
Abstract
This study aimed to explore the protective potential of influenza vaccination against occurrence of dementia in patients with chronic obstructive pulmonary disease (COPD), who are expected to be more vulnerable to influenza infection. This nationwide retrospective cohort study enrolled patients with COPD (aged ≥60 years) from 1 January 2001 to 31 December 2012 by using the Taiwan National Health Insurance Research Database. By applying time-dependent Cox proportional hazard model, we used multivariate analysis to calculate the adjusted HR (aHR) with 95% CI of dementia in relation to influenza vaccination among patients with COPD. Besides, patients were partitioned into four groups according to the vaccination number (unvaccinated, 1, 2-3 and ≥4 total vaccinations) to investigate the dose-response effect of vaccinations on the dementia incidence. This cohort study included 19 848 patients with COPD, and 45% of them received influenza vaccination. The aHR of dementia was 0.68 (95% CI: 0.62 to 0.74, p<0.001) comparing vaccinated patients with unvaccinated ones. Furthermore, there was a trend of dementia risk reduction with the vaccination number. For patients who received 2-3 vaccinations, the aHR was 0.81 (95% CI: 0.73 to 0.90), and for those received 4 vaccinations, the aHR was 0.44 (95% CI: 0.40 to 0.50), with p for trend <0.001. In conclusion, annual influenza vaccination can reduce the risk of dementia in patient with COPD in a dose-dependent manner.
Keywords
Significance of this study
What is already known about this subject?
Many preceding researches indicate that patients with chronic obstructive pulmonary disease have increased risk of cognitive decline or dementia.
Frequent exacerbations of chronic obstructive pulmonary disease worsen the inflammatory status, which likely plays a pathogenic role in dementia.
Influenza virus infection is one of the major causes of chronic obstructive pulmonary disease exacerbations.
What are the new findings?
After adjustment multivariate analysis, the adjusted HR (aHR) of dementia was 0.68 (95% CI: 0.62 to 0.74, p<0.001) comparing vaccinated patients with unvaccinated ones.
There was a trend of dementia risk reduction with the vaccination number.
For patients who received 2-3 vaccinations, the aHR was 0.81 (95% CI: 0.73 to 0.90), and for those who received 4 vaccinations, the aHR was 0.44 (95% CI: 0.40 to 0.50), with p for trend <0.001.
Annual influenza vaccination may reduce dementia development in patients with chronic obstructive pulmonary disease with a dose-response effect.
How might these results change the focus of research or clinical practice?
The result further strengthens the rationale for influenza vaccination in patients with chronic obstructive pulmonary disease, which could be a good reference for guidelines.
Introduction
Chronic obstructive pulmonary disease (COPD) is a chronic systemic inflammatory disease1 with feature of progressive and partially reversible airflow limitation. It is caused mainly by exposure to noxious gases, most commonly tobacco smoking.2 The most obvious consequences of COPD are hypoxia and hypercapnia, which may worsen during period of exacerbation, together with underlying escalated inflammation status. COPD is related to many comorbidities such as lung cancer, cardiovascular disease (eg, ischemic heart disease, hypertension and atrial fibrillation), metabolic syndrome, diabetes, osteoporosis and peptic ulcer.3 Nowadays, COPD and its exacerbation are considered potentially treatable and preventable. Influenza vaccination is currently recommended to patients with COPD.4
Dementia comprises a wide range of symptoms, and the most characteristic ones are decline in memory and deficit in one or more cognitive functions. In addition, these impairments must cause daily activity performance reduction. Alzheimer's disease is the most common type of dementia.5 The risk of dementia increases with age and doubles every 5 years after 65 years of age.6 Hypoxia and inflammation contribute significantly to pathogenesis of dementia. Cardiovascular disease is also associated with dementia. Many preceding researches indicate that patients with COPD have increased risk of cognitive decline or dementia.7 This was confirmed by a recent meta-analysis, in which COPD exacerbation was particularly strongly correlated with this cognitive dysfunction.8
The major cause of COPD exacerbations is viral or bacterial infection. Although rhinoviruses are most common viruses related to exacerbations of COPD, influenza viruses infection is more common in hospitalized patient due to sever exacerbation.9 There are some evidences from randomized trials showing that inactivated influenza vaccine can decrease exacerbations of COPD, especially those caused by influenza virus itself.10 Verreault et al demonstrated that previous vaccination against various viruses including influenza might prevent from subsequent Alzheimer's disease.11 Here, to explore the protective potential of influenza vaccination against occurrence of dementia in patients with COPD, who are expected to be more vulnerable to influenza infection, we initiated a nationwide retrospective cohort study using Taiwan National Health Insurance Research Database (NHIRD).
Materials and methods
Taiwan launched National Health Insurance (NHI) program in 1995, and today 98% of >23 million residents are under comprehensive health insurance coverage. In this research, we used the medical records of randomly sampled 1 000 000 beneficiaries enrolled in year 2000 from the Taiwan's NHIRD. The statistical characteristics of the sample group were similar to the population. All personal information in the sample group is scrambled and de-identified to protect privacy.
