
Abstract
Of the estimated 10 million youths living with HIV worldwide, 63 percent live in sub-Saharan Africa. This article focuses on migration as a risk factor of HIV infection among the youths in sub-Saharan Africa. The study is based on multilevel modeling, applied to the youth sample of the Demographic and Health Surveys (DHS), conducted from 2003 to 2008 in nineteen countries. The analysis takes into account country-level and regional-level variations. The results suggest that across countries in sub-Saharan Africa, migrants have on average about 50 percent higher odds of HIV infection than nonmigrants. The higher risk among migrants is to a large extent explained by differences in demographic and socioeconomic factors. In particular, migrants are more likely to be older, to have been married, or to live in urban areas, all of which are associated with higher risks of HIV infection. The higher risk among youths who have been married is particularly pronounced among young female migrants.
Keywords
The UN estimates that of the more than 1 billion youths (ages 15–24) worldwide, some 10 million are living with HIV, and of the 15- to 24-year-old people living with HIV, 63 percent live in sub-Saharan Africa (United Nations Population Fund [UNFPA] 2005). The predominant mode of HIV transmission in the high-prevalence countries of sub-Saharan Africa is heterosexual intercourse, and where heterosexual intercourse is the primary mode of HIV transmission, young women face significantly higher risks than men (United Nations Children’s Fund [UNICEF] 2003; UNAIDS 2004). In some parts of sub-Saharan Africa, the prevalence of HIV infection among women aged 15 to 24 is two to eight times that among men in the same age group (Clark, Bruce, and Dude 2006; Madkan et al. 2006; Gouws et al. 2008; Magadi 2011b). Adolescence is both a stage of increased vulnerability for HIV infection as well as a window of opportunity to curb the spread of the epidemic. A number of behavioral, physiological, and sociocultural factors make young people more vulnerable than adults to HIV infection.
Bankole and colleagues (2004) noted that adolescents are more likely to engage in risky sexual behavior, such as changing partners frequently, having multiple concurrent partners, or engaging in unprotected sex, all of which increase their risk of contracting HIV. On the other hand, adolescence presents a window of opportunity for introducing policies and educational programs that could change the course of the HIV epidemic in sub-Saharan Africa. The World Health Organization points out that during early adolescence, HIV rates are the lowest of any period during the life cycle, and focusing on young people is likely to be the most effective approach to confronting the epidemic, particularly in high-prevalence countries (Bankole et al. 2004).
Adolescents in many countries of sub-Saharan Africa face rural underdevelopment; widespread poverty; poor educational opportunities; and limited access to radio, television, and newspapers (possible sources of information about HIV/AIDS) (Bankole et al. 2004). Although one might expect migration to lead to increased media exposure and access to sources of information about HIV/AIDS among adolescents, existing evidence suggest higher HIV prevalence among the more mobile communities, such as urban residents. It has been argued that migration is not itself a risk factor for HIV infection but that the circumstances associated with movement increase vulnerability to HIV infection (UNAIDS 2009). Coffee, Lurie, and Garnett (2007) suggest that migration increases vulnerability to HIV primarily by encouraging increased risky sexual behavior rather than by connecting areas of high or low risk.
Studies addressing the impact of migration on reproductive health outcomes of young people in sub-Saharan Africa, including the risk of HIV infection, are limited. This article focuses on migration as a risk factor for HIV infection among the youths in sub-Saharan Africa. The study pays particular attention to gender disparities, the role of demographic and socioeconomic characteristics, and sexual behavior. The specific objectives are to (1) examine the association between recent migration status and the risk of HIV infection among these youths; (2) determine the extent to which individual, family/household, or contextual circumstances moderate the risk of HIV infection among migrant youths; and (3) examine the determinants of HIV infection among youth migrants in sub-Saharan Africa.
Data and Methods
The data
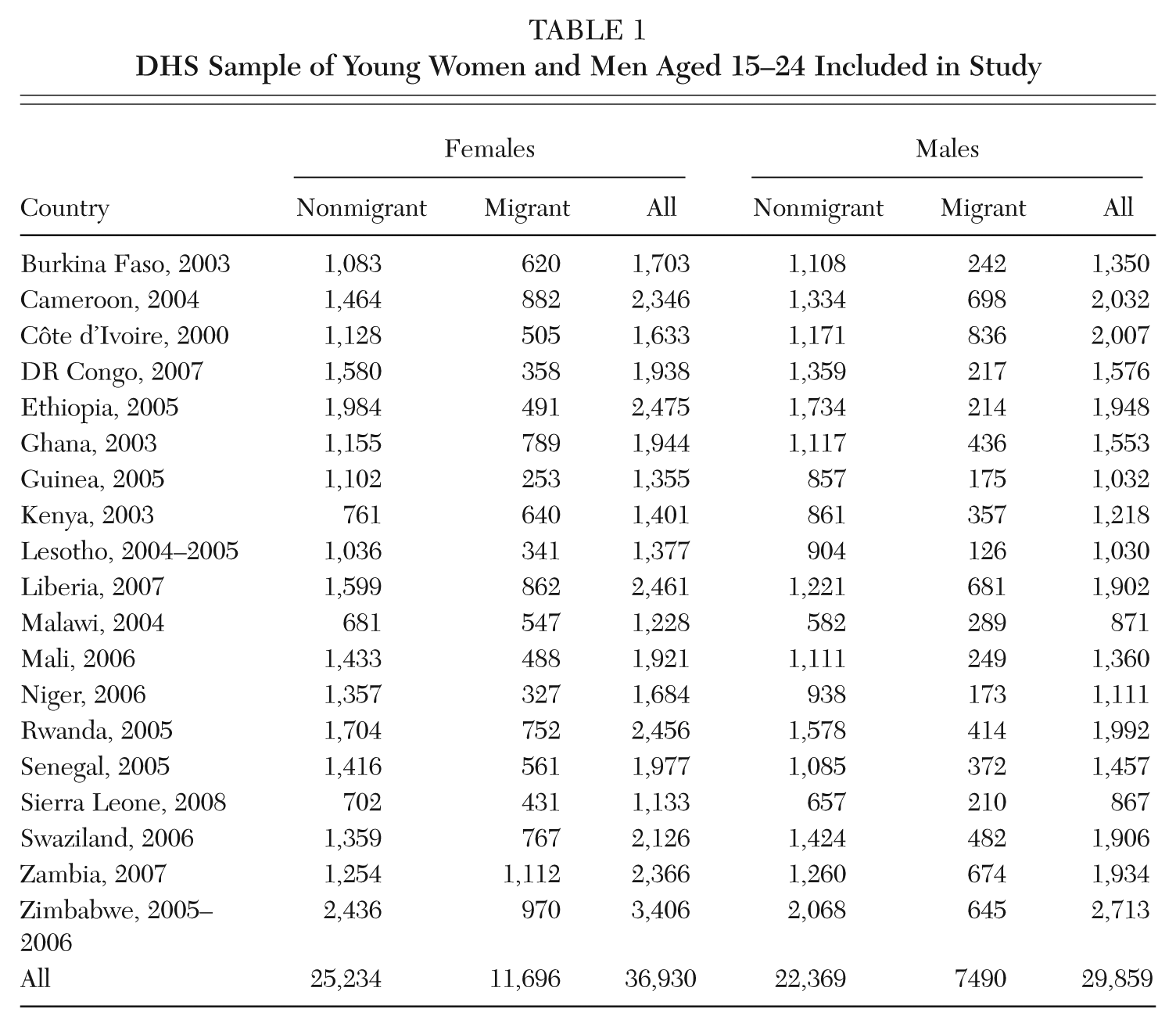
The data used in this study come from population-based sample surveys (Demographic and Health Surveys [DHS] and AIDS Indicator Surveys [AIS]) that were conducted between 2003 and 2008 in nineteen countries in sub-Saharan Africa as part of the DHS program. The DHS comprise nationally representative samples of women and men of reproductive age. Our study focuses on the youth sample. A summary of the DHS sample of young women and men aged 15 to 24 analyzed here, classified by migration status, is given in Table 1. For the purposes of this article, I define a recent migrant (referred to simply as a migrant) as a person who has lived in his or her current residence for no more than five years.
