
Abstract
There is confusion regarding reason and rational thought as a precondition for interventions designed using a reasoned action approach. To test their feasibility, two interventions were developed for use with persons with mental illnesses, using the reasoned action model. Preventing AIDS through Health (PATH) was delivered one-on-one by case managers to persons with mental illnesses who were HIV sero-negative, and another (PATH PLUS) was delivered by nurses to persons with mental illness who were sero-positive. Using these data, this article examines the utility of a reasoned action approach to HIV prevention among persons with a variety of serious mental illnesses. It appears that a reasoned action approach is useful for persons with severe mental illnesses and may be a useful strategy for changing intentions and behavior among this population. This has implications for further research on the role of nonnormative belief systems in predicting behavior.
Persons with serious mental illness are at increased risk to contract and transmit human immunodeficiency virus (HIV): estimates of the prevalence of HIV among persons with severe mental illness range from 4 to 23 percent compared to 0.4 to 0.6 percent in the general population (Blank et al. 2002; Rosenberg et al. 2001; M. Carey et al. 2004). Although high, these may be underestimates, signaling a hidden epidemic because cases of HIV in psychiatric populations are often missed by specialty mental health care providers (Brady et al. 2005; Rothbard et al. 2009). Note that epidemiological studies usually ignore the fact that mental illness and HIV infection are themselves part of a syndrome of medical and behavioral comorbidities (e.g., drug and alcohol use) that represent additional barriers to the design of effective interventions for this group (Anand et al. 2010; Hall and Prochaska 2009; RachBeisel, Scott, and Dixon 1999).
Persons with severe mental illness may present special challenges to the design of reasoned action–based interventions for two reasons. First, because a reasoned action mechanism of behavior change depends on the initial identification and then subsequent manipulation (Fishbein and Yzer 2003) of salient underlying beliefs relevant to the three determinants of intentions (i.e., attitudes, normative pressure, and behavioral control), any cognitive impairments or limitations in persons with serious mental illnesses may make identification of relevant underlying beliefs difficult. Without identifying these beliefs, effective interventions based on reasoned action theory are by definition impossible. An additional concern is the operation of a reasoned action model for mentally ill groups. Even if underlying beliefs can be elicited, they may not represent a coherent structure across respondents, may not correlate meaningfully with each other, and could be unrelated to the population-invariant “direct measures” of attitudes, social norms, and perceived behavioral control. In other words, even if all the appropriate reasoned action measures are present, if the underlying beliefs fail to predict the corresponding direct measures, the direct measures probably will predict intentions poorly, and intentions may not predict subsequent behavior (see the diagram of the reasoned action model in Ajzen [this volume]).
In this article, we investigate all of these issues using data from two HIV-prevention interventions among persons with a variety of mental illnesses to understand the structure of underlying beliefs in these persons and to analyze the utility of using a reasoned action model at the level of direct measures, intentions, and prospective sexual behavior. We then analyze the structure of the underlying injunctive normative beliefs and relate this latent variable to the direct measure of norms. Finally, we end with a discussion of the implications of our findings and a consideration of the role of reason and rationality in designing reasoned action–based interventions. First, however, the article summarizes studies investigating the underlying beliefs concerning sexual behavior for the severely mentally ill to answer the question “Can relevant beliefs be elicited from this population?”
Qualitative studies of severely mentally ill populations and their sexual behavior
Survey studies of persons with serious mental illness (M. Carey et al. 2004, 1997; Dickerson et al. 2004) are more common than qualitative studies of persons with severe mental illness and sexual risk behaviors. Furthermore, there are relatively few studies investigating underlying beliefs concerning sexual behavior for the severely mentally ill to determine if relevant beliefs can be elicited from this population. However, Gordon and colleagues (1999) reported on the results of sixteen focus groups done with thirty-six mentally ill participants recruited from an out-patient facility. Analysis of the qualitative text revealed consistent patterns of opportunistic high-risk sexual behavior, low levels of HIV-related knowledge, and low levels of HIV perceived risk. The authors make no mention of problems with eliciting these concepts from the focus group participants.
