
Abstract
The majority of alleged abuse or neglect reports to the U.S. child welfare system are either screened out prior to an investigation (i.e., at the “hotline” stage) or investigated only to be closed with no finding of immediate child safety concerns. Yet while many of these children and families are at risk of subsequent incidents of child maltreatment or child welfare system involvement, they are not systematically offered services or benefits intended to reduce this risk at the point that child protective services (CPS) ends its involvement. This article provides an overview of the “front end” of the child welfare system, commonly referred to as CPS, highlighting which families are served and which are not. We then argue for a systematic and coordinated child maltreatment prevention infrastructure that incorporates elements of “community response” programs that several U.S. states have implemented in recent years. Such programs are focused on families that have been reported to, and sometimes investigated by, CPS, but no ongoing CPS case is opened. We further argue that such programs need to pay particular attention to economic issues that these families face.
Keywords
Although the federal government created the Children’s Bureau in 1912, with the mission to study and report on a wide range of matters affecting the welfare of children, child protective services (CPS) in the United States were not formally codified by the federal government until 1962. In that year, Congress passed amendments to the Social Security Act that required states to establish statewide child welfare systems by 1975. Prior to the passage of these amendments, child protection activities were a function of nongovernmental entities, often called “Societies for the Prevention of Cruelty to Children” (SPCCs), which were not uniformly available within or across states (Myers 2004). The Title IV-E amendments to the Social Security Act established a dedicated funding stream to states to partially support (along with state-matching funding) the care and service needs of children who meet federal eligibility requirements and are placed in out-of-home care (e.g., foster care, institutional care) for reasons of abuse or neglect, and later for adoption and kinship guardianship assistance.
Several other major laws influencing child protection practice have passed since the early 1960s, but our approach to child protection in the United States is now at an inflection point. After steadily declining from 2002 to 2012, foster care caseloads have increased substantially since 2012 and are now at their highest level in more than two decades (Child Trends Databank 2019; Radel et al. 2018; U.S. Department of Health and Human Services 2019). Moreover, they may become more pronounced in the midst and aftermath of the COVID-19 pandemic to the extent that the pandemic creates or exacerbates economic stress within families, a known risk factor for child maltreatment (Slack, Berger, and Noyes 2017). This uptick may occur despite that child maltreatment reports decreased substantially during periods of school closures and state and local lockdowns due to a corresponding decline in children’s face-to-face interactions with mandated reporters in schools, childcare centers, and other child-serving systems (Stewart 2020; Welch and Haskins 2020). In addition, new evidence and new opportunity afforded by policy combine to warrant a rethinking of the approach to child protection in the United States, including research illustrating the striking cumulative incidence of childhood CPS system involvement (Kim et al. 2017; Wildeman et al. 2014), the exorbitant economic costs of child maltreatment (Peterson, Florence, and Klevens 2018), persistent disproportionality in CPS involvement by race and ethnicity (Dettlaff et al. 2011; Drake et al. 2011; Johnson-Motoyama et al. 2015; Wildeman et al. 2014), and the recent passage of the Family First Prevention Services Act of 2018 (P.L. 115-123) to expand the scope of child welfare systems further into the prevention realm.
In this article, we focus on the “front-end” of the U.S. child welfare systems, which comprises CPS functions, where reports of abuse and neglect are screened, and decisions are made to investigate and initiate services to address situations of child maltreatment. We review who is currently served by CPS and how effective these systems are in identifying maltreatment, and we attend to an important overlooked population of families at risk for child maltreatment—those reported to CPS, but that, upon further screening and investigation, are not ultimately served by that system. We then propose a prevention infrastructure that attends to this population, and we highlight the multiple systems external to CPS positioned to influence rates of child maltreatment.
Whom Do CPS Systems Serve and Not Serve?
Currently, CPS systems in the United States have four primary functions: (1) vetting referrals of alleged abuse and neglect incidents that an array of professionals and the general public report, (2) further assessing or investigating the referrals that appear to meet state statutory definitions of child maltreatment, (3) providing in-home services to families as well as services to families whose children are removed for safety concerns and placed in out-of-home care, and (4) closing cases of abuse or neglect through service plan completions or establishment of permanent placements for children who cannot remain or be reunified with their families of origin (Institute of Medicine and National Research Council [IOM and NRC] 2014).
The passage of the Adoption and Safe Families Act of 1997 established federal regulations for “Child and Family Service Reviews,” which carried the mandate of ensuring the safety, permanency, and well-being of children once they are involved in CPS. Notably, none of these functions and mandates supports the prevention of child abuse and neglect—rather, CPS systems are explicitly charged only with responding to allegations of child maltreatment and attending to the service needs of children and families once they are involved with CPS. With the recent passage of the Family First Prevention Services Act of 2018, states may now use Title IV-E (as well as Title IV-B 1 ) funding for the purpose of preventing out-of-home placements of children. Testa and Kelly (this volume) offer an overview of this new law and its implications for child welfare systems; Haskins (this volume) offers an overview of child welfare funding.
Over the last 25 years, many states have established “alternative response” (AR) (also called “differential response”) pathways within their CPS systems. States established AR pathways primarily in reaction to traditional CPS system practices that tended to treat families similarly despite variation in the level and nature of presenting risk and protective factors. Families with fewer and less serious risks or child safety concerns could be placed on an AR path characterized by greater collaboration between CPS and the family, and an “assessment” rather than an “investigation” approach to developing a service plan (Maguire-Jack, Slack, and Berger 2014). Under an AR model, families reported for less severe situations of maltreatment or maltreatment risk are offered voluntary services by CPS. The focus of the CPS caseworker’s initial contacts with a family is on collaborative needs assessment and developing a service plan to maintain child safety in the home and reduce the likelihood of maltreatment risk escalating. Under a traditional CPS model, an investigative approach is taken to determine whether maltreatment allegations should be substantiated and whether to open an ongoing case, remove a child from the home, and require services that are typically court-ordered and thus mandatory. The distinction between the two models or tracks is partly a function of how a caseworker approaches and engages with a family and partly a function of the stakes being much higher for a family under the traditional CPS model. We should note, however, that even families referred to an AR track are at risk of having a child removed from the home if caseworkers determine that the situation becomes unsafe for a child. Thus, despite the more collaborative model of AR, AR services are not entirely voluntary, given that families are most likely keenly aware of the potential for more intrusive levels of CPS involvement. Figure 1 provides an overview of the various decision points that capture the primary CPS functions, beginning with a report of child maltreatment to CPS, followed by a screening decision, an investigation or assessment decision, a child removal decision, and a case closure outcome.