DHS Sample of Young Women and Men Aged 15–24 Included in Study
The linkage of DHS HIV test results to the full DHS record (without personal identifiers) allows for an in-depth analysis of the socioeconomic, demographic, and behavioral factors associated with HIV infection among specific subgroups of the population. Sample data from the nineteen countries covered in this study were pooled for overall analysis for sub-Saharan Africa. Pooling the surveys is appropriate mainly because the DHS and AIS surveys were designed to collect cross-nationally comparable data on population and health issues.
Analytical methods
The analysis begins with a bivariate examination of the characteristics of youth migrants and the association between HIV infection among migrant and nonmigrant youths by various characteristics, followed by a multivariate analysis of migration as a risk factor for HIV infection that simultaneously controls for the effect of other important factors. It is important to note that all analyses are based on unweighted pooled data. Therefore, the bivariate distributions provide overall characteristics of the DHS youth sample analyzed, rather than the overall distribution of youths in sub-Saharan Africa. For multivariate analysis, use of sample weights is often debatable (see, for example, Winship and Radbill 1994). In this case, weighting is not desirable since the models include key factors that relate to varying sample weights such as urban/rural residence and random country effect.
The multivariate analysis involves application of multilevel logistic regression models to explore individual and contextual regional/country-level factors associated with the risk of HIV infection among youths aged 15 to 24 in sub-Saharan Africa. The outcome variable of interest is HIV positivity, while the key explanatory variable is migration status. Other explanatory variables considered as covariates in the analysis include individual/household-level socioeconomic and demographic characteristics (e.g., age, marital status, urban/rural residence, education, whether still in school, sex of household head, household socioeconomic status, orphanhood status [for 15- to 17-year-olds], and relationship to household head) and sexual behavior factors (e.g., age at first sexual encounter, premarital sex, condom use/non–spousal sex partner, 1 and multiple partners).
These covariates are introduced to the models in successive stages to establish potential pathways of the migration and HIV infection link. The analysis features multilevel modeling, placing particular emphasis on the extent of clustering of HIV infection among the youths within countries and regions (region within country), and considers potentially important contextual factors at country and regional levels, including HIV prevalence. The pooled data have a hierarchical structure with individuals nested within regions that are in turn nested within countries. In the multilevel analysis applied in this article, countries constitute the highest (third) level (n = 19), while regions within countries constitute the second level. The general form of the three-level logistic regression model used may be expressed as

where πijk is the probability of being HIV positive for an individual i, in the jth region in the kth country; X′ijk is the vector of covariates that may be defined at the individual/household, region, or country levels; β is the associated vector of usual regression parameter estimates; Y′ijk is a vector of covariates (a subset of X′ijk) that vary randomly at the regional level; Z′ijk is a vector of covariates (a subset of X′ijk) that vary randomly at the country level; and the quantities vk and ujk are the residuals at the country and regional levels, respectively. These are assumed to have normal distribution with mean zero and variances
The estimates of country- and region-level variances are used to calculate intraunit correlation coefficients to examine the extent to which HIV positivity among youths is clustered within countries (or regions within countries) in sub-Saharan Africa. These are derived after taking into account the effect of significant covariates. Since individuals within the same region are also within the same country, the intraregion correlation includes country variances (see, for example, Siddiqui et al. 1996). Thus, the intraregion (ρ u ) and intracountry (ρ v ) correlation coefficients are given by

and

where
The analysis based on multilevel random coefficient models allows for potential variation in the effect of migration status across countries and across regions within countries. The modeling is carried out separately for males and for females, and analysis is undertaken using MLwiN multilevel software with calculation of parameter estimates based on second order PQL procedure (Rasbash et al. 2005).
Data limitations
We recognize important data limitations that should be borne in mind in the interpretation of our findings. The first relates to our definition of a recent migrant—a migrant is defined as a person who has lived in the current place of residence for no more than five years. The DHS data used in this study are quite limited on information on the type or the characteristics of migration. For instance, the distance and nature of the migration are likely to affect the extent to which respondents remain in touch with family and whether social controls still apply. Our measure includes recent relocations that are to nearby places, as well as major moves to much more distant places—from rural to rural as well as rural to small city and small city to large city—meaning that the effects are hard to precisely measure and to distinguish. Thus, the overall proportion of our youth sample classified as migrants (32 percent of females and 25 percent of males) is higher than would be expected if a more conventional definition of migration were used.
The second data limitation relates to the problem of causality given the cross-sectional nature of the data, which makes it impossible to establish the time sequencing of the events of interest. For instance, we cannot establish whether HIV infection preceded migration or vice versa, or whether the observed relationships may result from predisposing conditions that are associated with both HIV risk and migration. The migration variable is designed to pick up recent migrations within the last five years, which means that migration occurred anywhere from shortly before the interview up to five years before the interview. On the other hand, the HIV test was administered around the time of interview. If it were positive, the infection could have taken place at any time in the past; it may have occurred after the respondent migrated, or before. Although the fact that the study population is between 15 and 24 years old somewhat reduces this problem—since most infections in sub-Saharan Africa are through heterosexual contacts and the mean age of initiating sex is in the mid- to upper teenage years—there is still some room for these two key variables not to occur in the expected chronological order (migration precedes and leads to HIV infection). Therefore, the observed relationships refer to mere associations rather than infer precise causal relationships.
A third limitation relates to missing data for some of the key explanatory variables— school attendance and orphanhood status. For instance, data on current school attendance were not available for those aged 18 years or older in some countries, while data on orphanhood status were only available for those under age 18 in ten of the nineteen countries. This limits the extent to which results for these variables could be generalized for the youth sample in sub-Saharan Africa. Nevertheless, it was worthwhile to incorporate these variables in the analysis by including a dummy category for “no data.” This enabled estimation of the effects of school attendance or orphanhood for cases where data were available, while at the same time controlling for potential bias that may result from exclusion of select cases or some countries with missing data from the analysis. Preliminary analysis established that whether or not these variables were included in the models did not significantly affect estimates of the other parameters.
