
Abstract
Background:
Neonatal pain is an extensive research field and there are many possibilities to treat pain in neonates. Acupuncture is one new and non-pharmacological option and a promising tool to reduce pain in neonates undergoing minor painful interventions during routine medical care.
Objectives:
This review summarises trials of acupuncture for pain reduction in neonates undergoing painful interventions during routine medical care.
Data source:
MEDLINE, Embase, CINAHL, electronic clinical trials registry platforms and reference lists were systematically screened for trials from their dates of inception to February 2017 (English language database search).
Study selection:
Inclusion criteria were (1) preterm or term neonates, (2) acupuncture for painful medical interventions and (3) formal pain assessment as a primary or secondary study outcome. We included only randomised controlled trials.
Data extraction:
Data were extracted using a standardised protocol and individual risk of bias was assessed.
Results:
The literature search revealed a total of 12 196 records. After application of inclusion criteria, five studies were included in this review. Two studies demonstrated significant pain reduction, one found equal outcomes in comparison to standard care, and two showed significantly higher pain scores with acupuncture alone.
Limitations:
The main limitation of the results is the heterogeneity across trials in acupuncture modality, acupuncture point selection, control groups and pain assessment (heterogeneity: I2=87%).
Conclusion:
The results of this review suggest that acupuncture may have a positive pain-relieving effect in neonates. However, due to the low number of available high-quality trials and heterogeneity across the studies it is not possible to state clear recommendations.
Introduction
It has been shown that neonates, despite the immaturity of the developing neonatal nervous system, are able to experience sensory and affective facets of pain, as brain regions that encode pain in adults are already active in term neonates. 1 However, pain and stress have a negative influence on the neonate’s rapidly developing neuronal structures, affecting functional connectivity or dynamic interconnectivity of the small neurobiological networks in the brain.2,3 Thus, neonates may have a reduced sensory threshold to pain, making them more sensitive and vulnerable in later life, especially during painful procedures. 4
In general, hospitalised neonates undergo many painful procedures for treatment or diagnostic purposes. 5 At present, the gold standard for pain relief during minor painful interventions in neonates is an orally administered sweet solution.6,7 However, other effective non-pharmacological methods to provide pain relief in neonates during these procedures are rare.
Therefore, it is highly important to improve pain management in neonates and to develop and study new and gentle strategies.
Acupuncture is a promising non-pharmacological technique for pain management in children and neonates, which is performed by stimulating somatic tissues with needles, laser, acupressure or non-invasive electrical stimulation.8,9 There has been extensive research into the mechanism of acupuncture analgesia in adults and animals, which involves both central and peripheral effects. Previous studies have demonstrated modulation of activity in multiple cortical and subcortical brain areas—for example, the brainstem, cerebellum and limbic areas—in humans undergoing acupuncture treatment.10,11 The pain-reducing effects of acupuncture could also be related to increased local blood flow after stimulation, which may lead to an accelerated washout of analgesic substances. Further studies have shown that regional skin and/or muscle blood flow increase due to manual acupuncture and that electroacupuncture causes cutaneous vasodilation through elevation of nitric oxide levels, calcitonin gene related peptide release from sensory nerve fibres via the axon reflex, and elevation of arterial blood pressure.12–15 It has also been shown that needle acupuncture and laser acupuncture are presumably comparable in their effects. 16
These mechanisms can probably lead to an analgesic effect of acupuncture in children as well as in neonates, because preliminary studies have shown a pain relieving effect of acupuncture in children and infants.17–20 In neonates, acupuncture is described as a safe technique and has shown effects on regional cerebral oxygen saturation.21–24
Therefore, we performed a systematic literature review to summarise the current available evidence on acupuncture techniques for pain management in term and preterm neonates.
Methods
Eligibility criteria
The research question was designed following the PICO (population-intervention-comparison-outcome) format: ‘In term and preterm neonates (defined as within the first 4 weeks of life), does acupuncture (including all invasive and non-invasive acupuncture modalities), in comparison to no intervention or any other pain therapy, lead to improved pain scores during painful medical interventions?’ We considered randomised controlled trials published between database inception and February 2017.
Inclusion criteria were (1) preterm (<37 weeks of gestational age) or term (>37 weeks of gestational age) neonates, (2) acupuncture for painful medical interventions and (3) formal pain assessment as a primary or secondary study outcome. Randomised controlled trials were included.
Among others, acupuncture modalities included needle acupuncture, light needling, acupressure, laser acupuncture, non-invasive electrical stimulation of (traditional) acupuncture points (NESAP) and moxibustion.
The MeSH (Medical Subject Headings) search terms were ‘complementary therapies’, ‘complementary medicine’, ‘acupuncture’, ‘pain’, ‘infant, newborn’ and various combinations of these. The search strategies for all databases are detailed in the Supplemental material.