K. Carey and colleagues (1999) conducted 90-minute focus groups with twenty-one clients with schizophrenia in regard to decision-making about substance use. The researchers used the “decisional balance” concept (Prochaska 2008) that is central to the transtheoretical model (TTM) developed by Prochaska and his research group at the University of Rhode Island. 1 The decisional balance inventory consists of the positive reasons (the “PROS”) and the negative reasons (the “CONS”) for adopting or not adopting a behavior, and the identification of the PROS and CONS is an important initial step in the process of behavior change using the TTM (Prochaska et al. 1991). Some PROS of substance use included forgetting your problems, being able to positively interact socially, improving feelings of self-confidence, and reducing pressure. Some CONS included physical problems due to substance use (e.g., headaches and other effects of withdrawal), exacerbation of psychotic symptoms, and negative social interactions (e.g., violence or arguments). The researchers did not report any problems with the identification of the PROS and CONS of either maintaining or ceasing substance use. To the contrary, they reported that the process was informative as a data-collection exercise and a useful therapeutic tool.
Schulze and Angermeyer (2003) conducted two-hour focus groups with twenty-five patients with schizophrenia (as well as family members and clinical professionals in separate groups) to document their experience of stigma. Four dimensions of the stigmatization were identified: interpersonal interaction (e.g., social isolation and the need to maintain secrecy), public image of the mental condition (e.g., the stereotype of the mentally ill as violent and dangerous), institutional discrimination (e.g., the experience of differential access to medical and social services), and access to “social roles” (e.g., finding and keeping employment and having a romantic partner). No issues were raised in their article about the patients’ inability to identify and discuss the components of these four themes.
Solomon and colleagues (2007) conducted in-depth interviews and focus groups with case managers and the severely mentally ill outpatients in a community mental health center as preliminary research for designing the Preventing AIDS through Health (PATH) intervention discussed below. Topics included perceived HIV risk and protective factors among the outpatients, barriers to discussion of sexual and other HIV-related risk factor behavior between case managers and clients, and recommendations for additional training for case managers. Barriers to effective communication seemed to be attributable to case managers and not client perceptions:
What also came through in this assessment was the disconnect between the willingness of consumers [i.e., out-patient clients] and the apparent discomfort of case managers regarding discussions related to sexual health issues. The barriers to addressing HIV prevention lie primarily with attitudes of the case managers, since the consumers displayed a great deal of openness and willingness to address issues of sexuality and risk behaviors during the focus groups. (Solomon et al. 2007, 149)
Finally, Tennille and colleagues (2009) conducted additional focus groups as preliminary research for designing the PATH PLUS intervention also discussed below. Four focus groups were conducted. The first two focused on condom use (five female African Americans and five multiethnic males), and the second set focused on the side effects of psychotropic medications on sexual behavior (five African American females and five multiethnic males). The themes that emerged were related to understanding how condoms help to prevent HIV infection, how psychotropic medications affected medication adherence, and how medications negatively related to male sexual performance in achieving and maintaining erections that made consistent condom use less likely. Other themes that emerged included how sexual issues were managed, including compromises necessitated by the interaction of medications and sexual situations and desire. No problems were mentioned in the article relevant to the performance of the clients in the focus groups. The authors summarized the focus group results as follows:
In our elicitation focus groups, participants discussed planning behaviors and employing reasoning in relation to making decisions about condom use. We found that this process was greatly influenced by dependence on medications to treat mental illness and sexual sequelae. The resulting fragility of sexual response reportedly interacted with intentions and ultimate decisions to use condoms. (Tennille et al. 2009, 36)
This review suggests that qualitative studies are both feasible and useful with severely mentally ill participants. It appears that underlying beliefs can be elicited. But can such data be modeled to conform to reasoned action theory? Before answering this question, the datasets used here need to be described.