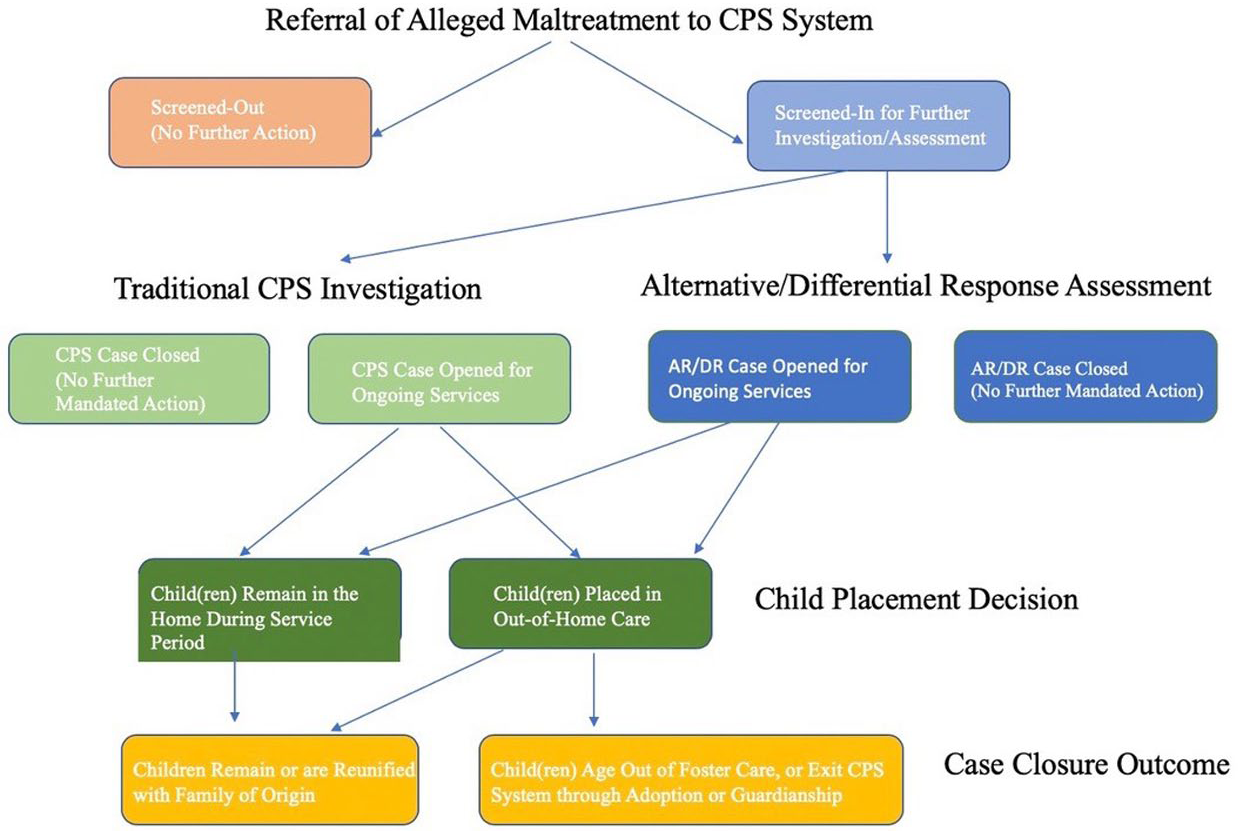
Family Pathways in Child Protective Services (CPS) Systems
The most recent data from the U.S. Department of Health and Human Services (2020) indicate that, in 2018, CPS systems received 4.3 million referrals (reports) of suspected child abuse or neglect involving 7.8 million children (5.9 percent of all U.S. children). Approximately 56.0 percent of these referrals were screened in for a CPS response (either AR or a traditional investigation), while 44.0 percent were screened out at the referral stage, meaning that CPS did not pursue these cases further. In all, 4.8 percent of U.S. children were the subject of a CPS investigation for alleged maltreatment. Of these, CPS determined 16.8 percent to be a child maltreatment victim (received a case disposition that the maltreatment allegations were substantiated or indicated), 2 14.0 percent received AR (such that they were not subject to the substantiation decision process), and 56.3 percent received a case disposition that the maltreatment allegations were unsubstantiated. As such, 9.2 per 1,000, or nearly 1.0 percent of U.S. children, were deemed to be maltreatment victims, with 84.5 percent of victims experiencing a single type of (substantiated) abuse or neglect 3 and 15.5 percent experiencing multiple types. 4 The vast majority of perpetrators were children’s parents (77.5 percent). Among those children who were investigated, 60.7 percent of children deemed victims and 29.0 percent deemed nonvictims (e.g., siblings of victims) received some postinvestigation services; these figures include the 22.9 percent of victims and 1.9 percent of nonvictims who were removed from their homes. Federal data do not provide information on the rate of cases opened for ongoing CPS services, so these percentages may not fully capture all families with continued CPS involvement following an investigation.
