
Abstract
Postural orthostatic tachycardia syndrome (POTS) is estimated to impact millions of people each year. However, there is no established gold standard for its treatment. Bupropion is a norepinephrine and a dopamine reuptake inhibitor and has been implicated as a potential treatment for POTS. We performed a non-randomized retrospective chart review on 47 patients with POTS with statistical analysis evaluating for significant findings including reduced orthostasis and improvement of symptoms with the use of bupropion. Bupropion was not associated with a statistically significant improvement in orthostatic vitals but there was an overall reduction in reported syncope. While the use of bupropion does not show a statistically significant impact on orthostatic vitals in patients with POTS, it did show a degree of improvement in syncope and as such might be useful in patients with syncope-predominant POTS.
Significance of this study
What is already known about this subject?
Postural orthostatic tachycardia syndrome (POTS) has no established gold standard for its treatment.
Most current treatment options have not shown substantial benefit in symptom reduction.
POTS symptoms can be devastating and greatly reduce quality of life.
What are the new findings?
Bupropion may help reduce syncopal events in this patient population.
Bupropion may benefit patients with POTS and syncope-predominant POTS.
Bupropion did not show any significant impact on orthostatic vital signs.
How might these results change the focus of research or clinical practice?
The results from this study can help medical professionals in treating patients with POTS. Current therapies are limited and have not shown good clinical outcomes in symptom reduction in this population. This study will allow clinicians to use another medication which may help in syncope-predominant POTS.
Introduction
Postural orthostatic tachycardia syndrome (POTS) is characterized by chronic orthostatic intolerance associated with a dramatic and inappropriate increase in heart rate (HR) on standing. More specifically, this refers to a HR increase of at least 30 beats per minute (bpm) or a rate that is greater than 120 bpm after standing with the absence of orthostatic hypotension. These patients can present with a wide range of symptoms, most typically including fatigue, headaches, difficulty with concentration, palpitations, shortness of breath, chest discomfort and light-headedness. More severe cases tend to present with syncope. Of note, patients with POTS do not typically present with orthostatic hypotension (a drop in systolic blood pressure >20 mm Hg or diastolic blood pressure >10 mm Hg within 3 minutes of standing). The cause behind POTS is unclear but there have been multiple proposed etiologies with most mechanisms related to the development of autonomic dysfunction in the form of abnormal venous pooling, baroreflex abnormalities and increased sympathetic response. Studies have also proposed connective tissue disorders, postviral illnesses and autoimmune disorders as triggers for the development of POTS.1–3 As documented in previous studies, managing POTS requires a multidisciplinary approach including non-pharmacologic (ie, lifestyle modifications in the form of exercise programs, compression stockings and increased salt and water intake) and pharmacologic therapies. Patients typically require several trials of different pharmacologic therapies but there does not appear to have been any uniformly successful pharmacologic agent in the management of POTS. The exact mechanism of action by which bupropion works is not entirely clear. What is known is that bupropion enhances both noradrenergic and dopaminergic neurotransmission via reuptake inhibition of the norepinephrine transporter and the dopamine transporter. This may provide some assistance with the autonomic dysregulation that patients with POTS experience. In this study we report our single-center experience with bupropion in patients with POTS. This is the first study to examine bupropion in patients with POTS.
Materials and methods
The objective data were collected via chart review (i.e. orthostatic vitals, medications taken, initial symptoms on presentation). Subsequent subjective data (ie, response to treatment) were obtained in the form of a phone interview. Consent was obtained verbally; no written consent was obtained given the retrospective nature of the study.
Our study includes all patients who were seen at the Syncope and Autonomic Disorders Clinic with an established diagnosis of POTS and who were currently or previously treated with bupropion for this diagnosis. Patients were diagnosed with POTS based on positive orthostatic vitals (ie, increase in HR of 30 bpm or more that occurs within the first 10 minutes of standing) or positive upright tilt table test. Of note, many patients were referred to our clinic from outside institutions with a previous diagnosis of POTS.
Chart review consisted of obtaining demographic data and comorbidities, as well as current and past medications. Follow-up was done via phone interview; of the 194 eligible patients who were contacted, 47 agreed to participate in the phone interview. Statistical analysis was performed using SPSS V.21.0 software (IBM); two-tailed p value <0.05 was considered statistically significant.
Results
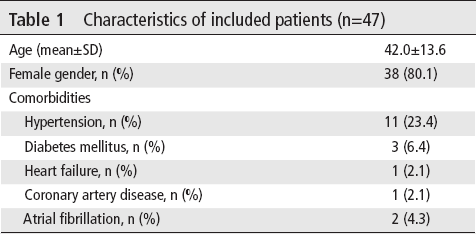
A total of 194 patients met POTS criteria and were currently or previously treated with bupropion who were included in the study. The patients were contacted to participate in the study and 47 patients agreed to participate via verbal consent (table 1).