Study design and patients
We used International Classification of Diseases, ninth revision, Clinical Modification (ICD-9-CM) codes to enroll all patients with a diagnosis of COPD in the sample group from 1 January 2001 to 31 December 2012. The initial cohort number was 100 317. Patients without a succeeding emergency or outpatient department visit, or hospitalization with a diagnosis of COPD in the following 1 year (n=42 845) were excluded because of the uncertainty of COPD diagnosis. Step by step, we also excluded patients aged <60 years (n=31 348), with a dementia-related diagnosis before the enrollment date (n=2986) and with influenza vaccination in the period of 6 months before the enrollment date (n=3200) (figure 1).
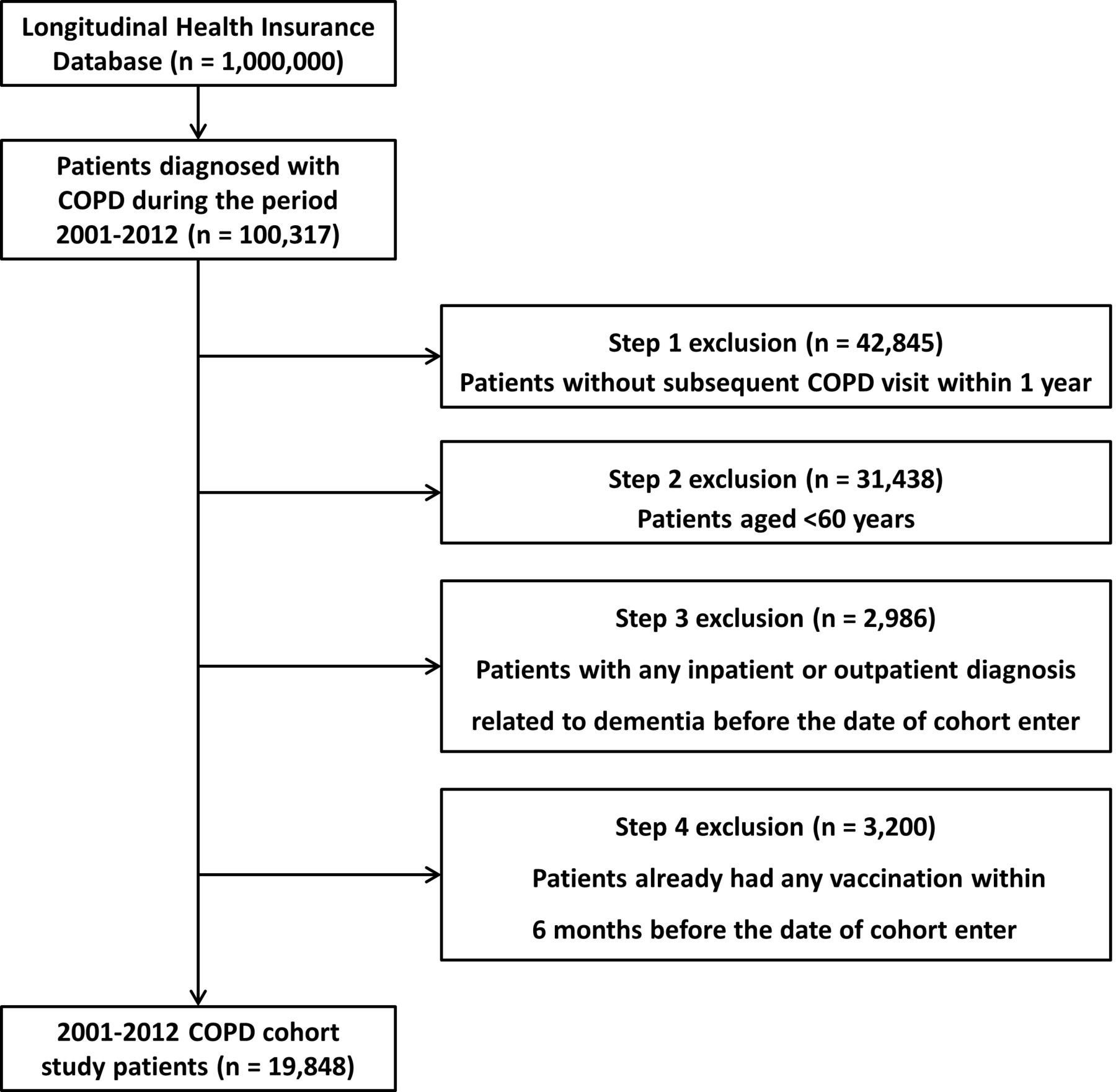
Patient selection process. COPD, chronic obstructive pulmonary disease.
