study was high enough to show significant differences between the three groups. We performed an a priori power analysis during the design of our study. Including n=153 patients, we performed one of the largest prospective, observer and patient blinded, randomised studies with three comparable groups with regards to baseline characteristics. Using sham and placebo groups, we also attempted to exclude the placebo effect 51 of acupuncture and non-specific effects of puncturing the skin by use of Streitberger placebo needles. We therefore do not consider significant type 2 errors likely to be responsible for the lack of effect of acupuncture in our study.
In contrast to other studies, we used validated questionnaires to evaluate the satisfaction levels of the patients and the endoscopists, and their experiences with sedation. The satisfaction levels of both the patients and the endoscopists were high in all three groups, probably due to the effect of deep sedation. 31 Furthermore, we integrated acupuncture in daily sedation practice—without using extra time—making it feasible for clinical use.
Future directions
For further studies it would be interesting to use the functional MRI approach of Chu et al. 38 to evaluate whether there is a modified brain reaction to noxious stimuli and acupuncture-evoked effects in deeply sedated patients.
Conclusion
Unilateral EA did not show any propofol-sparing sedative effect compared with sham and placebo acupuncture in patients deeply sedated for colonoscopy. It neither reduced the dosage of propofol and alfentanil, nor significantly lowered the number of adverse cardiorespiratory events. In addition, there were no significant differences in levels of satisfaction among patients and gastroenterologists between the EA group and the control groups.
Footnotes
Contributors
SE, NMdO, KS, MWH and BP were responsible for study design. SE drafted the manuscript. SE, NMdO, DB, PF, KS, MWH and BP critically revised the manuscript. All authors approved the final version of the manuscript accepted for publication.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval was obtained from the Medical Ethics Committee of the Academic Medical Centre, Amsterdam, the Netherlands (NL36861.018.11) on 6 May 2013.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by institutional funding only. The Streitberger needles were kindly provided by asia med.
Provenance and peer review
Not commissioned; externally peer reviewed.