Information sources
The search was originally run in July 2016 and updated in February 2017 using international electronic databases, electronic clinical trials registry platforms and reference lists of publications (English language database search).
MEDLINE was screened using the search platforms PubMed, Embase (1988–2017 week 04) was assessed via the search surface OvidSP, and CINAHL was checked on search platform EBSCOhost, with the last searches being performed on 24 January 2017. We searched the electronic clinical trials registry platform https://clinicaltrials.gov/, http://apps.who.int/trialsearch/ and the Pediatric Academic Societies’ 2000–2015 Archive Abstracts2View site (http://www.abstracts2view.com/pasall/) to identify ongoing or not yet published trials (last access on 19 February 2017). Lastly, we screened reference lists of relevant publications for articles matching our inclusion criteria.
Study selection
Two reviewers (JS, LPM) independently performed the systematic literature search and screened titles and abstracts of identified studies. If studies matched the predetermined inclusion criteria, full texts were obtained and reviewed. Reviewers then compared results and resolved potential differences by discussion.
Data collection process
One reviewer (JS) extracted data using a standardised protocol, which was then verified by a second reviewer (LPM). Disagreement was resolved by discussion. The following data were extracted: study author(s), year, country, study design, sample size, age of participants, painful medical intervention, acupuncture modality, acupuncture points, intervention treatment, control treatment and pain assessment.
Risk of bias in individual studies
We followed the guidelines of the Cochrane Handbook for Systematic Reviews of Interventions. 25 The risk of bias was evaluated by two reviewers (JS, LPM)— one was not blinded and the other was blinded to authors, institutions, journals and results of studies. Risk of bias was assessed for (1) sequence generation, (2) allocation concealment, (3) blinding of participants and personnel, (4) blinding of outcome assessment, (5) incomplete outcome data, and (6) selective outcome reporting. Risk of bias could be high (red), low (green) or unclear (yellow).
The participant was defined as the neonate, and personnel were defined as the acupuncturist and/or research team who carried out the intervention.