Statistical methods
In Taiwan, the government has been offering free annual influenza vaccination for citizens older than 50 years with systemic diseases such as chronic pulmonary diseases, cardiovascular diseases, chronic hepatitis, liver cirrhosis or type 2 diabetes mellitus since 1998. From 2001, the coverage was broadened to include all people aged ≥65 years. In this study, the vaccination history was recognized by the ICD-9-CM code V048 or by vaccine drug codes. Records related to the risk of dementia or protective factors according to previous study12 were also retrieved: age and sex; number of COPD-related hospitalization; the comorbidities of diabetes, cerebrovascular diseases, hypertension, dyslipidemia, parkinsonism, epilepsy, substance use and alcohol disorders, mood disorder, anxiety disorder, psychotic disorder and sleep disorder; statin, metformin, renin-angiotensin-aldosterone system inhibitors (RAASI, including angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers) and aspirin use; urbanization level and monthly income. The χ2 test was used to evaluate the differences between the vaccinated and unvaccinated groups in these variables.
We included vaccination status along with other variables (number of COPD-related hospitalization, age, sex, diabetes, hypertension, dyslipidemia, cerebrovascular diseases, parkinsonism, epilepsy, substance use and alcohol disorder, mood disorder, anxiety disorder, psychotic disorder, sleep disorder, level of urbanization, monthly income) in a multivariate analysis and determined whether vaccination status had a significant effect in reducing dementia incidence. The end point was the occurrence of dementia (ICD-9-CM codes 290.0, 290.1x, 290.2x, 290.3, 290.4x, 294.1, 331.0, 331.1 and 331.2) in patients with COPD