Another potential data limitation relates to the measurement for the HIV infection variable. Since some proportion of survey respondents refuse to be tested in DHS surveys, it is important to recognize potential bias that may result from this. In particular, one may argue that refusal is likely to be selective to those individuals who are more likely to be infected. However, previous examination into HIV testing in the countries included in this article by gender and other key factors showed reasonably high response rates and no clear systematic patterns that are likely to create bias in the analysis of HIV risk (Magadi and Desta 2011). Overall response rates for HIV testing were observed to be quite high, ranging from a low of 70 percent of eligible women (and 68 percent of eligible men) in Malawi to a high of 97 percent of eligible women (and 95 percent of eligible men) in Rwanda.
Finally, an important consideration in multilevel analysis relates to sample size at the various levels (see discussion in Magadi 2011a). In particular, it has been pointed out that statistical power for individual-level estimates depends on the number of individuals, while power for higher-level estimates depends on the number of groups (Kreft 1996; Snijders 2005). Thus, it is important to note that the relatively small number of countries in our analysis is likely to lead to reduced statistical power to detect significant country-level effects. This limits our examination of a number of potentially important macro-level contextual factors (such as country-level HIV prevalence) that may moderate the association between migration and HIV risk among youths.
Bivariate Analysis
Characteristics of youth migrants
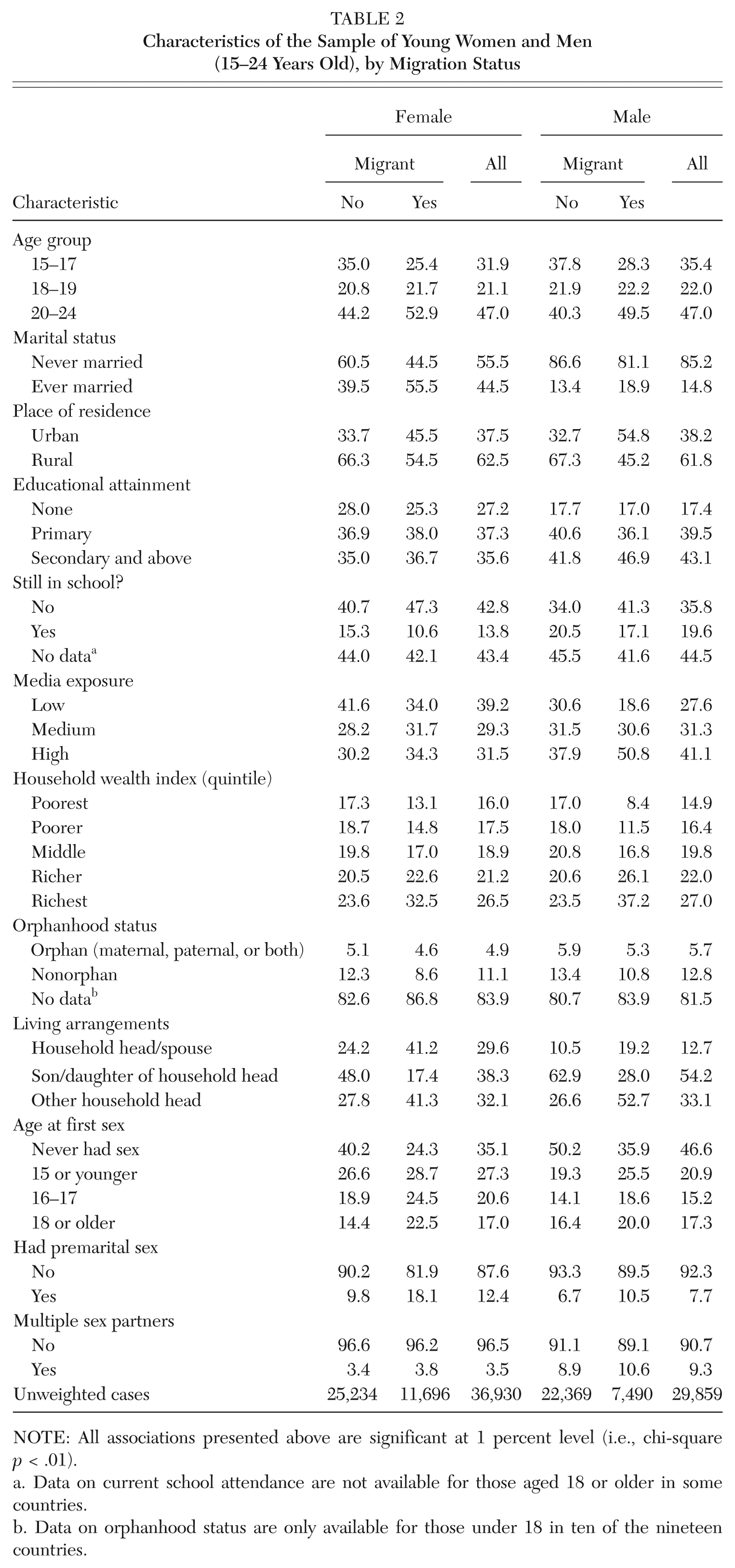
We start with a bivariate analysis of the distribution of our sample of youth migrants and nonmigrants according to various characteristics included in the analysis (Table 2). An understanding of the characteristics of youth migrants will help us to understand the extent to which the migrants represent a select group, which is useful for accurate interpretation of the patterns observed.
Characteristics of the Sample of Young Women and Men (15–24 Years Old), by Migration Status
NOTE: All associations presented above are significant at 1 percent level (i.e., chi-square p < .01).
Data on current school attendance are not available for those aged 18 or older in some countries.
Data on orphanhood status are only available for those under 18 in ten of the nineteen countries.
Among both female and male youths, migrants are significantly more likely to be older, to be ever married, to live in urban areas, to be out of school, to have higher media exposure, to live in richer households, to not be living with parents, to be sexually active, and to have had premarital sex or multiple sex partners (especially men) compared to their nonmigrant counterparts (Table 2). Furthermore, young female migrants are more likely to have attained at least primary level education, while young male migrants are more likely to have attained at least secondary level education than their nonmigrant counterparts. These associations are all highly significant (chi-square p < .01).