Taken together, these data highlight that the vast majority of reports result in no ongoing CPS intervention for the children and families who are their subjects. Specifically, the data indicate that (1) 44.0 percent of reports do not receive an investigation; (2) among the 56.0 percent of reports that are investigated, only 16.8 percent result in a maltreatment substantiation; and (3) only 60.7 percent of children deemed victims and 29.0 percent of those deemed nonvictims receive services. This suggests that only about 19.3 percent of reports result in ongoing (postinitial CPS response) services, whereas fully 80.7 percent do not. Furthermore, among those reports subject to an investigation, only 34.3 percent receive ongoing services, whereas 65.7 percent do not. Yet families referred to CPS only to have their case screened out or to have an investigation that does not result in a substantiation that abuse or neglect occurred—as measured by current legal thresholds—subsequently become reinvolved with CPS at high rates (Drake et al. 2003; Hindley, Ramchandanli, and Jones 2006; Jedwab, Harrington, and Dubowitz 2017). For example, recent evidence from Wisconsin indicates that between 2004 and 2016, 26.5 percent of families that experienced a report that was initially screened in (investigated) but received an unsubstantiated case disposition were rereported to CPS, and 22.1 percent had a subsequent screened-in report and 4.4 percent a subsequent substantiated report, within 12 months of the initial report. 5 Despite concerning rates of subsequent (and escalating) CPS involvement, however, preventive interventions are not systematically offered to this group of families, some portion of whom may never be in need of CPS intervention, some who may have had their CPS cases incorrectly closed at the screening or investigation stage, and some of whom may have persistent or increasing needs related to child safety that only become evident over time.
There is widespread variation across states in terms of mandatory-reporting laws, child abuse and neglect definitions and associated levels of evidence required for substantiation, and CPS system structures and features, as well as referral, investigation, substantiation, and postresponse service receipt (including out-of-home placement) rates. A discussion of variation in mandated-reporting laws and maltreatment definitions and levels of evidence required for substantiation is provided by Berger and Slack (this volume) and Font and Maguire-Jack (this volume). Key dimensions of state CPS system structures and features include the extent to which a system is state or county administered and whether a state (or county) has implemented AR. In all, forty states (including Washington, D.C., and Puerto Rico as states for this purpose) operate state-administered systems. Ten states operate county-administered but state-supervised systems (California, Colorado, Minnesota, New York, North Carolina, North Dakota, Ohio, Pennsylvania, Virginia, and Wyoming), and two states (Nevada and Wisconsin) operate hybrid systems in which some CPS functions are administered at the state level and others at the county level (Child Welfare Information Gateway, 2018). Centralized and decentralized CPS systems may produce different patterns across the systems’ decision points, leading to more or less consistent practice depending on the model. Currently, twenty-three states report AR data to the federal government, though additional states may engage in AR at the county or, to some extent, state level. Moreover, AR program designs vary across states.
There is also widespread variation across states in CPS reports (with rates ranging from 1.6 percent of children in Hawaii to 16.8 percent of children in Vermont), investigation (1.3 percent of children in Hawaii to 14.4 percent of children in West Virginia), substantiation (0.18 percent of children in Pennsylvania to 2.4 percent of children in Kentucky), and postresponse service receipt (18.7 percent of child maltreatment victims in Illinois to 100 percent of victims in Iowa and Tennessee; out-of-home placement rates among victims range from 5.2 percent in Kentucky to 48.8 percent in Hawaii) rates. 6 In addition, there is considerable county-level variation in these rates, as well, typically reflecting differences in both CPS practices and underlying sociodemographic characteristics of the population, as well as in the economic and sociopolitical contexts. Such variation may have substantial implications for the likelihood that children and families receive CPS services, which children and families receive services, and what types of services they receive. They may also reflect or affect CPS’s capacity to respond to and serve the population at risk in a specific locale.
How Well Does the CPS System Work in Identifying Child Maltreatment?
Given the profound implications of child maltreatment for children’s concurrent well-being and their ongoing well-being over the life course, as well as the extraordinarily intrusive and intensive nature of governmental intervention in response to child safety concerns, the stakes are high for CPS systems to simultaneously achieve high levels of sensitivity (the ability to correctly identify and serve families experiencing maltreatment) and high levels of specificity (the ability to correctly exclude families not experiencing maltreatment from CPS intervention). 7 Higher rates of sensitivity almost certainly lead to the overinclusion of families, whereas higher rates of specificity may lead to the underinclusion of families, two issues that have plagued CPS systems for decades (Waldfogel 1998). To date, the United States has conducted four National Incidence Studies (NIS) to estimate rates of child maltreatment in the general population, regardless of CPS involvement. Results from the most recent study, NIS-4, conducted in 2006, suggest an incidence rate of 17 per 1,000 children using a conservative standard, and 40 per 1,000 children using a more inclusive standard (Sedlak et al. 2010). That the NIS estimates of child maltreatment known to “community sentinels” well exceed rates of CPS involvement indicates that many children who may be victims of abuse or neglect are not known to CPS. Dettlaff and Boyd (this volume) provide insight about disparities in CPS involvement across racial and ethnic groups, stemming from historical, structural, and environmental challenges associated with racially biased practices, policies, and resource allocation contexts. New laws, the economy, changes to the social safety net, media coverage of egregious incidents of child maltreatment, and issues related to CPS system capacity can also affect patterns of overinclusion and underinclusion, as well as public health crises like the COVID-19 pandemic, currently depressing CPS reports around the country (Welch and Haskins 2020). In sum, there are a wide range of reasons that families may be overincluded or underincluded in CPS systems, some of which can be changed or influenced by these systems, and some of which cannot.
While not all families in need of intervention are reported to CPS systems, families at risk for child maltreatment may be served outside of the CPS system through participation in voluntary, community-based services, some of which are specifically designed to prevent child abuse and neglect. Jones Harden and colleagues (this volume) provide a broad overview of such prevention services, many of which have demonstrated effectiveness. One of the key challenges in the child maltreatment prevention field is getting families to participate and engage in prevention services when they are not asking for or seeking support. This may be particularly problematic in the child maltreatment prevention arena, where issues of child safety are paramount. Families who elect to participate in voluntary services may not be the families most in need of an intervention to prevent child maltreatment. This selection problem has not been adequately studied, leaving open the question of whether some evidence-based voluntary prevention services are effective for families with higher levels of need. The existing research on predictors of participation and engagement tends to focus on samples that have had some form of contact with program staff, rather than the universe of eligible participants regardless of whether program contact is made, or “enrollment” is measured as the percentage of available spots that participants fill (Maternal, Infant, and Early Childhood Home Visiting Technical Assistance Coordinating Center [MIECHV TACC] 2015). This hinders our ability to learn how to engage high-risk populations, where the very reasons behind the need for prevention services may prevent families from seeking them out on their own. It also motivates the need for intent-to-treat evaluation designs, where eligible participants are randomly assigned to a treatment or control condition and information is collected about them prior to offering the treatment group intervention services. Such designs afford the ability to better understand which participants are most likely to engage in treatment services, and whether engagement and persistence in services is tied to different types and degrees of need.