Characteristics of included patients (n=47)
Bupropion is usually started at a dose of 150 mg once daily and can typically be titrated to a dose of 300 mg; on occasion patients have been prescribed 450 mg daily. This dose can be titrated up according to symptoms and subsequent response to treatment. Selective serotonin reuptake inhibitors (SSRI) and selective norepinephrine reuptake inhibitors (SNRI) were the most commonly prescribed medications taken prior starting bupropion. 76.6% of patients reported taking SSRIs and SNRIs prior to starting bupropion and 44.7% of patients reported taking beta blockers and calcium channel blockers prior to starting bupropion. Seventeen per cent of patients were on dextroamphetamines/amphetamines, midodrine and pyridostigmine prior to starting treatment with bupropion (table 2).
Medication taken by patients before starting bupropion
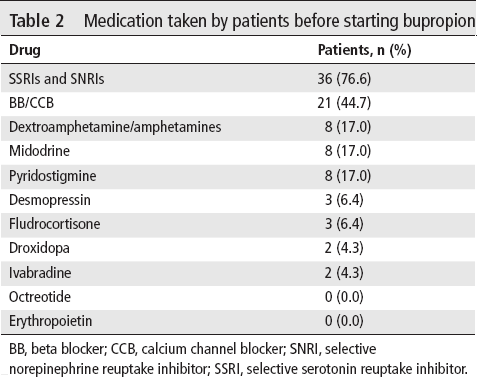
BB, beta blocker; CCB, calcium channel blocker; SNRI, selective norepinephrine reuptake inhibitor; SSRI, selective serotonin reuptake inhibitor.
Follow-up vital signs were available for all 47 patients after initiating treatment with bupropion. Based on our data, bupropion does not appear to have any statistically significant effect on orthostatic vitals. HR while sitting was 81.1±14.4 vs 82.7±15.3 (p=0.51); similarly, bupropion does not appear to have a statistically significant effect on standing HR (87.2±16.9 vs 92.4±16.2, p=0.81). Finally, there does not appear to be any statistically significant effect of bupropion on BP, sitting or standing (table 3).
Vital signs of patients before and after starting bupropion
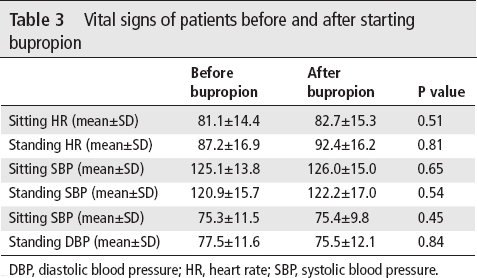
DBP, diastolic blood pressure; HR, heart rate; SBP, systolic blood pressure.
The most responsive symptom to treatment appears to be syncope. Out of 47 patients, 36 reported experiencing syncope. Of these 36 patients, 21 reported no further episodes of syncope and 15 continued to experience syncope, thus representing an overall 60% positive response rate. Patients did not report overall improvement in light-headedness, fatigue, palpitations, headache, exercise intolerance, trouble concentrating and vision changes (figure 1).
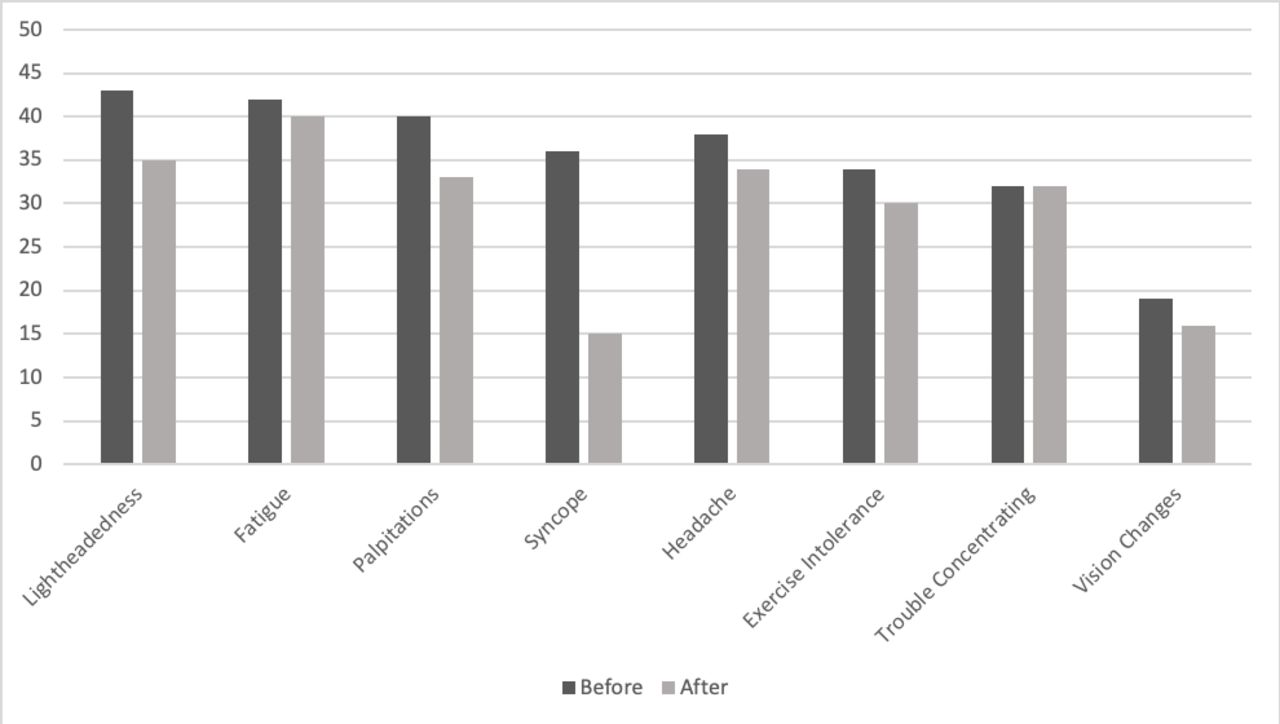
Number of patients reporting symptoms before treatment (dark) and after treatment (light).
Discussion and conclusion
The results of this study showed that there was no statistically significant improvement in orthostatic vitals with bupropion. However, the majority of patients presented with syncope prior to starting bupropion (36 patients); afterwards, only 15 patients of the initial 36 reported experiencing syncopal episodes. With regard to light-headedness, fatigue, palpitations, headache, exercise intolerance, difficulty concentrating and vision changes, there does not appear any overall improvement.
Of note, the vast majority of patients included in this study had vital signs that did not meet the diagnostic criteria for POTS. This could be further explained by the fact that the vast majority of these patients were already on an extensive regimen of medications that could skew assessment of orthostatic vitals in patients with POTS. As with our previous studies, there was a female predominance (80.1% female) and the average age of patients studied was 42.0±13.6 years.