Association between HIV infection among migrant and nonmigrant youths by various characteristics
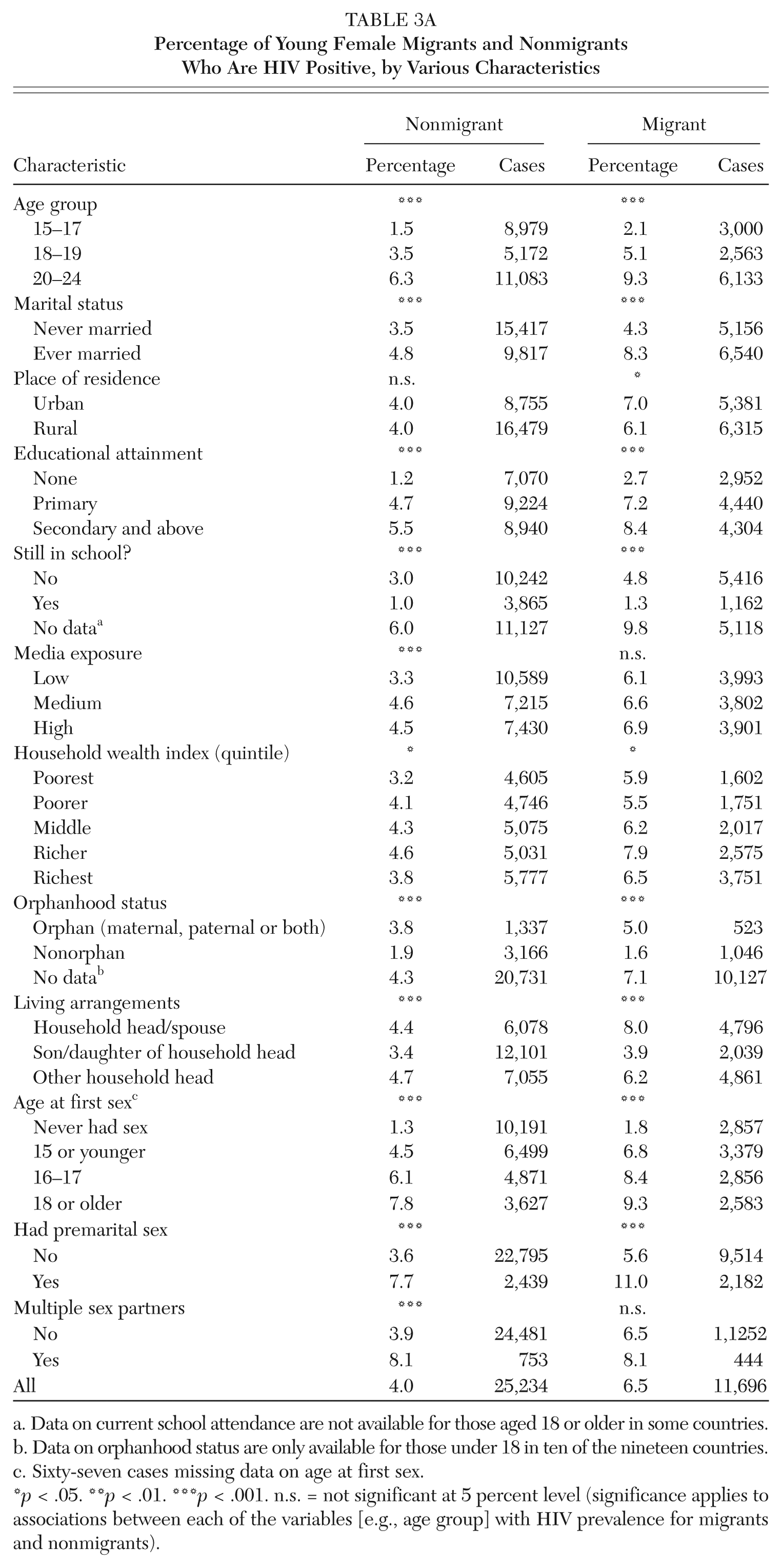
The percentage distribution of young female migrants and nonmigrants who are HIV positive by various characteristics is presented in Table 3a, while the corresponding data for young men are given in Table 3b.
Percentage of Young Female Migrants and Nonmigrants Who Are HIV Positive, by Various Characteristics
Data on current school attendance are not available for those aged 18 or older in some countries.
Data on orphanhood status are only available for those under 18 in ten of the nineteen countries.
Sixty-seven cases missing data on age at first sex.
p < .05. **p < .01. ***p < .001. n.s. = not significant at 5 percent level (significance applies to associations between each of the variables [e.g., age group] with HIV prevalence for migrants and nonmigrants).
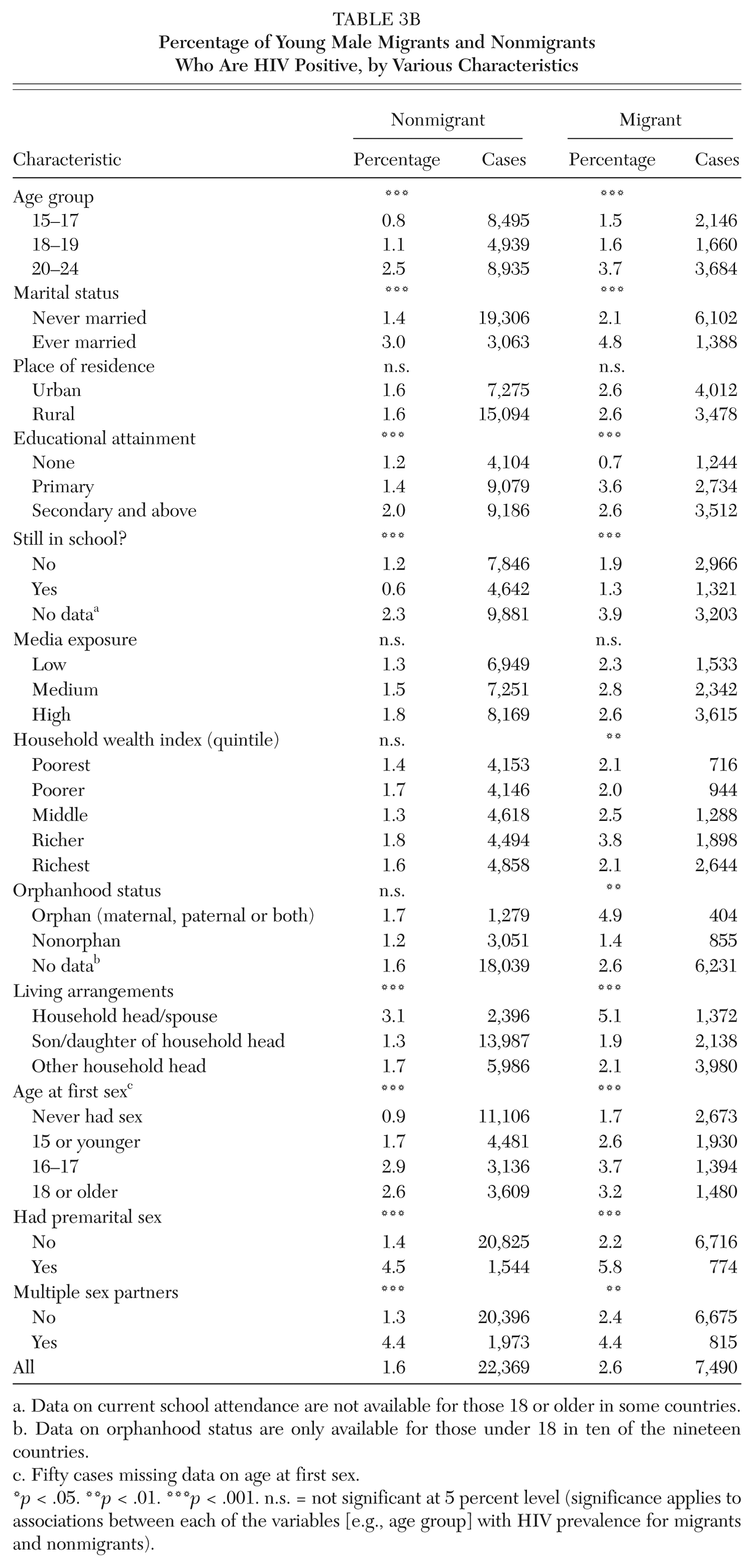
Percentage of Young Male Migrants and Nonmigrants Who Are HIV Positive, by Various Characteristics
Data on current school attendance are not available for those 18 or older in some countries.