Turning back to the CPS system, another consideration for system performance—one that internal system factors can arguably influence—is how often families reported to, but ultimately unserved by CPS, are rereported to CPS at some future point. If the system correctly ends involvement with families whose risk for maltreatment is low or nonexistent, then CPS recurrence among such families should be relatively low. However, several studies have demonstrated concerning rates of short-term CPS recurrence among families whose initial reports were unsubstantiated (Drake et al. 2003; Hindley, Ramchandani, and Jones 2006; Jedwab, Harrington, and Dubowitz 2017), suggesting that the system may be ending involvement with families who are actually in need of intervention to prevent child maltreatment—even if legally defined maltreatment has not yet occurred. These potential scenarios are further complicated by the fact that many families come to the attention of CPS for reasons related to poverty and material hardship (Slack et al. 2011), begging the question of whether their needs are best served by the CPS system. For the remainder of the article, we focus on the group of families for whom CPS involvement ends at the point of initial screening or investigation of a report of maltreatment. Little attention has, to date, been paid to this population at the point that CPS ends its involvement, even though this moment of contact creates an opportunity to assist families that may need and want assistance external to the child welfare system, and for whom such assistance may reduce future involvement with that system.
Families with Maltreatment Reports That Do Not Result in Ongoing CPS Involvement: An Underserved Population in Need of Services
As we described, approximately 80 percent of abuse and neglect reports do not result in ongoing intervention by CPS systems (U.S. Department of Health and Human Services 2020). Yet research suggests that a sizable percentage of families with this result are rereported to the system within a relatively short time frame. As such, families that come to the attention of CPS but are not provided ongoing services by that system constitute a population that may benefit from interventions to prevent the recurrence or escalation of risk factors for child maltreatment. Furthermore, families in this population may not be self-selecting into voluntary prevention programs in their community, rendering them underserved and, in most states, overlooked altogether.
Few existing services available to families at risk for or experiencing child maltreatment systematically attempt to engage or tailor services to meet the needs of families immediately following a CPS contact, when that contact does not result in ongoing CPS services. This is not to say that families who are reported to CPS are uninvolved in other service systems. In Wisconsin, for example, more than three-quarters of families whose cases are screened in for further investigation received Supplemental Nutrition Assistance Program (SNAP) benefits, and approximately 71 percent had BadgerCare (Wisconsin’s combined Medicaid and State Children’s Health Insurance program) coverage in the year prior to their CPS report. 8 However, such means-tested benefits may only partially address a family’s needs in terms of types or extent, or both. Furthermore, benefits tied to a family’s income and subject to regular redetermination requirements may fluctuate, creating economic stress and other hardships for a family (Ettinger de Cuba et al. 2019; Lee, Slack, and Lewis 2004). And families who are eligible for certain benefits may not take them up, sometimes by choice and other times because administrative burdens and hurdles prevent completion of the application process (Herd and Moynihan 2019; Wu and Eamon 2010). Moreover, these programs and benefits, which are intended to help families maintain stability, are not systematically enacted as part of a maltreatment prevention strategy.
In 2006, Wisconsin was one of the first states to design and implement a program, called community response (CR), which explicitly seeks to voluntarily engage families at the point that CPS decides not to open an ongoing case. 9 It is important to note that CR is not synonymous with AR programs that have proliferated in CPS systems around the country in recent decades. AR approaches are typically delivered within the context of CPS systems, whereas community-based prevention agencies that have no oversight by CPS provide CR services. Thus, CR participation is truly voluntary. CR fills a gap in the child maltreatment prevention continuum by serving families who “touch” the CPS system, but who are not further served by that system because their circumstances do not currently meet statutory definitions of maltreatment. This group may be offered ad hoc referrals to community services at the point of diversion from CPS, but typically they receive little to no further assistance at this juncture. The motivating rationale for contemporary CR programs is not a new story in the U.S. history of child welfare. As Testa and Kelly (this volume) describe, amendments to the Social Security Act in the mid-twentieth century laid a foundation for social services to promote stability for families receiving income support as an explicit means for keeping families intact. While these services were not offered at the same system point as CR programs, they targeted a largely similar population—disadvantaged families whose economic stressors could easily be conflated with “child neglect.”
CR programs aim to promote stable home environments for families experiencing stressors, prevent child maltreatment, and reduce rereferrals to CPS. CR interventions are meant to be short term (i.e., 12–16 weeks) and typically include at least one home visit from the CR worker; an assessment of family strengths, needs, and stressors; collaborative goal-setting between the primary caregiver(s) and the CR worker; and flexible funds for addressing critical immediate financial stressors. In many ways, CR programs mirror the premise and nature of kinship navigator programs that are eligible for federal funding through the Family First Prevention Services Act of 2018, discussed in Testa and Kelly (this volume), with the critical difference that CR programs are intended to keep children with their families of origin, rather than focusing on supporting kinship arrangements that emerge in response to the breakdown of a child’s birth or adoptive home, a point to which we return.
Using information from family assessments, staff work with the primary caregiver(s) to collaboratively set and prioritize goals to address select economic and/or psychosocial needs and assist with connecting the family to formal and informal resources (e.g., in-kind and cash benefits, parenting supports, mental health treatment, and child health and development services). Through the course of the intervention, the worker has at least biweekly contact with the participating family. Contacts include phone calls and in-home visits or face-to-face visits in a location convenient for the primary caregiver. Figure 2 illustrates the case flow of the intervention.