The outcome assessor was defined as the person who assessed the pain score as the main outcome parameter.
Synthesis of results
A structured synthesis of data summarised the results of included trials. Study characteristics and risk of bias assessment are presented as descriptive summaries.
Due to the low number of included studies, heterogeneity among trials and incomplete data reporting, we were not able to conduct a meta-analysis or any subgroup-analyses.
Heterogeneity was assessed using Review Manager 5.3.
Results
Study selection
A total of 12 196 articles matched our search criteria and were identified through all data sources. After excluding articles reporting study designs other than randomised controlled trials (n=9153), 3043 records were screened for titles and abstracts. Thirteen abstracts were included and full texts were assessed. After removing all duplicates, we included five studies in this systematic review.26–30 A PRISMA (Preferred Reporting Items for Systematic Reviews and Meta- Analyses) flow diagram is shown in Figure 1.
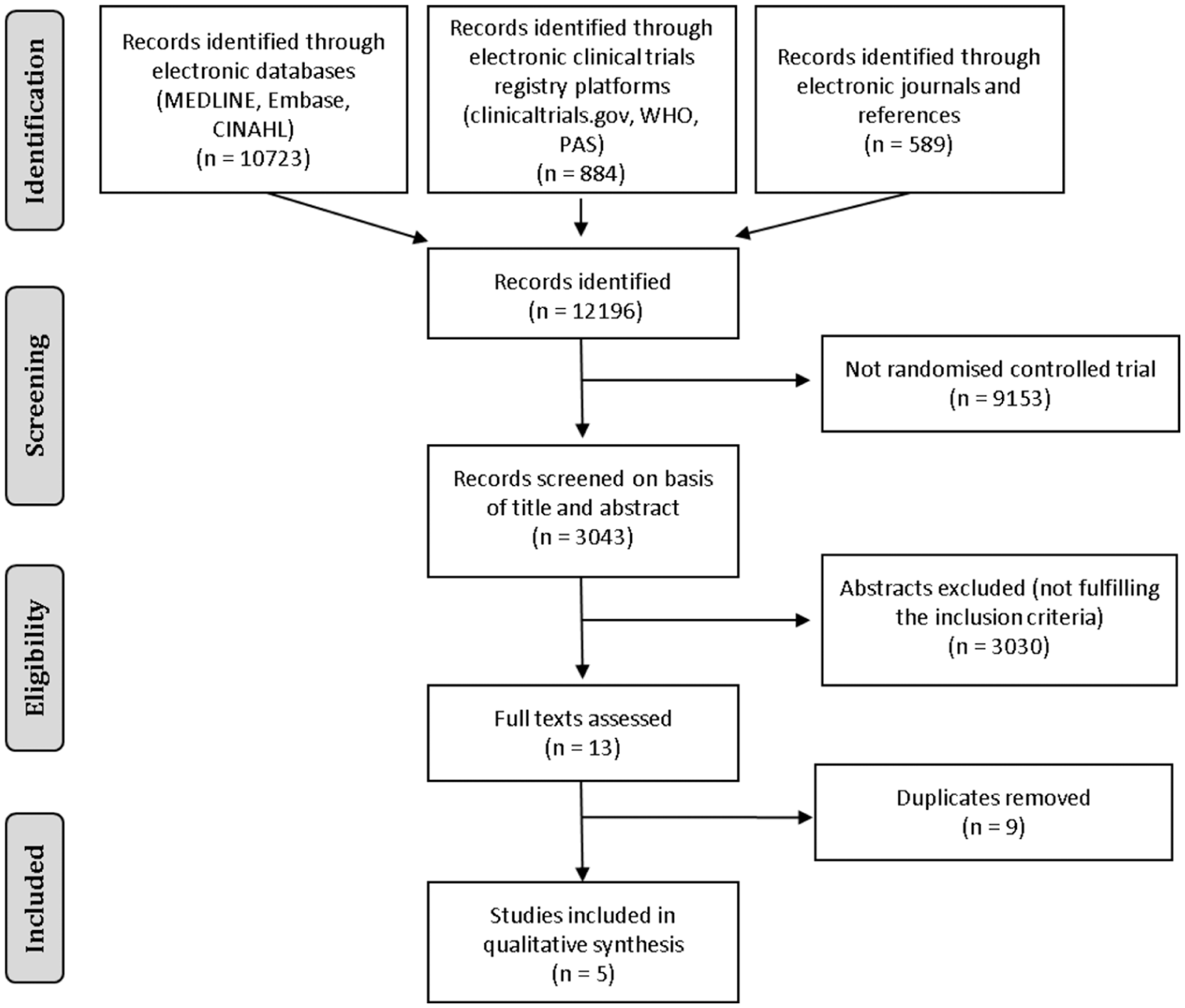
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram. WHO, World Health Organization; PAS, Pediatric Academic Societies.
Study characteristics and risk of bias assessment