Data on orphanhood status are only available for those under 18 in ten of the nineteen countries.
Fifty cases missing data on age at first sex.
p < .05. **p < .01. ***p < .001. n.s. = not significant at 5 percent level (significance applies to associations between each of the variables [e.g., age group] with HIV prevalence for migrants and nonmigrants).
The prevalence of HIV is consistently higher among young female migrants than nonmigrants across various demographic, socioeconomic, and sexual behavior factors (Table 3a). Among both migrant and nonmigrant young women, the prevalence of HIV is higher among those who are older, are ever married, have higher educational attainment, are out of school, are orphans, are not living with parents, and have had premarital sex. However, it is interesting to note that while HIV prevalence is higher among urban than rural residents who are recent migrants, the association between urban/rural residence and HIV infection is not significant for young women who are nonmigrants. Other factors that show different patterns of HIV infection between migrant and nonmigrant young women are media exposure and multiple sex partners. Greater media exposure and having multiple sex partners are associated with higher HIV prevalence among young female nonmigrants, but the relationships are not significant for female migrants.
The patterns observed for men (Table 3b) are generally similar to those observed for women, showing higher prevalence of HIV infection among both migrant young men and women (compared to nonmigrant young men and women, respectively), especially among those who are older, are ever married, have higher educational attainment, are not living with parents, and have had premarital sex. Furthermore, both migrant and nonmigrant young men who had multiple sex partners in the 12 months preceding the survey are significantly more likely to have HIV infection than their migrant and nonmigrant counterparts who did not have multiple sex partners. Urban/rural residence and media exposure are not significantly associated with HIV infection among both migrant and nonmigrant young men. However, while orphanhood status and household wealth are both not significantly associated with the risk of HIV infection among nonmigrant young men, these relationships are highly significant among young male migrants, suggesting that orphans or those in richer households (4th quintile) are more likely to be infected with HIV than their migrant counterparts who are nonorphans or live in poorer households.
Multivariate Analysis
What is the association between migration and risk of HIV positivity among the youths in sub-Saharan Africa?
Some of the results of the bivariate associations presented above may be partly or wholly attributable to possible confounding factors, including random subnational and national effects. In particular, the multilevel analysis takes into account possible variation in survey design and unobserved covariates across countries. In this section, we examine the independent migration risk factors of HIV infection among the youths, taking into account the effect of other important factors in the relationship. Factors considered to be important in HIV infection among youths in sub-Saharan Africa are introduced to the model in successive stages to help us understand potential pathways of the determinants (Table 4). Model 1 examines the overall risk factor of migration status across countries and regions (within countries) in sub-Saharan Africa. Model 2 takes into account the role of background demographic (age and marital status), socioeconomic (urban/rural residence, educational attainment, schooling status, media exposure, and household wealth index), and familial (orphanhood status, kinship [i.e., relationship to household head], and gender of household head) factors. The final model (model 3) includes sexual behavior factors.
Multilevel Logistic Regression Parameter Estimates of HIV Infection among Youths in Sub-Saharan Africa
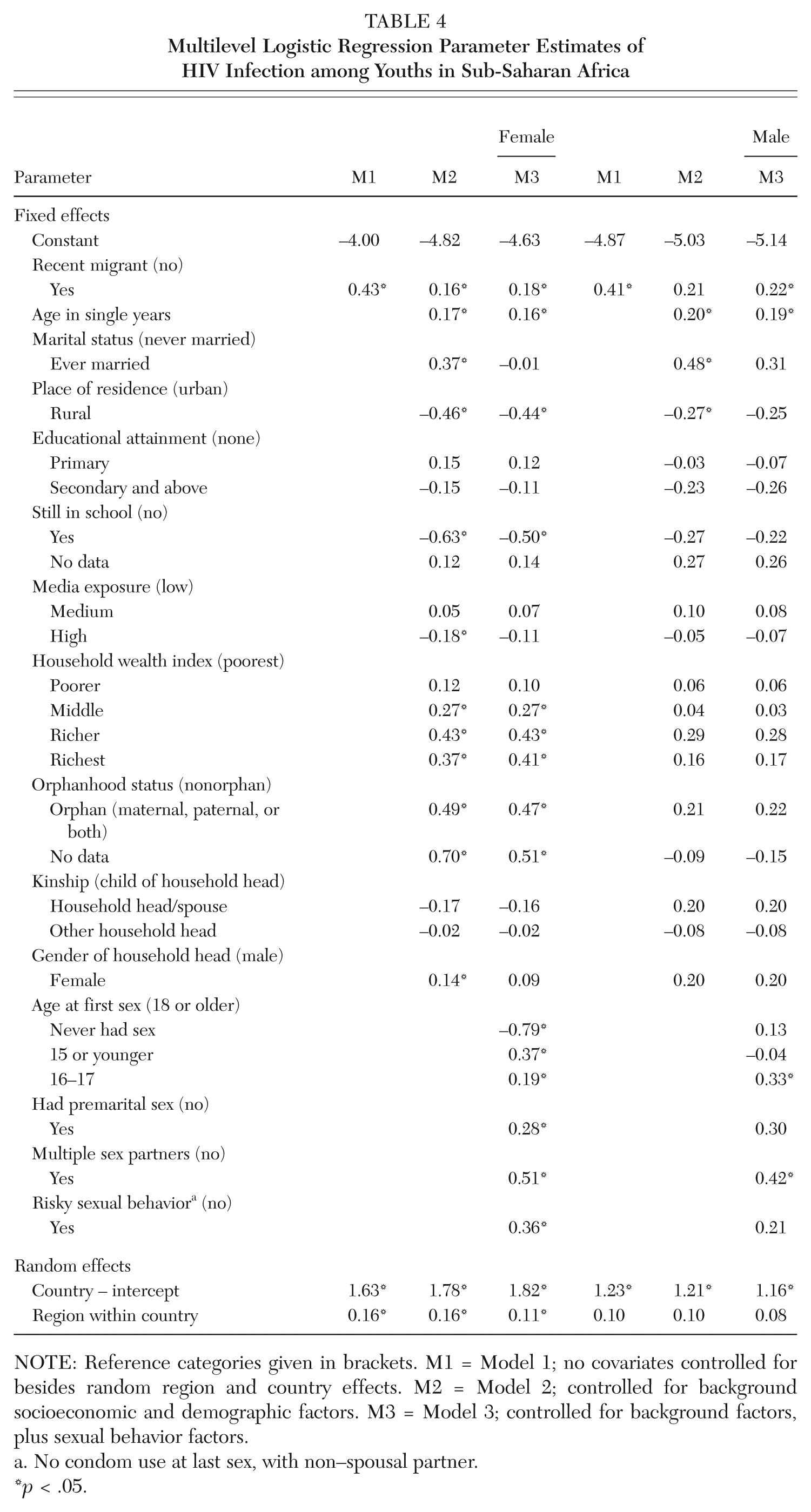
NOTE: Reference categories given in brackets. M1 = Model 1; no covariates controlled for besides random region and country effects. M2 = Model 2; controlled for background socioeconomic and demographic factors. M3 = Model 3; controlled for background factors, plus sexual behavior factors.