during the follow-up years. The cumulative incidence of dementia in vaccinated and unvaccinated patients with COPD was evaluated by the Kaplan-Meier method. By applying a time-dependent Cox proportional hazard model, we evaluated the HRs and 95% CI of dementia among vaccinated patients with COPD when compared with unvaccinated patients with COPD. The HRs were adjusted by using multivariate analysis. To evaluate the effect of vaccination, we made cohort stratification on age and sex first. For further evaluation, we also stratified dementia into three groups: Alzheimer's dementia (ICD-9-CM codes 331.0), vascular dementia (ICD-9-CM codes 290.4x) and others.
In addition, to investigate the dose effect of vaccinations on the dementia incidence, patients were partitioned into four groups according to the vaccination number (unvaccinated, 1, 2-3 and ≥4 total vaccinations). Sensitivity analysis was applied, and adjustments were made to evaluate the association of number of COPD-related hospitalization, age, sex, diabetes, dyslipidemia, hypertension, cerebrovascular diseases, anxiety disorder, statin use, metformin use, RAASI use and aspirin use with the incidence of dementia by different models.
We performed all of the analyses by SAS V.9.3 software. A p value of <0.05 was considered to be statistically significant if not otherwise specified.
Results
Table 1 demonstrates the characteristic of the study patients. This cohort study contained 19 848 patients with COPD, of which 45% (n=8868) received influenza vaccination while 55% (n=10 980) did not. Compared with vaccinated patients, unvaccinated patients displayed a significantly higher percentage of comorbidities including diabetes (p=0.004), cerebrovascular diseases (p<0.001) and sleep disorder (p<0.001). By contrast, vaccinated