Pain severity was assessed in three studies using the Premature Infant Pain Profile (PIPP)26,28,30 and in two studies using the Neonatal Infant Pain Scale (NIPS).27,29 The maximum PIPP score for preterm neonates is 21 points and for term neonates is 18 points. The NIPS score ranges from 0 to 7 points. Accordingly, the number of score points on the PIPP and NIPS score is directly proportional to the neonate’s pain intensity during the painful intervention.
All studies used a heel lance as the painful medical intervention. The study characteristics are stated as described in the original articles and are listed in Table 1.
Study characteristics of included trials
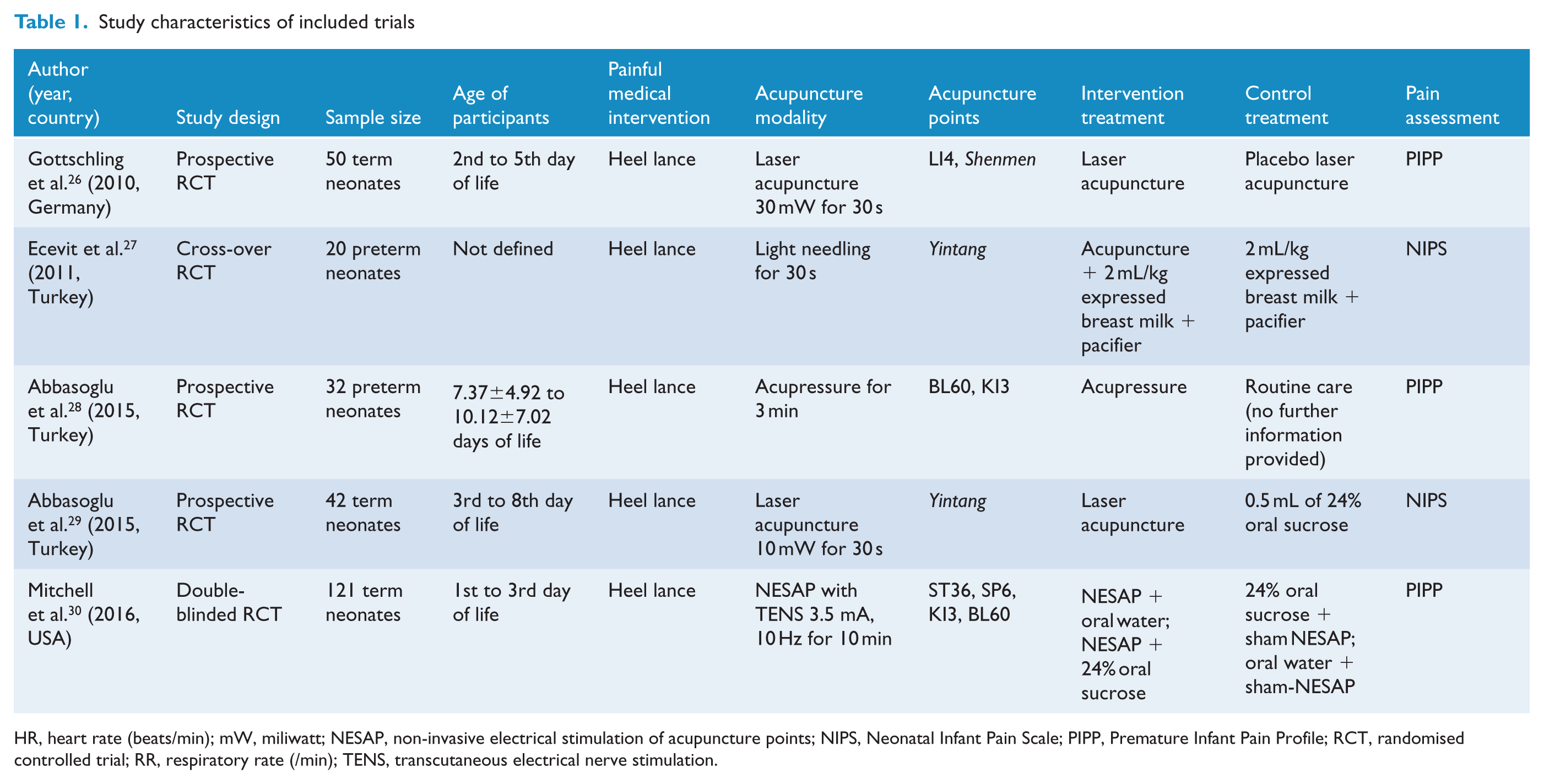
HR, heart rate (beats/min); mW, miliwatt; NESAP, non-invasive electrical stimulation of acupuncture points; NIPS, Neonatal Infant Pain Scale; PIPP, Premature Infant Pain Profile; RCT, randomised controlled trial; RR, respiratory rate (/min); TENS, transcutaneous electrical nerve stimulation.
Risk of bias within studies is summarised and described in detail in Table 2.
Risk of bias within studies
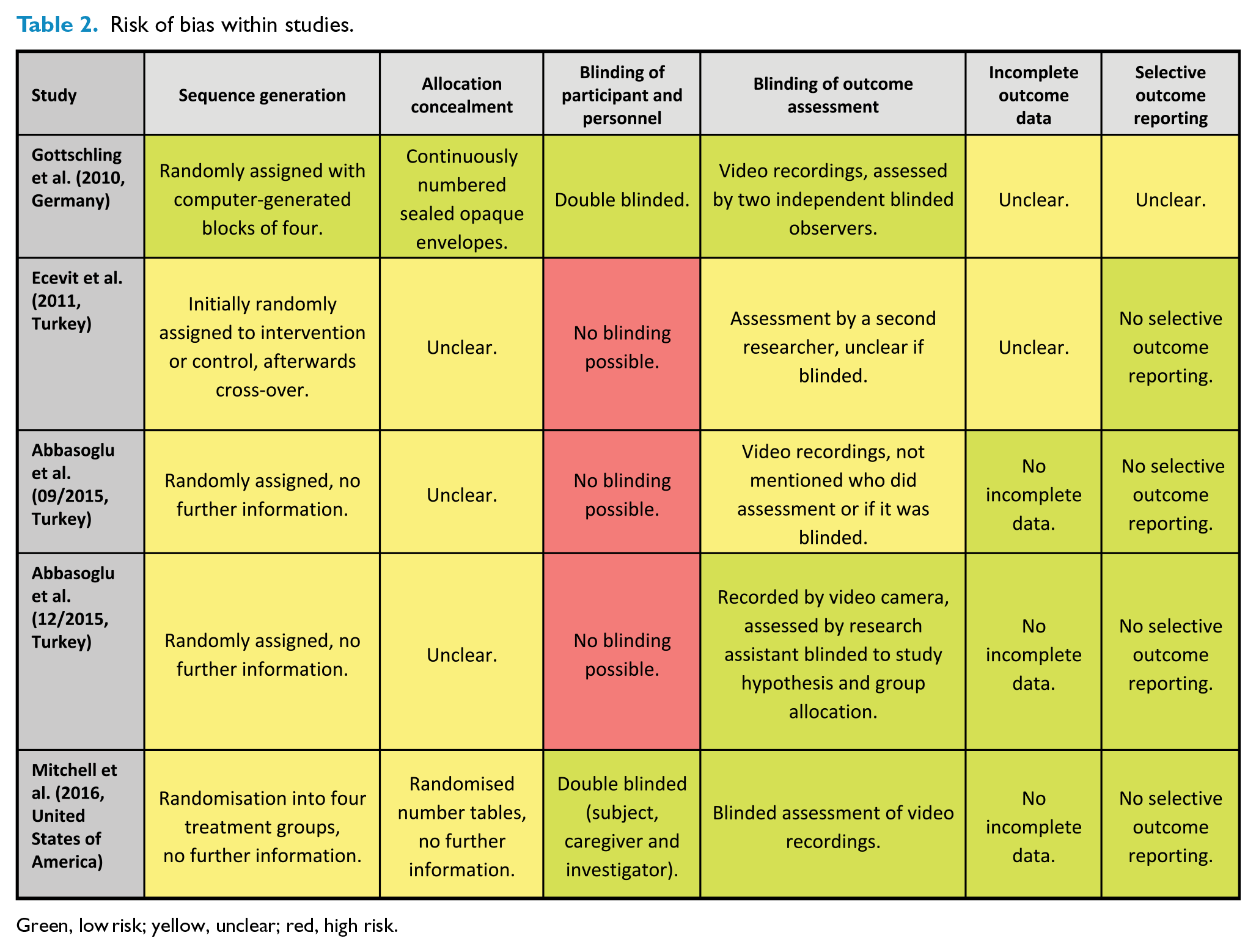
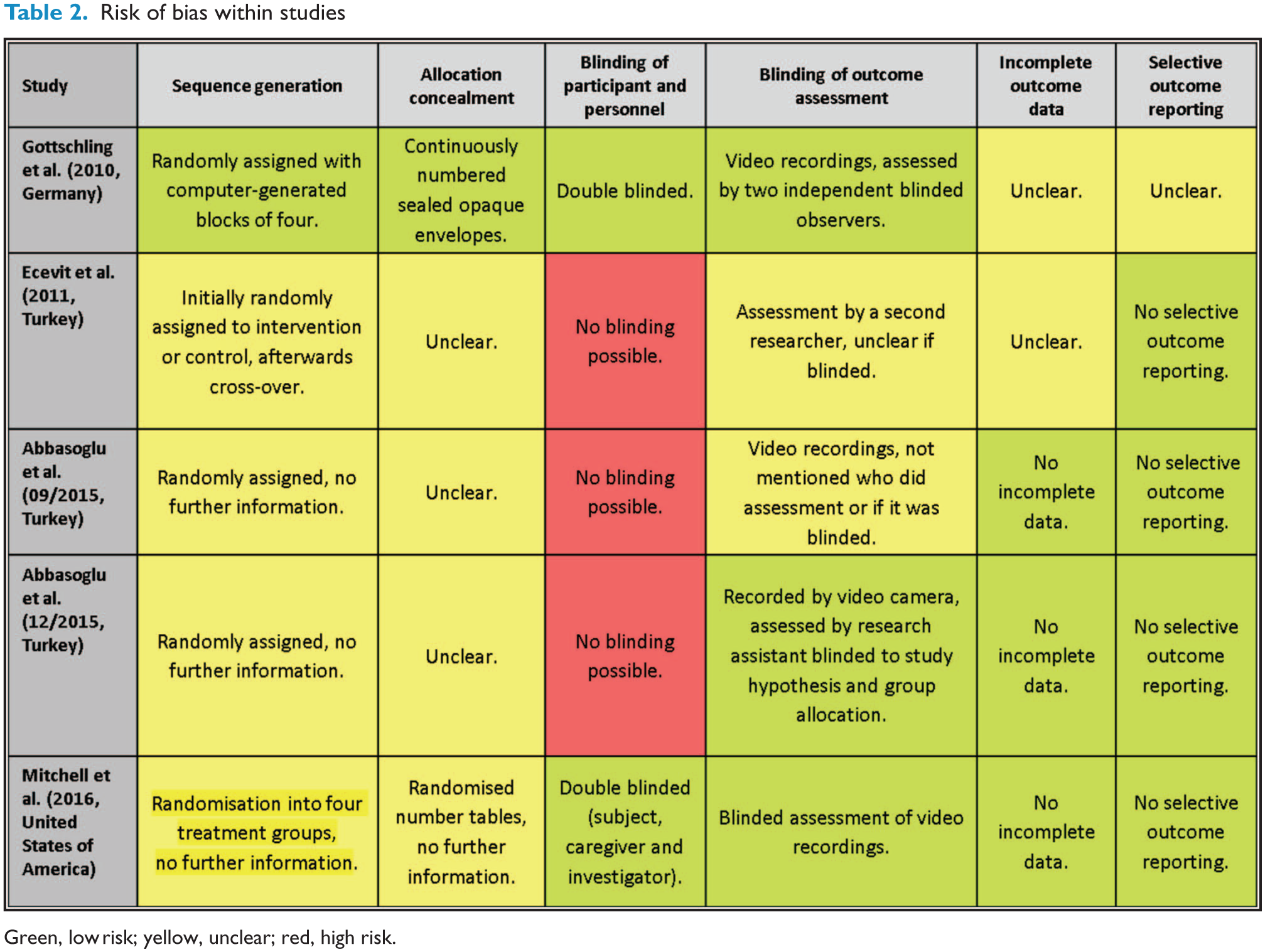
Green, low risk; yellow, unclear; red, high risk.