Methods and Measures
Study 1: PATH
PATH was a hybrid of two prevention interventions, Project RESPECT, an STD/HIV clinic-based multisite randomized trial (Kamb et al. 1998), and the Community-Based Outreach Model (CBOM; Wood 2000), both of which have been shown to be effective in reducing risk of blood-borne infections associated with substance use and sexual behaviors in the general population. The PATH program combined individually tailored components of both RESPECT and CBOM to address the areas of highest risk of infection through a case manager–delivered intervention for severe mental illness consumers who also abuse substances. The case manager was a primary care agent and mediator between the client and bureaucracy, simultaneously an advocate for the client and a representative of the formal organization to the client (Aviram 1990; Tennille, Solomon, and Blank 2010).
The PATH study utilized a cluster randomized design in which eighteen case managers delivered a manualized version of the PATH program of education to their caseloads and nineteen case managers delivered services as usual. Participants were eligible if actively receiving case management for mental illness and co-occurring substance use. Individuals were interviewed at baseline and at 3, 6, and 12 months. Measures included condom-use skills, symptoms of mental illness, and sexual risk-taking behaviors. PATH enrolled 281 participants in the city of Philadelphia through the Pennsylvania Hospital outpatient system from 2003 through 2008.
Study 2: PATH PLUS
PATH PLUS was a longitudinal randomized trial utilizing a control and intervention group design for persons with severe mental illnesses who were also HIV-positive. Severe mental illness was defined as having a disability due to mental illness and active involvement with community-based mental health services including case management. The intervention group was assigned an advanced practice nurse (APN) who provided in-home services and coordinated care among their other service providers for a year, with data collection at baseline and at 3, 6, and 12 months. The APNs collaborated with multiple prescribing providers, pharmacists, and case managers to organize medication regimens and help participants actively to cope with barriers to medication adherence and promote participants’ ability to self-care (Aiken et al. 1993). The protocol included a face-to-face meeting with each participant at a minimum of once a week. Control participants received standard care as usual and participated in the research interviews and provided blood samples for testing at the same intervals as experimental participants. Advertisements were placed in community mental health and HIV treatment facilities; participants who self-identified as being HIV-positive were eligible if they were followed by a case manager and their treating physician could confirm a co-occurring diagnosis of a serious mental illness. PATH PLUS enrolled 231 participants who were 18 years of age or older, able to understand spoken English, HIV-positive, and diagnosed with a mental illness.
These studies are appropriate for the purpose here. They both included follow-up data (the three-month follow-up data from both studies are used in this analysis), used a heterogeneous sample of respondents with multiple comorbidities including HIV infection and drug and alcohol use, did not focus on condom use as the intervention’s ultimate dependent variable, were designed using reasoned action theory, and used identical reasoned action data collection instruments. In the combined dataset (N = 230), 43 percent of the participants were male, 48 percent were HIV-positive, and 73 percent were black (the others were white or multiethnic). The biggest difference between the two studies is the HIV-positive status of PATH PLUS participants, so this respondent characteristic (as well as gender and race) is treated as a precursor variable that could potentially differentiate the respondents in the analysis (Hennessy et al. 2010).
Measures of reasoned action concepts
The PATH and PATH PLUS interventions distinguished between sexual relationships with “regular” and “casual” partners because previous research shows that practicing unsafe sex is generally higher with the former group than with the latter (Misovich, Fisher, and Fisher 1997). However, because sex with casual partners was very infrequent in both studies, we only used responses for regular partners here. The reasoned action intention measure was “In the next 3 months, how likely is it that you will use a condom for vaginal sex with a regular partner?” The responses were coded from 1 to 7, using extremely unlikely to extremely likely (average at first data collection = 4.88, SD = 2.41). The direct measure of attitude used the stem “My using condoms every time I have vaginal sex with my regular partner in the next 3 months would be: . . .” The responses were six semantic differential items: unpleasant/pleasant, difficult/easy, a turn-off/a turn-on, uncomfortable/comfortable, stressful/not stressful, and foolish/wise, all coded on a 1 to 7 metric with extremely, quite, slightly, and neither as the possible responses (mean at first data collection = 4.85, SD = 1.43, polychoric alpha =.86). The direct measure of injunctive normative pressure 2 used the stem “Most people who are important to me think I should use a condom every time I have vaginal sex with my regular partner.” The responses were coded from 1 to 7, using extremely unlikely to extremely likely (average at first data collection = 5.65, SD = 2.00). The direct measure of self-efficacy used the stem “Many things make condom use difficult, but if I really wanted to, I could always use a condom when I have vaginal sex with my regular partner.” The responses were coded from 1 to 7, using strongly disagree to strongly agree (mean at first data collection = 6.05, SD = 1.75).