patients displayed a significantly higher percentage of medical comorbidities including parkinsonism (p<0.001) and mood disorder (p<0.001). Besides, there were significant differences in the monthly income, and urbanization level as well as statin, metformin, RAASI and aspirin use between vaccinated and unvaccinated subgroups.
Characteristic of the sample population
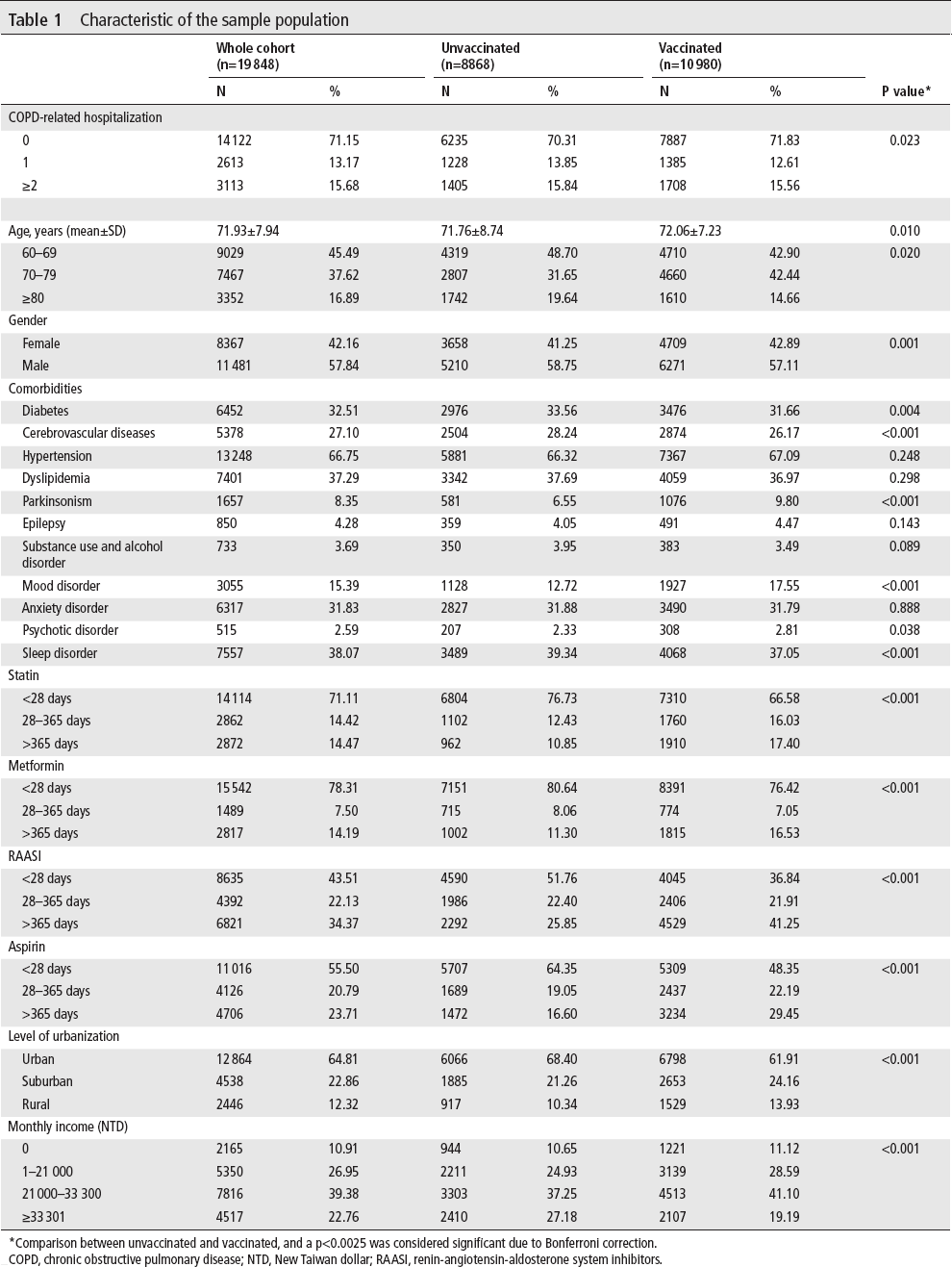
Comparison between unvaccinated and vaccinated, and a p<0.0025 was considered significant due to Bonferroni correction.
COPD, chronic obstructive pulmonary disease; NTD, New Taiwan dollar; RAASI, renin-angiotensin-aldosterone system inhibitors.
Table 2 shows the risk of dementia between the unvaccinated and vaccinated patients with COPD. The overall follow-up period was 34 898.8 and 73 535.9 person-years for unvaccinated and vaccinated patients, respectively. By applying multivariable analysis, the adjusted HR (aHR) of dementia between vaccinated patients and unvaccinated patients was 0.68 (95% CI: 0.62 to 0.74, p<0.001). The Kaplan-Meier estimation of cumulative dementia rate in the unvaccinated group was significantly higher than that in the vaccinated group (log-rank p<0.0001) as shown in figure 2. Further stratified analysis on dementia type shows that there is significant aHR reduction in vascular dementia as opposed to Alzheimer's dementia.
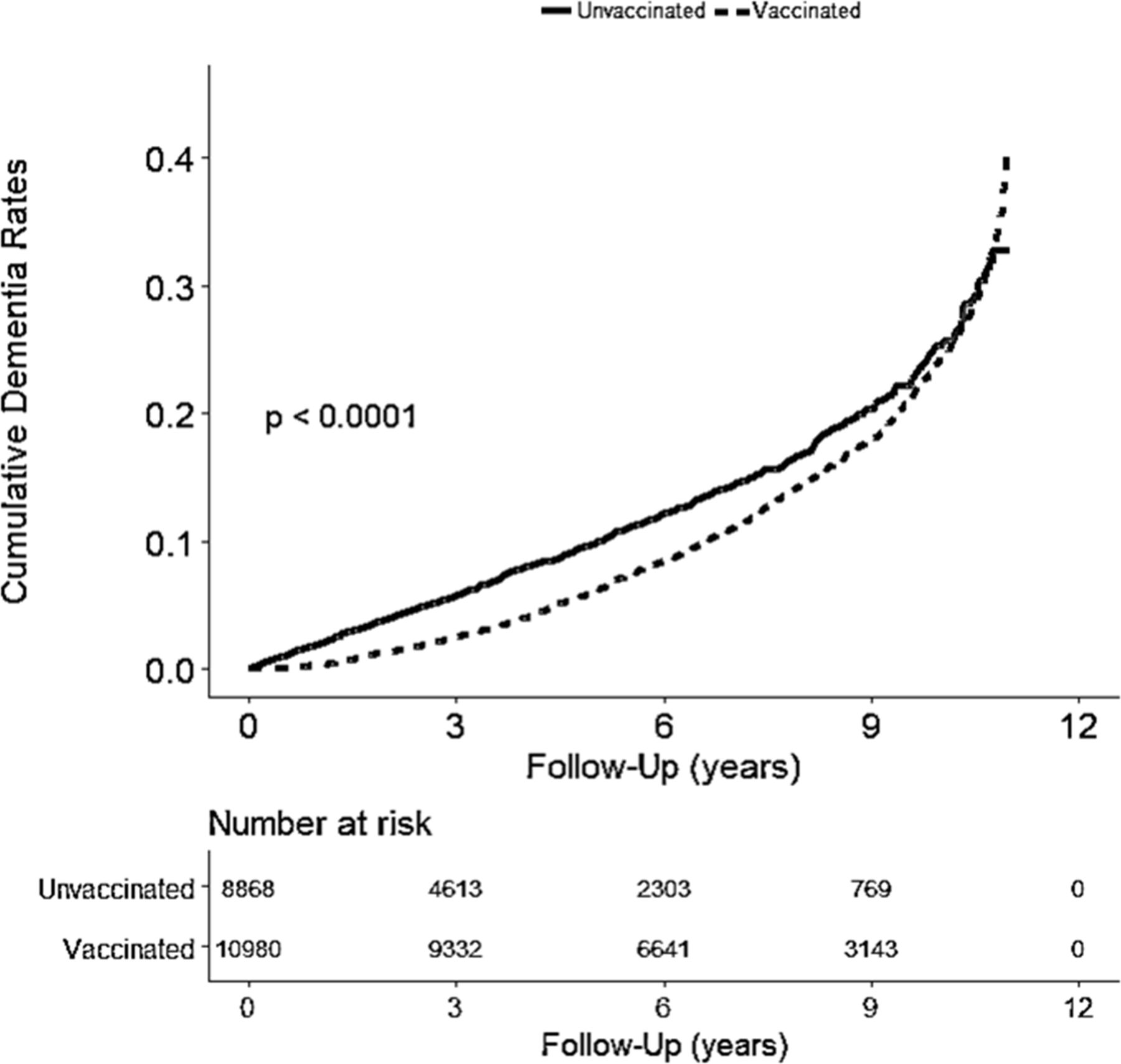
Cumulative dementia rates in elderly patients with chronic obstructive pulmonary disease in Taiwan (n=19 848) from 1 January 2001 to 31 December 2012 stratified according to vaccination status (log-rank test, χ2=37.342; df=1; p<0.0001).
Risk of dementia among unvaccinated and vaccinated in study cohort
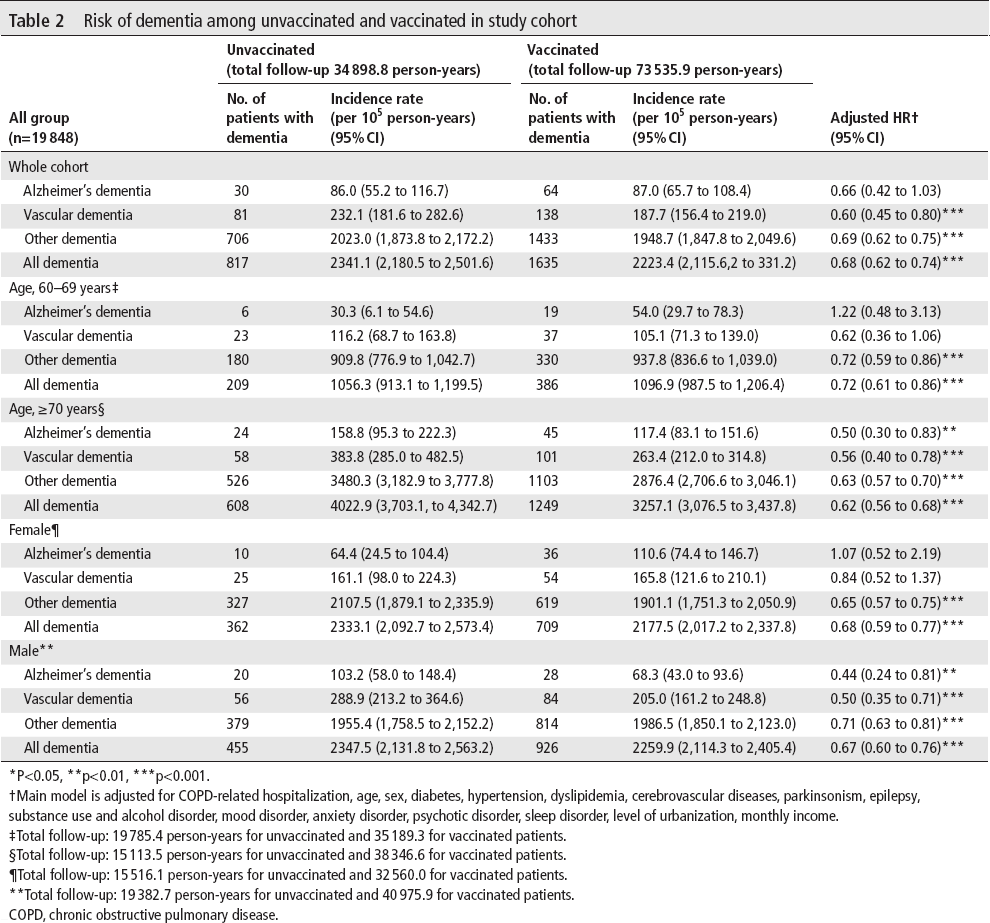
P<0.05, **p<0.01, ***p<0.001.