No condom use at last sex, with non–spousal partner.
p < .05.
The results in Table 4 suggest that both young women and men who are migrants have significantly higher risks of HIV positivity than their nonmigrant counterparts. Across countries and regions in sub-Saharan Africa, migrants have on average about 50 percent higher risk of HIV infection than nonmigrants. The higher risk among migrants is to a large extent explained by differences in demographic and socioeconomic factors. In particular, recent migrants are more likely to be older, to be ever married, and to live in urban areas, all of which are associated with higher risks of HIV infection. As might be expected, the higher risk of HIV positivity among the youths who are ever married is largely explained by sexual activity, particularly earlier age of sexual debut. Overall, both socioeconomic and sexual behavior factors appear more significant in explaining the risk of HIV infection among young women than among young men.
We investigated whether there was variation in the effect of migration status on the risk of HIV infection across countries, using random coefficient models. However, there was no evidence that the association between migration status and HIV positivity among the youths in sub-Saharan Africa varied significantly across countries with different HIV prevalence. This suggests that the patterns observed in the risk of HIV positivity by migration status are fairly consistent across countries in sub-Saharan Africa and may be generalizable for the region.
An examination of the gender disparity in the risk of HIV infection (see Table A1 in the appendix) suggests that across countries in sub-Saharan Africa, young women aged 15 to 24 have on average about triple (3.2 times) the odds of HIV infection as do their male counterparts of similar age. The odds are somewhat reduced (2.5 times) when demographic and socioeconomic characteristics are controlled for, but increased somewhat (2.8 times) when sexual behavior factors are controlled for.
Risk factors of HIV infection among youth migrants in sub-Saharan Africa
An analysis of factors associated with the risk of HIV infection among young female and male migrants (Table 5) suggests patterns similar to the ones observed for overall youths, with respect to age, marital status, urban/rural residence, orphanhood status, gender of household head, age at first sexual experience, and risky sexual behavior, 2 although the effect size for some factors appears larger for migrants. On average, a unit increase in age between ages 15 and 24 is associated with an increase in the risk of HIV infection of about 15–20 percent among young women and 20–25 percent among young men. The age patterns are fairly consistent between migrants and nonmigrants. The higher risk among ever married youths is particularly pronounced among young female migrants. For instance, young ever married women (migrants and nonmigrants combined) have about a 45 percent higher risk of HIV infection than their never married counterparts, but the risk is almost 80 percent higher among young female migrants.
Multilevel Logistic Regression Parameter Estimates of HIV Infection among Youth Migrants
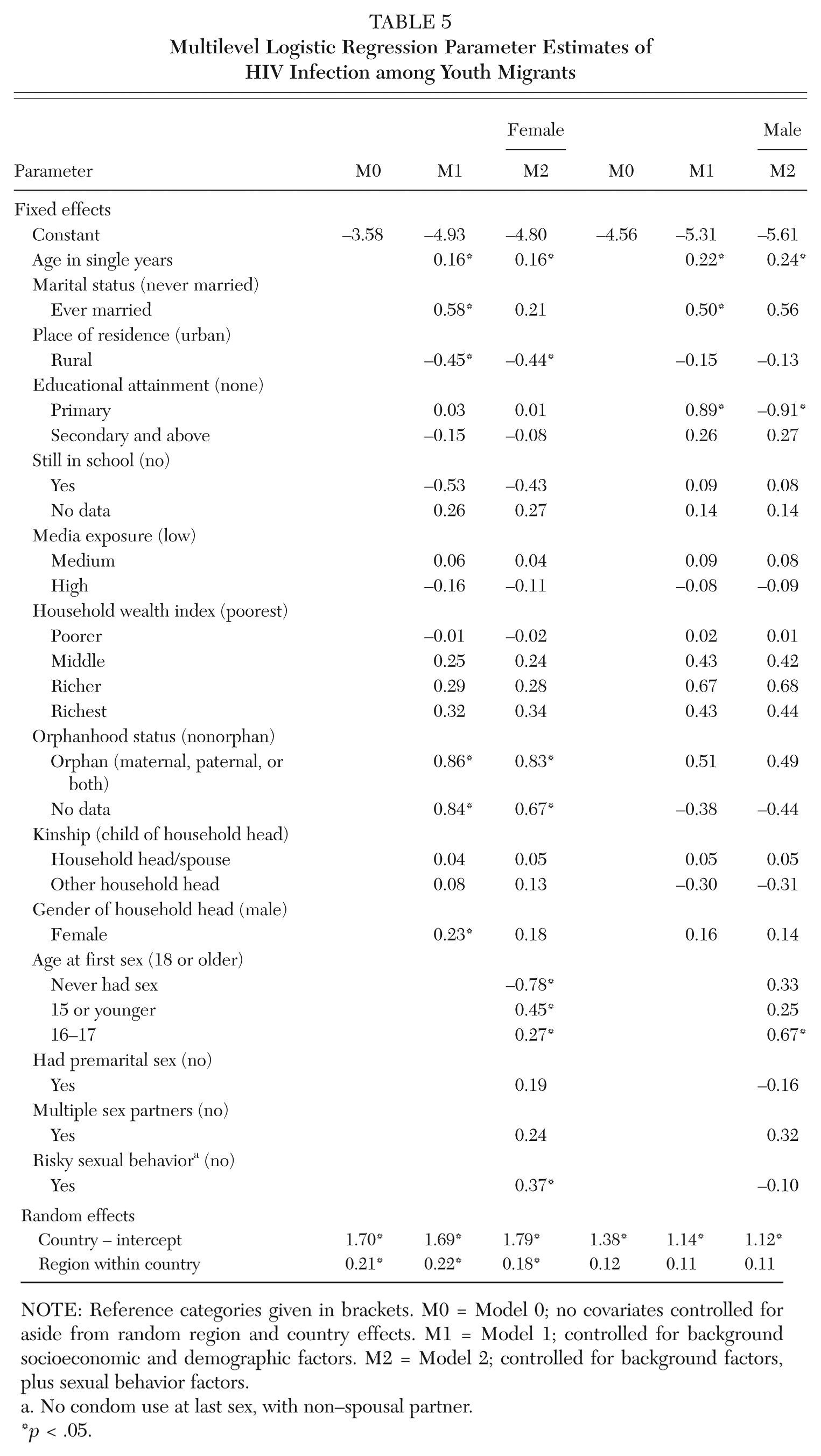
NOTE: Reference categories given in brackets. M0 = Model 0; no covariates controlled for aside from random region and country effects. M1 = Model 1; controlled for background socioeconomic and demographic factors. M2 = Model 2; controlled for background factors, plus sexual behavior factors.