Synthesis of results
We identified significant heterogeneity for pain scores and therefore these results must be interpreted with caution. All trials assessed pain scores with a trend toward less pain in the acupuncture group (risk difference −0.74 (−2.26 to 0.79), with high heterogeneity (I2=87%)). Heterogeneity could only be calculated for comparable study designs. It was not possible to compare with Mitchell et al. 30 due to its four groups. Assessment of heterogeneity is shown in Figure 2.
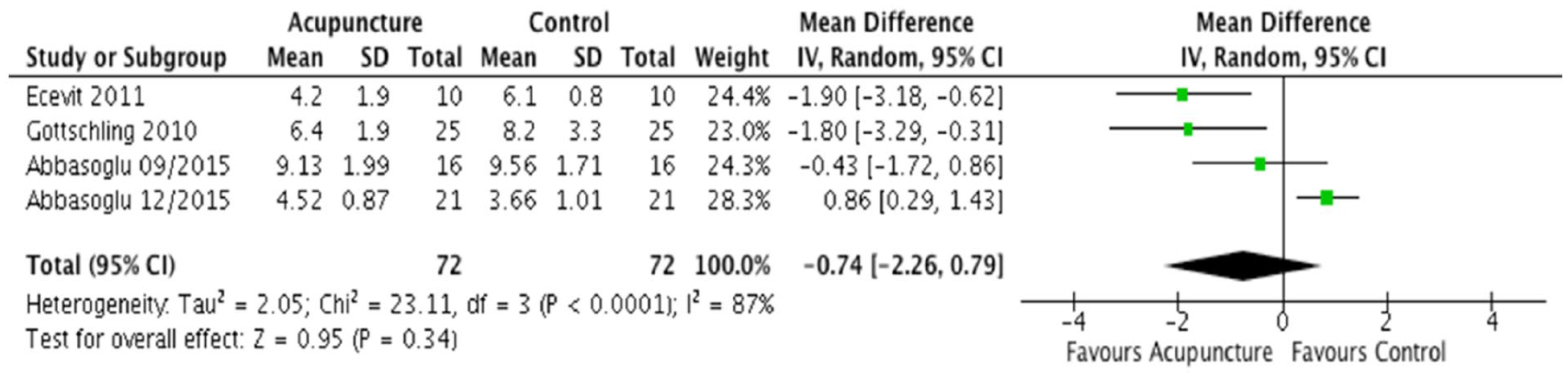
Heterogeneity assessment for outcome parameter pain score.
Results of individual studies
Results of individual studies are summarised and presented in Table 3.
Summarised results of individual studies

Green, low risk; yellow, unclear; red, high risk.
NESAP, non-invasive electrical stimulation of acupuncture points; NIPS, Neonatal Infant Pain Scale; PIPP, Premature Infant Pain Profile; RCT, randomised controlled trial.
Gottschling et al. 26 conducted a double blinded study using PIPP for pain assessment. The intervention group received laser acupuncture using a 30 mW soft laser (power density 3.8 W/cm2, 0.45 J/point, 830 nm) for 30 s at LI4 and at Shenmen, and the control group received placebo laser acupuncture. They designed it to be double-blind so the acupuncturist and the participant did not know if the laser was active (intervention group) or inactive (control group). The painful intervention was a heel lance for blood sampling for metabolic screening; it was not mentioned if a manual or automatic lancet was used. They showed significant differences between the intervention and control group favouring laser acupuncture (6.4±1.9 vs 8.2±3.3, P=0.013).
Ecevit et al. 27 designed a randomised crossover study and used NIPS as the pain score. The intervention group received light needling for 30 s at Yintang plus routine care, and the control group received routine care only (routine care was defined as 2 mL/kg expressed breast milk before heel lance and a pacifier). The painful intervention was heel lance for routine blood gas analysis done by the same person, who lanced the lateral portion of the heel (using a 30 gauge lancet). It was shown that the pain score in the intervention group was significantly lower than in the control group (4.2±1.9 vs 6.1±0.8, P<0.001).
The first study by Abbasoglu et al. 28 was a randomised clinical trial and used PIPP as the pain score. They compared acupressure for 3 min at BL60 and KI3 (intervention group) to routine care (control group, no further information given). The painful intervention was a heel lance to collect blood for routine screening performed by the same experienced nurse, although no further information regarding the lancet used was provided. There was no significant difference in the PIPP score between groups, with 9.13±1.99 in the intervention group and 9.56±1.71 in the control group (P=0.52).