Main model is adjusted for COPD-related hospitalization, age, sex, diabetes, hypertension, dyslipidemia, cerebrovascular diseases, parkinsonism, epilepsy, substance use and alcohol disorder, mood disorder, anxiety disorder, psychotic disorder, sleep disorder, level of urbanization, monthly income.
Total follow-up: 19 785.4 person-years for unvaccinated and 35 189.3 for vaccinated patients.
Total follow-up: 15 113.5 person-years for unvaccinated and 38 346.6 for vaccinated patients.
Total follow-up: 15 516.1 person-years for unvaccinated and 32 560.0 for vaccinated patients.
Total follow-up: 19 382.7 person-years for unvaccinated and 40 975.9 for vaccinated patients.
COPD, chronic obstructive pulmonary disease.
Table 3 shows predictors of dementia in patients with COPD besides vaccination status. The other significant predictors are age, comorbidities such as diabetes, cardiovascular diseases, hypertension, parkinsonism, epilepsy, substance use and alcohol disorder, psychotic disorder and sleep disorder.
Predictors of dementia in patients with COPD
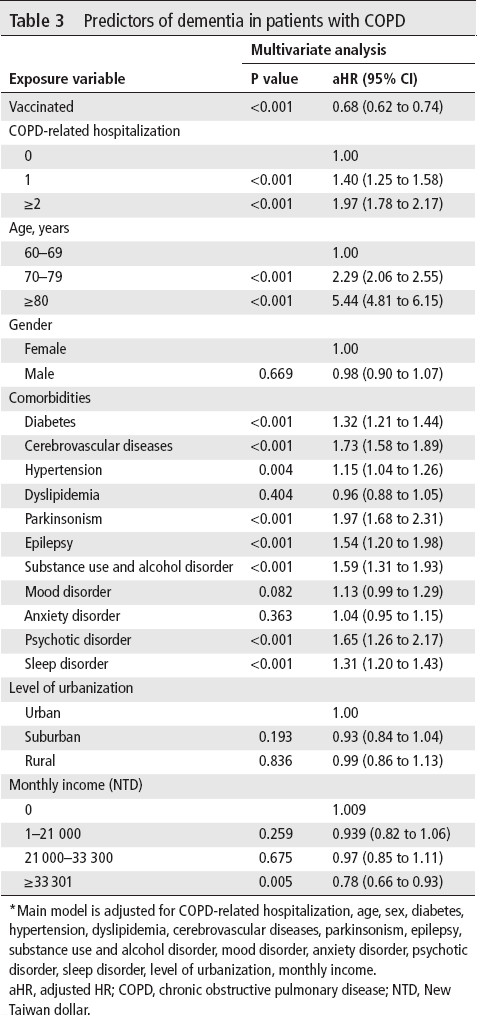
Main model is adjusted for COPD-related hospitalization, age, sex, diabetes, hypertension, dyslipidemia, cerebrovascular diseases, parkinsonism, epilepsy, substance use and alcohol disorder, mood disorder, anxiety disorder, psychotic disorder, sleep disorder, level of urbanization, monthly income.
aHR, adjusted HR; COPD, chronic obstructive pulmonary disease; NTD, New Taiwan dollar.
Table 4 shows the trend of dementia risk reduction with the vaccination number in the main model. For patients who received 2-3 vaccinations, the aHR was 0.81 (95% CI: 0.73 to 0.90), and for those who received 4 vaccinations, the aHR was 0.44 (95% CI: 0.40 to 0.50), with p for trend <0.001. In the sensitivity analysis by addition of covariates such as statin, metformin, RAASI or aspirin use to the main model, vaccination remained as an independent protective factor and reduced dementia in patients with COPD in a dose-dependent way. For the subgroup effects evaluation, the protective and dose effects were more predominant in patients with number of COPD-related hospitalization ≤1, aged ≥70 years and less statin, metformin, RAASI and aspirin using days (<28 days).