No condom use at last sex, with non–spousal partner.
p < .05.
Interesting gender differences are observed with respect to orphanhood status, gender of household head, and age at first sexual experience, all of which appear important for young female migrants but not their male counterparts. On average, young female migrants who are orphans have more than double the odds of HIV infection than their nonorphan counterparts of similar characteristics. This remains virtually unchanged even after risky sexual behavior factors relating to timing of first sexual experience, premarital sex, multiple sex partners, and non–condom use with non–spousal partner are all controlled for. Although male orphans also seem to have a higher risk than their nonorphan counterparts, there is no evidence that the relationship is statistically significant. Also, young female migrants who live in female-headed households; or had sexual debut early, before the age of 16; or reported non–condom use with a non–spousal partner are all significantly more likely to be infected with HIV than their counterparts of similar characteristics in male-headed households, or who had sexual debuts at age 18 or older, or did not engage in risky sexual behavior, respectively. However, there is no evidence that these relationships are significant among young male migrants.
Overall, there are significant variations in the risk of HIV infection among youth migrants across countries in sub-Saharan Africa, and to a lesser extent across regions within countries. The intraunit correlations suggest that about 34 percent of the total unexplained variation in the risk of HIV infection among young female migrants in sub-Saharan Africa is attributable to unobserved country-level factors. The corresponding figure for males is slightly lower at 25 percent.
An examination of the gender disparity in HIV infection among youth migrants suggests that across countries in sub-Saharan Africa, women are on average about three times more likely (odds ratio = 3.2) to be infected with HIV than their male counterparts (Table A2 in appendix). When background characteristics and sexual behavior factors (i.e., sexual activity and timing of sexual debut, multiple partners, premarital sex, and risky sexual behavior) are controlled for, the risk among women is still 2.5 times higher. The gender disparity in HIV infection among youth migrants is somewhat consistent with overall patterns for youths in sub-Saharan Africa (see Table A1).
Discussion and Conclusion
Our results suggest that both young women and men who are migrants across countries in sub-Saharan Africa have significantly higher risks of HIV positivity than their nonmigrant counterparts. The higher risk among migrants is to a large extent explained by differences in demographic and socioeconomic factors. The observed patterns partly support the argument that migration is not itself a risk factor for HIV, but that the circumstances associated with movement increase vulnerability to HIV infection (UNAIDS 2009). In particular, recent migrants are more likely to be older, to have been married, and to live in urban areas, all of which are associated with higher risks of HIV infection. As might be expected, the higher risk of HIV positivity among the youths who are ever married is largely explained by sexual activity, particularly earlier age of sexual debut.
The analysis of factors associated with the risk of HIV infection among young female and male migrants shows general patterns similar to the ones observed for youths overall, suggesting a higher risk among those who are older, who are ever married, who are urban residents, who are orphans, who are living in female-headed households, who initiated sexual activity at a younger age, and who reported non–condom use with a non–spousal partner. However, the effect size for some factors appeared larger for migrants than nonmigrants. In particular, the higher risk of HIV infection among orphans and ever married youths was particularly pronounced among young female migrants. It is important that efforts to curb the spread of HIV infection among youths in sub-Saharan Africa pay special attention to the particularly vulnerable subgroups, such as orphans or ever-married young female migrants.
The findings on risk factors of HIV infection among youths in sub-Saharan Africa highlight important gender differences. The observed gender disparities among youth migrants are generally consistent with overall patterns for youths in sub-Saharan Africa. For both migrant and nonmigrant youths, the risk of HIV infection among women was more than triple that of men. This disparity is to a small extent explained by demographic and socioeconomic characteristics, but not sexual behavior factors. The latter supports the view from earlier studies that sexual behavioral factors cannot fully explain the gender disparity in HIV infection and that greater biological susceptibility of women to HIV infection is possibly an important factor in explaining the male-female disparity in HIV prevalence (Glynn et al. 2001; Magadi 2011b). Greater biological susceptibility is particularly pronounced among youths, with young women (both migrants and nonmigrants) having more than double the odds of HIV infection of their male counterparts of similar background characteristics and sexual behavior. The particularly marked gender disparity in HIV infection among youths had been previously attributed to biological and psychosocial factors (Rosenthal, Smith, and Visser 1999; UNAIDS 2003) and to women having older sexual partners who have had greater exposure to the risk of HIV infection (MacPhail, Williams, and Campbell 2002; WHO 2003; Sa and Larsen 2008). Furthermore, both socioeconomic and sexual behavior factors were observed to be more significant in explaining the risk of HIV infection among young women than among young men. These findings highlight the importance of gender-specific interventions in curbing the spread of HIV infection among youths in sub-Saharan Africa.
Our analysis included an examination of whether there was variation in the effect of migration status across countries, but the results provided no evidence that the association between migration status and HIV positivity among youths in sub-Saharan Africa varied significantly across countries. This suggests that the patterns observed in the risk of HIV positivity by migration status may be generalizable across countries in the region of sub-Saharan Africa. However, this finding should be interpreted with caution, especially since the sample of nineteen countries included in this study does not necessarily constitute a random and representative sample of all countries in sub-Saharan Africa.
Overall, the results presented in this article provide a general picture of patterns relating to migration as a risk factor of HIV infection among youths across countries in sub-Saharan Africa. More targeted studies focusing on specific issues or individual countries would be required to guide specific policy and program efforts. Nevertheless, this article identifies some general issues that are useful for relevant international policy and programs across countries in sub-Saharan Africa, as well as for areas that warrant more targeted research. In particular, the observed vulnerability of orphans and ever married young female migrants calls for further research to better inform relevant international and national policies and programs.