Both PATH and PATH PLUS successfully elicited underlying attitudinal, normative, and self-efficacy beliefs. For example, there were eleven behavioral (attitudinal) beliefs elicited, all with the stem “Using a condom every time you have vaginal sex with your regular partner will: . . .” The outcome expectancies were (1) protect him/her from STDs, (2) protect you from STDs, (3) protect him/her from AIDS, (4) protect you from AIDS, (5) decrease your sexual sensation, (6) make sex less spontaneous, (7) mean that you don’t have enough money for other things, (8) make you lose your erection (men only), (9) make you feel cleaner, (10) make him/her think you have an STD, and (11) make your regular partner think that you think they have an STD. Note that except for item 8, all of these beliefs are similar to established underlying belief items regularly used for adolescent populations (St. Lawrence et al. 1994).
However, analysis of the direct measures suggests that intentions were primarily determined by normative considerations (see below), so to highlight the structure of these beliefs, only the injunctive normative underlying beliefs are discussed in detail here. These four measures used the stem “[Referent] think(s) that I should use a condom every time I have vaginal sex with my regular partner.” [Referent] was replaced with “My friends,” “My case manager,” “My doctor,” and “My regular partner”; these four normative belief items were coded from 1 to 7, using extremely unlikely to extremely likely. Means and standard deviations of these items at the first data collection were: friends (5.58, 1.98), case manager (6.08, 1.58), doctor (6.45, 1.28), and regular sex partner (4.65, 2.39). Therefore, injunctive norms were highest for the respondents’ doctors and case managers and lowest for the respondents’ regular sex partners.
The dependent variable was an ordinal measure of condom use with the stem “In the past 3 months, how often did you use a condom during vaginal sex with your regular sex partner?” The responses were coded on a 1 to 7 metric from never to all the time. At the first data collection the mean was 4.02 (SD = 2.63, N = 167), and at the follow-up data collection the mean was 4.12 (SD = 2.66, N = 124).
Statistical analysis to evaluate the reasoned action approach
First, we estimated the correlations between the reasoned action determinants of intentions and intentions at the first data collection point and self-reported condom use at the second data collection point. The expectations were that the three reasoned action predictors of intentions would be correlated but not redundant and that their relative association with intentions would indicate if all or only a subset are the main determinants of intentions for this group of respondents. Because prospective data on behavior were available, the correlations between all the reasoned action variables and behavior at follow-up were also of interest. Intentions, of course, should have the highest correlation with behavior.
Next, the combined effect of the direct measures on intentions at the first measurement period and the self-report of condom use at the second data collection were analyzed. As is standard with reasoned action analyses when precursor variables are important, we simultaneously modeled the three background variables of race, gender, and HIV status to control for initial differences among respondents. It was not necessary to include a variable for PATH or PATH PLUS because HIV status for the respondents was redundant with study type since all of the PATH PLUS and none of the PATH participants were HIV sero-positive. The error terms of the reasoned action mediators were correlated because reasoned action theory does not propose a causal order of the attitudinal, normative, or self-efficacy direct measures (Hennessy et al. 2010).
The third analysis presented here examined the structure of underlying injunctive normative beliefs and examined (1) how these beliefs varied across the types of respondents in the two studies, (2) whether these beliefs were internally consistent, and (3) whether the underlying beliefs were correlated with the direct measure of social norms. To address issue 1, we examined differences between the normative underlying beliefs, focusing on HIV-positive and HIV-negative respondents. For issues 2 and 3, confirmatory factor analysis of ordinal measures was appropriate (Brown 2006). Mplus (Muthén and Muthén 2006) was used for all the structural equation modeling because most of the dependent variables were ordinal. When Mplus encounters ordinal indicators, it implements a weighted mean and variance estimator that has been shown to have excellent statistical qualities even with small samples (Flora and Curran 2004). Mplus also has an advantage because it uses an advanced maximum likelihood estimation method that eliminates the bias of listwise deletion of observations when missing values are present (Enders and Bandalos 2001).