Sensitivity analysis of adjusted HRs of vaccination in risk reduction of dementia
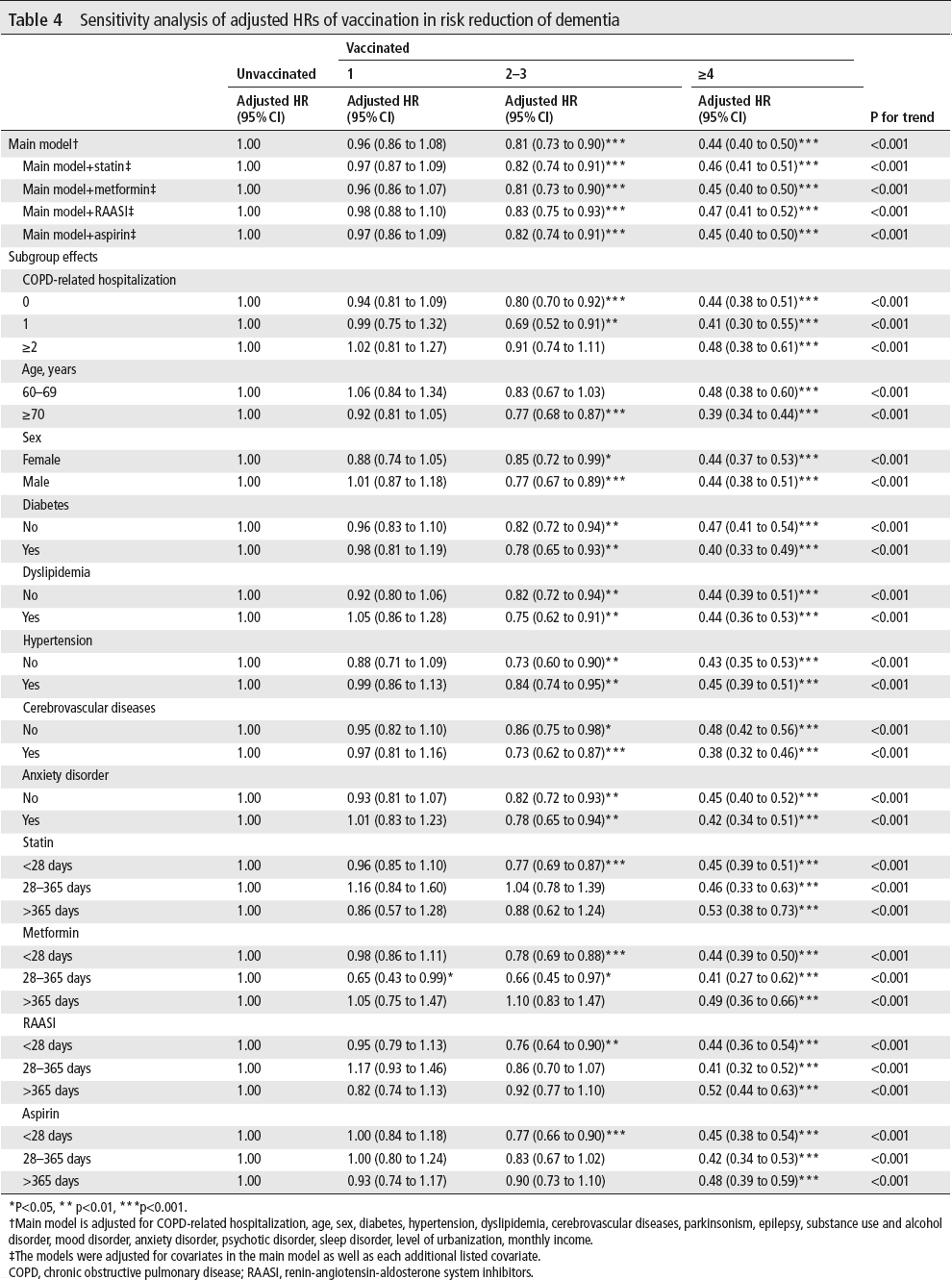
P<0.05, ** p<0.01, ***p<0.001.
Main model is adjusted for COPD-related hospitalization, age, sex, diabetes, hypertension, dyslipidemia, cerebrovascular diseases, parkinsonism, epilepsy, substance use and alcohol disorder, mood disorder, anxiety disorder, psychotic disorder, sleep disorder, level of urbanization, monthly income.
The models were adjusted for covariates in the main model as well as each additional listed covariate.
COPD, chronic obstructive pulmonary disease; RAASI, renin-angiotensin-aldosterone system inhibitors.