The second trial by Abbasoglu et al. 29 was also a randomised controlled trial but used NIPS to assess pain levels in term neonates. The intervention group received laser acupuncture using a 10 mW (0.113 J/point, 905 nm) laser for 30 s at Yintang, while the control group was treated with 0.5 mL of 24% oral sucrose solution. The painful intervention was a heel lance for metabolic screening, performed by the same experienced nurse using a clearly defined manual lancet by Broche. In this study, the intervention group showed a significantly higher NIPS score than the control group (4.52±0.87 vs 3.66±1.01, P=0.006).
The study by Mitchell et al., 30 designed as double blinded, placebo controlled trial, assessed PIPP changes from baseline (defined as PIPP score before treatment) during heel lance for metabolic screening (no further information given). The study evaluated four groups (values stated in relative changes±SD): NESAP with 1 mL of 24% sucrose solution (3.6±1.2, P<0.05), NESAP with water (5.0±4.0, P<0.01), sham NESAP with 1 mL of 24% sucrose solution (4.0±1.8, P<0.05), and sham NESAP with water (4.9±4.0, P<0.01). The electrodes were placed at ST36, SP6, KI3 and BL60. This study showed that NESAP (3.5 mA, 10 Hz) alone is not effective at relieving pain during heel lance in neonates, but it is when administered in combination with oral sucrose solution.
Discussion
Acupuncture is a gentle treatment tool, yet it is a relatively new research field in children and neonates.31,32 Acupuncture treatment for pain in the paediatric population has been investigated in several studies, including headache, abdominal pain, fibromyalgia, juvenile arthritis, complex regional pain syndrome, cancer pain and perioperative pain. 33 In most cases, acupuncture has demonstrated a pain relieving effect and good acceptance by patients and parents, so it has been suggested as a safe and cost-effective treatment modality for paediatric pain.34,35
Therefore, our aim was to review the evidence regarding the efficacy of acupuncture for pain management in neonates and to evaluate the methodological quality of the available studies to improve future research in this area.
We found a variance of results across studies. Due to their heterogeneity, the results cannot be summarised to give a clear statement about the efficacy of acupuncture.
The reasons for heterogeneity are discussed in detail below.
Acupuncture modality and acupuncture points
Laser acupuncture applied using 30 mW at LI4 and Shenmen for 30 s produced a significant reduction in the PIPP score 26 ; however, laser acupuncture with 10 mW at Yintang for 30 s resulted in a significantly higher NIPS score. 29 It is relevant to note that Abbasoglu et al. 29 used a 10 mW laser, resulting in a lower energy dosage (0.113 J/point) than the laser used by Gottschling et al. 26 (30 mW; energy dosage 0.45 J/point). Both studies used different acupuncture points, which are not comparable due to location and potential effect.
The study by Mitchell et al. 30 was the first randomised controlled trial using NESAP for pain prevention in neonates. NESAP applied with TENS (3.5 mA, 10 Hz) at ST36, SP6, KI3 and BL60 before, during and after heel lance produced significantly higher pain scores than NESAP alone and lower pain scores than NESAP+sucrose solution. Comparing its results to current research, little is known about NESAP in neonates, infants and children, especially in the context of pain therapy.36,37 NESAP has been shown to be effective in the treatment of autistic children and the prevention of postoperative vomiting following paediatric tonsillectomy (NESAP with 20 Hz for 5 min).38,39
In one study by Abbasoglu et al., acupressure at KI3 and BL60 for 3 min led to no differences between groups. 28 Routine care provided to the control group was not specified, and therefore it is difficult to interpret these results. Acupressure on the heel may have a pain relieving effect due to a local vascular effect.40,41
Two studies used the same acupuncture point Yintang. In the study by Ecevit et al. 27 light needling for 30 s generated a significant pain reduction compared with laser acupuncture at Yintang, done by Abbasoglu et al. 29 A possible explanation for this could be the low energy dosage used, resulting in insufficient stimulation of tissues at the location of the acupuncture point.
Regarding acupuncture modalities and needling locations, there was high heterogeneity across the studies. The selected traditional acupuncture points differed in their locations and their applications. This variance in treatment potentially explains the different results in terms of pain scores across studies.
Pain scoring and the painful intervention
Influence of blinded versus not blinded pain scoring and inter-assessor variability might be a further confounder. Another reason for differences in pain score variability could be the heel lance itself. In some studies it was unclear how the heel lance was performed. Utilisation of an automatic or a manual lancet and individual practice discrepancies might have influenced reported pain scores. 42 Therefore comparison of painful stimuli (for example, intensity and duration) across studies seems to be impossible.
Control groups
We also observed significant heterogeneity across con-trol groups. Interventions were compared with sham acupuncture, sweet solutions and/or routine care. Glucose or sucrose solutions are commonly used as controls because of their effectiveness at reducing pain in neonates and safety as a short-term application.43,44 Therefore, sweet solutions seem to constitute appropriate active comparators to evaluate the effectiveness of acupuncture pain therapy.