Results
Correlations between reasoned action measures and behavior
Table 1 shows the correlations between the three reasoned action mediators, contemporaneous condom use intentions, and reported condom use at the second data collection point. All the direct measure mediators are positively correlated but are certainly not redundant as suggested by some critics of the reasoned action approach (Ogden 2003): the determinant of the direct measure mediator correlation matrix is .81 and the largest variance inflation factor (VIF) is 1.18; both of these values suggest no problem with multicollinearity (Kennedy 2003; Rockwell 1975). The correlations between attitudes and social norms and intentions were substantial (>.4), while the correlation between intentions and self-efficacy was lower (<.2). This suggests that the primary determinants of intentions were both attitudinal and normative for these respondents. This primacy of attitudes and social norms is highlighted when the correlations between all four reasoned action variables and prospective reports of condom use are examined in the last row of the correlation matrix. Both attitudes and norms predicted behavior well, although of the four reasoned action items, intentions had the highest correlation, with prospective behavior at .568, and by itself accounts for more than 32 percent of the variance in condom use behavior.
Correlations of Reasoned Action Mediators, Intention, and Condom Use Behavior at Follow-Up

NOTE: N and significance level appear below correlation.
From these results, it appears that the reasoned action variables do quite well in predicting self-reported condom use for a sample of severely mentally ill respondents. Next, we conducted a multivariate analysis of the reasoned action model that included precursor variables so that partial effects of the reasoned action determinants on intentions could be estimated as well as the effects of respondent features, including race, gender, and HIV serostatus, on the reasoned action mediators.
Analysis of the direct measure model with precursor variables
Figure 1 shows the results in path analytic format of the analysis of the reasoned action model, using the direct measures and three precursor variables: ethnicity (black vs. all others), gender (males vs. females), and HIV status (positive vs. negative). The model fits well, although the root mean square error of approximation (RMSEA) is somewhat larger than is optimal due to the low degrees of freedom of the model as a whole. Looking first at the reasoned action components and the partial effects of the mediators suggests that norms were the primary determinant of intentions to use condoms, followed closely by attitudes. Self-efficacy seems to play virtually no role in predicting intentions to use condoms with regular partners among these participants once the other theoretical mediators were controlled. Self-efficacy also played virtually no role in predicting condom use, while intentions had a large effect, almost .70 of a standard deviation change in behavior given a 1 standard deviation change in intentions. Finally, note the efficiency of reasoned action theory in predicting condom use in this population: two predictors explain more than 56 percent of the variation in condom use behavior.

Reasoned Action Model Results (N = 230)
When we look at the precursor variables, gender and race play virtually no role in predicting levels of the three reasoned action mediators. However, HIV status is a very important precursor: HIV-positive respondents have significantly higher average values of self-efficacy (about half a point on the 1–7 scale) and injunctive normative pressure (about .9 of a point on the 1–7 scale) than HIV-negative respondents after adjusting for gender and ethnicity.
The structure of the underlying normative beliefs
The analysis of the direct measure model presented in Table 1 and Figure 1 showed that injunctive norms were the single best predictor of intentions and that, of the three precursor variables, HIV status of the respondent was the superior predictor of normative pressure. From a reasoned action perspective, this suggests that the beliefs underlying injunctive norms should vary by HIV status because the best theoretical predictor of any direct measure is its corresponding underlying beliefs (Fishbein and Ajzen 2010). Therefore, the four injunctive normative underlying beliefs should vary by HIV status, consistent with their variation in the single-item direct measure of normative pressure.
Table 2 presents the differences among the four underlying injunctive norm measures and HIV status. In every case, HIV-positive respondents report higher levels of perceived injunctive pressure than HIV-negative respondents when it comes to using condoms consistently with their main sex partner. This is entirely the expected pattern, given the results for the direct measure analysis presented in Figure 1.