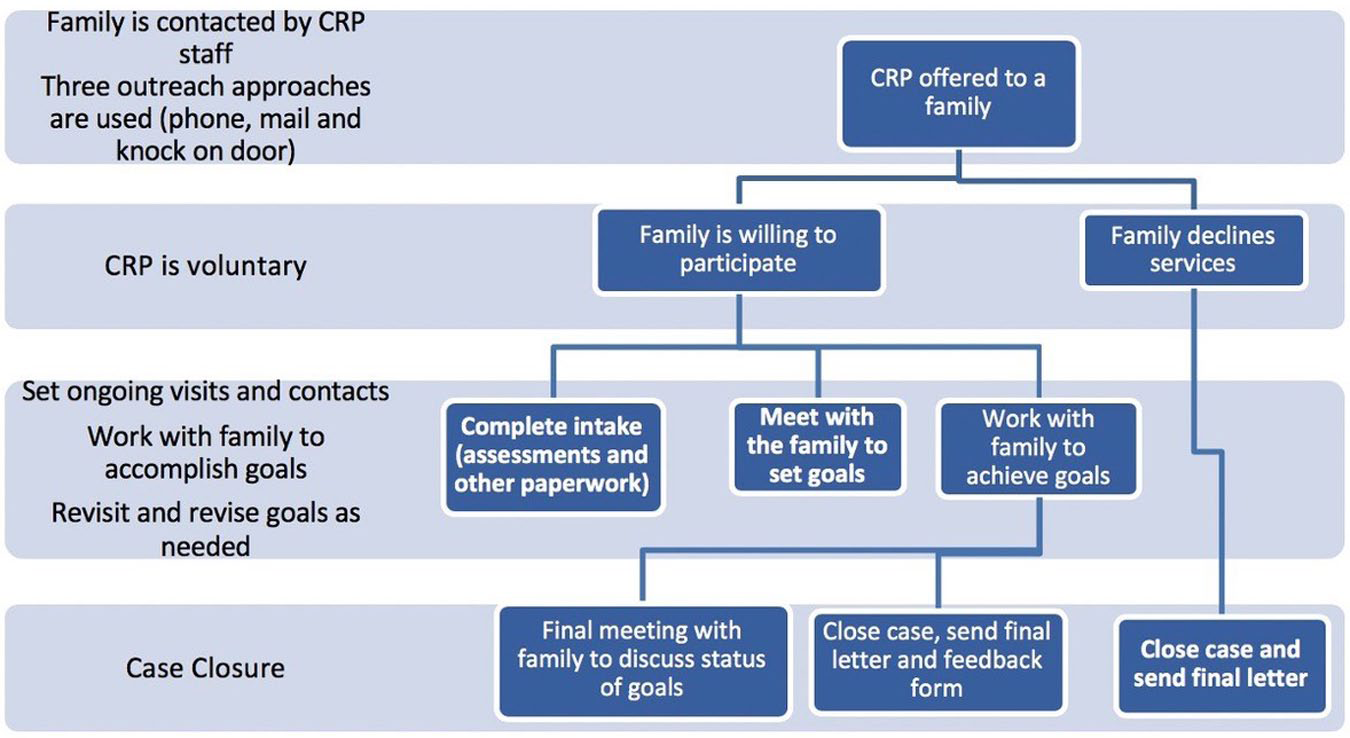
Community Response Case Flow
While the goal of expanding the child maltreatment prevention continuum by adding the CR component is laudable, whether CR was a feasible service model that families would want to access voluntarily, particularly on the heels of a CPS contact, was unknown. The initial six CR sites in Wisconsin participated in an implementation evaluation that allowed the Wisconsin Child Abuse and Prevention Board, Wisconsin Department of Children and Families, and site teams to learn whether and the extent to which families would participate in CR, the types of needs these families expressed, and their progress once enrolled in the program. The evaluation also allowed sites time to work through the initial stages of coordinating referrals from county CPS agencies. Given the novelty of working on a larger scale with families diverted from CPS, primary foci of the implementation evaluation were issues and concerns related to information-sharing, child safety, and how best to conduct outreach with the intended service population.
From the implementation evaluation, several key findings emerged (Maguire-Jack, Slack, and Berger 2014). First, the program acceptance rate by families ranged from 28 percent to 83 percent across sites, with an overall acceptance rate of about half. This exceeded the expectations of many of the program stakeholders. Second, sites that focused on families whose CPS involvement ended at the investigation stage tended to have higher participation rates than sites focusing on families that were screened out at the report stage. This made sense, given that families screened out at the report stage often had less accurate contact information. They also typically had no knowledge that they were the subject of a CPS report alleging child maltreatment, and many declined services out of concern that involvement in CR would lead to more unwanted surveillance. When CR sites received referrals from CPS, the CPS worker provided a referral reason, which was most often related to parenting concerns. During the intake and assessment phase for families engaging in CR, parents and other primary caregivers most often defined their primary needs as economic and material. Given that CR is voluntary, having insight about the needs that families identified is important. The implementation evaluation also found that participants’ reports of public benefit receipt were modest at CR intake, despite very low levels of family income; although it was unclear from the implementation evaluation whether the lower-than-expected take-up of public benefits was a result of ineligibility for reasons other than income level, family preference, or difficulties navigating these benefit systems (Herd and Moynihan 2019; Wu and Eamon 2010). On the whole, 70 percent of participants made significant progress toward at least one service goal, and 57 percent attained at least one goal, as assessed by the CR worker. Notably, family identification of an income-related service goal was highly predictive of goal attainment (although this could have, in part, been a function of income-related service goals being more easily attained than other types of service goals).
In 2017, the Wisconsin Child Abuse and Neglect Prevention Board collected data on seven CR sites to assess program participation and engagement. In this group of CR programs, the average service take-up rate was lower than it was for the earlier group of programs (fielded in the late 2000s), ranging across sites from only 5 percent to nearly 30 percent, with an average acceptance rate of 12 percent. 10 Roughly one-third (31 percent) of CR participants had a service goal related to housing, followed by goals related to accessing resources (28 percent), parenting needs (25 percent), employment (24 percent), and mental health (22 percent). Goals related to economic needs (transportation, accessing means-tested benefits, utilities, basic needs, employment, housing, and other financial needs) were collectively identified by 53 percent of CR participants. Using an intent-to-treat randomized control trial design, we are currently conducting a program impact evaluation to determine if the CR program led to reductions in future CPS involvement.