A 2013 randomized crossover trial looked at the role of SSRIs in patients with POTS to assess response to BP and reflex tachycardia. A total of 39 patients with POTS were studied, comparing orthostatic vitals in patients treated with sertraline and placebo. The study found that at 4 hours, there was no significant difference in standing HR and systolic BP; in addition, symptoms at 4 hours appear to have been worse.4 Similarly, in our study, patients treated with bupropion did not have any significant change in their orthostatic vitals. However, there was no report of overall worsening symptoms and as noted there are fewer patients experiencing syncopal episodes after initiating treatment with bupropion.
While a direct comparison between the 2 studies is not ideal, ours does suggest that bupropion might be better tolerated. In addition, bupropion appears to have a similar cost to SSRIs and SNRIs.
There are limitations for this study. It is a single-center observational study; without a control group it is difficult to assess the degree of placebo effect. In addition, this was a relatively small sample size and thus the overall improvement or lack thereof in orthostatic symptoms and vital signs could be underestimated. However, this study does provide physicians with subjective and objective data that can be used when deciding whether to treat patients with POTS with bupropion.
Another limitation was the phone call response rate—of the total 200 patients who were contacted, 47 agreed to participate in the study. Regardless, this study appears to be the first study integrating subjective and objective data with regard to response of patients with POTS with initiation of bupropion.
Overall, bupropion did not show any statistically significant improvement in orthostatic vital signs in patients with POTS. However, it did show an overall reduction in syncopal events in the studied cohort (36 patients with syncope prior to treatment, 15 afterwards). As such, bupropion may be an option for patients with syncope-predominant POTS; however, this study did not exhibit any statistical data to suggest this. Larger studies will need to be performed to further delineate the benefits of bupropion with regard to overall improvement in syncope in POTS.
Footnotes
Contributors
RV, MR, and ZN assisted in the conceptualization, data curation, analysis, investigation, methodology, writing, revision, and editing. MAS and ZA assisted in the conceptualization and methodology. BG assisted in the data curation, analysis, investigation, methodology, writing, revision, editing, and supervision.
Funding
The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests
None declared.
Patient consent for publication
Not required.
Ethics approval
Our study received institutional review board approval at The University of Toledo.
Provenance and peer review
Not commissioned; externally peer reviewed.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. All data have been deidentified. Reuse is only permitted if credited.