Average of Injunctive Normative Beliefs by HIV Status
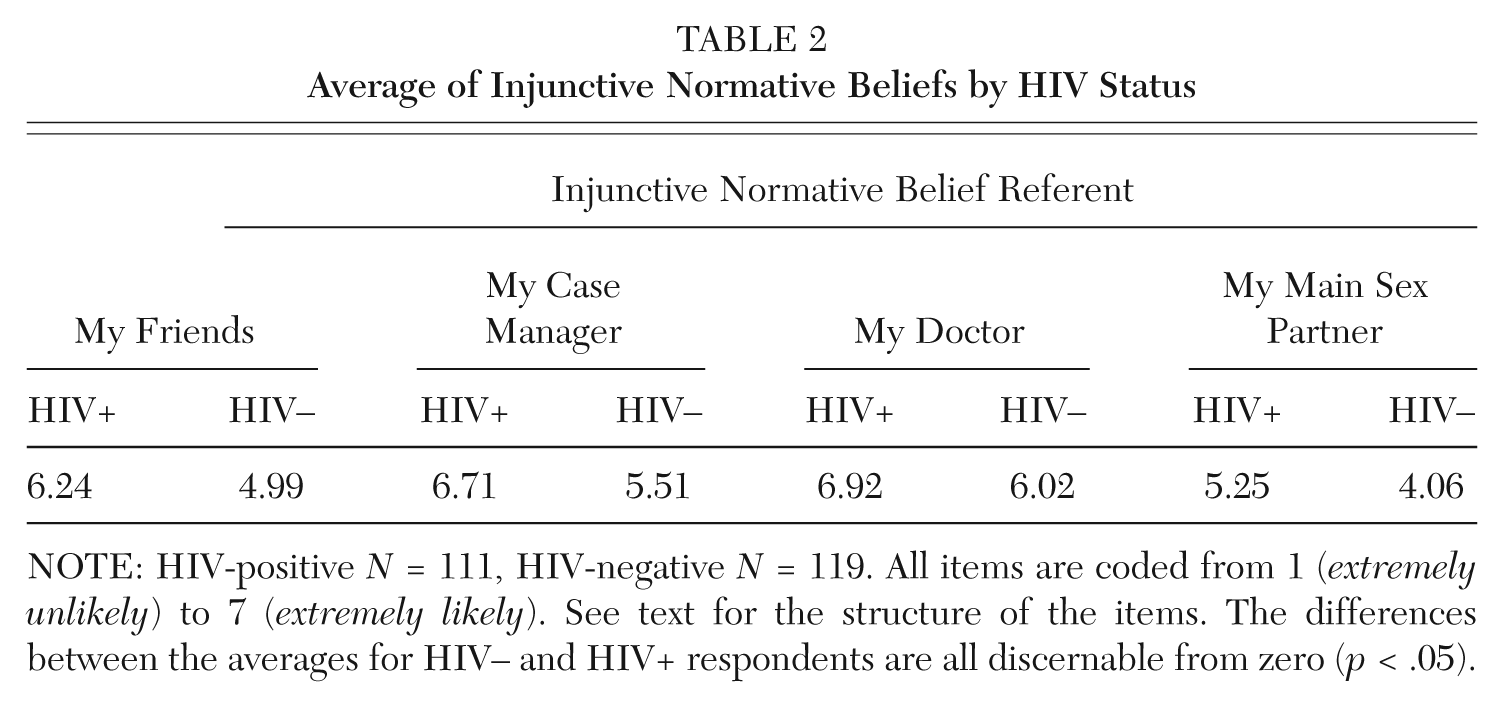
NOTE: HIV-positive N = 111, HIV-negative N = 119. All items are coded from 1 (extremely unlikely) to 7 (extremely likely). See text for the structure of the items. The differences between the averages for HIV– and HIV+ respondents are all discernable from zero (p < .05).