Following Wisconsin’s CR initiative, which the state launched in 2006, other states have developed and adapted CR models and engaged in evaluation activities. In Colorado’s CR program, the take-up rate for services was 23 percent, and like in Wisconsin, income-related needs were most prevalent among participants (Colorado Office of Early Childhood 2019). Pre-post tests showed significant improvement in protective factors and a decrease in prevention needs, and a comparison of CR participants to a matched control group showed less maltreatment and fewer out-of-home placements of children in the CR group. Nebraska’s CR program also found income-related needs to be most prevalent, and retrospective pre-post tests showed improvements in four out of five domains (Jackson, Tourek, and Skoglund 2019). 11
Marathon County, Wisconsin, a small rural region of the state, also evaluated CR. The take-up rate for CR services was approximately 50 percent, and a comparison of families whom the program served and eligible families whom the program did not serve due to program capacity limitations (i.e., a waitlist group) showed lower rates of subsequent CPS involvement, including CPS contacts that resulted in the out-of-home placement of children, for those who received CR services (Maguire-Jack and Bowers 2014).
Milwaukee County implemented a version of Wisconsin’s CR model, Project GAIN (Getting Access to Income Now), which focused exclusively on assisting families with economic needs (it did not address psychosocial needs). An intent-to-treat randomized control trial evaluated Project GAIN, and the treatment group participation rate for the later cohort of families was 22 percent. 12 Results showed statistically insignificant effects, on the whole. However, although still not statistically significant, effect sizes tended to favor the treatment group for later cohorts (i.e., those selected into the sample after the first two years of the evaluation) and especially for economically disadvantaged families (Slack et al. 2020). Specifically, for the most disadvantaged income subgroups, effect sizes tied to reductions in CPS recurrence ranged from 10 to 24 percent, suggesting that subgroup analyses may have simply lacked sufficient statistical power to attain statistical significance. For higher-income families, statistically insignificant effects were in the opposite direction, however, such that those with higher incomes who were in the treatment group were more likely to have CPS reinvolvement than those with similar income levels in the control group. In sum, the CR model is not a panacea for child maltreatment prevention, and it may not be equally effective for all families who are reported to CPS. Nonetheless, it does show promise with some families. Ongoing research is needed to understand the complexities of this intervention vis-à-vis the needs and circumstances of particular families.
Taken together, the various CR initiatives under way in the United States suggest that (1) some families whose CPS involvement ends at the maltreatment report screening or investigation stage are willing to participate in voluntary services to help meet their needs; (2) the needs that families identify are largely economic in nature; and (3) participation in CR services may reduce the likelihood of future CPS involvement, at least in the short term and for families experiencing high levels of economic hardship. The fact that the CR model operates externally to CPS and involves case management to help families access a variety of community-based services and resources, as well as means-tested benefits and supports related to employment and housing, situates CR in a larger context. That is, as Feely and colleagues (this volume) discuss, other systems that serve children and families are inextricably tied to efforts to reduce child maltreatment—systems that are designed to serve high-risk populations (e.g., criminal justice, mental health, economic support systems), as well as more universal systems and resources, such as schools, health care systems, and childcare. Feely and colleagues, therefore, argue that systems should recognize their role in child maltreatment prevention, something that is currently hindered by the siloed nature of the social welfare landscape in the United States.
But in the absence of a formalized system of services, benefits, and resources that authentically work together to reduce child abuse and neglect, is it possible to think about creating a child maltreatment prevention infrastructure? Our various social welfare, education, and health systems, among others, are heavily siloed, and individuals and families are faced with a maze of different eligibility and application procedures, rules, and regulations that can be difficult to navigate (Herd and Moynihan 2019; Slack et al. 2014; Wu and Eamon 2010), and about which families often lack information (Anderson 2002; Lee, Slack, and Lewis 2004). CR offers promise as a tool for helping families at risk for deeper-end involvement with CPS to access these systems as their needs and situations change. Such an approach is similar to the kinship navigator programs that the Family First legislation has authorized, and for which federal funding is available. Given that kinship navigator programs have garnered support in federal law despite not having a solid evidence base of their effectiveness, it can be argued that CR programs, which do show some evidence of effectiveness, may be better positioned to serve families at risk of deeper involvement with child welfare systems, including the placement of children into foster care (including kinship foster care), and to closely monitor these programs through rigorous evaluation.
Figure 3 offers an illustration of the various organizational and system components of a proposed prevention infrastructure. In the upper left corner of the figure, family support programs are community-based, voluntary programs that serve individuals or families universally (e.g., all resident families in a community), or selectively (e.g., families referred from other service providers due to the presence of risk factors for child maltreatment), regardless of past or current child welfare system involvement. In the lower right corner of the figure, traditional CPS systems intervene with children, parents, and families following a report of abuse or neglect that necessitates (as determined by an investigation and findings that align with the statutory scope of CPS) ongoing CPS involvement. AR programs serve families deemed to have low to moderate levels of risk following a maltreatment report, most commonly as an arm of CPS. CR programs are intended for families reported to CPS, but whose cases CPS closes at the point of a maltreatment report screening or investigation. Although CR programs are typically intended only for families reported to and diverted from CPS, they could potentially serve families who self-refer, as some CR programs in Wisconsin later chose to do. Families may move along this continuum at various points, according to their constellation of risk and protective factors and the service capacity of each component of the continuum.