Secondary outcome parameters
A secondary outcome parameter in four studies was the crying time during painful procedures.26,28–30 The assessment of crying time is a common surrogate parameter in trials of neonatal pain management.45,46 Two of the four studies demonstrated a significant reduction in crying duration in the acupuncture group.26,29
The study by Mitchell et al. 30 evaluated heart rate variability (HRV) and salivary cortisol levels as further markers. HRV did not show any significant differences before and after the heel lance between groups, although it has been used as a pain parameter in neonates in previous trials. 47 Due to difficulties in collecting adequate saliva, salivary cortisol levels were missing in ~50% of neonates and demonstrated no significant changes. 30
Blinding
Blinding in acupuncture trials with neonates is a difficult task. Usually, so-called ‘observer blinding’ is used to guarantee blinded assessment of the pain score. In two studies it was unclear whether the pain assessment was done blinded.27,28
Two authors conducted double blinded studies, meaning both the participant (the neonate) and the investigator were blinded.26,30 Both studies guaranteed a similar manipulation of the participant. The investigator was blinded due to the use of sham acupuncture. The study by Gottschling et al. 26 used laser acupuncture that was active in the intervention group and inactive in the control group. With this study design double blinding is possible, if the laser device is prepared so that everyone in the treatment room, including the acupuncturist, is unable to differentiate between the active and the placebo laser device.
In the study by Mitchell et al. 30 all neonates received the application of painless electrodes over the traditional acupuncture points, but in two groups it was switched on and in the other groups it was not. In two groups neonates received a pacifier with sucrose solution and in the other a pacifier with water in order to achieve blinding.
However, studies describing acupressure or needle acupuncture without sham interventions are unable to blind participants.
Safety
The efficacy of acupuncture for some diseases is promising and there have been no fatal side effects reported in children. 48 Furthermore, three recent reviews and some trials have suggested that acupuncture is a safe therapy in preterm and term neonates, in infants and in children.21,49–52 However, safety aspects were poorly reported in the reviewed trials. Only one trial clearly stated that no adverse events (AEs) occurred. 30
Accordingly, future studies should pay more attention to reporting on the safety of acupuncture, and should ideally report the occurrence and management of AEs to specify the relationship between AEs and acupuncture.
Furthermore, we found three ongoing trials examining acupuncture for pain management in neonates during our search in February 2017. These trials are currently being conducted in France, Australia and Austria. 53–55
Limitations
The main limitation of our results is the high heterogeneity across trials in terms of the acupuncture modality, acupuncture point selection, control groups and pain assessment. All included trials focused on pain management for a single heel lance, but not on pain relief for repeated minor painful procedures. Currently, there is no evidence to indicate whether acupuncture can be used repeatedly before periodic painful interventions. However, this would be an important application, because repetitive applications of ‘gold standard’ oral sweet solutions are associated with decreased effectiveness and can lead to hyperalgesia; furthermore, data on long-term outcomes are lacking.56,57
Conclusion
Due to heterogeneity of the acupuncture modality, traditional acupuncture point selection, control groups and pain scores, we could not perform a meta-analysis of the study results. According to the included studies, acupuncture may be a promising tool to reduce neonatal pain during minor painful interventions. Nevertheless, it would be important to provide a clear recommendation to add a new non-pharmacological therapy in pain management for clinical routine. However, further studies examining acupuncture-associated side effects, the safety and long-term effects of acupuncture, and a direct comparison of different acupuncture modalities and traditional acupuncture points are warranted.
Supplemental Material
AIM818673_Supplemental_material_SP1 – Supplemental material for Invasive and non-invasive acupuncture techniques for pain management in neonates: a systematic review
Supplemental material, AIM818673_Supplemental_material_SP1 for Invasive and non-invasive acupuncture techniques for pain management in neonates: a systematic review by Jasmin Stadler, Wolfgang Raith, Lukas P. Mileder, Georg M. Schmölzer and Berndt Urlesberger in Acupuncture in Medicine
Footnotes
Contributors
JS, WR and LPM conceptualised and designed the study, drafted the initial manuscript, and reviewed and revised the manuscript. JS and LPM collected data, carried out the initial analyses, and reviewed and revised the manuscript. JS, BU and GMS designed the data collection instruments, coordinated and supervised data collection, and critically reviewed the manuscript. GMS and JS performed statistical analysis. All authors approved the final version of the manuscript accepted for publication and agreed to be accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: JS is a fellow of the Doctoral School ‘Sustainable Health Research’ supported by the Medical University of Graz. JS is a recipient of DOC-med-fellowship of the Austrian Academy of Sciences at the Institute of the Medical University of Graz.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Patient consent
Not required.
Provenance and peer review
Not commissioned; externally peer reviewed.
Supplemental material
Supplemental material for this article is available online.