Table 2 shows that average values of normative pressure consistently differed between respondents by HIV status and that normative pressure—regardless of referent source—was always higher for HIV-positive respondents compared to HIV-negative respondents. But more questions can be asked about the structure of these belief items other than those about differences in their central tendency. For example, if the items were unidimensional in a factor analytic sense, this would be evidence of a consistent covariance structure. It would also be of theoretical interest to know how well the underlying belief items correlate with the direct measure of social norms. To address both issues, confirmatory factor analysis was used to construct the latent variable that best accounts for the correlations between the four items and simultaneously estimates the correlation between the latent variable and the direct measure of normative pressure used in Figure 1.
Figure 2 has these results. The overall model fits extremely well, and the latent variable (i.e., “injunctive normative belief”) predicts the four belief items, although the latent variable’s association is smaller for the respondents’ main sex partner than the other three referents. We believe that this lower factor loading is due to a gender difference between injunctive pressure from main sex partners. Although there are no gender differences for perceived injunctive pressure between male and female respondents for doctors, case managers, and friends, females perceive less injunctive pressure to use condoms from their (male) sex partners than males perceive from their (female) sex partners (female average = 4.25, male average = 5.17, t = −2.93, p = .004).
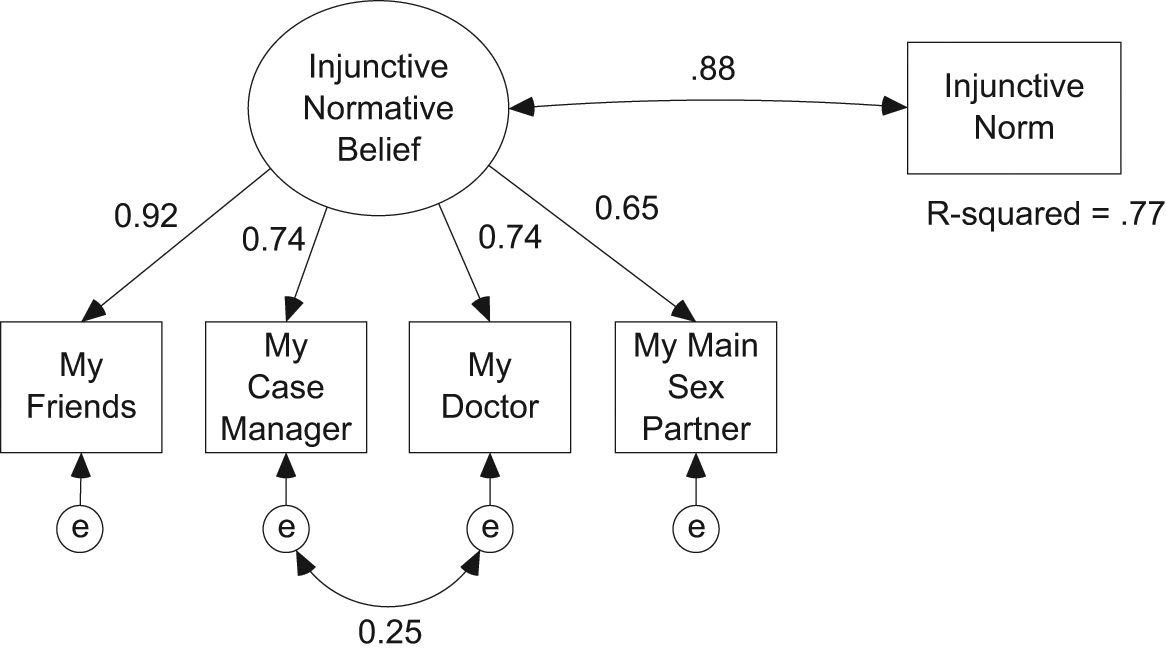
Measurement Model of Injunctive Normative Beliefs and Their Correlation with the Direct Measure of Injunctive Norms (N = 230)
Also note that the model required a correlated error (Gerbing and Anderson 1984; Bollen and Paxton 1998) between case manager and doctor referents. This is probably due to the fact that these two referents had shared responsibility for the respondents’ clinical care, would consult with each other, and presumably acted in a coordinated fashion in providing treatment. The question of whether there is a correlation between the latent variable and the direct measure of injunctive norms is also answered in Figure 2. It shows that the correlation between the latent variable and the direct measure is .88, a value that explains 77 percent of the variance in the direct measure.