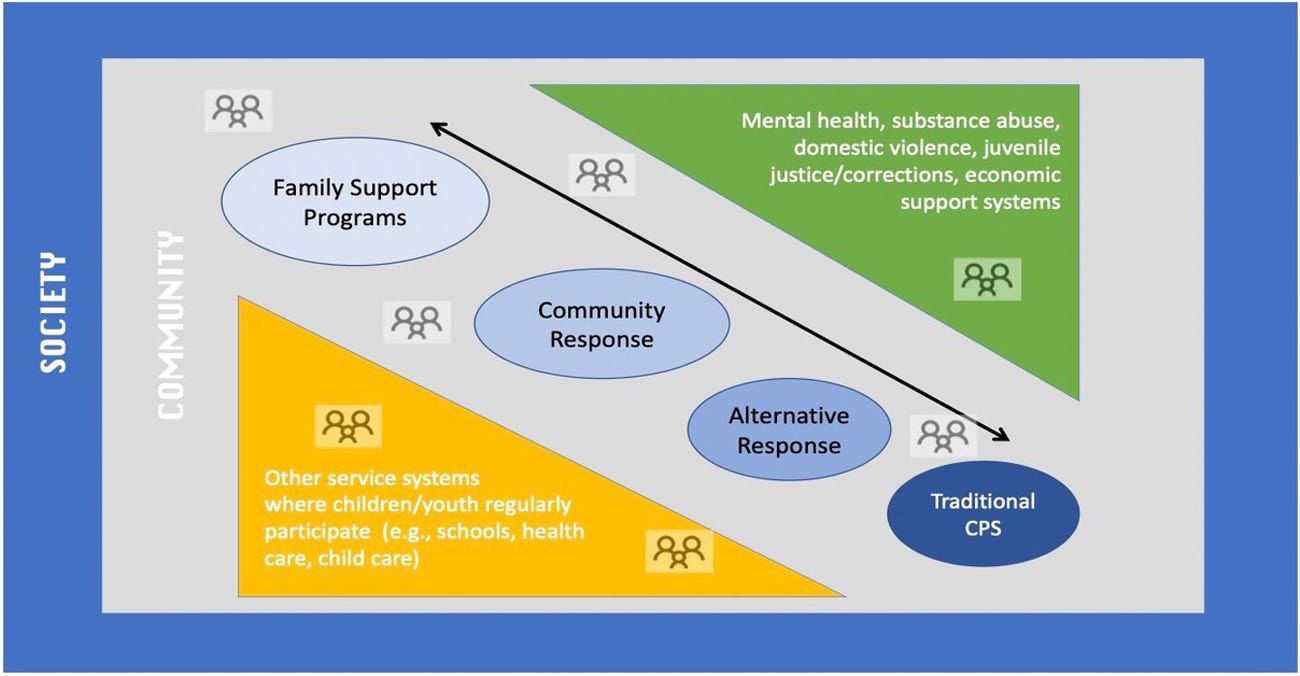
Components of a Child Maltreatment Prevention Infrastructure
Figure 3 also depicts service systems in which families may be dually involved, or which they may potentially access. These include involuntary systems such as corrections, systems designed to address other types of risk factors (e.g., mental health, economic support), as well as more universal or normative systems and programs, such as education, health care, and childcare. Throughout and across the formal components depicted in the figure are informal networks of kin, neighbors, and community members who interact with families on a regular basis, serving as sources of support (or impediments) to family functioning. Finally, this infrastructure must be attuned and responsive to community and societal influences that affect child maltreatment trends and outcomes, including changes in policies, economic shifts, and changes in community demographic composition.
All of these programs, systems, and networks may function independently or interactively in ways that can be supportive, but they may also operate in ways that can serve as barriers to child and family well-being (see Feely et al., this volume; Merritt, this volume). And when they operate in a siloed fashion, even if channels of information sharing and communication are established among them, child maltreatment prevention results are not necessarily achieved. A report from IOM and NRC (2014) articulates several elements deemed essential to building an “integrated system of care,” which can be grouped according to their focus on planning and collaboration activities (i.e., foundational infrastructure); operations and workforce development (implementation infrastructure); and fiscal capacity, community and political support, communications, and evaluation (sustaining infrastructure). The report highlights, in particular, the roles of organizational culture in program delivery and characteristics and contexts of interagency networks that are believed to engender and sustain interagency collaboration. In short, there are numerous and complex factors that need consideration in efforts to effectively design and leverage components of a prevention infrastructure. However, nearly 40 percent of U.S. children experience a CPS investigation at some point in their childhoods (Kim et al. 2017)—an astonishing statistic that warrants a commensurate policy response. It is nothing short of imperative that we establish a sustainable and well-resourced prevention infrastructure that can create meaningful reductions in child maltreatment.
One potential conclusion from our focus on CPS-diverted families and their high risk for reinvolvement with the CPS system is that the system should broaden its capacity to serve such families—that is, that more of these diverted families should actually be screened in for ongoing CPS services. We do not endorse this view for several reasons. First, CPS involvement tends to be unwelcomed by families, highly stigmatized, intrusive, antagonistic, and traumatic for families (see Dettlaff and Boyd, this volume; Merritt, this volume).
Second, decades of research on the etiology of child maltreatment have demonstrated that poverty and various measures of economic hardship are repeatedly correlated with indicators of child maltreatment and CPS involvement (Gelles 1992; Gil 1970; Giovannoni and Billingsley 1970; IOM and NRC 2014; Pelton 1978, 1981, 1994, 2015, 2016; Wolock and Horowitz 1979). Large-scale cross-sectional studies, such as the National Incidence Studies and the National Family Violence Surveys, have demonstrated an inverse association between income and maltreatment (Sedlak and Broadhurst 1996; Sedlak et al. 2010; Berger 2004; Gelles 1992). Research has also shown that various indicators of maltreatment correlate with community- or state-level poverty rates (Coulton et al. 2007, 1995; Drake and Pandey 1996; Maguire-Jack 2014), income inequality (Eckenrode et al. 2014), and welfare receipt rates and benefit levels (Paxson and Waldfogel 2002; Slack et al. 2003). Furthermore, within low-income populations or populations at elevated risk of child maltreatment, research has shown that economic hardship (e.g., welfare sanctions, utility shut-offs, unemployment, housing moves, self-reported material hardship) increases the risk of CPS involvement (McDaniel and Slack 2005; Courtney et al. 2005; Slack, Lee, and Berger 2007; Slack et al. 2004, 2011). And a growing body of national and international research suggests that this relationship is causal (Berger et al. 2017; Cancian, Yang, and Slack 2013; Lindo, Schaller, and Hansen 2013; Raissian and Bullinger 2017; Schneider, Waldfogel, and Brooks-Gunn 2017; Wildeman and Fallesen 2017).