Discussion
This nationwide retrospective cohort study found a risk reduction of dementia among patients with COPD who had received influenza vaccination. COPD is with multiple systemic consequences and comorbidities,13–15 including cardiovascular disease, metabolic disease, bone disease, psychiatric disease, infectious disease and lung cancer. Many studies have focused on the cognitive dysfunction—a subset of psychiatric disease in patients with COPD, and displayed some connections between these two diseases.16–27 In most studies on the relationship between COPD and cognitive function, impairments in either global or domains such as memory, attention, perception, executive and motor functions have been demonstrated.7 It appears that COPD is associated with dementia.20 21
Several mechanisms of cognitive impairment in COPD have been proposed.7 25 28 They are related to etiology, pathophysiology and comorbidity of COPD, like smoking, hypoxia, systemic inflammation and cardiovascular disease. Smoking is the major cause of COPD. Brain MRI revealed it is associated with frontal grey mater volume reduction, preclinical brain change such as silent stroke and atrophy.29 30 Cigarette contains some neurotoxic components and may cause direct brain damage, with a consequence of Alzheimer's disease.30 31 Smoking precipitates cerebral hypoxia and may also reduce cognitive function.32 Hypoxia is related to declines in all domains of cognitive function.32 Compared with non-hypoxemic patient, hypoxemic patient showed poorer cognitive performance.33 Deficiency of neurotransmitters related to oxygen-dependent enzymes during hypoxemia may be the underlining pathogenesis.28 34 The level of inflammatory markers C reactive protein and interleukin-6 elevate in patients with COPD. This implies that inflammation may also play role in the cognitive impairment.35 36 Inflammation leads to elevated cytokine levels, alternation in coagulation balance and platelet dysfunction. These changes might promote thrombotic tendency or cause endothelial damage. Cardiovascular diseases result in cerebrovascular hypoperfusion and microemboli to the brain.37 There is also an association between hypertension and cognitive decline in elderly people.38 Advanced brain imaging facilities including high-resolution MRI, diffusion tenser imaging, functional MRI and MRI spectroscopy have demonstrated direct evidence of brain structure and functional alternations in patients with COPD,28 such as cerebral microbleeds,39 white matter microstructural damage40 and cerebral metabolism.41 One of our results that there is significant aHR reduction in vascular dementia is compatible to these findings.
Table 3 shows that the number of COPD-related hospitalization and was a significant predictor of dementia development. Table 4 shows that the protective and dose effects were more predominant (the aHR is significant only by 2-3 vaccinations) in patients with number of COPD-related hospitalization ≤1. This means that the stronger predictor for dementia development, the higher vaccination number is needed to achieve protective effect, in other words, more vaccinations has more potent protection for dementia development in patients with COPD.
Singh et al found that patients with COPD history >5 years have the risk of developing mild cognitive impairment in a time-dependent relationship.25 26 Schou et al demonstrated that cognitive dysfunction is related to the severity of COPD in patients with severe to very severe COPD.24 Crisan et al also described the significant cognitive status deterioration in advanced stage of COPD, and notably after exacerbation episode.16 These findings provide reasons for more early and more aggressively interventions against COPD to prevent the development of cognitive dysfunction. COPD and its comorbidities exert negative impaction on dementia. From another point of view, dementia results in poor quality of life and decreases the patient's ability of COPD self-management.42 Influenza vaccination can decrease incidence of hospitalization and mortality.43 Annual influenza vaccination is currently recommended to patients with COPD4 as cumulative evidences reveal that inactivated influenza vaccine can decrease exacerbations of COPD.10 Lower probability of exposure in inflammatory and hypoxic status is expected, and this may reduce dementia development. Studies also showed influenza vaccination is related to diminished cerebrovascular events,44 45 which is closely related to dementia occurrence. More specifically, Verreault et al has demonstrated that previous influenza vaccination may prevent from subsequent Alzheimer's disease.11 It is plausible that influenza vaccination has synergistic protective effect against dementia in patients with COPD. This effect might be further enhanced with increasing vaccination number.
The strength of this research is the large sample size by using a nationwide papulation-based data to explore the protective potential of influenza vaccination against dementia in patients with COPD. However, there are some limitations that should be considered. First, the diagnoses of COPD, dementia and related comorbidities were exclusively based on ICD-9 codes made by doctors for insurance claims. The diagnostic accuracy from the database should be taken into account. However, the claim records in the NHIRD have been validated.46 Also, the NHI administration retrieved medical records randomly for diagnosis validation. Hospitals will subject to heavy penalty once inadequate ICD-9 coding was found. Second, several confounding factors such as smoking status, alcohol drinking, other over-the-counter drugs using, body mass index and severity of COPD were unavailable in the NHIRD. Lastly, this study is not a prospective randomized controlled trial, therefore, the firm cause and effect relationship between influenza vaccination and protective effect against dementia in patients with COPD could not be established.
Conclusion
In this study, we first demonstrate that influenza vaccination may reduce dementia development in patients with COPD, particularly in patients with vascular dementia. A dose-response effect of the number of vaccination was also observed. Further prospective study is required to clarify the underlying mechanism.
Footnotes
Contributors
J-CL and K-YL were involved in the conception and design of the study. C-SL and Y-AF contributed to data acquisition and analysis. C-SL drafted the manuscript. C-CC, J-CL and K-YL provided the final revision. All authors provided final approval of the version to be published.
Funding
The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests
None declared.
Patient consent for publication
Not required.
Ethics approval
The study design was approved by Taipei Medical University Joint Institutional Review Board (N201708051).
Provenance and peer review
Not commissioned; externally peer reviewed.
Data availability statement
All data relevant to the study are included in the article.