Footnotes
Appendix
Gender Disparity in HIV Infection among Youth Migrants in Sub-Saharan Africa
| Parameter | M0 | M1 | M2 |
|---|---|---|---|
| Fixed effects | |||
| Constant | −4.62 (0.296) | −5.46 (0.425) | −5.49 (0.440) |
| Gender (male) | |||
| Female | 1.16 (0.091)* | 0.86 (0.101)* | 0.93 (0.104)* |
| Age in single years | 0.16 (0.020)* | 0.16 (0.021)* | |
| Marital status (never married) | |||
| Ever married | 0.63 (0.106)* | 0.41 (0.123)* | |
| Place of residence (urban) | |||
| Rural | −0.37 (0.100)* | −0.36 (0.099)* | |
| Educational attainment (none) | |||
| Primary | 0.15 (0.143) | 0.13 (0.143) | |
| Secondary and above | −0.13 (0.153) | −0.09 (0.154) | |
| Still in school (no) | −0.39 (0.219) | −0.35 (0.219) | |
| Yes | 0.12 (0.301) | 0.10 (0.302) | |
| No data | |||
| Media exposure (low) | |||
| Medium | −0.02 (0.101) | −0.01 (0.101) | |
| High | −0.17 (0.116) | −0.14 (0.116) | |
| Household wealth index (poorest) | |||
| Poorer | −0.02 (0.152) | −0.03 (0.152) | |
| Middle | 0.27 (0.145) | 0.27 (0.145) | |
| Richer | 0.36 (0.149)* | 0.36 (0.149)* | |
| Richest | 0.35 (0.167)* | 0.38 (0.167)* | |
| Orphanhood status (nonorphan) | |||
| Orphan (maternal, paternal, or both) | 0.70 (0.250)* | 0.70 (0.252)* | |
| No data | 0.50 (0.214)* | 0.37 (0.215) | |
| Kinship (child of household head) | |||
| Household head/spouse | 0.02 (0.132) | 0.01 (0.131) | |
| Other household head | −0.01 (0.119) | 0.00 (0.019) | |
| Gender of household head (male) | |||
| Female | 0.25 (0.085)* | 0.23 (0.085)* | |
| Age at first sex (18 or older) | |||
| Never had sex | −0.38 (0.156)* | ||
| 15 or younger | 0.37 (0.108)* | ||
| 16–17 | 0.33 (0.100)* | ||
| Had premarital sex (no) | |||
| Yes | 0.15 (0.101) | ||
| Multiple sex partners (no) | |||
| Yes | 0.12 (0.154) | ||
| Risky sexual behavior a (no) | |||
| Yes | 0.26 (0.107)* | ||
| Random effects | |||
| Country – intercept | 1.42 (0.502)* | 1.46 (0.520)* | 1.48 (0.524)* |
| Region within country | 0.18 (0.056)* | 0.18 (0.058)* | 0.16 (0.053)* |
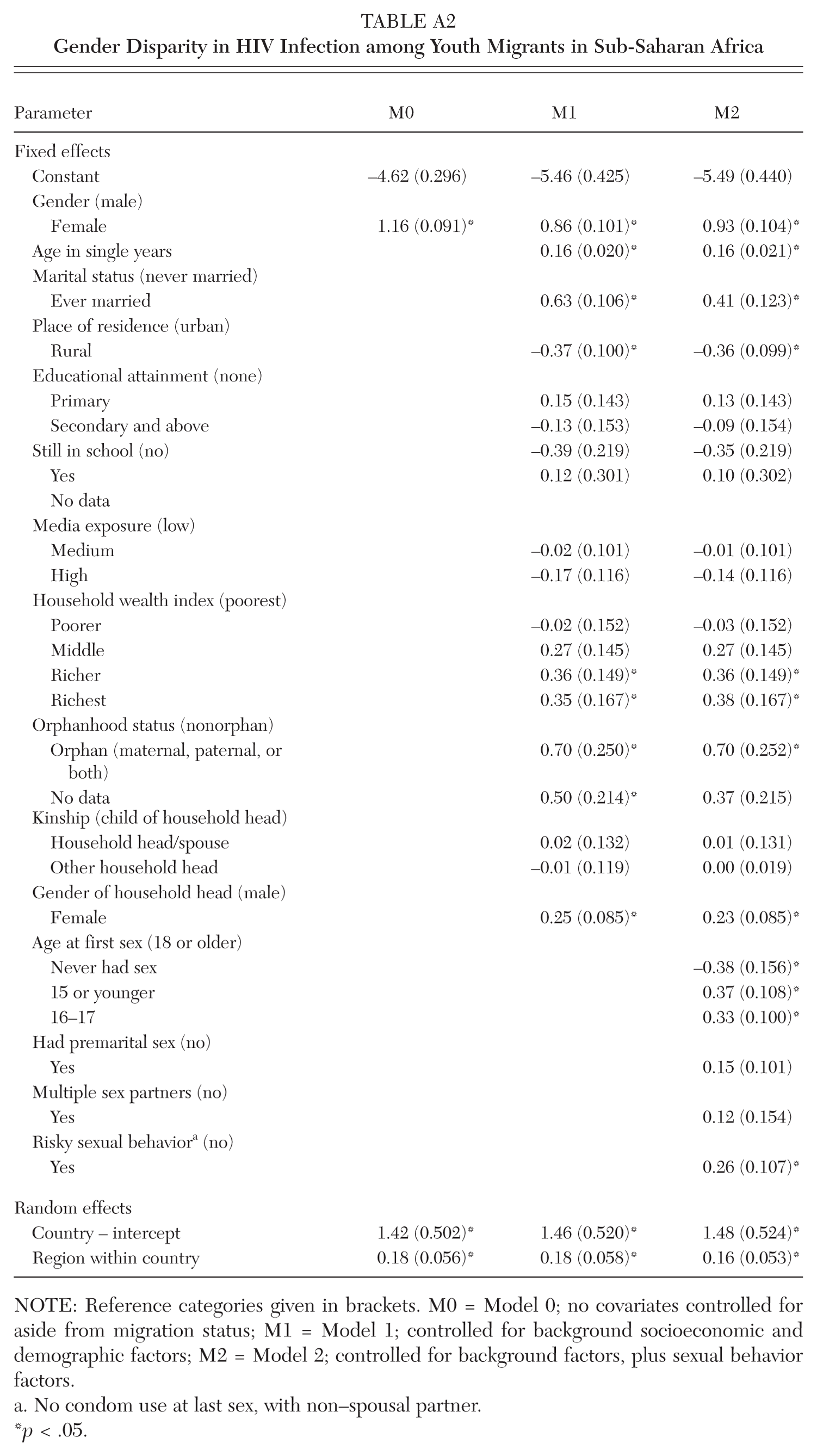
NOTE: Reference categories given in brackets. M0 = Model 0; no covariates controlled for aside from migration status; M1 = Model 1; controlled for background socioeconomic and demographic factors; M2 = Model 2; controlled for background factors, plus sexual behavior factors.
No condom use at last sex, with non–spousal partner.
p < .05.
NOTE:
This study was part of a secondary data analysis project on HIV/AIDS and the well-being of children in sub-Saharan Africa, sponsored by the UK Medical Research Council (MRC). The data analyzed were provided by the Demographic and Health Surveys (DHS) program, ICF Macro, Calverton, Maryland.
Notes
Monica A. Magadi is a professor of social research in the Department of Social Sciences at the University of Hull in the United Kingdom. Her background is in demography and social statistics. She focuses on international research in the area of reproductive health in sub-Saharan Africa, including maternal/child health, HIV/AIDS, and adolescent sexual and reproductive health.