Third, studies that exploit exogenous changes to the economic safety net in the United States suggest that maltreatment rates and risks are sensitive to the accessibility and generosity of social welfare benefits (Berger et al. 2017; Cancian, Yang, and Slack 2013; Raissian and Bullinger 2017). Finally, the United States has a residual welfare state, which is characterized by siloed systems with policies and rules that can be complex to navigate and even conflictual in their requirements, and an increasing reliance on policy levers and administrative practices that restrict access to the safety net (Herd and Moynihan 2019; Fox and Feng 2019). These factors, coupled with the knowledge that families diverted from CPS identify economic stressors as their primary concern, points us in the direction of taking a closer look at how various social welfare benefit programs and systems might more adequately address the basic needs of families struggling on the economic margins. We concur with Feely et al. (this volume) that a more synergistic system is needed that considers the provision of basic needs a necessary component for the “safe and consistent care” of children and see their mission as one aligned with child maltreatment prevention. And like Roygardner, Hughes, and Pulasci (this volume), we believe that secondary prevention efforts, such as CR, in the context of larger scale efforts to prevent child maltreatment, are a critical component of a prevention infrastructure.
Leroy Pelton was one of the earliest scholars to draw attention to the role of poverty in the child welfare system and as a risk for one’s involvement in it (Pelton 1978, 1981, 1994, 2015, 2016). He was particularly concerned about what he viewed as a tendency for the child welfare system to conflate poverty with child neglect and to place the onus of responsibility for perceived neglect on the parent, rather than on the systems and contexts in which a family is situated. One policy recommendation from Pelton deserves particular attention: he recommended that a “social dividend, an annual common cash benefit would be allocated to every member of the community, adjusted only for household size, and would replace current public assistance and entitlement cash distribution programs, as well as tax-break programs” (Pelton 2015, 36; see also Pelton 2005). This recommendation is similar to contemporary calls for a universal basic income (UBI) (Hughes 2020), an idea first seriously considered in the United States by President Nixon, in the form of a guaranteed minimum income, proposed as part of his Family Assistance Plan (Quadagno 1990). Although Nixon’s proposal was ultimately defeated, it has renewed relevance today. Given the complexities of and costly system oversight required for the myriad means-tested benefits that compose the U.S. economic safety net, coupled with the growing evidence that safety net transfers have the potential to prevent child maltreatment, a UBI has the potential to create a minimal standard of economic stability for families and reduce the need for deeper-end systems involvement. Indeed, the National Academies of Sciences, Engineering, and Medicine’s (2019) recent report A Roadmap to Reducing Child Poverty, estimates that providing a modest monthly universal child allowance could lead to a dramatic reduction in poverty for families with children.
In sum, we make three policy recommendations stemming from our review of whom the CPS system serves and does not serve, and the implications for child maltreatment prevention. First, systems that serve children and families external to the child welfare system should develop—through workforce training, policies, and practice shifts—a greater understanding of their role in child maltreatment prevention, and their capacity to reduce demands on deep-end systems like child welfare. Second, programs such as CR should be eligible for Family First funding, given their similarity to kinship navigator programs (already eligible under this legislation), their emerging evidence base, and their ability to reach an identified population known to be at high risk for future CPS involvement. We also urge that such programs be subject to rigorous evaluation. Third, given the staggering rates of childhood CPS involvement in the United States, the robust evidence that economic stress and instability contribute to this involvement, and the inherent complexity of this country’s siloed economic safety net, we argue that a universal child allowance would contribute to a meaningful reduction in the need for CPS intervention. We recognize that our final recommendation may face more of an uphill battle than the previous two and, if it were to be enacted, may reduce (but not eliminate) the need for the first two proposals. However, we believe that with this policy solution, we would likely see immediate impact on child maltreatment rates that would generate longer-term savings to society.
Conclusion
In this article, we have provided an overview of the “front end” of the child welfare system, commonly referred to as child protective services or CPS, and its performance with respect to identifying families in which child maltreatment has occurred or is at risk of occurring. This review is offered at a moment when child protection practices in the United States are shifting to encompass more prevention-oriented services, which necessitates a critical look at the infrastructure currently in place for preventing child abuse and neglect. We present components of a prevention system that should be considered in efforts to better coordinate and deliver proactive services to families at risk of child maltreatment and CPS involvement, with particular attention to a previously overlooked population—families reported to but diverted from CPS.
This population is the largest group to encounter CPS, yet historically the system has done little to engage and offer them services to prevent maltreatment recurrence and rereports to CPS. We argue that the diversion of families reported to CPS should not necessarily be considered a failure of CPS systems but, rather, a reflection of the insufficient social safety net for disadvantaged families in the United States. Meaningful and significant reductions in child maltreatment in the United States will not likely be accomplished without attending to safety net programs and systems to ensure that they are facilitating (and not hindering) access by eligible families, providing reasonable levels of support, and working together to coordinate service delivery. More robust antipoverty policies and programs are not the panacea for child maltreatment; nor will they diminish maltreatment risk for every child. However, given the extensive evidence demonstrating a strong relationship between economic disadvantage and child maltreatment, including evidence that this relationship is causal, concerted efforts to address poverty are a worthwhile investment from a prevention perspective.
Footnotes
Notes
Kristen S. Slack is a professor at the University of Wisconsin–Madison School of Social Work. Her research focuses on understanding the role of poverty and economic hardship in the etiology of child maltreatment, caseload dynamics of child welfare systems in relation to other public benefit systems, and community-based programs designed to prevent child maltreatment.
Lawrence M. Berger is Vilas Distinguished Achievement Professor of Social Work and former director of the Institute for Research on Poverty at the University of Wisconsin–Madison. His research focuses on the ways in which economic resources, sociodemographic characteristics, and public policies affect parental behaviors and child and family well-being.