Discussion
In summary, it appears that severely mentally ill persons can report coherent underlying beliefs related to the three main reasoned action concepts. In addition, these beliefs covary with social characteristics in predictable ways. HIV-positive respondents have higher levels of self-efficacy and normative pressure to use condoms than HIV-negative respondents, most likely because, similar to the general population, most are responsible and concerned about protecting their sex partners from infections. Also, similar to the dynamic that exists in the general population, females felt less injunctive pressure to use condoms from their male sex partners than males perceived from their female sex partners. More specific to persons with mental illnesses is that respondents included their case managers and doctors as part of their injunctive normative referents.
Given the context of the intervention, these results could be expected; HIV-positive respondents have, after all, a much higher risk of infecting others with the virus, and to measure higher levels of perceived normative pressure in this group is an encouraging finding. In addition, our analysis of the reasoned action model and the internal consistency of the normative beliefs shows good fit and plausible results. In fact, our quantitative results may actually be better in terms of model goodness of fit and the proportion of variance accounted for in this population than for the general population (Albarracín et al. 2001; Webb and Sheeran 2006).
Most of the participants in our sample were being treated for their mental illnesses during the study period, and any assumption that, as a group, the respondents lacked capacity for rational thought would be erroneous. The assumption that a reasoned action approach is inherently dependent on individual rationality is equally flawed. Our findings conflict with the assertion that the reasoned action approach constitutes an overtly “rational” system of explanation and prediction (Reyna and Farley 2006, 5). This type of criticism displays a fundamental misunderstanding of how reasoned action theory operates. A reasoned action approach assumes that the major determinants of intentions are constructed from the underlying beliefs and follow consistently (i.e., are accessible) from them (Ajzen and Fishbein 2000). How the determinants of intentions are cognitively organized and processed to produce an intentionality toward a target behavior—be it logically, axiomatically, heuristically, intuitively, or reactively, or by using “fuzzy logic” or any other cognitive processing system (Reyna and Farley 2006)—is not part of reasoned action theory. The important point here is that reasoned action theory assigns no privileged status to “rational” processing of the underlying beliefs in producing intentionality compared with “irrational” processing toward the same outcome (Ajzen 2001). In fact, we would suggest that salient nonnormative beliefs may be highly predictive of both intentions and behaviors.
The irrelevance of rationality also applies, of course, to the underlying beliefs themselves: they need not be factually accurate, logical, or internally consistent. Examples of salient nonnormative underlying beliefs are easy to imagine. For example, HIV vaccine trials need to recruit volunteer participants (Hennessy et al. 1996; Frew et al. 2010), but a positive endorsement of the belief that “volunteering for a HIV vaccine trial promotes a government strategy designed to identify and control sexual and ethnic minorities” would probably be negatively related to volunteering, no matter how irrational this assertion may appear to HIV researchers. Political examples are also relevant: voting for Tea Party candidates may be well predicted by the belief that “voting for a Tea Party candidate will help to expose the fact that President Obama was born in Kenya” or “voting for a Tea Party candidate will help to reveal that bailouts of major American banks are schemes of large financial interests to maintain and expand their economic influence.” It is likely that elicitation studies conducted with members of fringe political groups (e.g., neo-Nazis, religious fundamentalists) would identify similarly strongly held nonnormative underlying beliefs, and again, the truth or rationality of these beliefs would be unrelated to the effectiveness of a reasoned action approach to predicting intentions and subsequent behavior. In the case here, the PATH and PATH PLUS projects did not identify any such nonnormative or unconventional beliefs, but they did identify some that were specifically relevant to the research population. This finding highlights the need for conducting elicitation studies (see Middlestadt, this volume) when the population of interest is unfamiliar to reasoned action researchers.
Footnotes
This research was supported by grants from the National Institute on Drug Abuse (RO1-DA-015627 “HIV Prevention Program among Substance Abusing SMI”) and the National Institute for Nursing Research (RO1-NR-008851 “Nursing Intervention for HIV Regimen: Adherence among SMI”).